
Abstract
Background:
Coronavirus illness (COVID-19) has spread globally and is affecting everyone severely. The evaluation of educational needs (knowledge, attitudes, and practices) is important in controlling COVID-19 situations. The goal of this study is to find out what adults in Ardabil City know, how they feel, and what they do about the COVID-19 infection.
Methods:
In November 2021, a cross-sectional descriptive-correlational survey of 384 people was conducted using stratified-cluster sampling in Ardabil. The researchers created a self-reported questionnaire with 23 items as the data collection technique. The quantitative data were evaluated using descriptive statistics, the chi-square test, the correlation coefficient, and regression analysis.
Results:
The correct answer rate for this research found that 73.17% of participants (n = 281) had appropriate knowledge, 61.19% (n = 235) had favorable attitudes, and 69.53% (n = 267) had enough practice behavior. However, knowledge was related to gender, employment, and location of residence. Age, marital status, education level, and location of residence were all connected with attitude. Age, gender, and marital status were all related to the behavior. The findings of linear regression analysis revealed that knowledge and attitude influence behavior.
Conclusion:
The study findings revealed a high degree of understanding of COVID-19, a positive attitude, and a strong commitment to good practices. Knowledge, attitudes, and behaviors were influenced to varying degrees by age, marital status, education level, employment, and location of residence. Furthermore, knowledge and attitudes influenced behaviors.
Introduction
COVID-19 infection is a new species of the coronavirus family that was first identified in Wuhan city, Hubei province, China, and from there it spread to other countries.1–3 The new coronavirus pandemic in 2021 posed a global health concern. 4 On January 30, 2021, the Director-General of the World Health Organization (WHO) declared the outbreak of coronavirus as a public health emergency and an international concern.5,6 The virus spreads through small droplets from coughing, sneezing, and talking.7,8 Adults may also become infected by touching a contaminated surface and then touching their faces (eyes, nose, and mouth). The transmission also occurs through aerosols that can stay suspended in the air for longer periods.9–11
Statistics showed that the majority of deaths and cases of COVID-19 occurred in people above the age of 50. In people with the underlying disease, there is a risk of infection in the whole population, and the importance of prevention increases in asymptomatic carriers. Asymptomatic people can transmit the disease to a great extent and thus increase mortality.9,12,13 People’s health and safety norms in society play an important role in the transmission and control of this disease. Preventive behaviors that can eliminate the cycle of the disease can include washing hands with soap and water or disinfectant solution; not touching; not rubbing; disinfecting purchased items; car and home environment; social distancing; and home quarantine. 5 For example, preventing the disease requires public health measures like washing hands with soap for at least 20 s, spending less time with other people, putting people in quarantine who have been in contact with an infected person and putting infected people in quarantine. Actions like these need people’s awareness.5,14 A survey showed that health education programs aimed at improving COVID-19 knowledge were helpful for Chinese residents to hold optimistic attitudes and maintain appropriate practices. During the SARS epidemic in 2003, a study evaluated the level of awareness about the disease among older adults. Then the researchers provided them with health education by telephone and assessed the change. 15 In the Mya KS study, 45% of participants washed their hands regularly, 34% avoided travel or trips, and 58% avoided crowded areas to prevent COVID-19. About 47% always covered their mouth and nose during coughing and sneezin. 16 A study showed that 22% of the general population’s preventive behaviors were acceptable. In another study conducted on 240 medical students in Iran, only 85.5% of the participants scored low on the observance of preventive behaviors, and the study researchers cited the level of literacy and greater awareness of this group as one of the reasons for this.17,18 One of the main measures in this situation is protective and healthy behaviors by all members of society. People need to be aware of preventative behaviors to achieve optimal outbreak control. This study aims to assess the KAP of society about COVID-19. The results of these surveys could help people who plan for public health and other health workers.
Materials and methods
Study design and study population
A cross-sectional study was carried out from November 21 to December 25, 2021, with 384 adults (20–80 years) in Ardabil (Ardabil is an ancient city in northwestern Iran and the capital of Ardabil Province) to assess the educational needs among adults in the COVID-19 infection through a web-based survey (because it was not feasible to do a community-based national sampling survey during this government-imposed lockdown). The sample size was determined based on inclusion criteria, 95% confidence level, and 80% test power. The eligibility criteria to participate in this survey were to be adults (20–80 years old), be a resident of Ardabil, be a social media user, have a smartphone, and be willing to participate in the study.
