
Abstract
Patient-reported outcomes of mental health treatment, such as perceived effectiveness, are important. They indicate whether treatment is perceived to reduce symptoms and minimize psychiatric disability. Outpatient treatment for depression typically includes medication or counseling, either alone or in combination. This study examines the relationship between treatment modality and perceived effectiveness of treatment. Using a sample of adults who received outpatient treatment for depression from the 2015-2016 National Survey on Drug Use and Health (N = 4169), logistic regressions estimated the odds of rating treatment as effective among persons who received medication only, counseling only, and a combination of medication and counseling. There were no differences in perceived effectiveness between counseling only and medication only. However, receiving both was associated with greater odds of rating treatment as effective. Poor self-rated health and severe mental illness were associated with lower perceived effectiveness of medication. Those with substance use problems had lower odds of rating counseling and both counseling and medication as effective. A combined treatment for depression may be perceived as better than single-modality treatment. Therefore, there might be benefits to increasing access to both forms of treatment for persons less likely to rate either single modality as effective.
Background
Depression is one of the most common mental disorders and a leading cause of disability worldwide.1,2 The most common outpatient treatment modalities for depression are medications and counseling (psychotherapy), either alone or in combination.3,4 In the United States, the incidence and prevalence of depression have increased steadily, 5 and although treatment rates have also increased,6,7 a significant proportion of people who would benefit from treatment do not receive the services they need.8,9 This treatment gap increases the economic burden, societal costs, and consequences of untreated mental illness on individuals and the society.10 -12 Understanding barriers to treatment is important and has been the subject of substantial research attention.13 -17 While informative, this research does not connect the treatment gap to patient-reported outcomes of care. Patient-reported outcome measures are important indicators of the extent to which health services improve the lives of those who receive them. 18 How people rate the outcomes of care that they receive might influence overall perceptions of treatment and future use of mental health services.
One of the central challenges in the provision of treatment services for depression is determining which treatment approaches work for who. 19 Patients’ views of the effectiveness of different types of treatment are important but underexplored in psychiatric services research. Indeed, perceived effectiveness of treatment indicates overall satisfaction with mental health services 20 and influences support for policies that improve psychiatric services. 21 The effectiveness of mental health services can be measured using instruments that assess changes in symptoms. Changes in general functioning including self-reported improvements in symptoms matter and are as much treatment goals as physician-assessed measures of treatment effectiveness. 22 Generally, clinician-rated measures of depression treatment effectiveness have higher effect sizes than patient-reported outcomes of services. 23 Given that self-reported depression treatment outcomes are more conservative, they might be useful measures of treatment effectiveness as they present a lower chance of overestimating the benefits of treatment. In addition, how people subjectively describe outcomes of treatment may tell us whether treatment or counseling helped them. Perceived effectiveness of mental health services also indicates patient-centeredness and the quality of care, explains why people dropout of treatment, and predicts future engagement with mental health services.24-26 Therefore, one way of improving the utilization of mental health services is to improve the perceived effectiveness of treatment.
In the current study, we identify factors associated with perceived effectiveness of mental health services among adults with depression. We examine the relationship between treatment modality, patient characteristics, and perceived effectiveness of depression treatment. Maximizing outcomes of mental health services—including perceived effectiveness of treatment—might depend on the degree to which there is a match between individual characteristics and treatment modalities.
Methods
Data
We used de-identified public-use data from the 2015-2016 National Survey on Drug Use and Health (NSDUH). The NSDUH is a multistage probability sample survey conducted by the Substance Abuse and Mental Health Services Administration and provides annual national estimates on substance use, mental illnesses and mental health service use among the civilian, noninstitutionalized population ages 12 years and above in the United States. 27 Survey response rates were 55.2% and 53.5% in 2015 and 2016, respectively. The analytic sample for our analyses consisted of adults who met the criteria for having a major depressive episode in the past year. The NSDUH has a variable that indicates whether respondents received mental health treatment. We limited our sample to persons who reported that they received professional mental health services in an outpatient setting in the form of prescription medication, treatment, or counseling (N = 4169).
