
Abstract
Purpose:
Trastuzumab, a humanized anti-human epidermal growth factor receptor 2 (anti-HER2) antibody delivered intravenously, has revolutionized the treatment of patients with breast cancer overexpressing HER2 protein. Recently, a newer subcutaneous formulation was shown to have comparable efficacy to the initial intravenous trastuzumab. In this study, we aimed to evaluate the impact of subcutaneous trastuzumab on the health-related quality of life (HRQoL) of patients diagnosed with early or metastatic HER2-overexpressing breast cancer.
Methods:
Patients were provided with the EORTC QLQ-C30 (European Organization for the Research and Treatment of Cancer Quality of Life Questionnaire-Core 30) and the BR-23 questionnaires. The scoring of questionnaires and patient’s sociodemographic and clinicopathologic characteristics were recorded and analyzed by descriptive and correlation statistics employing t test and 2-way analysis of variance.
Results:
A total of 163 patients agreed to participate in the study. About 90 of 163 patients (55.21%) received subcutaneous trastuzumab and 21 patients intravenous trastuzumab (12.88%). A control group of 52 HER2+ patients received chemotherapy without trastuzumab (31.90%). Patients receiving subcutaneous trastuzumab were older and of more advanced disease stage compared with those receiving chemotherapy (58.5 vs 51 years, 39.8% vs 28.8% advanced disease). In univariate analysis, subcutaneous trastuzumab was associated with less nausea and vomiting (P = .002) but worse cognitive function (P = .013) and dyspnea (P = .042). Patients who have received >8 cycles of subcutaneous trastuzumab reported less diarrhea (P = .049) and systemic therapy side effects (P = .015). Multivariate analysis showed that patients without comorbidity receiving subcutaneous trastuzumab had less treatment side effects, less upset by hair loss, and higher emotional functioning. Of note, mastectomy and subcutaneous trastuzumab were associated with improved role functioning (P = .021). In metastatic disease, no negative impact of subcutaneous trastuzumab on HRQoL was found.
Conclusions:
The administration of subcutaneous trastuzumab improved certain symptoms and did not adversely affect most of the assessed functional scales. Particularly, in the metastatic setting, subcutaneous trastuzumab had no negative impact on HRQoL.
Keywords
Introduction
The overexpression of human epidermal growth factor receptor 2 (HER2) results in deregulated proliferation signaling at the cellular level and a clinically more aggressive disease with poor prognosis.1,2 Trastuzumab, a humanized anti-HER2 monoclonal antibody, provided intravenously in combination with chemotherapy and endocrine therapy was shown to improve the overall survival of patients with early or metastatic breast cancer.3–6 At 11 years’ follow-up analysis of patients participating in the HERA (HERceptin Adjuvant) clinical trial, where intravenous trastuzumab was administered for 1 year following adjuvant therapy, an impressive 26% reduction in the risk of death was shown. 6 Another landmark clinical trial investigating the role of intravenous trastuzumab in the metastatic setting indicated a reduction in the relative risk of death by 20%. 5 Furthermore, 3 clinical studies investigating the health-related quality of life (HRQoL) in patients with metastatic breast cancer treated with intravenous trastuzumab substantiated its beneficial effect on the quality of life of patients, particularly those with responsive disease. 7
In 2012, HannaH study showed that subcutaneous trastuzumab, administered over 5 minutes, has a pharmacokinetic profile and efficacy noninferior to standard intravenous administration, with a similar safety profile. 8 Compared with the intravenous counterpart, the subcutaneous trastuzumab formulation has many clinically meaningful advantages including a less invasive, safer, and a shorter time of administration. 9 In addition to these advantages, the subcutaneous administration requires less preparation and administration expenses, manpower engagement, and day clinic time resulting in reduced health care system burden and costs. 10 The PrefHer study compared sequential subcutaneous trastuzumab for 4 cycles followed by intravenous trastuzumab and vice versa in patients with HER2+ early breast cancer and showed that the subcutaneous administration was both well tolerated and the preferred option between the 2 formulations. 11
Despite the advantages of the subcutaneous over the intravenous formulation and the preference of patients in receiving the new drug delivery method, literature is still scarce regarding the impact of the new formulation on HRQoL parameters. Health-related quality of life is assessed by a tool that contains a wide meaning which encompasses emotions, life satisfaction, health beliefs, adaptability, and functionality, in relation to disease and life span. As a result, a HRQoL study exploits the impact of the health status on quality of life.12,13
The aim of this prospective study was to assess HRQoL in patients with early, locally advanced, or metastatic HER2-overexpressing breast cancer under treatment with standard therapy including subcutaneous trastuzumab.