Data collection procedure
Data was collected via a questionnaire designed with the Google survey tool. The link to the survey form was shared randomly as an invitation to participation through social media groups and people’s volunteers. The researchers also shared the link with their contact list. The questionnaire included questions in two parts. Part one (socio-demographic information): age, gender, education level, occupation, marital status, monthly family income, and part two (educational need assessment): knowledge, attitude, and practices toward the COVID-19 infection. The researchers received a total of 454 eligible participants’ feedback, but of those responses, 384 completed questionnaires were selected for the study.
Measurement tool
Socio-demographic information was obtained through close-ended and open-ended questions. The questions were related to their age, gender, education level, occupation, marital status, and monthly family income (this variable was divided into a low socio-economic class family income <30 million Rial, a moderate socio-economic class family income of 30–10 million Rial, and a high socio-economic class family income >10 million Rial). For need assessment, participants’ knowledge of COVID-19 was assessed using six questions, which were adapted from previous research with “true,” “false” or “not sure.” Each correct response to a knowledge item has been assigned 1 point, 0 points have been assigned to each incorrect/not sure response. For knowledge items, the total score ranged from 0 to 6. The higher score indicated the adequacy of knowledge about COVID-19. Bloom’s cut-off of 80% (≥4.8) was used to define adequate knowledge.
The attitude section included five questions, and the responses were assessed using a three-point Likert scale: “Disagree,” “Not sure,” and “Agree”; each weighing 5–15 respectively, and ≥12 was set as a cut-off value for positive attitudes toward COVID-19.
The practice section consisted of four questions that were adapted from the WHO recommendations for the prevention of COVID-19 transmission. The responses to each item were assessed with a two-point Likert scale: “Never” and “Always”; each weighing 0–4 respectively, and a cut-off value of ≥3.2 was set for good practices. Besides, two questions about the main source of information, a favorite educational resource, and use of public transportation were also included.
