
Abstract
Adipose-derived stem cells (ADSCs) are rapidly becoming the gold standard cell source for tissue engineering strategies and hold great potential for novel breast reconstruction strategies. However, their use in patients with breast cancer is controversial and their oncological safety, particularly in relation to local disease recurrence, has been questioned. In vitro, in vivo, and clinical studies using ADSCs report conflicting data on their suitability for adipose tissue regeneration in patients with cancer. This review aims to provide an overview of the potential role for ADSCs in breast reconstruction and to examine the evidence relating to the oncologic safety of their use in patients with breast cancer.
Keywords
Introduction
Breast cancer represents a significant health care burden, with an estimated 1.7 million new cases diagnosed worldwide annually. 1 Approximately 40% of patients with breast cancer require mastectomy to achieve locoregional disease control; recent trends show that higher numbers of women eligible for breast-conserving surgery (BCS) are opting for mastectomy and rates of contralateral and bilateral prophylactic mastectomy are also rising.2–7 Mastectomy is associated with significant aesthetic and psychosocial morbidity, which is improved by breast reconstruction.8,9 Current reconstructive approaches include autologous tissue transfer, prosthetic implants, and biological matrices; however, these approaches remain limited by the potential for complications at the donor and reconstruction sites. Increasing patient expectations for improved aesthetic outcomes means that surgeons are persistently attempting to optimise surgical technique and investigating new and improved approaches to breast reconstruction. This has driven research in the direction of tissue engineering strategies in an effort to develop superior breast reconstruction alternatives. Adipose-derived stem cells (ADSCs) have become the gold standard as a cell source for tissue engineering. 10 They are particularly attractive for breast reconstruction as they exhibit potential for proliferation, preferential differentiation to adipocytes, and maintenance of mature adipose graft volume. However, the oncological safety of their use for adipose tissue regeneration, particularly in patients who have had a malignancy has been questioned.11–15 Concern stems from the characteristics that make ADSCs attractive for tissue engineering, namely, their proliferative and differentiation capacity along with stromal support of cancer cells and delivery of locally inflammatory cytokines and/or growth factors. The aim of this review is to examine the current use of ADSCs in adipose tissue engineering, specifically related to breast reconstruction with a focus on cellular biology; use in breast surgery; oncological safety; and the effect of adjuvant therapies on the regenerative potential of ADSCs.
Breast Reconstruction: Current Approaches and Limitations
The National Institute of Clinical Excellence (NICE) guidelines recommend that all suitable patients undergoing mastectomy for breast cancer should be offered immediate breast reconstruction. 16 Contemporary breast reconstruction approaches can be categorised as follows:
Implant-based reconstruction. Encompassing (a) implant-only reconstructions performed as a 2-stage procedure with placement of a tissue expander which is subsequently replaced with a permanent implant at a later operation or (b) single-stage, direct to fixed-volume permanent implant reconstruction with or without an acellular dermal matrix (ADM);
Autologous reconstruction. Using pedicled tissue flaps (eg, latissimus dorsi [LD] flap), which tend to be myocutaneous, or free tissue transfer (eg, deep inferior epigastric perforator [DIEP] flap), which may be composed of myocutaneous tissue or solely adipose tissue along with perforating vasculature.
Until recently, autologous flap procedures were the most common reconstructive approach. Contemporary trends have seen implant-based reconstruction become more common in the United States and Europe,17–21 possibly explained by shorter and less complicated procedures and increased use of ADMs which have been shown to improve cosmetic outcomes by allowing for better definition of the infra- and lateral mammary folds, reduced capsular contracture rates, and the provision of an additional biocompatible layer between the prosthesis and the overlying skin. 22 Traditionally, single-stage immediate implant-based reconstruction with total muscle coverage of the implant was only achievable in small-breasted women as it is limited by the degree of expansion of the overlying pectoral muscles. This may be overcome by placement of a tissue expander prosthesis which can be inflated over time and replaced by a permanent implant at a second surgery, or alternatively using an ADM with the permanent implant, obviating the need for total muscle coverage. 23 Short-term complications of implant-based reconstructions include seroma, haematoma, infection, and skin necrosis, with implant extrusion and rupture being long-term possibilities.24,25 A significant longer term complication of implants is capsular contracture; the formation of a firm, fibrous tissue capsule surrounding the implant. This constricts over time, resulting in a spherical appearance of the breast which feels firmer than desired, chronic chest wall discomfort, and restricted shoulder rotation. The increasing use of ADMs in implant-based reconstruction has reduced the rate of capsular contracture; however, it remains a significant problem. Capsular contracture has a cumulative incidence of 6% to 18% in non–ADM-assisted implant reconstructions, compared with <5% in ADM-assisted procedures. 26 Post-mastectomy radiation therapy (PMRT) has deleterious effects on aesthetic outcomes and complication rates in implant-based reconstruction as it can affect the symmetry, volume, and projection initially achieved at the time of reconstruction. Post-mastectomy radiation therapy also increases the rates of grade 3 and 4 capsular contracture and reduces the skin quality of the mastectomy flaps 27 leading to an increased risk of necrosis and implant loss.