Materials and Methods
The study was conducted in the context of a Postgraduate Course (master’s thesis) in Health Care Services Management, Greek Open University, Patras, Greece, and a University of Athens Research Board and Ethics Committee approval was obtained. Patients were asked to provide informed consent prior to responding to the questionnaires.
Patients
From December 2015 to May 2016, patients with HER2+ breast cancer, either by immunohistochemistry or by fluorescent in situ hybridization, were identified in 5 Cancer Day Clinics in Athens and asked to participate in this observational study.
Patients with HER2+ early and metastatic breast treated with subcutaneous trastuzumab or chemotherapy and subcutaneous trastuzumab were eligible. Additional main inclusion criteria included older than 18 and less than 80 years of age, an Eastern Cooperative Oncology Group performance status of 0 or 1, and a normal baseline left ventricular ejection fraction. Exclusion criterion was participation of patients in a clinical trial but concomitant treatment with pertuzumab was allowed.
Sociodemographic and clinicopathologic characteristics of patients such as age, profession, marital, educational and financial status, smoking habits, comorbidities, type of surgery, disease stage, and treatment details were recorded anonymously in a dedicated statistical database.
Questionnaires
The HRQoL was assessed with the QLQ-C30 (Quality of Life Questionnaire-Core 30) and the complementary BR-23 questionnaire as previously described. 14 The Greek-validated version of the questionnaires 15 was administered to the patients after providing informed consent. It was completed anonymously at a single time point during their treatment.
Briefly, the EORTC QLQ-C30 (European Organization for the Research and Treatment of Cancer QLQ-C30) version 3.0 is a standardized, validated questionnaire which incorporates 5 functional scales (physical, role, emotional, cognitive, and social), 9 symptom items (fatigue, nausea/vomiting, pain, dyspnea, insomnia, appetite loss, constipation, diarrhea, and financial difficulties), and a global health status scale.
The complementary breast cancer module QLQ-BR23 comprises 4 functional scales (body image, sexual functioning, sexual enjoyment, and future perspective) and 4 symptom items (systemic therapy side effects, breast symptoms, arm symptoms, and upset by hair loss). 14
QLQ-C30 and QLQ-BR23 scoring guidelines were provided by the EORTC scoring manual. 16 The functional scales and the global health status were scored positively (ie, “very much” is best) in a 4-tier and 7-tier scale, respectively, whereas symptoms were scored negatively in a 4-tier scale. 16
Treatment schedules and patient groups
Patients were treated with standard therapeutic protocols outside a clinical trial. In the adjuvant setting, patients received the following every 3 weeks: sequential therapy with 4 cycles of doxorubicin/cyclophosphamide, 4 cycles of docetaxel/trastuzumab, and 14 cycles of trastuzumab as previously reported. 17 In the first-line metastatic setting, patients were treated every 3 weeks with docetaxel/trastuzumab followed by maintenance trastuzumab as previously described. 18 In the neoadjuvant setting, the therapeutic protocol applied included doxorubicin, paclitaxel, and CMF/trastuzumab. 19 Patients with estrogen receptor–positive disease received endocrine therapy as per guidelines. 20
Based on the timing of questionnaire completion, patients were allocated into 3 groups. Group A comprised patients receiving subcutaneous trastuzumab ± chemotherapy ± endocrine therapy, group B intravenous trastuzumab ± pertuzumab ± chemotherapy ± endocrine therapy, and group C chemotherapy without trastuzumab. The latter group included patients with early or metastatic breast cancer that overexpressed HER2 and, who at the time of questionnaire, were not treated with trastuzumab as, for example, when administered anthracycline-based chemotherapy.