Measures
Respondents were asked whether in the 12 months preceding the survey, they received treatment or counseling for mental health and if they received prescription medication for mental health from a doctor or health professional. We created a mutually exclusive variable for treatment modality: (1) medication only (respondent received prescription medication only), (2) treatment/counseling only (respondent reported seeing a doctor or health professional about their mental health but did not receive any medications), and (3) medication and counseling/treatment (respondent received prescription medication and also talked to a health professional about their symptoms). In the NSDUH, respondents who were prescribed medications were asked how much the medications helped with their symptoms. Respondents who received counseling were also asked how much it helped them. Consistent with other research, 28 we created a binary variable for perceived effectiveness of treatment: not effective if the respondent said “not at all” or “a little” and effective if they said “some,” “a lot,” or “extremely.” Among those who received both medication and counseling, treatment was considered effective if either medication or counseling was rated as having helped some, a lot, or extremely. Respondents’ reports of perceived effectiveness of treatment were not validated by clinicians.
Patients also reported what best described how they entered care. The pathway to care variable was created with 3 mutually exclusive categories: (1) independent entry if the respondent decided on their own to get treatment, (2) asked by someone if respondent entered care because someone else thought they should, and (3) ordered if the respondent was ordered to enter into care. Sociodemographic covariates include sex (male and female), race/ethnicity (non-Hispanic white, non-Hispanic black/African American, Latinx/Hispanic, and other), age category (18-25, 26-34, 35-49, 50-64, 65+ years), residence size (large metro, small metro, nonmetro), highest level of education (<high school, high school, some college, college graduate), employment status (not looking/not in the labor force, unemployed, employed), and level of poverty, <100% of the federal poverty level (FPL), 100% to 199% FPL, and ⩾200% FPL. We included the following health status variable: self-rated overall health (poor/fair vs good/v.good/excellent), health insurance status (insured vs uninsured), whether respondent met Diagnostic and Statistical Manual of Mental Disorders (DSM) criteria for substance abuse or dependence (yes/no), respondent’s probability of having a severe mental illness (0.0-0.9), and whether the respondent also received mental health treatment in an inpatient setting in the past year (yes/no). The probability of severe mental illness was computed for each respondent using responses to questions that assessed past year major depressive episode, in addition to serious suicidal ideation, psychological distress and disability scores using the World Health Organization Disability Assessment Schedule (WHODAS).
Analysis strategy
We describe the characteristics of respondents and then compute odds of rating treatment as effective for each treatment type while controlling for respondents’ characteristics and their pathway into care. We applied weights in all analyses to ensure that our estimates represent the population from 2015 to 2016 and adjusted standard errors for the complex survey design.
Results
Characteristics of the sample of respondents who used professional outpatient mental health services for depression are presented in Table 1. About two-thirds of the respondents received both medication and counseling, 1 in 10 received medication only and almost a quarter received counseling only. Overall, about 8 in 10 respondents with depression thought that the treatment they received was effective. Almost 5% of the respondents were ordered into treatment and the majority independently sought treatment for depression (82.4%). Respondents are predominately women (71%). Nine in 10 had health insurance, 20% met criteria for substance abuse or dependence, and 60% met the criteria for likely severe mental illness.
Characteristics of adults with major depression and who received outpatient treatment for depression, 2015-2016 National Survey on Drug Use and Health.
