
Abstract
Background:
Salmonella and Shigella infections are a common public health problem throughout the world. The risk of getting infections is high, where asymptomatic street food vendors are preparing foods and vending. Current knowledge of antimicrobial susceptibility pattern is essential for appropriate treatment and management of these infections.
Objective:
This study was aimed to determine the prevalence, antimicrobial susceptibility pattern, and associated factors of Salmonella and Shigella among asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia.
Methods:
A cross-sectional study was conducted among 218 randomly selected asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia from May to July 2017. Data on the sociodemographic and associated factors were collected using a pretested structured questionnaire. The stool specimens collected were examined for Salmonella and Shigella using recommended culture methods. The antimicrobial susceptibility test was done using the disk diffusion technique. Data were described using descriptive statistical tools. Logistic regression models were used to identify the factors associated with Salmonella and Shigella infections. A P-value ⩽ .05 was considered statistically significant.
Results:
The overall prevalence of Salmonella and Shigella was 8.7% (95% confidence interval: 5.6, 10.3). The most common isolates were Salmonella (6%). Most of the isolates were resistant to amoxicillin (97.7%), ampicillin (89.5%), and tetracycline (68.4%). Almost half (47.4%) of Salmonella isolates were multidrug resistant. Food vendors who did not wash hands with soap after the use of the toilet (adjusted odds ratio: 3.3, 95% confidence interval: 1.2, 7.9), and who had untrimmed fingernails (adjusted odds ratio: 4.4, 95% confidence interval: 1.5, 9.3) had higher odds of Salmonella and Shigella compared with their counterparts.
Conclusions:
The carrier rate of Salmonella and Shigella was relatively low. Most isolates have developed resistance to amoxicillin, ampicillin, and tetracycline. The odds of Salmonella and Shigella was high among those who lack a habit of hand washing with soap after the use of the toilet and with untrimmed fingernails. Regular screening and appropriate hygienic control measures are needed in place to reduce the risk of infections.
Introduction
Foodborne gastroenteritis caused by enteric bacterial pathogens in human remains a major public health problem worldwide. 1 According to the Centers for Disease Control and Prevention (CDC) report, an estimated 48 million illnesses, 128 000 hospitalizations, and 3000 deaths occur in the United States each year due to foodborne diseases. 2 It was also estimated that about 700 000 deaths per year in Africa were caused due to foodborne and waterborne diseases. 3 The problem is exacerbated in countries, where lack of food handling practices, inadequate food safety laws, weak regulatory systems, lack of financial resources to invest in safer equipment, and lack of food safety training are common.2,4
The term “street foods” refers to a wide variety of plant and animal origins, such as green papaya salad, fried biscuit, stir-fried rice noodle, fried egg, juices, macaroni, salad, tomato stew, and sandwich are commonly sold. They are sometimes prepared in areas with busy economic activities and heavy movement of people such as transportation centers, schools, parks, market area, theaters, and other similar business centers.5–7 The consumption of these foods is common in many countries,8,9 where unemployment is high, salaries are low, and work opportunities and social programs are limited.3,10 The safety of street foods, on the other hand, becomes the major source of concern for food control officers. 7
Individuals who are asymptomatic can equally be the source since enteric microorganisms found in all warm-blooded animals.4,11 Contaminated fingernails play a great role in transporting pathogens from the source to the food items and then from the food to the body. 12 The most common pathogenic bacteria implicated in foodborne infections include Salmonella, Shigella, Escherichia coli, Listeria, Campylobacter species, Enterobacter spp., and enterotoxigenic Staphylococcus aureus.13,14 Infections associated with Salmonella and Shigella are among the major public health problems in tropical and subtropical regions of the world. In Ethiopia, the carriage rate of Salmonella among food handlers ranges from 0.9% to 6.9%,15,16 whereas that of Shigella ranges from 0% to 5.9%.17,18
Nowadays, increasing resistance to commonly used antimicrobial agents by Salmonella and Shigella is a challenge to modern medicine and has far-reaching implications as an emerging public health problem with huge risk to global health security.19,20 The emergence of resistance to most frequently prescribed antimicrobial agents in bacteria is mediated by the target drug modification, changes in bacterial cell permeability and, most importantly, the production of hydrolysing enzymes, namely β-lactamases.19,21 The use of drugs without genuine prescription, self-medication, and misuse are also suggested to augment the emergence of antimicrobial resistance. 22 The consequences may be felt hardest in resource-limited settings because second-line antimicrobials for resistant bacteria may be unavailable or unaffordable.23,24
Several studies have been conducted on salmonellosis and shigellosis in Ethiopia. Most of these are restricted to health facilities, food handlers working in universities, cafeterias, restaurants, or hotels with or without antimicrobial susceptibility testing.6,14,18,25 There is limited information about Salmonella and Shigella among street food vendors. This study was conducted to determine the prevalence, antimicrobial susceptibility pattern, and associated factors of Salmonella and Shigella among asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia.
