
Abstract
Objectives:
This study aimed to investigate the correlations of religiosity and psychological resilience with mental health among cancer patients and to examine whether religiosity and psychological resilience can predict mental health.
Method:
The sample consisted of 329 patients. Researchers applied Islamic Religiosity Scale, Wagnild and Young Resilience Scale, and the scale of Hospital Anxiety and Depression.
Results:
The results showed that there are positive, statistically significant correlations between religiosity and psychological resilience, while there were negative, statistically significant correlations of religiosity and psychological resilience with mental health. And there are correlations between the alternative therapeutic interventions currently used to religiosity and psychological resilience, while there were no statistically significant correlations between alternative therapeutic interventions that the patient will use in the future to religiosity and psychological resilience. The results also revealed the possibility of predicting mental health through religiosity and psychological resilience.
Conclusion:
These results emphasized the importance of increased religiosity and psychological resilience among cancer patients.
Keywords
Introduction and Theoretical Background
Cancer is a global problem. In 2010, cancer has infected more than 8 million people worldwide. The World Health Organization 1 report indicates that more than two-thirds of these new cases and cancer deaths will occur in the third world countries, where infection rates remain increased. 2 Breast cancer is the most common cancer in the world, among women, with 22% in all cases, and in Saudi Arabia the number of new cases of breast cancer is about 2741 cases of cancer in women. Breast cancer ranks first among Saudi citizens for both men and women (15.9%; see Saudi Ministry of Health, 2019). 3
Many studies have shown that there are many physiological and psychological changes that occur when cancer patients are directed to take chemotherapy or combination therapy (surgical, chemotherapy) or radiotherapy, which affects their mental health.
Religion and cancer in Saudi
Saudi Arabia represents the heart of the Muslim world, being viewed as the birthplace of Islam. It is the home of 2 of Islam’s holy sanctuaries, Mecca the Blessed and Madinah the Radiant.
The Holy Quran and the Sunnah provide the framework for Islamic law (Shareaa), which governs all aspects of life of every Muslim. The Holy Quran is observed as the authority of how to surrender to Allah’s will in various circumstances in life. The Sunnah considers to be complemented to the Holy Quran; it could be defined as the teachings and sayings of the Prophet Muhammad. The Prophet Muhammad said, “There is no disease that Allah has created, except that He also has created its treatment.” Cultural medicine in Islam is regularly reported as the Medicine of the Prophet. Examples for that are black seed, honey, olive oil, Zamzam water, Camel milk, and Camel urine. Recitation of the Holy Quran for all patients has a healing effect on the body, mind, and heart. Given that Saudi is a highly religious society, very little is known about the exact nature of religious role that plays in the lives of cancer patients in Muslim countries in general and in Saudi Arabia in particular.
More recently, Alqahtani et al 4 mentioned that from the patient’s point of view in Saudi Arabia, cancer affect much more than the physical body; it also affects the mind, the spirit, and social relationships.
Religion and health in general
For many people, religion and spirituality are important aspects of everyday life. A survey has found that 59% of people worldwide describe themselves as religious. Previous studies have recognized that most cancer patients rely on religion to help themselves to cope with the illness and its treatment. 5 Results of an interview survey conducted by The National Health showed that 69% of cancer patients reported praying for their health compared with 45% of the general US population. 6
Seeman et al 7 argued that religiosity/spirituality is linked to health-related physiological processes—including cardiovascular, neuroendocrine, and immune function. Hill et al 8 show that regular religious attendance was associated with a wide range of healthy behaviors, such as preventive care use, vitamin use, infrequent bar attendance, seat belt use, walking, strenuous exercise, sound sleep quality, never smoking, and moderate drinking. Similarly, in their study, Park et al 9 found that daily spiritual experiences were related to greater performance of health behaviors, while religious struggle was related to less.
There is an increasing interest in the role of religion in the context of health, illness, and health care practice; frequently, patients who are already religious become extremely religious when diagnosed with cancer, while others who are less religious search for spirituality occasionally and a linking to a power outside themselves after being diagnosed with cancer. 10
In the review of 18 quantitative studies about religion/spirituality and psychological well-being among breast cancer survivors, Schreiber and Brockopp 11 found that limited relationships exist among religion, spirituality, and psychological well-being, and also there was a sufficient evidence to include a brief, clinically focused assessment of women diagnosed with breast cancer regarding the importance of a given belief system as they face the diagnosis and treatment of their disease. Engel (1977) 12 argued that psychological and social factors influence biological functioning and play a role in health and illness. Recently, Arnout and Ahed (2019) 13 recommended the necessity and importance of applying the Biopsychosocial-Spiritual Model in all institutions that provide health care to patients with physical and psychological illnesses.
