
Abstract
Education of health and social care professionals is essential in preparation to confidently and effectively support families affected by dementia to undertake advance care planning. This article describes a training needs analysis of Admiral Nurses, dementia specialists, in facilitating advance care planning for future care.
Methods:
A questionnaire survey was completed by Admiral Nurses attending end-of-life care masterclasses in 2017 and 2018. Both quantitative (years registered as a nurse, years as an Admiral Nurse and subjective level of confidence in completing advance care plannings) and qualitative data (interventions perceived to increase confidence) were collected.
Findings:
There were 75 completed responses (two incomplete returns). There was no correlation between levels of confidence and years registered as a nurse. However, there was a small positive correlation between confidence and number of years as an Admiral Nurse (r = 0.23; p < 0.05). Themes identified qualitatively to enhance practice were advanced communication skills, supervised practice, resources to frame conversations and a guide and template for advance care planning.
Conclusion:
Although Admiral Nurses are specialists in dementia, several educational initiatives could be employed to better enable them to support advance care planning for families affected by dementia. This training needs analysis is contributed towards developing an educational intervention for Admiral Nurses to improve advance care planning support.
Introduction
Advance care planning
Caring for people who are at the end of life is an important role for many health and social care professionals. One of the aspects of this role is to discuss with individuals their preferences regarding the type of care they would wish to receive and where they wish to be cared for, if they lost capacity and were unable to express a preference in the future. In the condition of dementia, loss of capacity is inevitable at some stage of the illness; sometimes, this may happen early in the illness making the offer and support of advance care planning (ACP) as soon as possible after diagnosis essential to planning ahead. 1
Conversations around prognosis, palliative care and end of life can be challenging for the professional, the person with dementia and their families, but are important for improving patient experience. 2 Such open conversations are often welcomed by the patient or their family as a chance to gain more information about their prognosis and treatment options and to exercise some choice and preference. 3 , 4 This is not the case for every patient; for some patients and their families, not talking about death and ‘not giving up’ is how they want to approach life, even at the end. 5 However, they should be given the opportunity to have a conversation. 2 A human rights approach suggests that every effort should be made to ascertain a person’s wishes and preferences at any stage of dementia. 6