The subcutaneous trastuzumab was administered in the fixed dose of 600 mg every 3 weeks and the intravenous formulation in the dosage of 6 mg/kg every 3 weeks after a loading dose of 8 mg/kg. 8
To balance a potential bias on HRQoL due to the concomitant chemotherapy side effects, an additional HRQoL analysis was performed for ≤8 or >8 trastuzumab cycles.
Statistical analysis
The distribution of categorical characteristics was summarized as counts and corresponding percentages, whereas for the distribution of scores, means and standard deviations were estimated. Associations between categorical characteristics were assessed using the Pearson χ2 test. Potential differences in the HRQoL scale scores between groups A and C were investigated via t test. The same statistic was used to test the association of trastuzumab cycles (≤8 vs >8 cycles) and HRQoL scale scores. Furthermore, full factor 2-way analysis of variance (ANOVA) tests were applied for each one of the HRQoL scales, including trastuzumab group and each one of the sociodemographic (age, education, marital status, children, income) and disease-related (smoking, stage of disease, comorbidity, surgery) factors as independent variables. To allow for a possibly different effect of group A to the HRQoL scales within different levels of other factors, an interaction term between group A and the other sociodemographic or disease-related factor was included. In total, nine 2-way ANOVA models for each scale were conducted. In case of a significant interaction, further tests were performed to assess the association of group A and HRQoL scale within the levels of the interacting factor separately. All analyses were conducted at a 5% level of significance using SPSS v20.0 statistical package (IBM Corporation, Armonk, NY, USA).
Results
From December 2015 to May 2016, 180 patients with early or advanced HER2-positive breast cancer offered standard therapy with trastuzumab in 5 Cancer Units in Athens were asked to participate in this prospective observational study. Seventeen patients did not provide consent. Patients completing the QLQ-C30 and the complementary BR-23 questionnaire were allocated into 3 different groups based on which drug schedule was offered when responded to the questionnaires. Specifically, based on the timing of questionnaire completion, group A comprised patients receiving subcutaneous trastuzumab ± chemotherapy ± endocrine therapy, group B intravenous trastuzumab ± pertuzumab ± chemotherapy ± endocrine therapy, and group C chemotherapy without trastuzumab. Group A (90 patients; 55.21%, subcutaneous trastuzumab) and group B (21 patients; 12.88%; intravenous trastuzumab) included a total of 111 patients receiving trastuzumab either contemporarily with a chemotherapy backbone regimen or as single-agent maintenance treatment after chemotherapy completion with or without endocrine therapy. Group C comprised 52 patients (31.90%) who, at the time of questionnaire completion, were receiving anthracycline-based chemotherapy without trastuzumab.
Patients’ sociodemographic, disease, and therapeutic characteristics according to the treatment group are shown in Table 1. The mean age of patients among the 3 groups was 57.1 years and did not differ significantly. There were some differences among the 3 treatment groups. The subcutaneous trastuzumab group included more patients with basic educational status and low monthly income (€501-€1000) compared with the control group (P = .001 and P = .008). The intravenous trastuzumab group included more singles compared with the other 2 groups (P = .005). Some disease-related differences were also observed among the 3 groups. The subcutaneous trastuzumab group had higher number of patients with locally advanced disease and mastectomies, the intravenous trastuzumab group had more patients with metastatic disease, and the control group had more patients with early-stage disease and breast surgery that occurred within the previous 6 months (P < .05; Table 1). Importantly, in this study, 23.6% of the patients had metastatic disease.
Sociodemographic, disease, and treatment-related characteristics of patients according to trastuzumab group (χ2 test).