Religion as coping with cancer
According to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV), 14 cancer is one of the causes of posttraumatic stress disorder (PTSD), as it is a severe stress factor that threatens the lives of individuals with it.
Emmons 15 reported that one of the factors contributing to positive outcomes may be having a spiritual orientation to life which protects people from undesirable and non-adaptive behaviors such as destructive, social, or even personal behavior. And King 16 emphasized that spirituality plays an important role in all the steps of health care, especially its management, treatment, and healing.
The role of religion in coping with illness in general, and cancer in particular, has received quite little attention as an arena of study. Religion as a coping strategy could be defined as “applying cognitive behavioral techniques, in the face of stressful life events, that arise out of one’s religion.” 17 This role of religion in coping strategies is frequently observed as an emotional processing (eg, provide hope, forgiveness, comfort, love, and other emotional benefits), but it can have a cognitive processing (eg, reviewing the illness as part of Allah’s willing) as well as behavioral processing (eg, praying; avoidance of alcohol, tobacco, and drug use).18,19
In the same context, Park et al 20 found that both spiritual identity and the use of religious coping were positively related to fruit and vegetable intake, while private prayer was marginally positively related among breast cancer. And Gioiella, Berkman, and Robinson (1998) 21 found the inclusion of spirituality as part of the routine patient assessment and intervention. Clinical intervention that would increase a patient’s level of spiritual awareness can help decrease the patient’s level of psychosocial distress.
Religion and quality of life
Weber and Pargament 22 mentioned that religion has the energy to enhance mental health. Religion was defined as a meaning system that influences persons to cope with significant life stressors and promote mental health by enhancing psychological well-being and fostering meaning-making coping. 23
Several studies have examined the relationship between religion and psychological issues. The reviews of these literatures informed that religion has a positive relationship to psychological issues. A growing body of these studies has observed the association between religion and psychological issues in cancer patients and survivors. 24
Religion has been linked to plentiful results in adjustments to the cancer experience. In a recent meta-analysis for more than 44 000 patients, religion confirmed positive associations with multiple factors of health-related quality of life.19,24,25
Resilience among cancer patients
Cancer is the most prevalent and serious disease, and each stage of cancer has a different impact on the lives and mental health of patients.
Thus, Seiler and Jenewein 26 mentioned that the cancer experience is associated with positive and negative life changes. They found that biological, personal, and social factors contribute to cancer patients’ resilience.
Despite the considerable psychological impact that was linked to cancer diagnosis and its treatment, several patients show notable resilience. Resilience was conceptualized broadly as a dynamic process that involves adaptation to stressful conditioning, an adaptation that supports healthy levels of psychological functioning in the face of traumatic circumstances. 27
Extensive literature studies were conducted to investigate the role of resilience during one or more stages of cancer. Molina et al 28 revealed that promoting resilience is a critical element of patient psychosocial care. Likewise, Solano et al 29 detected a strong relationship between resilience and hope among metastatic colorectal cancer patients. And Dong et al, 30 in their study, found that resilience mediated the relationship between perceived social support and posttraumatic growth among colorectal cancer survivors. And Gao et al 31 showed that the higher level of resilience was related to less anxiety symptoms among patients with oral cancer.
Therefore, according to Seiler and Jenewein,
26
resilience is an important area for cancer patients because it may provide a protection against the negative effects of stress by lessening or absorbing the shock of a cancer diagnosis, the impact of aversive events, and related life changes and thus improve mental health and treatment outcomes. (p. 29)
Study Objectives
Few researchers have focused on resilience in linking with religion and mental health of cancer patients. To the best of the authors’ knowledge, this subject has not been presented in any Arab literature before. As it has been recommended in previous studies, and according to the reported relationship between religion and spirituality and mental health, there is a need for greater discrimination between differing cultures and traditions and increased focus on the situated experiences of patients belonging to certain societies. 22
Consequently, this study sought to provide a comprehensive summary of the relation between religion, resilience, and mental health among breast cancer patients in Saudi Arabia. We hypothesized that religion would be associated with better mental health among breast cancer patients. Additional analyses examined whether dimensions of religious and psychological resilience were predicting mental health (anxiety/depression).
Methodology
Population and sample
The statistical population of this study includes all patients diagnosed with breast cancer. From this population, we choose a random sample of 329 breast cancer patients, their age range between ⩽26 and ⩾45 years.