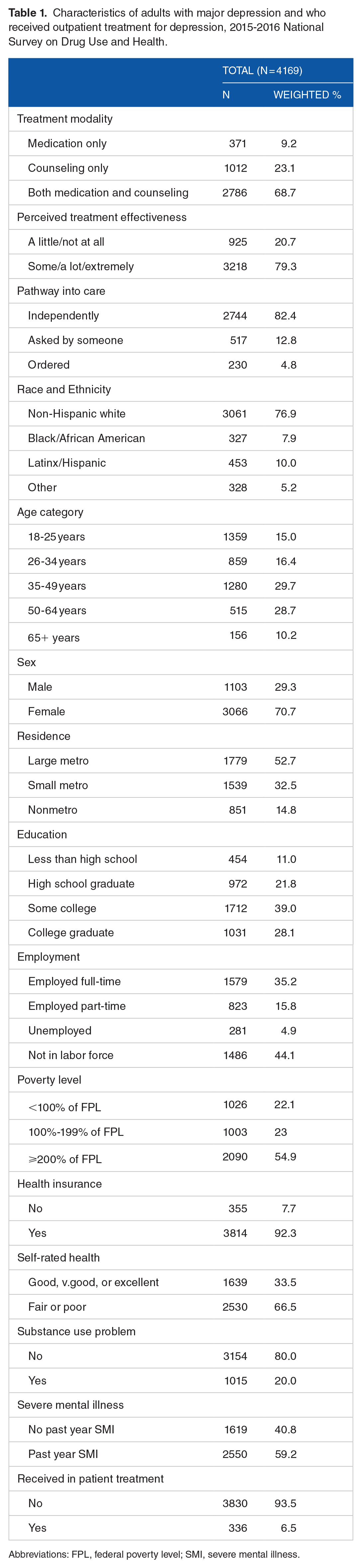
Abbreviations: FPL, federal poverty level; SMI, severe mental illness.
We examined factors associated with perceptions of treatment effectiveness (Table 2). In the full sample, there were no differences in the perceived effectiveness of treatment between recipients of counseling-only treatment and those who received prescription medication. However, persons who received both medication and counseling had significantly greater odds (odds ratio [OR] = 2.35; standard error [SE] = 0.58) of rating treatment as effective. Being ordered into care was associated with lower odds of perceived effectiveness of treatment (OR = 0.50; SE = 0.15). Compared with whites, blacks/African Americans had significantly lower odds of rating treatment as effective (OR = 0.49; SE = 0.11). Older age was associated with greater odds of perceiving mental health services as effective. Respondents who rated their overall health as fair or poor and adults with severe mental illness were less likely to rate treatment as effective were less likely to believe the treatment was effective.
Odds of perceiving treatment as effective.
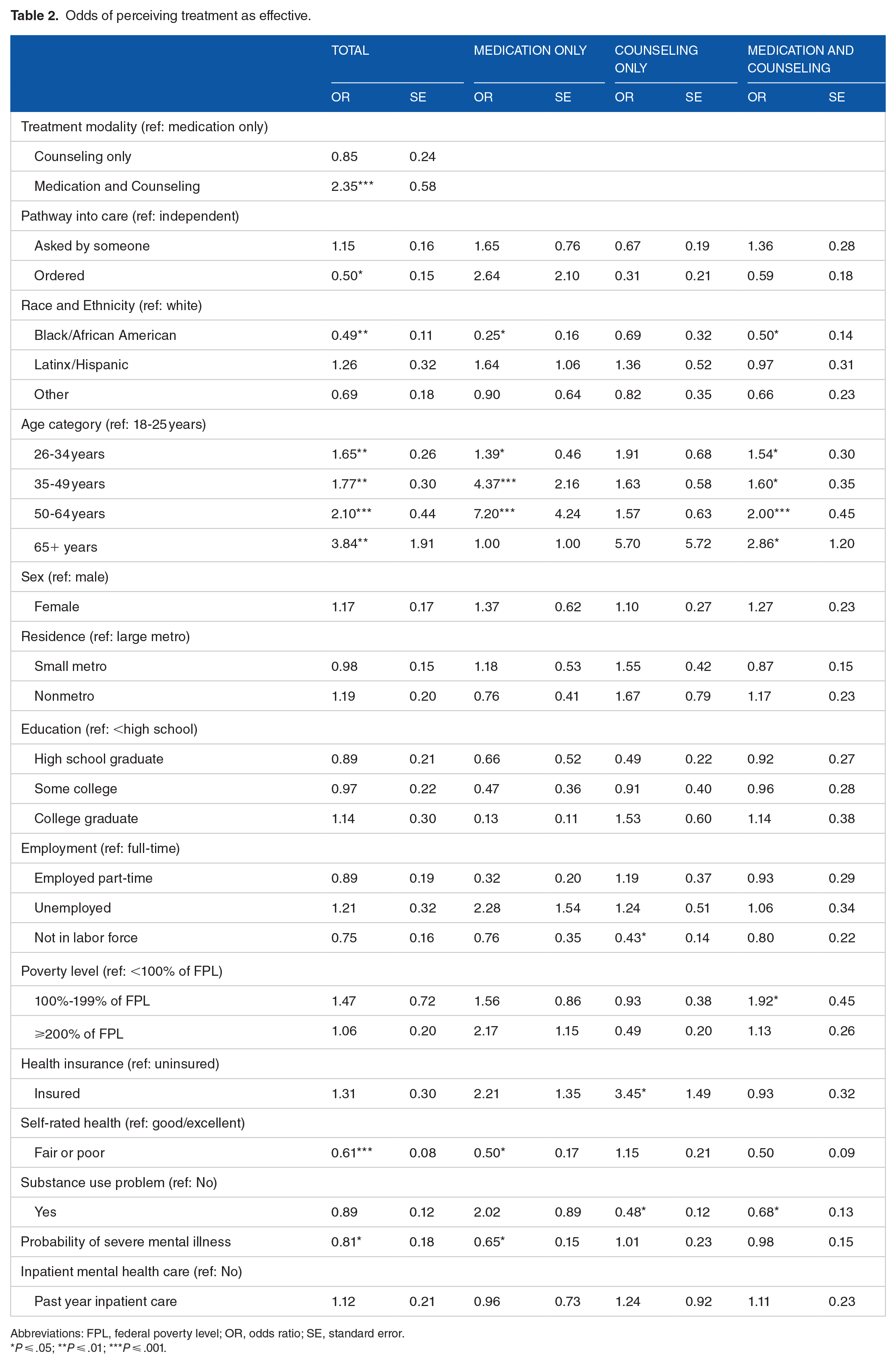
Abbreviations: FPL, federal poverty level; OR, odds ratio; SE, standard error.
P ⩽ .05; **P ⩽ .01; ***P ⩽ .001.
Among adults who used only prescription medication for the treatment of depression, race, age, and health status were associated with perceived effectiveness of medication. Blacks were less likely than whites to rate medications as helpful (OR = 0.25; SE = 0.16), and persons aged 26 to 64 years were more likely than 18 to 25 year olds to rate medications as effective. However, the odds of perceiving medications as effective were lower among persons with fair or poor self-rated health compared with those with good self-rated health (OR = 0.50; SE = 0.17), and 0.1 increase in the probability of having a severe mental illness was associated with 35% lower odds of rating medications as effective (OR = 0.65; SE = 0.15).