Many health and social care professionals find discussions about planning for end-of-life care difficult to initiate with a person with dementia;7–9 similarly, many often see this as the responsibility of another member of the multidisciplinary team; 10 consequently, in the United Kingdom, there is no standardised or clear pathway that details when, how and by whom ACP discussions are initiated and reviewed. However, it is important that from the outset, there is informed communication within the family about the diagnosis of dementia, its course and prognosis and planning for future care while the person with dementia has the capacity to do so. The reticence to initiate such conversations is multifactorial involving a lack of confidence, lack of knowledge or lack of skills.10–12 Professionals can overcome such barriers to initiating these conversations through receiving targeted education, practice and reflection on experiences in preparing them to confidently and effectively support families affected by dementia and to facilitate complex interventions such as ACP. 13
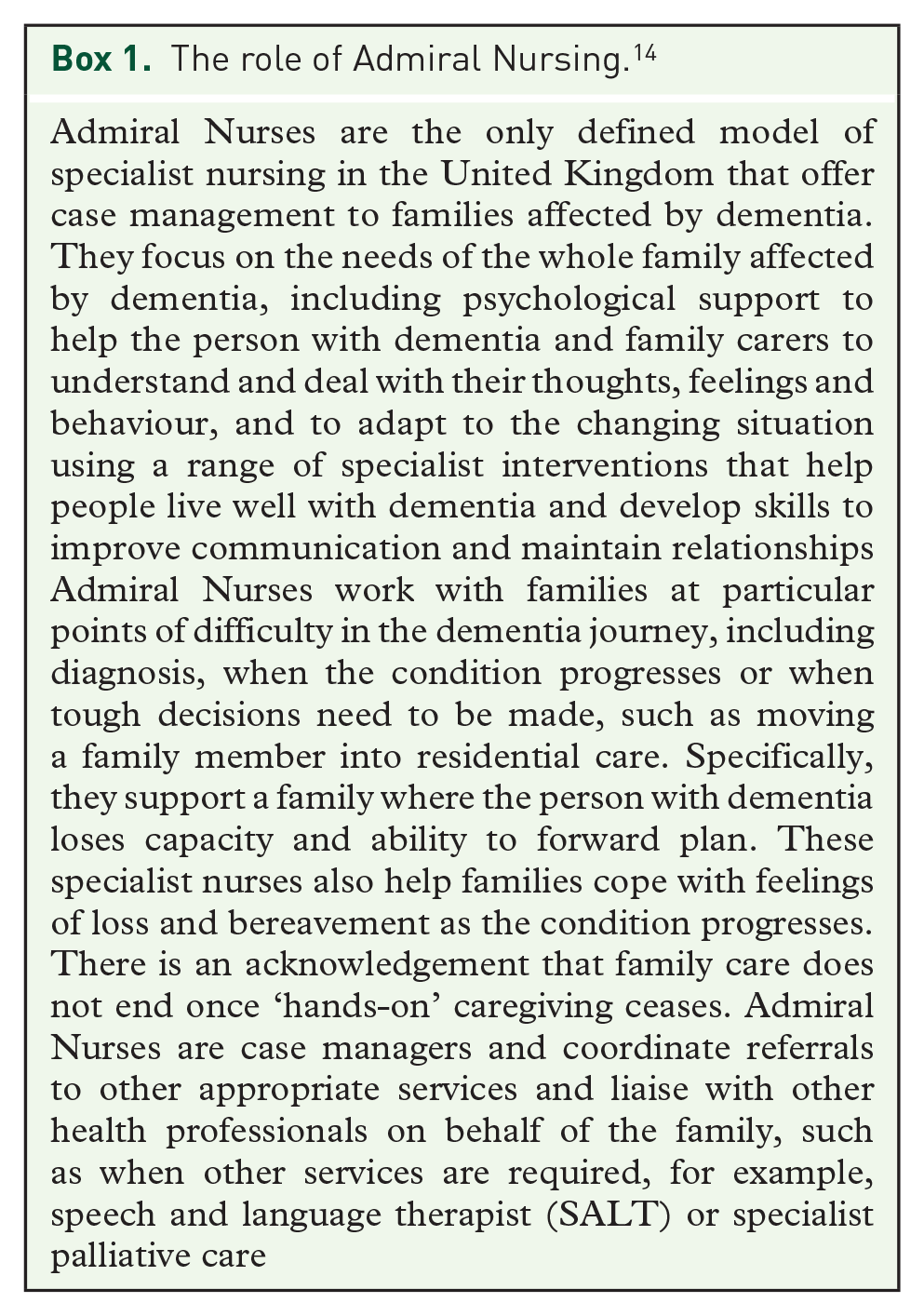
This article describes a training needs analysis (TNA) undertaken by the Professional and Practice Development Team of Dementia UK (the charity that is the ‘home’ of Admiral Nursing, www.dementiauk.org) in preparing a programme of education to support Admiral Nurses (see Box 1 and https://www.dementiauk.org/for-professionals/what-do-admiral-nurses-do/) in their facilitation of an ACP intervention as currently there is no standardised educational approach to the development of Admiral Nurses skills in undertaking ACP or difficult conversations. In designing a programme, we also explored current levels of confidence as well as the nurses perceived educational needs to better facilitate ACP discussions in their everyday practice.
There has been no consistent training approach for Admiral Nurses in initiating ACP conversations. In 2010, an early master class focusing on ACP in dementia was piloted with a group of 10 Admiral Nurses. 15 However, the main policy thrust at this time was in living well with dementia 16 with only a small, but growing, interest in also dying well with dementia and the possibility in planning for an end of life that ACP could offer this group of people. There has since been a sporadic and inconsistent approach to the intervention of ACP across Admiral Nursing until the recent user-centred design methodology to develop the Dementia UK ACP guide and template, 17 thus requiring a robust approach to education of nurses to aid its implementation.
The role of Admiral Nursing. 14
Training needs analysis
A TNA is essential in establishing the continuing processional development of a health care workforce 18 and is a well-established process in organisational development that seeks to identify the gap between the knowledge and skills of an individual or organisation and the need for training.