Tools
Islamic Religiosity Scale (40-Item Scale of Islamic Religiosity Attitude)
This scale was prepared by Marwa. 32 It consists of 40 items distributed into 4 dimensions: worship, virtues, forbidden, and beliefs. The individuals respond by using a 4-point Likert-type scale. The validity and stability of the scale were verified, the Cronbach alpha coefficients for dimensions and for the scale as a whole were 0.604, 0.847, 0.512, and 0.872, respectively, the low reliability of the 2-dimensional worship and creed is due to the low number of items, unlike the virtues and the scale as a whole. These results indicated that the Scale of Islamic Religiosity Attitude is reliable. To verify the validity of the scale, we used the confirmatory factor analysis (CFA). The quadratic model of the scale was tested to verify the suitability of its design for the new sample. The results showed that because the sample evaluation of forbidden dimension is 0, the dimension has become statistically constant and the statistic deals with the variables and does not deal with the constants, so this dimension was excluded because the sample is not different in the response to it, and the model to be verified is the tripartite model.
From Figures 1 and 2, the values of t corresponding to the path coefficients do not fall in the period (–1.96, 1.96), which means the significance of the path parameters. The model also achieved the conditions of good match (0). Therefore, the research team is satisfied with the scale criterion applicable to the new sample and that the data model complies with the theoretical model of the scale when it is prepared in the original version.

Path parameters of the triad model of Scale of Islamic Religiosity Attitude.

Values of t corresponding to the path coefficients of the 3-dimensional model of religiosity.
Wagnild and Young 14-Item Resilience Scale
The scale prepared by Wagnild and Young 33 contains 14 items spread across 5 dimensions: self-reliance (1, 5, 7, 12, 14), the meaningfulness (2, 9, 13), balance (3 and 10), perseverance (6 and 8), and existential aloneness (4 and 11). The individuals respond by using a 6-point Likert-type scale (1 = strongly disagree to 6 = strongly agree). The Cronbach alpha coefficients for dimensions and for the scale as a whole were 0.822, 0.724, 0.549, 0.734, 0.753, and 0.928, respectively; these results indicated that the Resilience Scale (RS) is reliable. To verify the validity of the RS-14, we used the CFA, and the 5-dimensional model was tested. The results are shown in Figures 3 and 4.

Path parameters of the 5 model of the psychological resilience test.

The t values corresponding to the path coefficients of the 5 model of psychological resilience.
From the Figures 3 and 4, we notice that the t values corresponding to path coefficients do not fall within the period (–1.96, 1.96). This indicates the significance of the path parameters. The value of the chi-square was a sign. The chi-square has many disadvantages and therefore it is recommended to be used together with other indicators of good fit. From sensitivity to the volume of correlation coefficients, high correlation coefficients lead to an increase in the value of a chi-square, and the chi-square is affected by the size of the sample, so we adopted alternative indicators, root mean square residual (RMR) = 0.03 is close to 0, goodness of fit index (GFI) was 0.984 (<0.90), adjusted goodness of fit index (AGFI) was 0.951 (>0.90). This result indicated that the RS scale is suitable for measuring the psychological resilience.
The 14-Item Hospital Anxiety and Depression Scale
This scale prepared by Alqahtani 34 contains 14 items distributed across 2 dimensions: anxiety (1, 3, 5, 7, 9, 11, 13) and depression (2, 4, 6, 8, 10, 14). The individuals respond by using a 6-point Likert-type scale (1 = strongly disagree to 6 = strongly agree). The Cronbach alpha coefficients for dimensions were 0.680 and 0.577, respectively, these results indicated that Hospital Anxiety and Depression (HAD) scale is reliable. To verify the validity of the HAD-14 scale, we used the CFA, and the 2-dimensional model was tested. The results are shown in Figures 5 and 6.

Path parameters of the model of anxiety and depression scale.

Values of t corresponding to the path parameters of the model of the anxiety and depression scale.
From Figures 5 and 6, the values of t corresponding to path coefficients do not fall within the period (–1.96, 1.96). This indicates the significance of the path parameters. The value of the chi-square was a significant because the chi-square is affected by the size of the sample, so we adopted alternative indicators, RMR = 0.038 is close to 0, GFI was 0.926 (>0.090), AGFI was 0.897 (>0.80). This result indicated that the anxiety and depression scale is suitable for measuring anxiety and depression.
Research design
A descriptive design was used in this study to examine the relationships between religiosity, resilience, and mental health, and to detective the differences in religiosity, resilience, and mental health due to demographic variables (duration of cancer, treatment stage, cause of cancer from the point of patient view), as well as test the possibility of predicting mental health through the level of religiosity or psychological resilience among breast cancer patients.
Data analysis
The obtained data were analyzed by using SPSS 25.0 (statistics package for social sciences) and LISRAL to test validity and reliability of the scales used in this study and in response to the study questions about correlation, differences, and predictability. After we tested the data normal distribution (see Table 1), the results showed that the values of normality tests were significant. This means that the distribution of the data are not consistent with the normal distribution curve. Consequently, the nonparametric statistic should be used to analyze the data if necessary.