Among persons who received counseling but no medications, only employment status, health insurance, and substance use were associated with perceived effectiveness of counseling. Compared with full-time workers, those not in the labor force were less likely to rate counseling as effective (OR = 0.43; SE = 0.14). Insured persons were significantly more likely to rate counseling as effective compared with those who were uninsured (OR = 3.45; SE = 1.49). Persons who met the criteria for a substance use problem were less likely to rate counseling as effective (OR = 0.48; SE = 0.12).
Finally, among those who received both medication and counseling, race, age, poverty level, and having a substance use problem were associated with perceived effectiveness of treatment. African Americans had 50% lower odds of rating treatment as effective (OR = 0.50; SE = 0.14) compared with whites. Older persons were more likely to rate treatment as effective compared with persons 18 to 25 years of age. Persons within 100% to 199% of the federal poverty level had greater odds of perceiving treatment as effective compared with those living below 100% of the poverty level (OR = 1.92; SE = 0.45), and those who met criteria for a substance use problem were less likely to rate treatment as effective (OR = 0.68; SE = 0.13).
Discussion
The main findings from this study are that patient characteristics and treatment modality influence subjective assessments of treatment outcomes. Specifically, there are no differences in patient-reported outcomes of counseling-only treatment and medication-only treatment. However, patients who receive both medication and counseling are more likely to perceive treatment as effective. Prior research suggests that treatment efficacy is slightly greater when combination treatment is used for depression.29-31
Most respondents in this study believed that the treatment they received helped, and most received combination treatment for depression. If perceived treatment effectiveness is any indication of efficacy, then our findings are encouraging. But we also found that poor self-rated health and greater probability of having a severe mental illness (full sample and those receiving medication-only), and substance use problems (those receiving counseling-only and combined treatment) were associated with low perceived effectiveness of treatment. This is troubling because we expect treatment to benefit people with severe mental illnesses and those with substance use problems.