Training is described as the acquisition of skills, concepts or attitudes that result in improved performance within the work environment. 18 , 19 TNA examines an operational domain (in this case ACP) so that the initial skills, concepts and attitudes of the human elements of a system can be effectively identified and appropriate training can be specified. 19
A TNA is the first stage in a cyclical process (see Figure 1) that will identify a training need and what training will address the need(s).19–21 There are three reasons why one might undertake a TNA: to meet an individual’s learning needs (as in personal professional development), in preparation for the introduction of new system task or technology (such as the introduction of a new intervention) or a desire for organisational benefit (such as preparation for the implementation of a new policy).

The cyclical process of identifying and responding to training needs.
Identify educational needs
The TNA process helps the trainer and the person requesting training to specify the training need or performance deficiency. Assessments may be formal (using survey and interview techniques) or informal (asking some questions of those involved). 22 Often training is provided based upon what an organisation requires of their workforce or may be guided by external drivers, such as national surveys or curriculum, policy or outcomes from enquiries into poor practice cases.
The TNA in the context of this article was conducted to explore the knowledge, skills and levels of existing confidence that enable Admiral Nurses to facilitate ACP with families affected by dementia. Admiral Nurses demonstrate various competencies that relate to their specialist role and at three levels of increasing expertise; advanced, specialist and expert as detailed in the Admiral Nurse Competency Framework (ANCF). 23 However, the competency domains of the ANCF are broad and provide overarching headings to describe practice. To prepare for the implementation of the ACP intervention, Dementia UK wanted to be more exact in identifying the specific competencies required to support ACP. Usually, a TNA will seek to find the difference between the expected and actual levels as a performance gap; however, Dementia UK in launching their bespoke ACP guide and template wanted to ensure that its implementation was better enabled through all participating Admiral Nurses receiving targeted training and development and to the same level. Therefore, it was important to understand both the subjective educational needs of individual Admiral Nurses and also the requirements in fulfilling the project implementation objectives.
Method
The TNA was conducted during five master classes focusing on end-of-life care in dementia with Admiral Nurses across the United Kingdom held between 2017 and 2018. The master classes delivered a 1-day educational event that focused on the palliative and end-of-life care needs of people with dementia and issues for their family carers. The learning outcomes included recognition of good practice and potential barriers in end-of-life care; an exploration of the experience of end-of-life care for the person living with dementia and their families and an appreciation of collaborative working. The master classes were commissioned from the Association of Dementia Studies, University of Worcester by Dementia UK. While bringing together the Admiral Nurses to explore palliative and end-of-life care, it was an appropriate and opportune time to undertake the TNA survey (see Box 2).
Advance Care Planning Conversations survey.

Statistical analysis
The information collected from the participants consisted of their perceived confidence of undertaking ACP discussions with families on a scale of 1–10 (1 corresponding to low confidence and 10 to high confidence); whether or not they had facilitated ACP processes before (as a Yes or No response); the number of years registered as a nurse and the number of years practising as an Admiral Nurse. The last two items were collected as ‘0–5 years’, ‘6–10 years’, ‘11–15 years’ and so on; they were recoded to mid-point values for the summary and analysis.
Qualitative analysis
A qualitative approach was taken to the data taken from the final section of the survey that invited free text comments on what participants felt would increase their confidence; this drew upon a naturalistic interpretive approach. 24 , 25 Free text data from the final section of the survey were sorted and themed; such content analysis is a useful approach to examining data within a given context and in the triangulation of data collected through mixed research methods. 25
Findings
A total of 93 nurses attended the palliative and End-of-Life Care National Master Classes held across the United Kingdom and were invited to complete the ACP survey. There was an 83% response rate (n = 77) of which two were removed due to incomplete information. Of the 75 valid responses, the median value of the confidence indicator was 8% and 85% of the responses were between 6 and 9 on the scale, inclusive. The mean number of years registered as a nurse was 20.6 and the mean number of years registered as an Admiral Nurse was 4.8, with 79% of the respondents having ‘0 to 5’ years in this role.