Methods
Study setting and period
The study was conducted among street food vendors in the Dire Dawa city, Eastern Ethiopia from May 2017 to July 2017. The Dire Dawa city is located at a distance of 510 km from Addis Ababa, Ethiopia. It has 9 Kebeles (small administrative units) and a total of 453 000 populations. Currently, there is a total of 560 registered street food vending in the city (source: Dire Dawa Administration Health Bureau, 2016).
Study design
A community-based cross-sectional study was conducted among asymptomatic street food vendors in the Dire Dawa city, Ethiopia.
Source population
All individuals working in a street food vendor in the Dire Dawa city were the source population.
Study population and eligibility criteria
All food vendors working in registered street food vending without current clinical symptoms of salmonellosis or shigellosis such as gastroenteritis, diarrhea, fever, vomiting, and abdominal cramp and age ⩾ 18 years were included in the study. Those who had taken antimicrobial treatment two weeks prior and during data collection were excluded from the study.
Sample size determination
The sample size was determined using a single-population proportion formula with the assumptions of 1.96 standard normal deviations at 95% confidence interval (CI), 5% margin of error, and 10.5% proportion of Salmonella among street food vendors in Nigeria. 26 The calculated sample size was 201. The sample size was further increased to 221 taking into account a 10% non-response rate.
Sampling technique
A comprehensive list of existing street food vendors along with the number of individuals involved in food processing and handling was obtained from the Dire Dawa Health Bureau. The selection of the study participants was performed using a simple random sampling technique (lottery method).
Data and sample collection
Data related to the sociodemographic profile of the participants and associated factors were collected using a pretested questionnaire adapted from different kinds of literature.18,27–29 The questionnaire included information on sex, age, educational status, income, and personal hygiene among others. Five data collectors (3 professional nurses, 1 laboratory technician, and 1 medical microbiologist) were recruited. Data were collected through face-to-face interviews. After proper instruction, each study participant was asked to bring 2 g of stool specimen in clean, dry, leakproof disposable stool cups. Approximately, 1 g of stool was immediately transferred into the Cary Blair transporting medium (Oxoid, Ltd, Basingstoke, UK), labeled, and transported within 30 minutes of collection in ice-packed cold box (4°C) to the Dire Dawa Regional Health Research Laboratory for bacterial identification.
Culture and identification
The isolation and characterization of Salmonella and Shigella spp. were performed based on the standard procedure described by Cheesbrough, 30 with some modifications. Briefly, a mixture of a stool sample (1 mL) was transferred from the Cary Blair medium into a tube containing 9 mL of Selenite F broth (Oxoid, Ltd) and incubated at 37°C for 24 hours to enrich the bacteria. An inoculum from Selenite F broth was subcultured onto deoxycholate agar (DCA) and xylose lysine deoxycholate (XLD) agar (Oxoid, Ltd). After overnight incubation at 37°C the growth of Salmonella and Shigella was differentiated by their colony characteristic appearance on XLD agar (Shigella: red colonies, Salmonella red with a black center) and DCA (Shigella: pale colonies, Salmonella black center pale colonies). Further identification was done biochemically using analytical profile index 20E (API 20E; bioMérieux SA, France) and Gram stain. Pure colonies with or without black centered on DCA or XLD was picked and suspended in sterile normal saline (0.85% NaCl). API 20E microtubes were filled up to the edge with the suspension. Sterile oil was added into the arginine dihydrolase, lysine decarboxylase, ornithine decarboxylase, hydrogen sulfide, and urease production test compartments to create anaerobiosis. Reading of the result was done as per the manufacturer’s instruction after overnight incubation at 37°C.