Consistent with previous work, being black/African American compared with being white, and being ordered to seek care, was associated with lower perceived effectiveness of treatment for depression, compared with seeking care independently. 28 Independent entry into care and being white might indicate fewer barriers to care as well as access to resources.13,32,33 The association between increasing age and perceived effectiveness of treatment might reflect satisfaction with psychiatric services or attitudes toward mental health services, both of which become increasingly positive as people get older.34,35 Antidepressants are among the most commonly prescribed medications in the United States especially young and middle-age adults.36-40 It is not surprising then that among those who only used medications, being 26 years or older was associated with greater odds of perceived effectiveness of medications. Not being in the labor force was associated with lower odds of perceived effectiveness among persons receiving combination treatment. We think being employed may indicate access to resources that might shape expectations of treatment and that matter for subjective outcomes of mental health services. This warrants further investigation. Similarly, more research is needed to understand why health insurance increases odds of perceived effectiveness among persons having received counseling but not among those who received both counseling and medication.
People with depression might engage in substance use as a means to cope with depression 41 and while medications can help with depression, they often have less desirable effects for people with substance use disorders due to antidepressant and substance interactions.41,42 Counseling is assumed to lead to lasting therapeutic alliances. 43 Given that comorbid depression and substance use disorders might indicate complexity, it is concerning that among the subsamples who received counseling only and both counseling and medications for major depressive disorder, those who met criteria for substance use disorder were less likely to perceive treatment as effective compared with their peers with no substance use problems.
Our findings should be considered along with certain caveats. First, treatment modalities and perceived effectiveness of treatment might depend on unobserved factors beyond the patient characteristics measured here. Information on characteristics of the mental health system, nature of health insurance plans, mental health literacy, and specific types of mental health providers was not available. Second, who might have more severe depression, such as persons dealing with homelessness and incarcerated individuals, are less likely to be captured in noninstitutionalized surveys such as the NSDUH. Third, the absence of information, such as dosage of depression medication, specific kind of psychotherapy, or frequency of treatment would provide more context for patients’ perceptions of treatment effectiveness. In the NSDUH, it is unclear the extent to which seeing or talking to a provider about depression constitutes counseling. We are unable to tell who provided counseling or prescribed medications, and whether the kind of supportive clinical care provided alongside antidepressant management might have been perceived as counseling. Information about the content of psychological counseling would have also strengthened our findings.
Conclusions
Treatment modality affects subjective assessments of depression treatment. Perceived effectiveness of treatment reflects both patient-reported experiences of care and patient-reported outcomes of care; important indicators of the quality and efficacy of psychiatric services.44,45 Understanding sociodemographic and health characteristics of patients that influence these measures might help improve psychiatric services and eliminate the depression treatment gap. Research on depression treatment helps us determine who is likely to seek treatment and which treatment is associated with reduced clinical symptoms. This study adds to the literature on depression treatment services by demonstrating that factors such as how people enter into care and the specific kind of treatment they receive are associated with whether they rate treatment as effective.
We also show that factors that are associated with the perceived effectiveness of one treatment modality may not matter for another treatment modality. There may be benefits to increasing access to both medication and counseling for persons who are less likely to rate a single modality treatment as effective. This includes people ordered into care and blacks/African Americans who are generally less likely to rate mental health services as effective. Finally, the association between comorbid substance use, treatment modality, and perceptions about the effectiveness of treatment for depression underscores the challenges of identifying which treatment approaches might work for who. Given the high comorbidity between substance use (including the current focus on opiates) and depression, researchers need to redirect attention to finding treatment approaches that work for persons with psychiatric and substance use comorbidities.
Footnotes
Author Contributions
Sirry Alang conceptualised the study and led the data analysis. Donna McAlpine assisted with the data analysis and led the interpretation of findings.
Declaration of conflicting interest:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.