
Abstract
Objective:
Bone is the most common site of metastasis in breast cancer. Prognostic factors for predicting bone metastases in breast cancer are controversial yet. In this study, we investigated clinical factors associated with secondary bone metastasis of breast cancer.
Methods:
In total, 1690 patients with breast cancer recorded between 2002 and 2012 in Motamed Cancer Institute, Tehran, Iran entered in the retrospective study. We studied age, menopausal status, histologic type, tumor size, number of cancerous axillary lymph nodes, serum concentrations of alkaline phosphatase (ALP), carcinogenicity antigen (CEA), cancer antigen (CA)-153, and hemoglobin (HB) in 2 groups with bone metastases (n = 123) and without it, respectively. We applied logistic regression to identify bone metastasis prognostic factors in breast cancer patients and calculated the cut-off value, sensitivity, and characteristics of independent prognostic factors using receiver operating characteristic (ROC) curve analysis.
Results:
Menopause, larger tumor size, and the greater number of cancerous axillary lymph nodes increased the chance of bone metastases significantly (P < .05). There was no significant difference between mean groups with and without bone metastases regarding serum concentration of CEA, CA-153, HB, and histopathologic type (P > .05). Logistic regression showed that age (odds ratio (OR) = 1.021), menopausal status (OR = 1.854), number of cancerous axillary lymph nodes (OR = 1.065), a tumor size between 2 and 5 cm diameter (OR = 2.002) and more than 5 cm diameter (OR = 4.009), and ALP (OR = 1.005) are independent prognostic factors associated with bone metastases. The ROC curve showed that the abovementioned factors have comparable predictive accuracy for bone metastases.
Conclusions:
Age, menopausal status, number of axillary lymph node metastases, tumor size, and ALP were identified as prognostic factors for bone metastasis in patients with breast cancer. So patients with these characteristics should be monitored more precisely with regular follow-ups.
Introduction
Breast cancer (BC) is the most common malignancy and a major cause of morbidity and mortality among women. During the past decade, the mortality rate has declined because of early detection by mammography, surgery, and more advanced treatment. But its recurrence in distant areas ranges from 20% to 30% of patients. 1
Bone is the most common site of metastasis and is also the most common site of first distant relapse. 2 In total, 60% to 75% of metastasis in BC is diagnosed as bone metastasis (BM) at first. 3 BM significantly reduces 5-year survival and causes serious complications 4 ; however, BC patients with BM seem to have a longer survival than those with cancer in other metastatic sites. 5 The most common symptoms of BM are severe osteodynia, pathologic fractures, and nerve compression. 3
In addition, the osteolytic metastasis can cause a remarkable reduction in bone tissue which ultimately leads to skeletal-related events including pathological fracture, spinal cord compression, hypercalcemia, bone loss and severe pain. 6 A clear complete understanding of the process of metastasis of BC can be beneficial in preventing and treating the disease. However, there is a wide range of patients who have no clinical symptom which is leading to missing detection of BM.7,8
Imaging study is still the primary method for diagnosing BM, and bone scintigraphy is routinely used for the detection of BMs. Although bone scintigraphy as a non-specific approach has traditionally shown good sensitivity for detection and assessment of the extent of BM, the negative side effects of continued radiation to BC follow-up cannot be ignored. It could not provide enough information for early diagnosis. 9 Thus, it is necessary to find a way to detect BM in patients with BC for early diagnosis and treatment. Early diagnosis of BMs from BC is a beneficial for its timely intervention and preventing pathologic bone fracture.