Tests of Normality.

Results
The results about the relationship between the level of religiosity and psychological resilience among cancer patients
We used Pearson correlation coefficient to calculate correlations between religiosity (dimension and total scores) with the dimensions of psychological resilience and its overall score. The results are shown in Table 2.
Correlation coefficients between religiosity and psychological resilience.

P ⩽ .01.
From the results shown in Table 2, there are positive, statistically significant correlations between the dimensions of religiosity—except the forbidden, where it was a constant value—and the total score with all dimensions of psychological resilience and its overall scores with statistical significance level (0.01).
The results about the differences in the level of religiosity and psychological resilience due to the duration of cancer
We use the Kruskal-Wallis test used for calculating differences in the level of religiosity and psychological resilience due to the duration of cancer. The results shown in Table 3.
Results of the Kruskal-Wallis test for differences in the level of religiosity and psychological resilience in light of the duration of cancer.

From Table 3, the results indicated that there are no statistically significant differences due to the duration of cancer in both religiosity and psychological resilience. This may be due to the fact that the Saudi society is by its nature a religious society and there is a close correlation between the religiosity and psychological resilience. God teaches us how to face predestinations in our lives and how to control them and win the reward of God.
The results about the differences in the level of religiosity and psychological resilience due to the stage of cancer treatment
The Kruskal-Wallis test calculated to detective the differences in the level of religiosity and psychological resilience due to the duration of cancer. The results are shown in Table 4.
Results of the Kruskal-Wallis test for differences in the level of religiosity and psychological resilience due to the cancer treatment phase.
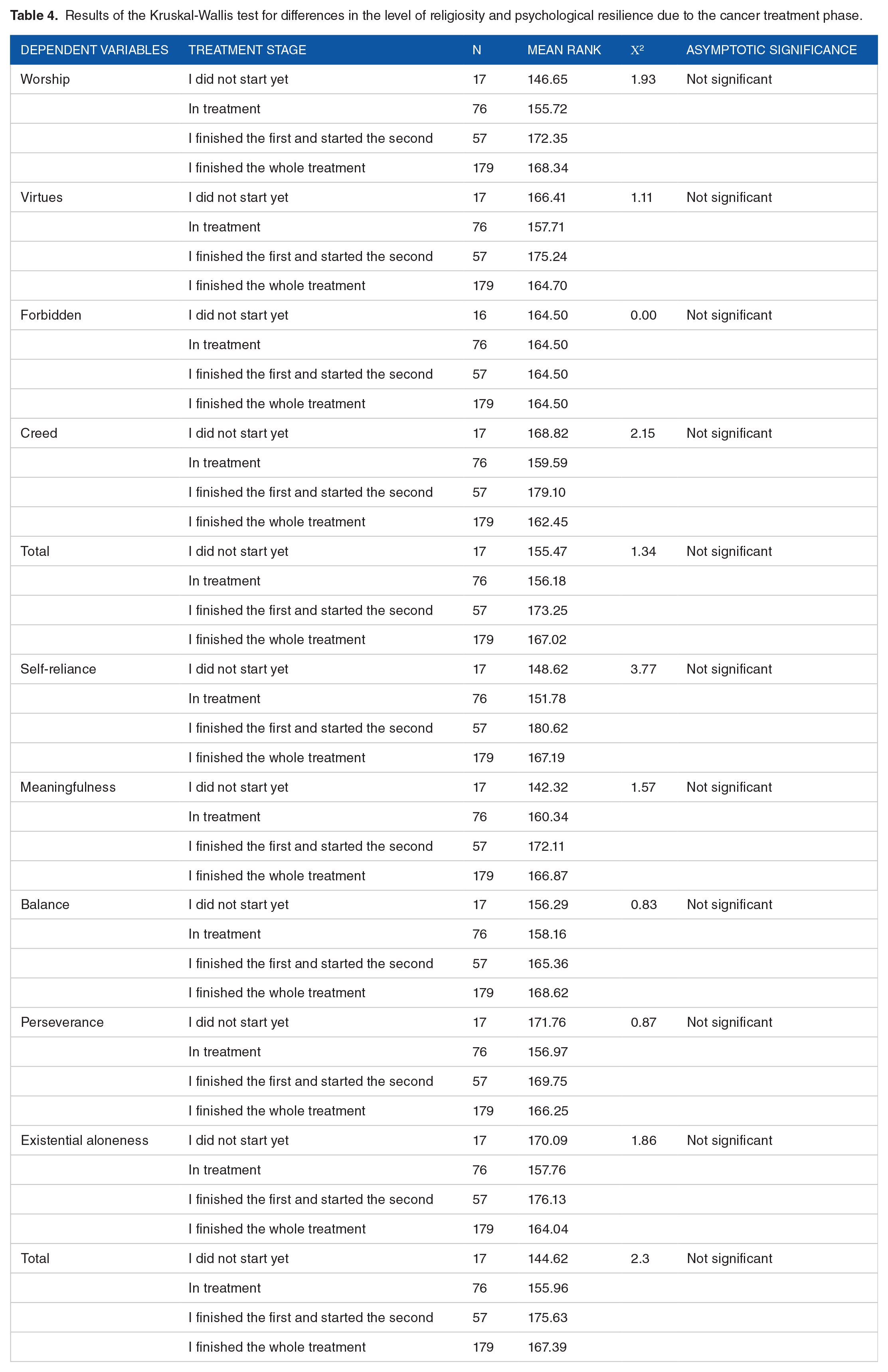
From Table 4, the results indicated that there are no statistically significant differences due to the stage of cancer treatment in each of religiosity and psychological resilience.