There was no correlation (using Pearson’s r) between the level of confidence and the number of years registered as a nurse. However, correlation between confidence and the number of years as an Admiral Nurse did show a low but significant positive association (r = 0.23, p < 0.05). The mean confidence score for those who had completed an ACP was 7.66 and the mean for those who had not was 6.37; the difference is significant with p < 0.05 on a two-tailed t test.
Summarising the results as a simple linear model, deriving confidence score as a function of ACP/no ACP experience and years as an Admiral Nurse yields:
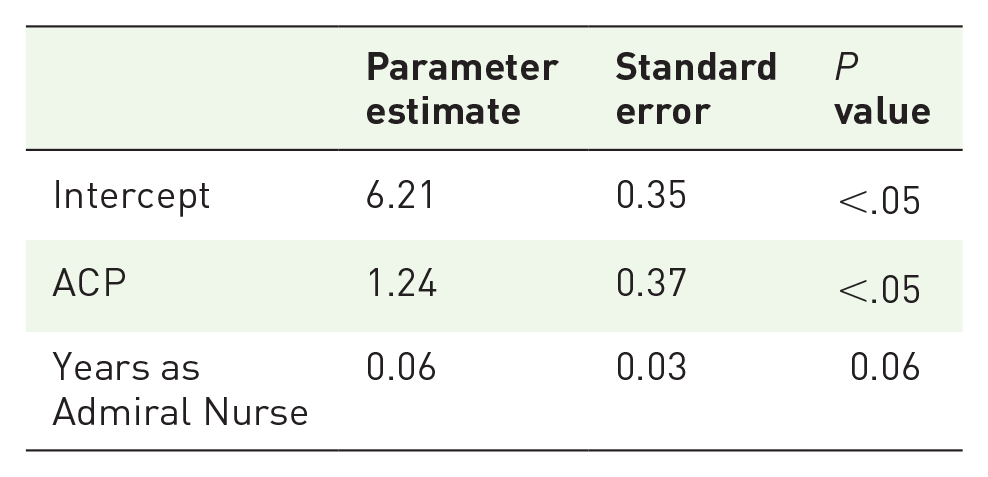
The adjusted R2 (the variance accounted for by the model) is 15.6%. Hence, we suggest that this overall picture supports the notion that ACP experience is a small but significant contributor to confidence levels, although clearly there are other factors that influence the confidence measure which may include factors not examined here and the inherent difficulty of measuring that attribute accurately.
The nurses were finally asked to consider, in a free text response, what specific educational interventions, materials or activities would enhance their confidence to aid their facilitation and practice in ACP. All respondents added free text comments. Four main themes arose from the qualitative data, which were; a need for more practice in ACP, having specific tools and templates for ACP available to them, resources and aids to initiating ACP conversations and being supported to develop greater confidence to initiate ACP conversations. The nurses felt that having more supervised practice of ACP in role was the most significant intervention that would enhance their ability to undertake end-of-life care conversations with 25% (n = 19) of the nurses proposing this approach.
Discussion
Analysis of the TNA responses indicated several areas of concern and identified educational needs of the Admiral Nurses. These were themed according to the strength of their responses and are discussed accordingly; education that would increase their confidence to initiate and undertake ACP discussions, having supervised practice and shadowing the practice of others, and various resources that could be deployed during the process.
Confidence in holding the conversation
The literature reveals that professionals often lack the confidence and the skills in breaking bad news and in initiating the process of ACP with sensitivity and empathy.2,10,11,12,26 In this TNA, the nurses reflected fairly high levels of confidence in initiating ACP discussions with families affected by dementia. As with many other professionals, Admiral Nurses do not have formal training or supervision to support undertaking difficult conversations. Their responses indicated a perceived need to standardise education for all Admiral Nurses and for peer support and reflection on practice. Just over half of the respondents had not yet facilitated an ACP intervention, although many seemed to anticipate high confidence in doing so in the future. However, 22% (n = 17) did not provide a response to this question. This accounted for over one-third of the sample. There may be several reasons for this, such as, a reluctance to admit to a lack of confidence as they may feel it as fundamental to their role. Interestingly, the role of the Admiral Nurse can involve many difficult conversations related to dementia, such as diagnosis, prognosis, behaviours that are distressing; Admiral Nurses are generally confident in initiating and managing these sorts of interactions. It may be that the above topics are often generated or raised by family members, whereas discussions about ACP for end-of-life care require the Admiral Nurse to raise the issue when family members are reluctant to do so. 27 , 28
Practice in role
A quarter, 25% (n = 19) of the nurses believed that having more (and supervised) practice holding ACP conversations would be helpful with some adding that the opportunity to shadow other nurses undertaking ACP conversations could be part of this. Modelling how to initiate and manage ACP discussions 29 , 30 could be one educational offer to the nurses but there may be steps that could be taken to develop the nurses’ confidence and skills, before such practice was undertaken, such as a practice placement with a hospice ACP team.