Several fundamental studies have been conducted to find out demographic, clinical, pathological, and genetic factors affecting the BM in BC patients. International Breast Cancer Study group studied BM in a group of 6000 patients. They reported a number of cancerous axillary lymph nodes, large tumor size, and estrogen receptor as the risk factors for BM. Diessner et al 10 applied 5 different models to investigate clinical risk factors associated with BM and reported that age is the most relevant factor affecting BM. Wen-Zhao Chen indicated that BC patients with more axillary lymph node metastases, high serum concentrations of cancer antigen (CA)-125, CA-153, and alkaline phosphatase (ALP), and low level of hemoglobin (HB) were closely related to BMs. Combined axillary lymph node metastases, CA-153, and ALP with HB have the highest predictive accuracy for BMs in BC. 6
Evidence has shown that BM risk depends on BC subtype.11,12 Biomarkers such as luminal A BC with estrogen receptor (ER)/progesterone receptor (PR)+ may have a higher tendency to develop BM. 13 More than 60% of primary tumors, which were ER/PR positive, finally lead to BM. 14 Also, risk of BM in BC patients who are hormone receptor (HR) positive is 1.66 times higher than that in those with HR-negative BCs. 15
Because the routinely used tumor markers in BC cannot accurately predict the risk of metastasizing to bone, 16 other risk factors are required for early diagnosis and treatment. To our knowledge, risk factors such as serum concentrations of CA-125, CA-153, and ALP for BMs from BC have been examined in a few studies and remain still unclear. So, in this retrospective study, we studied the correlation between clinico-pathological parameters of the bone marrow to identify the prognostic factors for detecting BMs early in BC patients.
Materials and Methods
Study design
This retrospective study was conducted on patients who had referred to Motamed Cancer Institute, Tehran, Iran between 2002 and 2012. All the participants had obtained informed consent. The study was performed in accordance with the guidelines and approved by the Ethics Committee of the Tehran University of Medical Sciences. The presence of BC was diagnosed based on histopathologic analysis of biopsy and open surgical specimen. BM and other organ metastases were identified via a positive bone scan. In a few cases, local computed tomography (CT) and magnetic resonance imaging (MRI) were used to confirm the diagnosis. Patients with metabolic bone disorders, end-stage renal disease (ESRD), malnutrition, and malignancy were excluded from the study. In addition, patients with metastasis to other distant organs, including the lung, liver, and brain, were also excluded from the study.
Data collection
Demographic and clinical data, including age, menopausal status, histologic type, number of cancerous axillary lymph nodes, tumor size, carcinogenicity antigen (CEA), CA-153, ALP, and HB, were extracted from the patients’ medical records. Then, the association of the above factors with BM in BC was investigated.
Statistical analysis
Statistical analyses, including mean and standard deviations of continuous variables and percentages of categorical variables, were performed using SPSS 19.0 software (SPSS Inc, Chicago, IL, USA). Initially, patients with BC were divided into 2 groups: with BM and without BM then t-test and chi-square test were used to detect the differences between the 2 groups. We applied logistic regression to identify independent prognostic factors for BM in BC patients. Then the receiver operating characteristic (ROC) curves and the areas under the curve (AUCs) were calculated to evaluate the predictive accuracy of prognostic factors. The ROC curve analysis was first applied to a single factor and then for a combination of diagnostic factors. Statistical significance was set at P-value less than .05.
Results
Clinical features of patients
This study included 1690 patients with BC and a total of 123 patients (7.3%) had BMs. Clinical features of patients are shown in Table 1. The results showed that the mean (SD) age of patients with BM, that is, 49.55 (13.51), was significantly higher than that in patients without BM, which is 47.06 (11.10) (P = .028). At the time of diagnosis, 58.3% of the cases were menopausal. There was a remarkable statistical difference in BM between postmenopausal and premenopausal women (P = .001) as postmenopausal women are more likely to have BMs. In total, 67.4% of BC patients were in the histopathologic invasive ductal carcinoma (IDC) group. There were no statistically significant differences in histopathologic type between BC patients with and without BM (P > .05). About 23.5% of patients had 1 or more lymph node metastases. Comparison of patients with and without BM showed that the lymph node metastasis groups were significantly different (P = .036). Moreover, there was a remarkable difference in the incidence of BMs between the different tumor size groups (P = .001).
Clinical characteristics of patients with breast cancer.