The results about the differences in the level of religiosity and psychological resilience due to the cause of cancer from the patient’s point of view
Because the variables are nominal variables, we used both eta and analysis of variance (ANOVA) analysis. The results are shown in Table 5.
The value of the eta2 to association between causes of the cancer and each of religiosity and psychological resilience.

It is clear from Table 5 that there is a low association between the belief in the cause of the disease and the religiosity and psychological resilience of breast cancer patients. Whereas the eta values (0.02 weak, 0.05 average, 0.14 strong, and 0.5 very strong).
The results shown in Table 6 indicated that there are no statistically significant differences in religiosity and psychological resilience due to the belief by patients about the causes of cancer.
Results of analysis of variance table for differences in religiosity and psychological resilience due to cause of cancer.

The results about the relationships between the level of religiosity and psychological resilience to alternative therapeutic interventions (medicine prophetic) that have been used or that the cancer patients thinks of using
Because the variables are nominal variable, we used the eta2 to determine the association between the variables. The results are shown in Tables 7 and 8.
The value of the eta2 for the correlation of alternative therapeutic interventions currently used and both religiosity and psychological resilience.

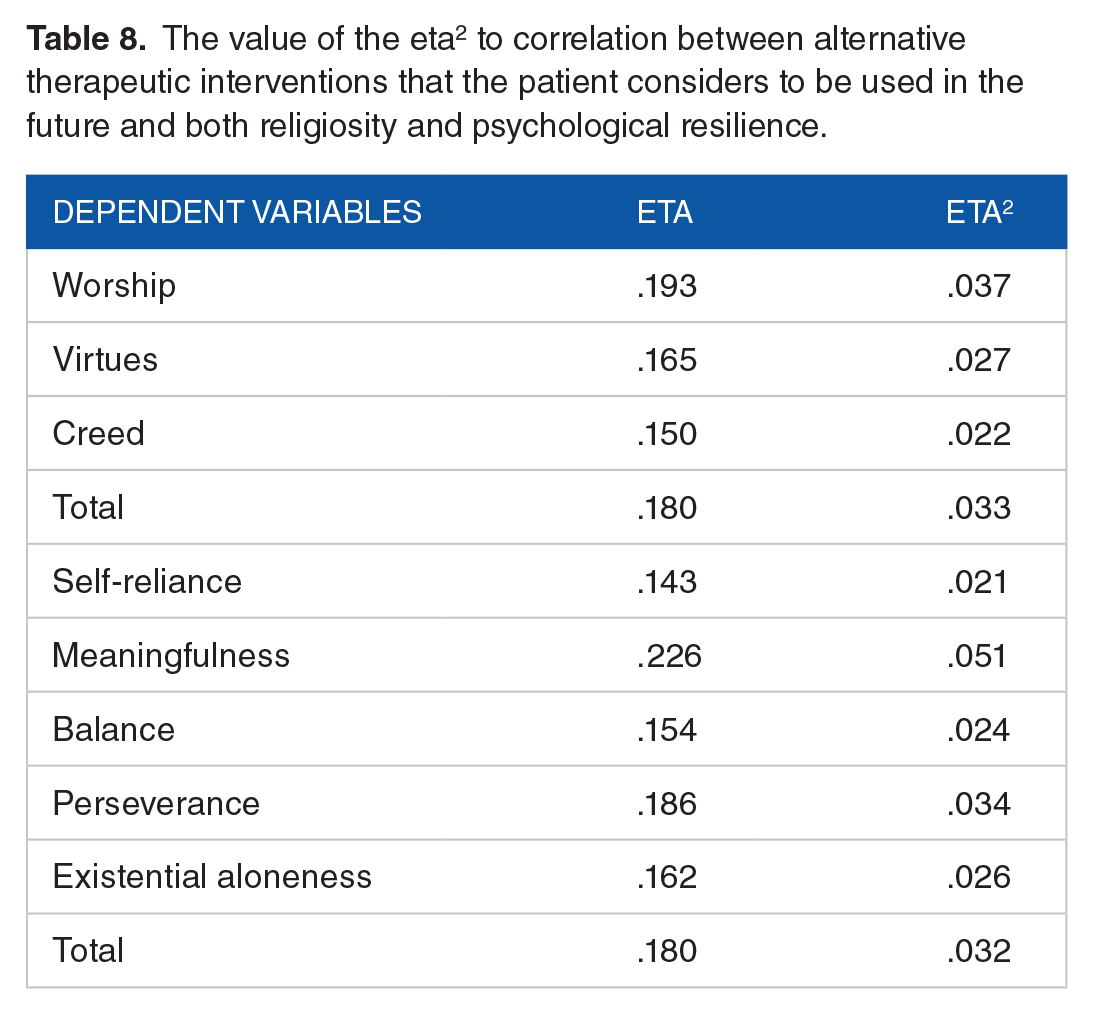
The value of the eta2 to correlation between alternative therapeutic interventions that the patient considers to be used in the future and both religiosity and psychological resilience.