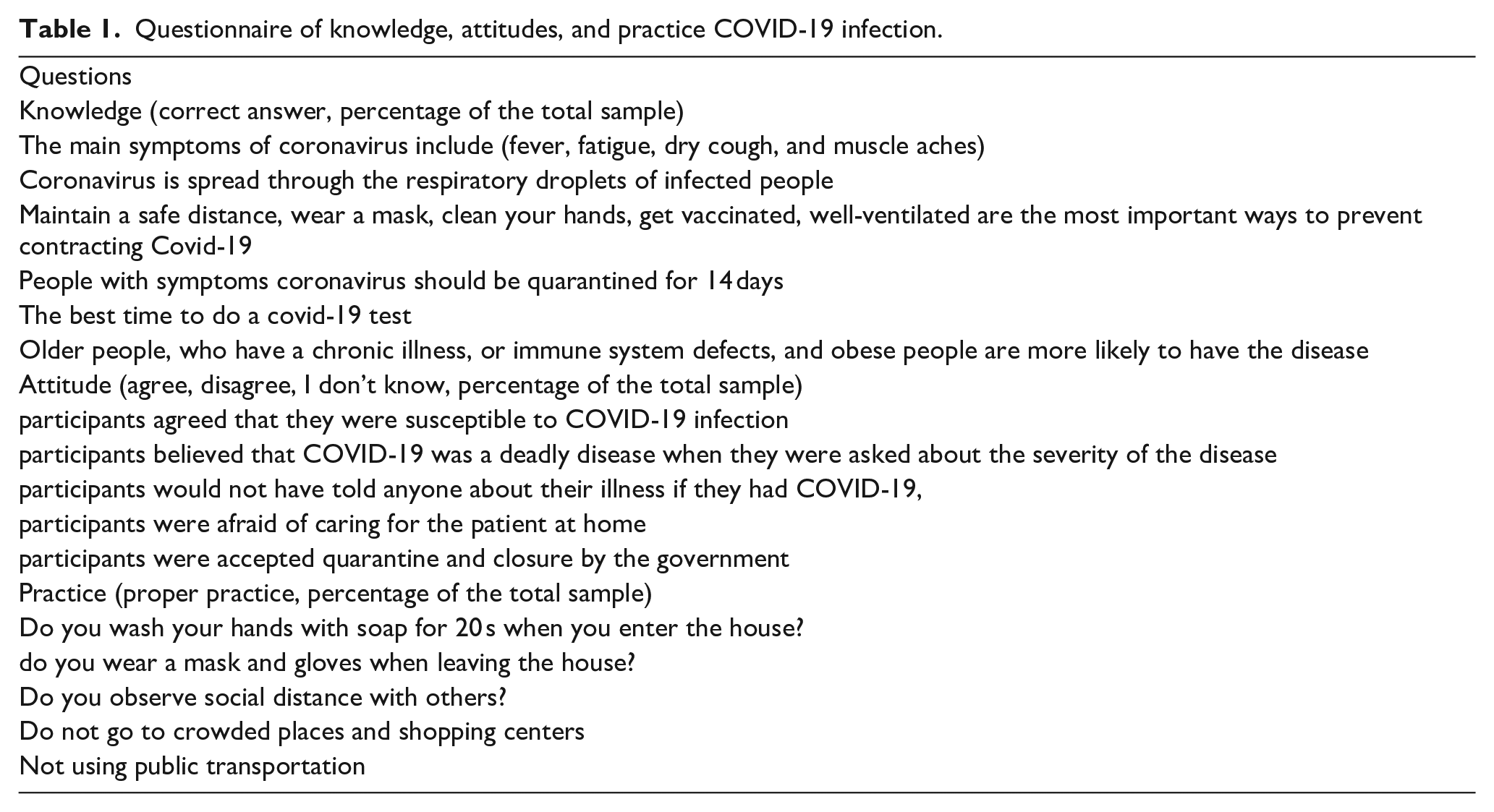
The validity of the questionnaire was determined by two methods of face validity and content validity, which were confirmed by experts in health education, The total content validity index (CVI) in the “relevancy,” “simplicity,” and “clarity” were equal to 83.6, 92.9, and 91.7. The reliability of the questionnaire was further evaluated through internal consistency (α = 0.83) and test-retest (r = 0.82). The list of questions is given in Table 1.
Questionnaire of knowledge, attitudes, and practice COVID-19 infection.
Statistical analysis
Fully completed questionnaires were extracted from Google forms and exported to the Microsoft Excel 2010 software for coding. The data was then exported to the Statistical Package for Social Science (SPSS) version 23 software, which was used to analyze the quantitative data using descriptive statistics, the chi-square test, the correlation coefficient, and regression analysis. Level of p < 0.05.
Results
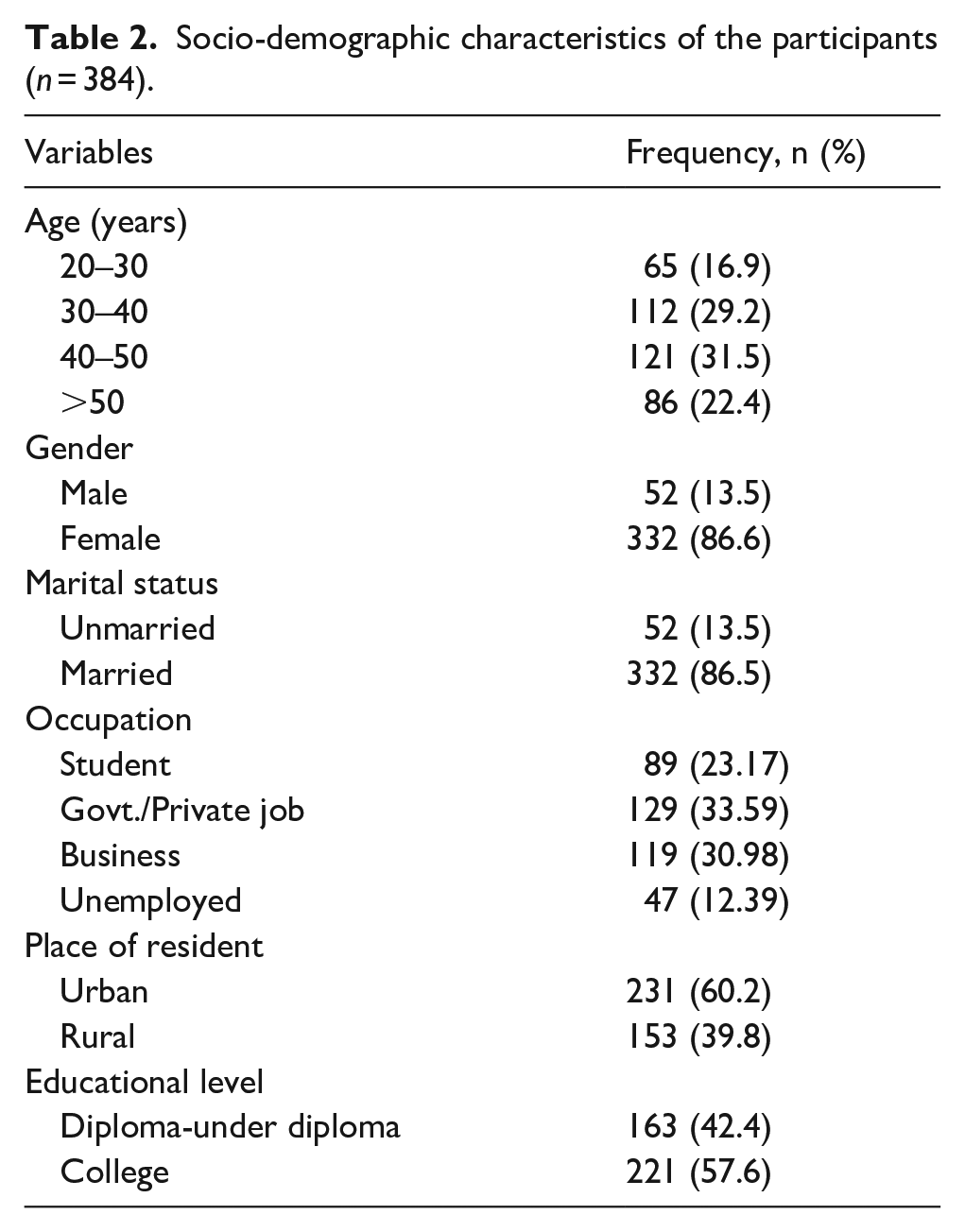
A total of 384 participants completed the survey questionnaire and participated in this study, with a mean age of 42.47 ± 12.07 years. The majority of the participants were female (n = 213, 55.4%), married (n = 332, 86.4%), and had a college degree (n = 163, 42.4%). The rest of the participants had an education level diploma or below. Among the respondents, 89 (23.17%) were students, and 129 (33.59%) were employed either by the government/a private company. Most of the participants were from urban areas (n = 231, 60.1%) and rural areas (n = 153, 39.8%). A detailed description of the socio-demographic characteristics of the participants is shown in Table 2. Social media such as WhatsApp and Instagram were the main sources of information about COVID-19 among participants. 34.1% of participants relied on TV and radio, 43% followed cyberspace, and 22.9% on friends and family to get information about COVID-19. This study revealed that 73.17% of participants (n = 281) had sufficient knowledge, 61.19% (n = 235) had positive attitudes, and 69.53% (n = 267) had adequate practice behavior.
Socio-demographic characteristics of the participants (n = 384).