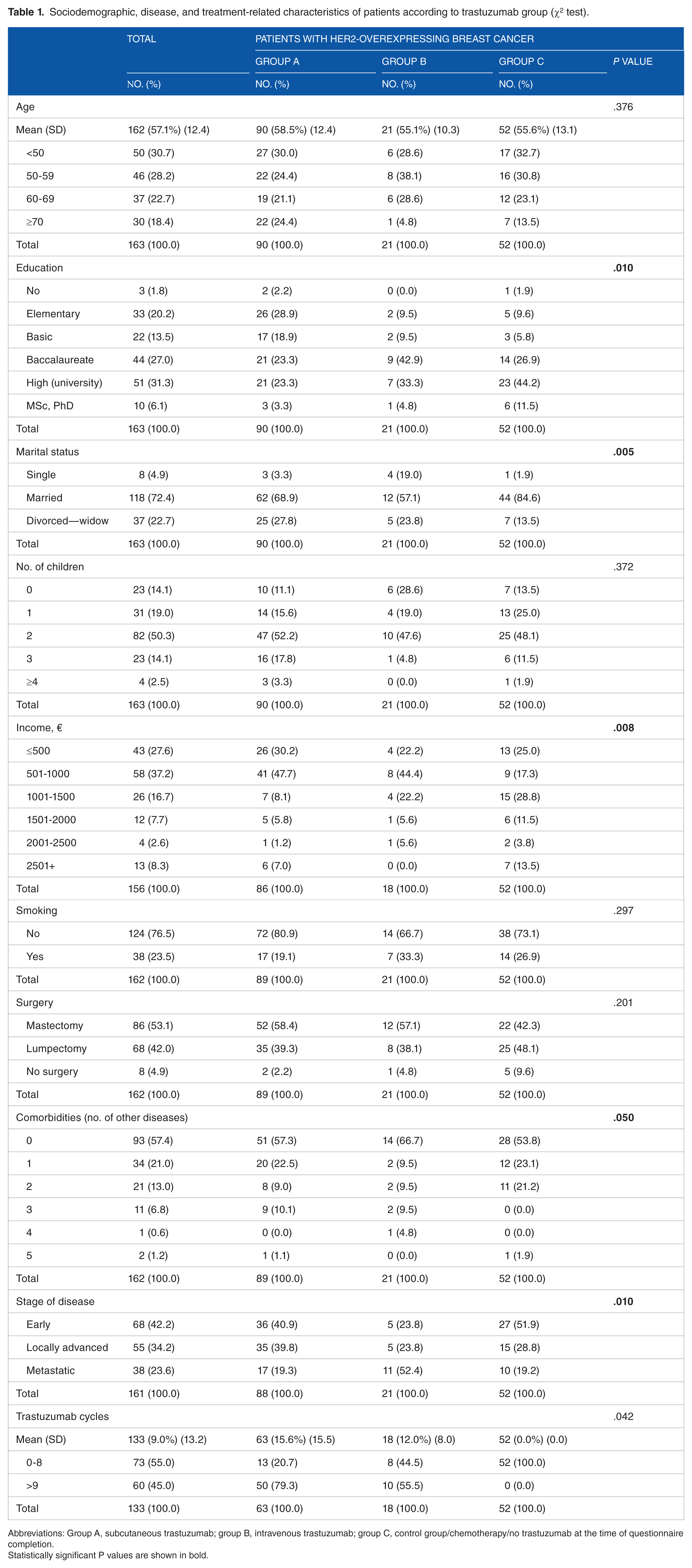
Abbreviations: Group A, subcutaneous trastuzumab; group B, intravenous trastuzumab; group C, control group/chemotherapy/no trastuzumab at the time of questionnaire completion.
Statistically significant P values are shown in bold.