The results shown in Table 8 indicated that there is a moderate correlation between alternative therapeutic interventions currently used and each of religiosity (worship, creed, and total score) and psychological resilience (all dimensions and total score except the meaningfulness dimension) in breast cancer patients.
It is clear from the results shown in Table 9 that there is no correlation between the alternative treatment interventions that the patients considered in the future to each of religiosity and the psychological resilience (all dimensions and the total score except the meaningfulness dimension) among cancer patients.
The value of the eta2 to correlation between alternative therapeutic interventions that the patient considers to be used in the future and both religiosity and psychological resilience.

The results shown in Tables 8 and 9 indicated that there are moderate correlations between the alternative therapeutic interventions currently used to both religiosity (worship, creed, and total score) and psychological resilience (all dimensions and the total score except the meaningfulness dimension), while the results found that there were no correlation between alternative therapeutic interventions that the patient thinks of future use to each of religiosity and psychological resilience (all dimensions and total score except the meaningfulness dimension) among cancer patients.
The results about the contribution of religiosity and psychological resilience to predict cancer patients’ mental health (depression/anxiety)
We used the Stepwise Regression. The results are shown in Table 10.
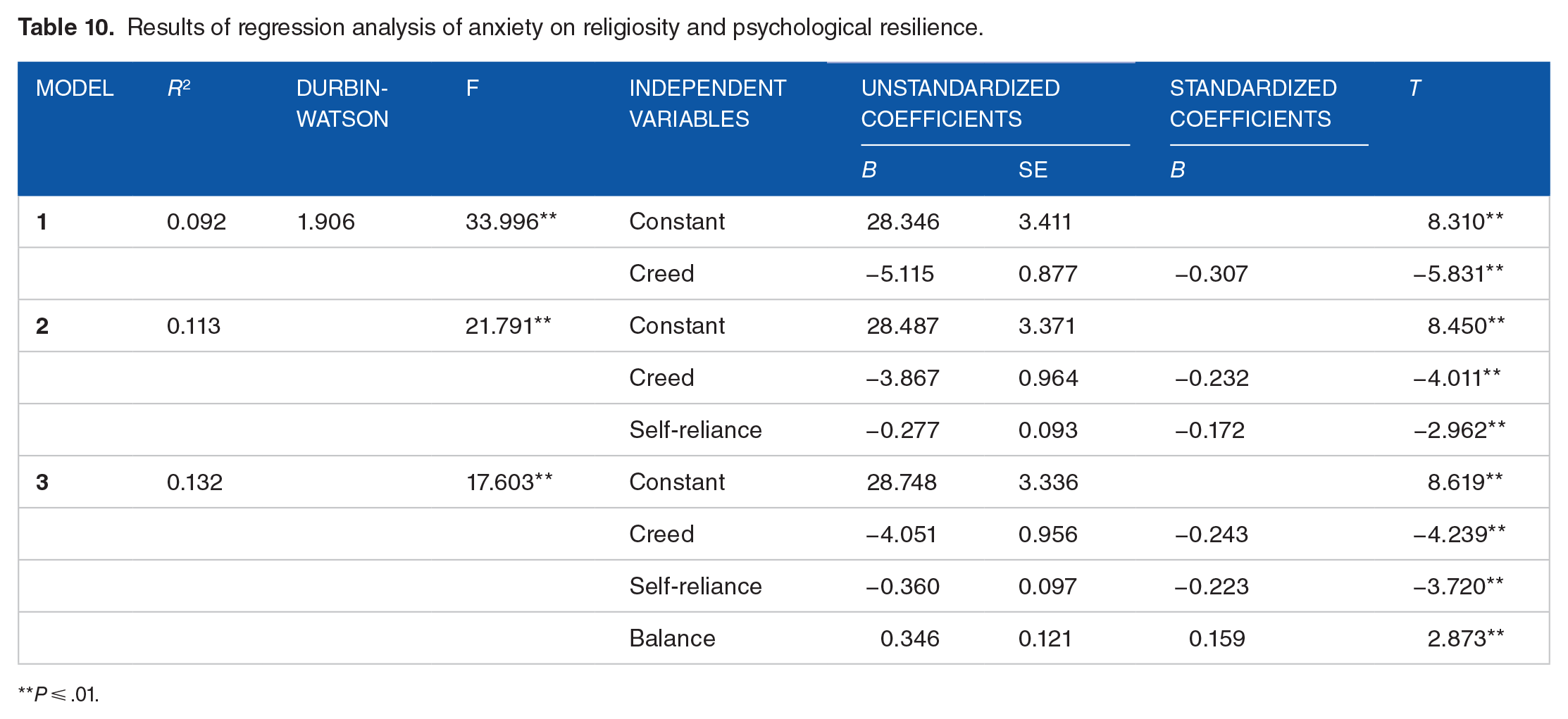
Results of regression analysis of anxiety on religiosity and psychological resilience.
P ⩽ .01.
From the results shown in Table 10, the creed explains 9.2% of the variation in anxiety, creed, and self-reliance, explaining 11.3% of the variation in anxiety, and the 3 variables of creed, self-reliance, and balance explain 13.2% of the total variance of anxiety among cancer patients. And the Darben-Watson coefficient was close to 2, which meant that the effect of the residue was weak, and all P values of the 3 models indicate that there is an effect of the independent variables in each model on the dependent variable (anxiety).
These results indicated that the most important factors affecting anxiety among cancer patients were cured, followed by the first dimension of psychological resilience (self-reliance), and then the third dimension of psychological resilience (balance). The following equation can be formulated to predict anxiety among cancer patients from religiosity and psychological resilience
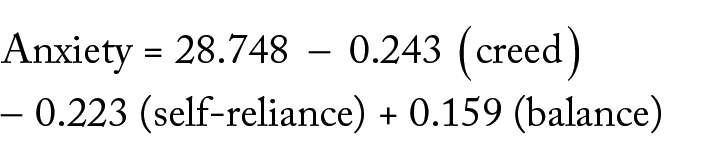
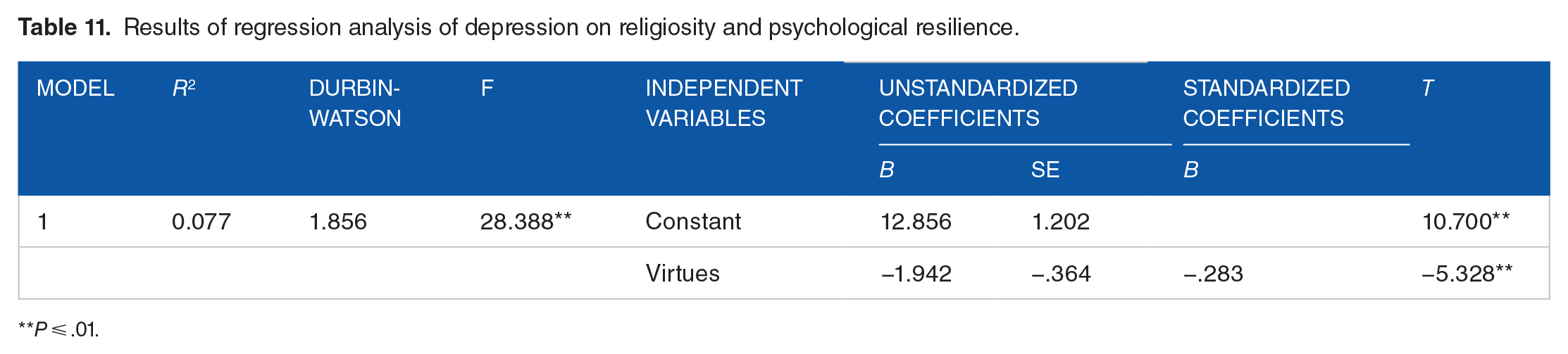
The results shown in Table 11 indicated that the virtues account for 7.7% of the total variance of depression in breast cancer patients, and the Derbin-Watson coefficient was close to 2. The results also show that the most influential factor in depression was virtues, while there was no effect on the other dimensions of religiosity or psychological resilience on the scores of depression, and the equation of prediction is Depression = 12.856 – 1.942 (virtues).