Knowledge about COVID-19
The mean COVID-19 knowledge score for participants was 4.37 ± 1.41(range: 0–6). A higher proportion of the participants (n = 243, 62.2%) was identified with main clinical symptoms of coronavirus of COVID-19 (The main clinical symptoms of coronavirus include fever, fatigue, dry cough, and muscle aches). 71.3% (n = 274) of the participants knew how the disease spread, 72.3% (n = 278) perceived the common ways to prevent the infection, and more than half of the participants had adequate information on how to use, replace the facial mask and home care (quarantine). But only 33.9% knew when to go for a PCR test, 74.7% participants identified individuals at risk for COVID-19 (elderly, pregnant women, people with chronic diseases). Participants’ knowledge significantly differed across genders, occupations, and residence places and income (p < 0.05, Table 3).
Prediction of COVID-19-related behaviors.

Attitude toward COVID-19
The mean attitude score was 8.08 ± 1.86. About 67.4% (259) of the participants agreed that they were susceptible to COVID-19 infection, and 30.4% (117) of the participants believed that COVID-19 was a deadly disease when they were asked about the severity of the disease. But 42.1% (162) of the participants would not have told anyone about their illness if they had COVID-19, and 52.9% (n = 203) were afraid of caring for the patient at home; 71.4% (n = 274) accepted quarantine and closure by the government. The researchers found a statistically significant association between attitude and socio-demographic variables such as age group, gender, and marital status (p < 0.05, Table 3).
Practices toward COVID-19
In terms of practices toward COVID-19, 65.1% (n = 250) of the participants always washed their hands with soap or hand sanitizer. 71.8% (n = 276) always wore a facial mask when going outside. Even though 56.7% (n = 218) maintained safe distance with people and 34.9% (n = 134) did not maintain social distancing due to the use of facial masks.
70.8% (n = 272) of participants visited crowded places over the past week, 71.6% (n = 275) used public transportation at least once in the past week. The participant’s practice score was significantly different in terms of age-groups, gender, and marital status (p < 0.05, Table 3).