Antimicrobial susceptibility testing
Antimicrobial susceptibility tests were performed on the Mueller-Hinton agar (Oxoid, Ltd) using the Kirby-Bauer disk diffusion method as described by the Clinical and Laboratory Standards Institute (CLSI). 31 Three to five pure colonies were picked with a sterile loop and mixed with sterile normal saline (0.85% NaCl) to prepare a uniform suspension equivalent to 0.5 McFarland standards. The suspension was uniformly spread onto a Mueller-Hinton agar plate using a sterile cotton swab. The plate was left at room temperature for 3 to 5 minutes to dry. The antimicrobial disks (Oxoid, Ltd) tested were ampicillin (10 μg), amoxicillin (10 μg), chloramphenicol (30 μg), ceftriaxone (30 μg), ciprofloxacin (5 μg), gentamicin (10 μg), nalidixic acid (30 μg), sulfamethoxazole-trimethoprim (23.75/1.25 µg), and tetracycline (30 μg). After incubating the plates at 37°C for 24 hours, the zone of inhibition including the disks was measured using a digital caliper to the nearest whole millimeters and interpreted as sensitive, intermediate, or resistant based on CLSI 31 interpretive breakpoints. Multidrug resistance (MDR) was defined as simultaneous resistance of the isolates to 2 or more classes of antimicrobial agents. 32
Data quality control
Initially, an English version of the questionnaire was developed. It was translated for actual data collection into local languages (Amharic, Afan Oromo, and Somali) by language experts and back to English by other experts. The reliability of each version questionnaire was checked on 22 street food vendors in Harar town, Eastern Ethiopia. Stool specimens were collected aseptically and transported under recommended conditions. The preparation of each used medium was made according to the manufacturer’s instruction. The sterility of each medium was checked by incubating overnight at 37°C. Media with any growth were discarded. Reference bacterial strains such as E coli (ATCC 25922), S aureus (ATCC 29213), Shigella flexneri (ATCC 12022), and Salmonella typhimurium (ATCC 14028) were used for media and antimicrobial performance check. All internal quality control testing values fell within the reference ranges. The collected data were checked and verified by the research team.
Data analysis
Data were coded, verified, and entered into EpiData version 3.1 (EpiData Association, Odense, Denmark) and exported to the Statistical Package for the Social Sciences (SPSS) version 25.0 (SPSS Inc, Chicago, IL, USA) for analysis. Data were described using descriptive statistical tools such as frequency, percent, mean, and standard deviation. The association between independent variables and the outcome variable was assessed using the bivariate and multivariate logistic regression models. A variable with a P-value < .25 in the bivariate analysis was further analyzed using the multivariate logistic regression. A P-value ⩽ .05 in the multivariate logistic regression analysis with 95% CI was considered statistically significant.
Results
Sociodemographic characteristics
Of 221 food vendors, 218 were participated in this study, making a response rate of 98.6%. The mean age of the study participants was 34.9 (±5.9 standard deviation) years. Among the respondents, 97.7% were female. Most of the respondents were married (56%). Almost half (48.6%) of the respondents were attended primary cycle education. More than half (65.6%) of the participants earned an average monthly income of 43.7 to 87.3 USD (Table 1).
Sociodemographic characteristics of asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia (n = 218), 2017.

Prevalence and associated factors
Of the total stool specimens examined (218), Salmonella and Shigella were recovered from 19 specimens, providing the overall prevalence of 8.7% (95% CI: 5.6, 10.3). Most of the isolates were Salmonella 13 (6%) (95% CI: 4.1, 9.8), followed by Shigella organisms 6 (2.8%) (95% CI: 1.3, 4.5). The highest prevalence of Salmonella and Shigella was recovered from those who did not wash hands after the use of toilet with soap (15.2%), those with untrimmed fingernails (13.3%), and primary cycle educated group (13.2%). In the bivariate logistic regression analysis, the odds of Salmonella and Shigella were high among food vendors who had a primary cycle education, lack of hand washing habit after the use of the toilet with soap, lack of hand washing before food preparation and handling, and those with untrimmed fingernails. However, in multivariate analysis, the odds of Salmonella and Shigella remain higher only among those who did not wash hands with soap after the use of the toilet (adjusted odds ratio [AOR]: 3.3, 95% CI: 1.2, 7.9) and those with untrimmed fingernails (AOR: 4.4, 95% CI: 1.5, 9.3) than their counterparts (Table 2).