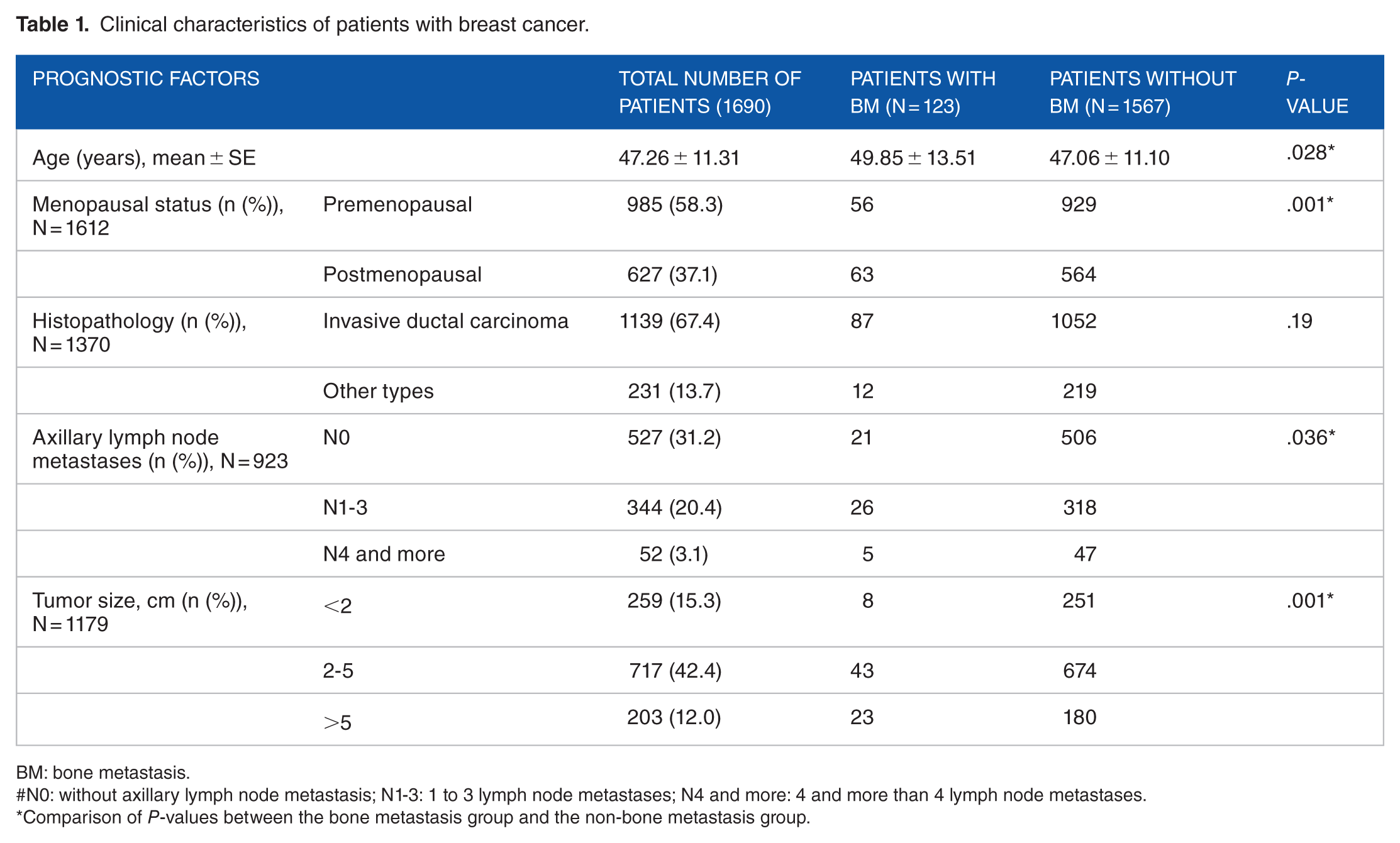
BM: bone metastasis.
#N0: without axillary lymph node metastasis; N1-3: 1 to 3 lymph node metastases; N4 and more: 4 and more than 4 lymph node metastases.
Comparison of P-values between the bone metastasis group and the non-bone metastasis group.