In this study, 23% of participants thought that antibiotics could be a cure for COVID-19 infection. One-third of participants considered local treatments, such as gargling with hot water, drinking honey, and lemon juice, to cure COVID-19. 39.1% of the people who took part thought that education, 38.8% law, and 22.4% vaccines were the most important ways to stop this disease. The results of linear regression analysis showed that attitude and knowledge had a correlation with practice (p = .001) (Table 4).
Relation between socio-demographic characteristics and mean KAP score.

Discussion
The COVID-19 infection is a global threat due to the lack of vaccines and definitive treatment. In this regard, health education and incubation is the most important strategies for disease management.17,19,20 In this present study, we evaluated educational needs (knowledge, attitudes, and practices) toward COVID-19 among adults in Ardabil, Iran.
From the 384 respondents, the accurate response rate revealed that 73.17% of participants had sufficient knowledge, 61.19% had positive attitudes, and 69.53% had adequate practicing behavior. However, knowledge was associated with gender, occupation, and place of residence. Attitude was associated with age, marital status, level of education, and place of residence. The practice was associated with age, gender, and marital status. The results of linear regression analysis showed that knowledge and attitude affect behavior.
In the Mya Kyaw 15 study, results showed that participants were very aware of the transmission of the disease, but 14% of them did not have any knowledge about the symptoms of COVID-19 infection. 21 Our results showed that the participants had the best knowledge about the symptoms and prevention of the disease. Conversely, the lowest level of knowledge was related to the diagnostic tests and incubation time. In a study, results revealed that the lowest level of knowledge among nurses was about COVID-19 and ways of prevention, disease symptoms, and the incubation period.22,23 Differences in outcomes between the studies may be due to the difference in timing and the diverse composition of participants. 24 It is important for health systems to examine the needs and temporal and spatial conditions of the participants before the educational interventions.25,26
The results of our study showed that the level of COVID-19 knowledge differed by socio-demographic factors, which could make them more vulnerable to the pandemic. This result coincides with those of other similar studies performed among public and healthcare professionals in various studies.4,27–32
In the present study, participants showed extremely positive attitudes toward COVID-19. A total of 67.4% of participants considered themselves vulnerable. Moreover, 58.9% of the participants considered it a dangerous disease, 52.9% expressed fear of infection for themselves and their families, and 45.3% would not tell anyone if they were infected. The role of the government in controlling the disease was considered important, which was similar to the results obtained from Gao’s study. Evidence from the SARS epidemic demonstrated that a high level of trust in the government allowed the disease to be successfully controlled, 4 and a recent KAP study on COVID-19 found a positive attitude among 90.8% of Chinese people.33,34
The majority of the public adhered to good practices concerning COVID-19 infection, potentially because they had good COVID-19 knowledge and a positive attitude, which ultimately translated into good practice.
However, the least common practices among participants were hand washing, social distancing, and not avoiding family gatherings. Perhaps the shortage of protective equipment, such as alcohol gel or “sanitizer, and contradictory information during the outbreak triggered the pandemic.31,35,36 The results of a survey of the Sari Birth Cohort showed that practice among those participating during the pandemic is weak.37,38
This study explored that age was a factor that influenced the public’s knowledge about COVID-19. The younger people had less knowledge than their counterparts, which was potentially attributed to the increases in social experience and knowledge associated with age. Marital status, education, occupation, and place of residence all had an impact on KAP. Married people had a better grasp of knowledge, more protective attitudes, and higher adherence.
Conclusion
In conclusion, the findings of this research evaluated the knowledge, attitude, and practice of adults in the COVID-19 infection. This study also showed that a considerable number of adults were adequately knowledgeable about this pandemic and discovered a positive attitude but were insensitive to appropriate preventive measures, which could be alarming. Therefore, effective health education is required to identify the gaps and initiate planning accordingly.
Footnotes
Acknowledgements
Our grateful thanks go to all participants in the present study.
Contributions
NN, RT, and NK, conceptualized and designed the study. FC, SSO, and AF collected the data and conducted the formal analysis. AM, NH, and AEFA drafted the manuscript. NN, AZ and FY critically reviewed the manuscript. All authors approved the final version of this manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was drawn from a research project (No. IR.AUMS.REC. 1399.089) sponsored by the Deputy of Research and Technology at AUMS. Participants were aware of the purpose of the study and provided informed consent prior to accessing the questionnaire and participated voluntarily. No compensation was provided, and all collected data was stored securely.
Patient consent for publication
Consent from the patient for publication was taken before collecting the data from them.
Informed consent
Written informed consent was obtained from participation.
Availability of data and materials
All the datasets supporting our findings have been presented in the manuscript; the datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.