Factors associated with Salmonella and Shigella infections among asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia (n = 218), 2017.

Abbreviations: AOR, adjusted odds ratio; CI, confidence interval; COR, crude odds ratio.
Significant at P-value < .25; **significant at P-value ⩽ .05.
Antimicrobial susceptibility pattern of the isolates
Among all antimicrobials tested against the isolates, the higher phenotypic resistance was observed to amoxicillin (97.7%), ampicillin (89.5%), and tetracycline (68.4%). Higher sensitivity was observed to ceftriaxone (100%), ciprofloxacin (89.5%), gentamicin (84.2%), nalidixic acid (73.7%), and sulfamethoxazole-trimethoprim (68.4%). The higher level of resistance was observed to amoxicillin (92.3%), ampicillin (92.3%), and tetracycline (76.9%) by Salmonella isolates, and amoxicillin (100%), ampicillin (83.3%), and chloramphenicol (66.7%) by Shigella isolates. On the other hand, 100% sensitivity was detected in each of ceftriaxone and ciprofloxacin, 76.9% to each of chloramphenicol, gentamicin, and nalidixic acid by Salmonella isolates, and 100% sensitive to each of ceftriaxone and gentamicin, 66.7% to each of ciprofloxacin and nalidixic acid, and 66.6% to sulfamethoxazole-trimethoprim by Shigella isolates (Table 3).
Antimicrobial susceptibility pattern of Salmonella and Shigella isolates among asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia, 2017.

Abbreviations: AM, ampicillin; AMX, amoxicillin; C, chloramphenicol; CIP, ciprofloxacin; CN, gentamicin; CRO, ceftriaxone; I, intermediate; NA, nalidixic acid; R, resistance; S, sensitive; SXT, sulfamethoxazole-trimethoprim; TE, tetracycline.
MDR pattern of the isolates
The overall prevalence of MDR (resistance to ⩾2 classes of antimicrobial agents) Salmonella and Shigella isolates were (57.9%). The most frequent MDR was observed in Salmonella isolates (47.4%). The frequent resistance was seen to ampicillin, amoxicillin, and tetracycline (36.4%), followed by ampicillin, amoxicillin, and sulfamethoxazole-trimethoprim (27.2%) (Table 4).
Multidrug resistance pattern of Salmonella and Shigella isolates identified from asymptomatic street food vendors in the Dire Dawa city, Eastern Ethiopia, 2017.
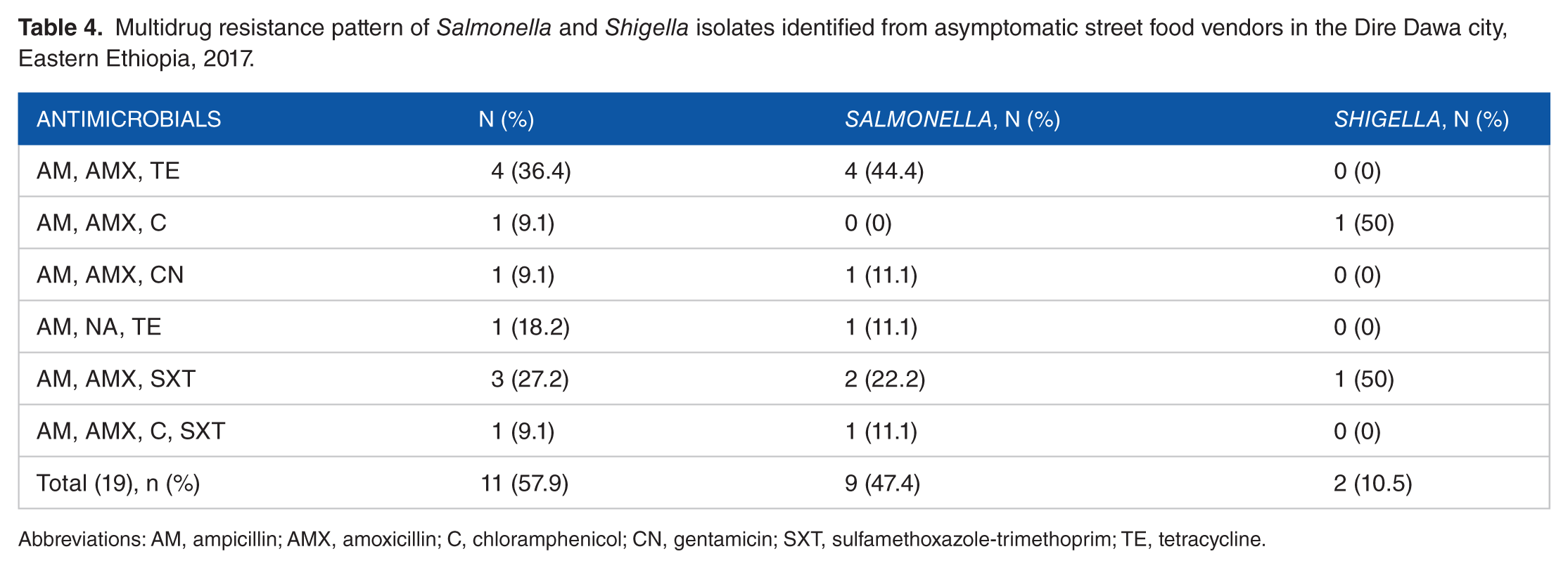