The univariate analyses of HRQoL scales by trastuzumab groups (group A vs group C) are shown in Figure 1. Group A exhibited a statistically significant lower score in cognitive function compared with group C (P = .013). Patients of group A reported significantly more dyspnea (P = .042) but less nausea/vomiting (P = .002) compared with those of group C. Group A patients experienced more breast and arm symptoms compared with those of group C (P = .047 and P = .049, respectively). Importantly, group A patients reported less side effects and toxicity from systemic therapy compared with those of group C (P = .001; Figure 1). No significant differences were found between groups A and B in any of the HRQoL parameters assessed, whereas patients of group B reported less nausea compared with those of group C (P = .031; data not shown).

Mean scores of HRQoL scales by treatment group. HRQoL indicates health-related quality of life; group A, subcutaneous trastuzumab; group C, control group/chemotherapy/no trastuzumab.
The HRQoL responses of patients in group A were further evaluated depending on the number of subcutaneous trastuzumab cycles (≤8 vs >8 cycles). The univariate analyses indicated that diarrhea and systemic therapy side effects mean scores were significantly lower in patients who were administered more than 8 cycles of subcutaneous trastuzumab (P = .049 and P = .015, respectively; Table 2).
Health-related quality of life scoring according to ≤8 or 8> cycles of subcutaneous trastuzumab within group A.

Abbreviations: df, degrees of freedom; t: Student t variable.
Statistically significant P values are shown in bold.
The main effect of each independent variable and the interaction between them were calculated by 2-way ANOVA models and are shown in Supplementary Table 1. Differences in systemic therapy side effects and arm symptoms scores were observed between groups A and C. Patients in group A without comorbidity showed less systemic therapy side effects compared with group C (P < .001). Patients with early or locally advanced disease experienced more arm symptoms in group A compared with group C (P = .049; Figure 2).

Mean scores of HRQoL scales by treatment group, patient, and disease-related parameters. BRAS, arm symptoms; BRBI, body image; BRHL, upset by hair loss; BRST, systemic therapy side effects; DI, diarrhea; EF, emotional function; FI, financial problems; group A, subcutaneous trastuzumab; group C, control group/chemotherapy/no trastuzumab; Herc., trastuzumab; Lump., lumpectomy; Mast., mastectomy; RF, role function; SL, insomnia.
Although the main effects of treatment groups on the scale scores were not significant (group A vs group C), there was interaction with sociodemographic or disease-related factors. Role function mean score, among patients submitted to mastectomy, was significantly higher in patients of group A than of group C (P = .021). Significant interaction was also found for upset by hair loss scores in relation to trastuzumab groups and to absence of comorbidity. Particularly, upset by hair loss mean score was lower for group A (P = .029; Figure 2).
Significant interactions related to sociodemographic characteristics were also identified. Single/divorced patients receiving subcutaneous trastuzumab had higher insomnia score (P < .001) and lower body image score (P = .005). Interestingly, patients receiving subcutaneous trastuzumab and not having children had significant lower score for upset by hair loss (P = .032) and for financial problems (P = .006; Figure 2).
Importantly, the study of the influence of subcutaneous trastuzumab on any of the HRQoL parameters in relation to disease stage indicated no statistically significant negative impact, particularly in the metastatic setting (Table 3).
Impact of subcutaneous trastuzumab on health-related quality of life parameters in relation to disease stage.

Abbreviations: HRQoL, health-related quality of life; F, F distribution variable.
Discussion
Insights into the molecular subtypes of breast cancer have aid to identify 2 subgroups of HER2-positive disease: one overexpressing estrogen receptors (endocrine therapy responsive; luminal B) and one not expressing estrogen receptors (endocrine therapy unresponsive; HER2 enriched) that may respond to anti-HER2 therapy with trastuzumab. 21 This observational study provides real-world data regarding the impact of subcutaneous trastuzumab on the HRQoL of patients with breast cancer receiving treatment in 5 hospitals in Athens, Greece. Patients voluntarily compiled the EORTC QLQ-C30 and the complementary BR-23 questionnaire. Several patient and disease-related parameters were also recorded and analyzed for their potential effect on HRQoL. To the best of our knowledge, no data exist regarding the impact of subcutaneous trastuzumab on HRQoL in patients with metastatic breast cancer, outside a clinical trial.