The t-test showed that serum ALP concentration was statistically significant in patients with and without BM, the serum concentrations of ALP were significantly higher in patients with BMs compared with those without bone lesions (P = .019), and other parameters were not significantly different (Table 2). The results of logistic regression analysis showed that age, menopausal status, tumor size, number of cancerous axillary lymph nodes, and ALP are the independent prognostic factors in patients with BC as the growth of the mentioned factors is associated with an increased risk of BM (Table 3). The sensitivity and specificity analyses of predictive prognostic factors were conducted using the ROC curve and AUC (Figure 1 and Table 4). According to the results from the analysis of the ROC curve, the number of cancerous axillary lymph nodes with sensitivity and specificity of 73.1% and 46.4%, respectively, was the most accurate predictive factor (AUC = 0.62, P < .001). The cut-off values for age and tumor size were 49 and 2.5, respectively (Table 4).
Differences in clinical factors between patients with and without bone metastases.

ALP: alkaline phosphatase; CA: cancer antigen; CEA: carcinogenicity antigen; HB: hemoglobin.
Risk factors for predicting bone metastases in patients with breast cancer.

ALNM: axillary lymph node metastases; CI: confidence interval; MS: menopausal status; OR: odds ratio; TS: tumor size.
B represents the coefficient of regression.
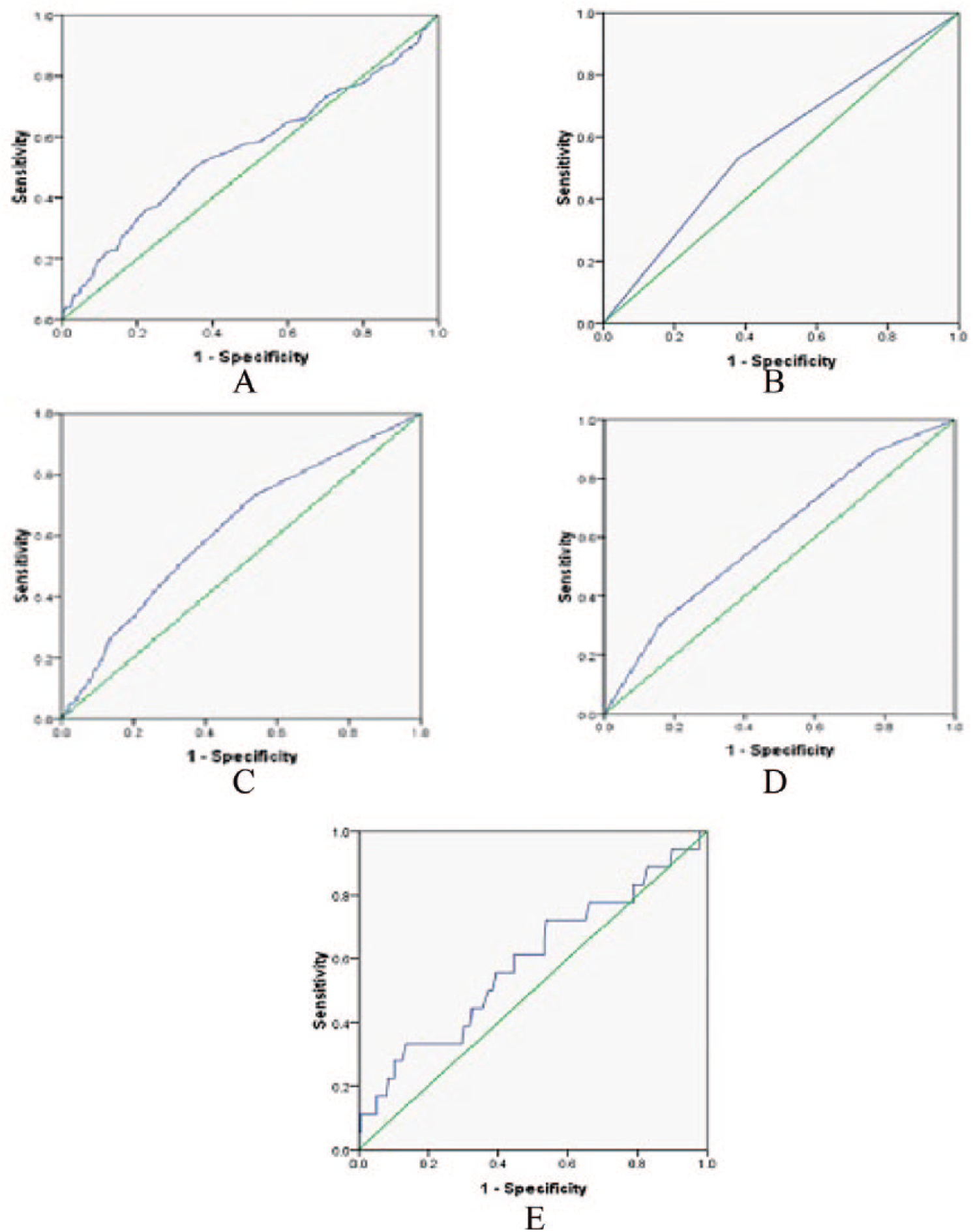
The receiver operating characteristic (ROC) curves of prognostic factors for detecting bone metastases in breast cancer: (A) the ROC curve of age, (B) the ROC curve of menopausal status (MS), (C) the ROC curve of axillary lymph node metastases (ALNM), (D) the ROC curve of tumor size (TS), and (E) the ROC curve of alkaline phosphatase (ALP).