Abbreviations: AM, ampicillin; AMX, amoxicillin; C, chloramphenicol; CN, gentamicin; SXT, sulfamethoxazole-trimethoprim; TE, tetracycline.
Discussion
Salmonellosis and shigellosis continue to be an important cause of morbidity and mortality worldwide.5,9,29 The transmission mainly occurs via the food chain (from fingers to food, and finally to the consumers) largely due to the poor health status of the food vendors, their personal hygiene, knowledge, and practice.18,33 In addition, poor food handling and sanitation practices, inadequate food safety laws, and weak regulatory systems contribute to the spread of foodborne pathogens.2,3
In this study, the overall prevalence of Salmonella and Shigella was 8.7% (95% CI: 5.6, 10.3). This was much lower compared with the previous study conducted in Jubail, Saudi Arabia (89.7%) 34 and Abuja, Nigeria (57.8%). 26 The carriage rate of Salmonella (6%) (95% CI: 4.1, 9.8) was comparable with the study conducted in Arba Minch, Ethiopia (6.9%). 16 It was relatively higher than reports from different parts of Ethiopia such as in Haramaya (3.6%), 14 Jimma (2.7%), 28 and Dilla (0.9%) 15 and African countries like Omdurman, Sudan (3.8%), 35 and Kumasi, Ghana (2.3%). 29 However, it was lower than the study findings in Kaduna, Nigeria (42.3%), 26 Tamil Nadu, India (17.14%), 36 and Lagos, Nigeria (17%). 37 The variation in the magnitude among the studies might be attributed to the difference in educational level, hand washing practices, personal hygiene, and awareness of food vendors on hygienic food preparation and handling.
Shigella has substantial public health threat because few cells of organisms (10-100 bacilli) are enough to elicit bacillary dysentery that may lead to shigellosis outbreaks. 38 In this study, the prevalence of Shigella isolates was 2.8% (95% CI: 1.3, 4.5). This was in agreement with the study conducted in Haramaya, Ethiopia (1.4%), 14 but it was lower than those in reports from Abuja, Nigeria (15.5%) 26 and Debre Markos, Ethiopia (5.9%). 18 The isolation of a higher rate of Shigella emphasized the need for close supervision of food vendors at the workplace because asymptomatic carriers significantly contributed to the spread of various pathogens,4,27 which might have a significant impact on public health in the community.