Chemotherapy regimens universally administered in patients with breast cancer include taxanes, alkylating agents, and anthracyclines. These agents may induce serious side effects, such as bone marrow toxicity, nausea/vomiting, fatigue, and hair loss, compared with a monoclonal antibody. To balance a potential negative effect of the chemotherapy backbone on HRQoL in group A, an additional HRQoL analysis was performed based on the number of the trastuzumab cycle administered at the time of questionnaire compilation. Specifically, HRQoL was separately assessed in patients who had received maximum 8 or more than 8 cycles of subcutaneous trastuzumab at the time of questionnaire compilation, as many clinicians administer chemotherapy for 6 to 8 cycles particularly in the adjuvant setting. As a result, during the first 6 to 8 cycles of treatment patients experienced chemotherapy-related side effects, whereas the following cycles did not.
Patients with HER2-overexpressing metastatic breast cancer pose a distinct challenge as they are often heavily pretreated and have substantial remaining toxicity. It is therefore crucial that further treatment does not exacerbate symptoms. There is lack of real-world data regarding the impact of subcutaneous trastuzumab on the HRQoL of patients with metastatic disease. Data on patients’ preference and HRQoL were derived from the HannaH pivotal study 8 investigating subcutaneous trastuzumab in the neoadjuvant setting and from the PrefHer study 11 where patients received subcutaneous trastuzumab in the adjuvant setting.
Earlier studies 7 had investigated the impact of intravenous trastuzumab on HRQoL in patients with metastatic breast cancer with QLQ-C30 and BR-23 questionnaire and indicated an improvement in fatigue, body image, and social functioning. Recently, the results of the randomized MetaspHer study (NCT01810393), the first clinical trial assessing patient’s preference in metastatic setting, confirmed patients’ preference of subcutaneous over intravenous trastuzumab as reported in early stage by PrefHer study. 22 Our analysis did not find any major differences of impact on HRQoL between subcutaneous and intravenous trastuzumab. Based on the published literature, 23 when pertuzumab was required as first-line treatment, trastuzumab was provided as an intravenous formulation. However, the small sample of patients receiving concomitant pertuzumab and intravenous trastuzumab in our study precludes safe extrapolations.
Trastuzumab in its new subcutaneous formulation may be more practical for the patients compared with the old intravenous one. The preference for subcutaneous trastuzumab was evident in the PrefHer study in which a positive feedback was given in 77% and negative in 22% of participating patients. 11 Real-world data from 7 cancer centers in Germany including patients who had sequentially received subcutaneous and intravenous trastuzumab confirmed the preference of subcutaneous over the intravenous formulation in 70% to 90% of the cases. 24 Quality of life assessment represents one of the most important therapeutic goals and a primary end point in many modern clinical studies. Most of them assess the HRQoL by employing standardized questionnaires such as EQ-5D (Euroqol), SF-6D (Short Form 6D), 15D (15 Dimension), QWB (Quality of Well-being), HUI (Health Utilities Index), AQoL (Assessment of Quality of Life ), QLQ-C30, and FACT (Functional Assessment of Cancer Therapy).25–30
In the CLEOPATRA study, 31 a deterioration of HRQoL was observed in the first 6 cycles when intravenous trastuzumab was administered concurrently with pertuzumab and chemotherapy. The HRQoL improved significantly after the 18th week when chemotherapy was discontinued. It was therefore speculated that HRQoL deterioration was due to chemotherapy toxicity. To balance this effect, HRQoL was assessed in 2 subgroups of patients: those who had received >8 and those who had received ≤8 cycles of trastuzumab. This was based on the current clinical practice of administering chemotherapy during the initial 6 to 8 cycles of treatment. Similar to the CLEOPATRA study, we showed that patients who had received >8 cycles of subcutaneous trastuzumab had less diarrhea (P = .049) and chemotherapy side effects (P = .015).