Cut-off values, sensitivities, and specificities of predictive risk factors for bone metastases.

ALNM: axillary lymph node metastases; ALP: alkaline phosphatase; AUC: area under the curve; MS: menopausal status; TS: tumor size.
In addition, ROC curve analysis was conducted for various combinations of prognostic factors to identify the accuracy of combined factors for diagnosing BM (Table 5 and Figure 2). The results showed that among the combinations of prognostic factors, combined axillary lymph node metastases, tumor size, and menopausal status have the highest predictive accuracy for BM in BC (AUC = 0. 7, P < .001).
Analysis of predictive accuracy of combining different prognostic factors for bone metastases in breast cancer.

ALNM: axillary lymph node metastases; AUC: area under the curve; MS: menopausal status; TS: tumor size.

The receiver operating characteristic (ROC) curves of different combinations of prognostic factors for bone metastases: (A) the ROC curve of TS + ALNM and (B) the ROC curve of TS + ALNM + MS.
Discussion
Bone is the most common site of BC metastasis. It is often related to poor prognosis and low quality of life in patients. Therefore, early diagnosis of bone metastatic lesions in BC patients is important. Diagnostic methods, including CT and positron emission tomography-computed tomography (PET-CT) are costly and time-consuming. Bone scan is a common method for the detection of BMs in patients with distant tumor, but is not able to detect osteolytic metastasis.17,18 Analysis of serum tumor markers’ concentrations and prognostic factors for BMs are effective in early detection of BMs. Early diagnosis of BMs in BC patients may lead to timely intervention and may prevent pathologic bone fracture. Therefore, we studied the correlation between clinico-pathological parameters of the bone marrow to identify the prognostic factors for BMs in BC patients.
In this study, the rate of BM was 7.3%, which is less than 13.2% and 15.33% reported by Liede et al 19 and Chen et al, 6 respectively. At the time of diagnosis, 58.3% of the women were menopausal and more than half of the patients were older than 46. Considering the higher incidence of BM between patients aged 49 and older, it is implied that elderlies and postmenopausal patients are more likely to have a higher risk of BMs.
Further analysis with logistic regression showed that age and menopausal status are prognostic factors for BM. It also showed that a 1-year increase in age increased the risk of BM by 1.02-fold. Age above 49 is a major predictive factor for BMs. A retrospective study in Germany also reported that people aged more than 65 have a higher risk of BMs and reported that age is the most important prognostic factor for BM. 10
Menopausal status may also contribute to the BM development in patients with BC, because estrogens are essential for bone regeneration and their lack may increase the chance of BM. 20
In a study in the United Kingdom, with 367 patients, older and menopausal women were more likely to develop BMs. 21 In our study, menopausal women are 1.85 times more likely to have BMs than premenopausal women.