Plasmid-encoded resistance to ampicillin and chloramphenicol and chromosome-encoded resistance to nalidixic acid and ciprofloxacin have been reported.19,36 In this study, a higher rate of resistance to amoxicillin (97.7%), ampicillin (89.5%), and tetracycline (68.4%) by Salmonella and Shigella was observed. Overuse and misuse of antimicrobials in both humans and animals for the treatment of various diseases and inadequate surveillance coupled with the rapid spread of resistant bacteria contributed to the problem.22,39 The finding was in line with the study conducted elsewhere.10,14 However, the sensitivity to ceftriaxone (100%), ciprofloxacin (89.5%), gentamicin (84.2%), and nalidixic acid (73.7%) was high, and hence they are the drugs of choice for the treatment of salmonellosis and shigellosis. If the clinician considered these antimicrobials when prescribing, the positive outcome may be higher and the emergence of resistance can be minimized. Public health measures such as improving personal and food hygiene, intensive health education, and effective and commendably connected surveillance programs at a multidisciplinary level could also mitigate the emergence of antimicrobial resistance.24,40
Currently, the increasing prevalence of MDR among Salmonella to clinically important antimicrobial agents has been an emerging problem. 10 The higher rate of MDR observed by Salmonella isolates (47.4%) in this study contributes to the increment of untreatable Salmonella in the community. Infections caused by MDR strains also with no doubt result in higher morbidity and mortality as antimicrobials for resistant bacteria may be scarce or unaffordable.23,24 The finding was relatively in line with the study conducted in Sudan (47.1%), 41 but it was lower than the study reports from Haramaya, Ethiopia (88.9%) 14 and Tamil Nadu, India (83.3%). 36 The enormity of higher MDR observed to ampicillin, amoxicillin, and tetracycline that is most frequently prescribed for Salmonella and Shigella treatment in our country is another concern. Clinicians may force to remove these antimicrobials from the treatment modality. There is a need to strengthen infection prevention measures, monitor utilization of drugs, and expand surveillance of resistant Salmonella and Shigella strains.
Many factors may contribute to the differences in the prevalence of Salmonella and Shigella at different times, places, and conditions. Poor personal hygiene and environmental sanitation are known to potentiate the transmission of Salmonella and Shigella strains in many developing countries.4,27,29 In this study, the odds of Salmonella and Shigella was higher among food vendors who did not wash hands after the toilet visits with soap than those who did. The finding was in agreement with other similar studies.28,37 The odds of Salmonella and Shigella was also higher among food vendors who did not trim fingernails. The finding was supported by other studies conducted elsewhere.7,14,16 Given the time and money required to advance environmental sanitation and personal hygiene, the most valuable option to ensure the health safety is health education and regular screening of food vendors with a view to treating those found infected with sensitive antimicrobials until they are cured.
This study has at least 3 limitations. First, there might be contamination in a small number during the culture process. Second, fingernail contents and food samples that could help increase the probability of determining the true point prevalence of Salmonella and Shigella were not considered. Third, characterization of the isolates to species level was not possible due to lack of serological tests, but it is believed that the culture and biochemical used was sufficient for identification to the genus level. In spite of these limitations, the information generated from this study has been considered valuable as combined epidemiological and various microbiological techniques were used to determine the prevalence, antimicrobial susceptibility pattern, and associated factors of Salmonella and Shigella infections.
Conclusions
In conclusion, the overall prevalence of Salmonella and Shigella was relatively lower compared with other similar studies. Most isolates were resistant to ampicillin, amoxicillin, and tetracycline. Treatment of asymptomatic carrier requires further knowledge of the antimicrobial susceptibility pattern in the study setting. The odds of the carriage were high among food vendors who did not wash their hands with soap after the use of the toilet and had untrimmed fingernails. Periodic health screening, ensuring compulsory treatment, and guidance on personnel and workplace hygiene may result in the decrease of Salmonella and Shigella infections. Further in-depth epidemiological studies on a large sample size by incorporating fingernail contents and food specimens are essential to optimize the health of food vendors.
Footnotes
Acknowledgements
We would like to thank the Institutional Health Research Ethics Review Committee of the College of Health and Medical Sciences, Haramaya University for providing ethical clearance. Our gratitude also extends to the Dire Dawa Health Research Regional Laboratory for material support and the study participants for their kind cooperation.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection was financially and materially supported by the Health Bureau and Health Research Regional Laboratory of the Dire Dawa City Administration.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
GT conceived and designed the study. GT, HM, ZT, and DM were involved in the study design, data analysis, and interpretation of the findings, wrote the manuscript, made critical revisions, and reviewed and approved the final manuscript.
Ethical Approval
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee (IHRERC) of the College of Health and Medical Sciences, Haramaya University (Approval No. IHRERC 156/2017). Study permission was also secured from the Dire Dawa City Administration Health Bureau.
Informed Consent
Informed, voluntary, written and signed consent was obtained from each participant prior to data and sample collection. Those who were positive for Salmonella or Shigella were referred to the nearest health facility for appropriate treatment of the infection.