Our analysis did not show any significant differences in the HRQoL parameters assessed between patients receiving subcutaneous trastuzumab and patients receiving intravenous trastuzumab.
Univariate analysis of our data revealed a deterioration of cognitive function in patients from group A receiving subcutaneous trastuzumab (P = .013) which can only be explained by the large number of patients in this group receiving chemotherapy. 32 It was additionally noted that patients of group A were older compared with those of the control group, a variable that may have its own impact on cognitive function. 33
Although no significant effect of subcutaneous trastuzumab on other functional scales (except for cognitive function) was observed, in multivariate analysis, patients of group A without comorbidity showed a significant improvement in emotional function. It is also noteworthy that in multivariate analysis, patients of group A, who had undergone mastectomy, improved their role functioning compared with patients of group C (P = .021). However, no causality between patient and disease-related factors and differences in functional scales score can be claimed in patients receiving subcutaneous trastuzumab.
As far as symptoms are regarded, the univariate analysis showed a significant improvement of nausea and vomiting and side effects of systemic therapy in patients of group A compared with those of group C (P = .002 and P = .001, respectively). However, more arm symptoms were reported in patients of group A. Interestingly, in multivariate analysis, the presence of metastatic disease negated the adverse effect of the subcutaneous trastuzumab on arm symptoms. This is clinically significant as patients with metastatic disease are often symptomatic due to heavy tumor load and it is vital that treatment does not aggravate symptoms.
Another interesting finding is that patients, without comorbidity, receiving chemotherapy had more toxic effects from systemic therapy compared with those of group A (P < .001). Comorbidity could be a confounding factor as patients might ironically attribute comorbidity-derived symptoms to treatment. In the absence of this confounding factor, it was chemotherapy that had a negative impact on HRQoL but not subcutaneous trastuzumab. This finding underlines the favorable profile of the antibody. Importantly, patients in group A, without comorbidity, experienced less upset by hair loss compared with those of group C.
Although we did not perform a specific cost analysis of the different treatment groups, a previous study has indicated that the cost of treatment with subcutaneous trastuzumab is lower than that with intravenous trastuzumab in the management of patients with early and metastatic breast cancer overexpressing HER2. 10 Hence, the substitution of the intravenous with subcutaneous formulation can produce valuable savings for the Greek health care system, especially in the current economic environment where hospitals’ pharmaceutical budget has significantly been reduced. 10 Furthermore, here, we do not provide a correlation of our results on HRQoL with patients’ survival parameters, as this study has a short time of follow-up and not enough events have occurred for such analysis.
To the best of our knowledge, this is the first study to report real-world data of the impact of subcutaneous trastuzumab on the HRQoL of patients with early and metastatic breast cancer overexpressing HER2. In our study, subcutaneous trastuzumab did not deteriorate any of the HRQoL parameters assessed in all subgroups of patients. However, due to the observational nature of this study, the results should be interpreted with caution as no causality can be claimed and certain differences between treatment groups may be due to chance. Undoubtedly, more reports are needed to further confirm the association of subcutaneous trastuzumab with HRQoL in this particular setting.
Conclusions
Subcutaneous trastuzumab is an effective and patient-friendly drug which does not adversely affect HRQoL parameters, most importantly, in the metastatic setting. Most clinical studies exclude patients of poor performance status and recruit patients under strict inclusion criteria. Our study may therefore provide information that better reflect real-world practices. However, due to the small number of participating patients and the absence of longitudinal follow-up on HRQoL parameters, further studies evaluating the impact of subcutaneous trastuzumab on HRQoL are warranted.
Footnotes
Acknowledgements
The authors thank Ms Fotini Pappa for her valuable support on this project.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Study conceived and planned: JS, EP. Involved in data collection and analyses: all authors. Main preparation of the manuscript: AK, JS. All authors reviewed and approved the final manuscript.
Informed Consent
Informed consent was obtained from all participants responding the questionnaires indicated in the study.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.