In dementia care, building a therapeutic relationship with all those in any given case is central to the role of the Admiral Nurse, and expert communication skills are essential in situations that involve discussions around diagnosis, prognosis and a family’s concerns and feelings. There are educational interventions that can specifically target and increase a professional’s confidence in delivering such interventions, such as Advanced Communication Skills Training (ACST) courses.31–33 Breaking bad news and discussing ACPs and shared decision-making have been a traditional focus of ACST in cancer care. 34 , 35 The overriding aim of the ACST course is to develop the confidence of the practitioner in initiating and managing difficult conversations, such as delivering the diagnosis of a life-limiting condition or supporting ACP. Such training has traditionally focused on communication between health care professionals and patients diagnosed with cancer during their formal assessment interview and include emphasis on skills for building a relationship, providing structure to the interview, initiating the session, gathering information, explaining, planning future care and closure of the interview. 36 Most approaches to teaching communication in health care incorporate cognitive, affective and behavioural components, with the general aim of promoting greater self-awareness. 37
There is a place for the simulation of scenarios in a safe, classroom setting that would allow the Admiral Nurses to test out certain conversation plans or use of materials. Several studies have demonstrated the value to using a defined communication model within the framework of simulation training.38–40 Simulation training is commonly used in undergraduate end-of-life care education for nurses and other disciplines 41 , 42 as it is considered more effective than classroom teaching alone for professional training in addressing complex areas of care and emotionally charged clinical scenarios. 41 , 43 , 44 Simulation training is an educational process that has long been in use in medical student training through the use of Objective Structured Clinical Examinations (OSCEs); simulated scenarios using actors and assessment of the practice of a trainee by qualified doctors. 45 There is also some evidence supporting the use of simulation training in improving confidence in ACP for doctors 30 and nurses and social workers. 46 Simulation is a relatively new concept in nurse education and comprises the physical re-enactment of connected components of care and is of particular value in increasing confidence and skills before exposure to live patient practice.
Education in practice
In a randomised controlled trial involving 61 clinical nurse specialists who attended an ACST workshop, Heaven and colleagues 38 found that clinical supervision or action learning sets were of significant value in supporting them to take ‘theory into practice’. They randomised half of the participants to a follow-up of 4 weeks of clinical supervision, aimed at facilitating the transfer of their newly acquired knowledge and skills into practice, with the controls having no follow-up. Assessment of their practice was carried out before the course, immediately after the supervision period of 4 weeks and then 3 months later. Performance was measured, using the Medical Interview Aural Rating Scale (MIARS) 47 to assess the nurses’ ability to use key skills, respond to patient cues and identify patient concerns. Comparing both groups performances, the study demonstrated that while training enhances skills, without the follow-up clinical supervision, it may have little effect on their clinical practice.
The Admiral Nurses all attend monthly peer group clinical supervision; 48 however, it may be more appropriate to use focused action learning sets to provide dedicated support to take the theoretical knowledge and skills gained in ACST fully into practice and maximise the opportunity to facilitate ACP.
Models of communication
In the TNA, the nurses identified several resources that they perceived would be beneficial in enhancing and developing their practice such as materials to support communication. Good, effective communication is essential in enabling ACP for people with dementia. Communication is a two-way process but in people with dementia their ability to communicate with others (expressive aphasia) and to receive the communication of others (receptive aphasia) becomes increasingly difficult as the condition progresses. The Admiral Nurses are very experienced in holding difficult conversations with families at various points, such as diagnosis, when behaviours challenge, moving into residential care. They use different approaches and models according to the person and the situation; however, there has been no consistent approach to education in respect of this to date. Several models of communication – sometimes referred to as cognitive maps 49 – have been developed to support the initiation of these difficult discussions (e.g. see Box 3).