In this study, there was no significant difference between ductal types in the 2 groups with and without BMs. Some studies indicate that there is no relationship between the histologic type and the BM, and other studies have reported a small association. 20
In this study, BC patients who were in groups of 1 to 3 cancerous axillary lymph nodes have a significantly higher frequency than the other groups. Additional analysis showed that the number of metastatic axillary lymph nodes is one of the prognostic factors for BM in patients with BC. The increase in the number of metastatic axillary lymph nodes increased the risk of BM by 1.065-fold. Colleoni et al 22 also found that patients who had 4 or more cancerous axillary lymph nodes at the time of diagnosis had the highest frequency of BMs in BC. The number of axillary node metastases appears to be an important prognostic factor for BMs in BC.
From the analysis of tumor size, tumors larger than 5 cm in size increased the risk of BM by 1.065-fold than tumors less than 2 cm. The tumor size between 2 and 5 cm did not differ significantly from the tumor less than 2 cm. Based on the analysis of the ROC curve (AUC = 0.61), a cut-off value of 2.5 for tumor size predicts the occurrence of BMs. Several studies have reported tumor size as a prognostic factor for BM.23,24 Wei et al 23 reported that tumors with BM had a mean size of 2.8 cm when tumors without BM had a mean size of 1.8 cm.
Considering serum concentrations of ALP, CEA and CA-153 had a significantly different mean value in both groups with and without BMs. According to logistic regression analysis, ALP was a prognostic factor for BMs, as an increase in ALP increased the risk of BM 1.005 times. ALP as a bone formation marker is most widely used for assessing BMs in breast and prostate cancers. Ritzke et al 25 showed that ALP in combination with CA-153 had the highest sensitivity for predicting BMs. Chen et al 6 showed that an ALP serum concentration above 100.5 u/L is a risk factor for BM. In this study, the results showed that the serum level of ALP was correlated with a BM in BC, with a cut-off value of 230 U/L. It meant that ALP > 230 U/L was a risk factor for developing BM in patients with BC.
Previous studies have reported that a shortage of red blood cells containing HB is a common complication that affects more than 50% of cancer patients. Kawai et al 26 identified a component of the BMs associated with prostate cancer and reported it as HB. Henke et al 27 reported that the level of HB is a significant prognostic factor in metastatic BC. In this study, HB levels in BC patients with BMs were not significantly different.
Moreover, we analyzed various combinations of prognostic factors to identify the accuracy of the combined factors of BM. Among the combinations of prognostic factors, combined axillary lymph node metastases, tumor size, and menopausal status have the highest predictive accuracy for BM in BC.
The generalizability of these results is subject to several limitations. First, the study was conducted by relying on only 1 database of an organization (Tehran Breast Cancer Research Center of Tehran University of Medical Sciences), although the criteria were designed to cover minimizing selection bias. Second, the study was retrospective and some clinical data were missing, which may affect the results of the analysis. Also, we just collected information from patients with BC at the time of diagnosis and the study did not include some data, such as patient survival rates and follow-up treatment data. Therefore, a multi-center, prospective study is suggested to be conducted to assess the results of this study.
We conducted a retrospective study on a large population of patients with BC to investigate the prognostic factors of BMs. In our study population, 7.3% of cases had led to BMs. The age above 49, axillary lymph node metastases, tumor size greater than 2.5 cm, postmenopausal status, and high concentrations of ALP were identified as the major prognostic factors of BMs in patients with BC. So patients with these characteristics should be monitored more precisely with a regular follow-up. It can be beneficial in early diagnosis of BMs from BC and prevention and treatment of the disease. For newly diagnosed patients, the values of ALP > 230 U/L could be used as an additional factor for determining the risk of developing BMs. However, the validation of this factor in clinical practice needs further study to confirm. Despite the use of the retrospective methodology, a multi-center, prospective study is suggested to be conducted to assess the results of this study.
Conclusions
Age, menopausal status, number of axillary lymph node metastases, tumor size, and ALP were identified as the risk factors for BM in patients with BC. So patients with these characteristics should be monitored more precisely with regular follow-up.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
AY designed the study and analyzed the data. SD and HZ prepared initial draft and literature review. AA participated in data acquisition and draft edition. HSH assisted in data analysis and finalized the draft. All authors read and approved the final manuscript.