Results of regression analysis of depression on religiosity and psychological resilience.
P ⩽ .01.
Discussion
Brest cancer patients exposed to chronic stress has caused a wide range of psychological negative health outcomes. It is important to understand that risk factor of cancer patients’ stressful experience may be mediated by individual factors, such as personality traits, sex, ethnicity, religion, beliefs, and human culture.
This study revealed that mental health correlated with religiosity and psychological resilience. This finding is compatible with Behere et al 35 reporting that religiosity provides guidelines, which can help patients to devise a course for their lives and to cope with life stresses. Arnout 36 mentioned that individuals with high spiritual intelligence invest more effort and persist longer than individuals with low spiritual intelligence. Therefore, it may be expected that those with high spiritual intelligence will choose effective or problem-centered coping strategies, whereas those with low spiritual intelligence use negative emotional strategies.
In their review, Moreira-Almeida et al 37 mentioned that the positive impact of religion on mental health is more robust for who are faced with stressful circumstances such as those with medical illness (such as cancer). The higher levels of religion are positively correlated with mental health indicators and with less depression, suicidal thoughts and behavior, and drug/alcohol. The results of earlier studies showed that religiosity associated with heath indicators (Hill et al, 2003; Schreiber et al, 2012; Park et al, 2018)20,38,39 and related to quality of life.19,24,25
The results of this study consisted of findings of systematic reviews that reported positive correlations between religion and mental health. Bonelli and Koenig 40 found that there was good evidence that religious involvement correlated with better mental health in the areas of depression, substance abuse, and suicide; some evidence in stress-related disorders and dementia. And the review of 74 articles published between January 2000 and March 2012 conducted by AbdAleati et al, 41 findings of past studies, found that religion could play an important role in mental health. Recently, Färber and Rosendahl, 42 in their systematic review and meta-analysis, found a strong association between resilience and mental health in the somatically ill.
In addition, the findings of this study also consisted with systematic reviews that found resilience was correlated negatively with symptoms of mental problems in patients with physical illness, cancer, and chronic disease.43-47
Davydov et al 48 argued that resilience can be viewed as a defense mechanism, which helps individuals to cope effectively adversity. Bowes and Jaffee 49 mentioned that most definitions of resilience include the overcoming of stress, adversity, and environmental risk. From the perspective of positive transformations, resilience plays an important role in maintaining mental health, restoring homeostasis, and increasing the level of functioning. 50
Several factors that promote resilience include religion. Religion has been exposed to be a key in promoting resilience among older adults. 51 About the role of religion and resilience for patients, Jones et al 52 found correlations between the higher levels of spirituality with improved quality of life, life satisfaction, mental health, and resilience for spinal cord injury patients.
Religion is seen as providers of path for coping with health and illness in Muslim culture. Exploiting the natural resources of religion can promote resilience mechanisms in negative life events 53 and can enhance recovery by providing faith and hope in being able to overtake after a cancer diagnosis and recover health. 54
All of these findings emphasized that each of religiosity and psychological resilience plays a role in coping with the stress of cancer, and, in turn, it relieves the negative effects of it. Thus, if we need to recover the homeostasis and mental health of breast cancer patients, it is necessary to improve their religiosity and psychological resilience skills through counseling interventions.
Conclusion
Through the results of this study, it is clear that cancer is considered as a stressor situation for patients and caused many mental health problems such as anxiety and depression in all stages of cancer continuum. And each of religiosity and psychological resilience were contributed statistically significant directly to the product of the breast cancer mental health.
These results emphasized the importance of developing each of religiosity and psychological resilience among cancer patients in Arabic Countries to increase their mental health. These results have a future direction in the field of counseling and psychotherapy for cancer patients, to plan counseling interventions that aimed to decrease psychological distress and mental disorders among cancer patients.
Footnotes
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Deanship of Scientific Research at Princess Nourah bint Abdulrahman University through the Fast-track Research Funding Program.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Nawal A Al Eid, Mohammed MJ Alqahtani and Boshra A Arnout were responsible for the conceptualization and acquisition of the data. Mohammed MJ Alqahtani and Boshra A Arnout were responsible for the methodology. Mohammed MJ Alqahtani and Boshra A Arnout were responsible for the writing, review, and/or revision of the manuscript. Nawal A Al Eid, Khaldoun Marwa, Hajar S Alswailem, and Al Anoud Al Toaimi were responsible for the administrative, technical, or material support. Nawal A Al Eid was responsible for the study supervision.