Communication models.

As Russell 52 argues, one size does not fit all; either from the perspective of the patient or indeed that of the professional. However, such models have a formulaic approach that includes preparation, person-centeredness, empathy and acknowledgement of emotions and concerns and in eliciting individuals’ wishes and preferences. 51
Models of communication can provide a framework within which professionals can ensure their conversations will have a flow that is clear, satisfactory in respect of ensuring a completeness, promote quality outcomes and provide a sense of safety as the professional tests out their skills and resource materials to effect ACP.
Conversation prompts for families
Twenty percentage (n = 17) of the respondents felt that various facilitative materials such as conversation prompt cards, guides/booklets and ACP templates would make a difference in enabling them to initiate and sustain difficult conversations. In 2009, the National Council for Palliative Care (NCPC) set up the Dying Matters Coalition (DMC) 53 to promote public awareness of dying, death and bereavement. Changes in the way society views dying and death have impacted on the experience of people who are dying and bereaved. The coalition’s mission was to help people to talk more openly about dying, death and bereavement, and to make plans for the end of life. The DMC premise was that lack of openness about death and dying may have affected willingness to engage with and take more control in planning end-of-life care. Such initiatives acknowledge that the general population find it difficult to consider what these conversations might include as well as how to initiate them with health care professionals. Professionals may also be in a similar position and find it difficult to not only contemplate their own death and dying yet are expected to support their patients to do so.
Several organisations have developed resources aimed to help the lay public to consider the important issues they may need to think about when planning for end of life. However, these resources can also support health care professionals to start conversations and use as conversation prompts. There are many conversation aids, such as prompt cards, card games, picture cards, to help patients and families consider what is important to them at the end of life (see Box 4).
Conversation prompt resources.

However, there is still a lack of research to demonstrate the benefit and outcomes to using such communication aids. Peterson and colleagues 54 used focus groups with 36 older community-dwelling participants to explore differences between those who had engaged in ACP discussions and those who had not. They found several overarching themes that influenced engagement or not, these included, being proactive or passive/reactive; discussions about death being seen as normal or abnormal; family resistance/disconnection. Positive experiences of ACP discussions were where participants felt the professionals were confident in raising and discussing the main issues. Peterson and colleagues 54 argue that research is needed on health care practitioners’ use of tools to help patients discuss their end-of-life care preferences with family and others. Research is also required to measure the outcomes of using conversation prompt cards in facilitating ACP discussions in families affected by dementia. There is limited evidence relating to the development and evaluation of communication interventions for patients with life-limiting illnesses. 55 However, a successful intervention should include combined components of training, patient discussion and education. 55
Limitations to this study
This was a small and pragmatic TNA that was conducted towards the end of a training event on end-of-life care in dementia for a specialist group of dementia nurses. While further perceived training and education needs have been identified, the survey could have been more inclusive in its approach to identify specific personal inhibitors and enablers to facilitating ACP for people with dementia and their families.
Admiral Nursing is the only defined specialist nursing case management model in the United Kingdom; however, it may have been useful to include other professionals who offer ACP to people with dementia to contrast and compare levels of confidence and identify training needs to see whether they are comparable.
Conclusion
There is limited evidence relating to the development and evaluation of communication interventions to support ACP in families affected by dementia. However, much can be learnt from the use of a multicomponent educational intervention as employed in other life-limiting conditions, such as cancer. Although Admiral Nurses are specialists in dementia care, there are several educational initiatives that can be employed to better enable them to support ACP for families affected by dementia. Results of the TNA and the nurses’ identification of factors that would enhance both their confidence and skills to undertake ACP would benefit from including the combined components of communication training, supported by shadowing and supervised practice and a range of resources and materials to facilitate discussion. This TNA was the first step towards development of an educational intervention for Admiral Nurses in preparation of piloting an ACP intervention with the purpose of extending the discussions with the person with dementia as far into the advanced stages of the illness trajectory as possible.
Footnotes
Conflict of interest statement
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.