Although the number of autologous reconstructions being performed has been surpassed by implant-based approaches, this approach still has a prominent role in post-mastectomy breast reconstruction, particularly in patients who have poor skin quality of the mastectomy flaps or for whom delayed reconstruction is preferred. 28 The most widely used pedicled flap was traditionally the LD flap 29 ; however, this is now being surpassed by the DIEP flap, although LD reconstruction is still popular as a salvage or delayed breast reconstruction technique.30,31 Free flaps include DIEP flaps and transverse rectus abdominis muscle (TRAM) flaps, which is also used as a pedicled flap. More recently developed flaps include the superior and inferior gluteal artery perforator flaps, transverse upper gracilis flap, superficial inferior epigastric artery flap, and profunda artery perforator flap. Autologous reconstructions are more cosmetically natural in shape and texture than implants. They provide skin coverage in cases of poor quality of the mastectomy flaps or delayed breast reconstruction. It is believed that DIEP reconstruction is more suitable in patients who will require PMRT as muscular atrophy is a significant complication of LD reconstruction that may occur post-radiotherapy. 32
Although initial complication rates for autologous reconstructions may be higher, they provide a more consistent and durable reconstruction over time. 33 Unfortunately, autologous reconstruction is associated with morbidity at the donor and reconstruction site. Tissue flap necrosis and loss may occur secondary to ischaemia of transferred tissue. Complications may arise from the donor site in the form of, eg, an incisional hernia in the case of a TRAM flap (incidence of 1.2%-8%) or donor site seroma in LD flaps (incidence of 70%-80%).34,35 These operations require longer admissions and recovery times. 36 Autologous flap procedures are also longer and more technically challenging, particularly in the case of DIEP flaps which require the formation of a microvascular anastomosis. 37
Due to the complications associated with current breast reconstruction methods, there is an urgent need to develop superior alternatives that will achieve the aesthetic goal of establishing a natural appearing breast shape. The preferred approach would include an autologous or biocompatible component to minimise foreign body reactions but without the requirement for extensive surgical resection at a donor site. Regenerative medicine approaches hold exciting potential in this regard, and recent efforts have focused on cell-based regeneration of adipose tissue.
Adipose-Derived Stem Cells
There has been increasing interest the potential of autologous fat as a donor source for effective breast reconstruction. Autologous fat is thought to be a superior method of soft tissue augmentation due to a range of properties including biocompatibility and versatility; it is non-immunogenic, has similar mechanical properties to breast tissue, appears more natural than implants or pedicled flaps, and is associated with minimal donor site morbidity. 38 Recent scientific interest has focused on the potential for adipose tissue engineering to generate sufficient volumes of fat for breast reconstruction. Adipose tissue engineering requires a stem cell with the capacity for differentiation into mature adipocytes.
Stem cells are an undifferentiated cell type with multipotent capacity.39,40 Adult/somatic stem cells are multipotent cells within adult tissues which maintain and repair the tissue in which they are found and are capable of differentiating into mature cell types such as osteoblasts, adipocytes, and chondroblasts, in addition to a lack of expression of HLA-DR surface molecules. 41 Adult/somatic stem cells are more abundantly available and avoid the ethical considerations associated with the use of embryonic stem cells (ESCs) for tissue regeneration.10,42 Adult stem cells are found in almost all adult tissues; mesenchymal stem cells (MSCs) have been harvested from tissues such as trabecular bone and periosteum, synovial membrane, skeletal muscle, skin, teeth, and periodontal ligaments.10,43–49 However, the most widely harvested and studied adult stem cells are those from bone marrow, adipose tissue, and peripheral blood. 50 Adipose-derived stem cells are rapidly becoming the gold standard as a cell source for tissue engineering and regenerative medicine. They are contained within the stromal vascular fraction (SVF) of adipose tissue and hypothesised to improve wound healing, tissue regeneration, and graft retention. 51 According to the International Federation for Adipose Therapeutics and Science (IFATS) and International Society for Cellular Therapy (ISCT) joint statement on ADSCs, these cells are identified phenotypically as a CD45−, CD235a−, CD31−, and CD34+ cell population. They differ from bone marrow–derived cells (BMSCs) in that they are positive for CD36 and negative for CD106. They are also capable of trilineage differentiation. 52
Adipose-derived stem cells possess certain advantages over BMSCs and ESCs. They are isolated with less invasive techniques, offer a higher cell yield than bone marrow aspirates (>1000× stem cell number per gram of tissue) or umbilical cord blood,40,53 have significant proliferative capacity in culture with a longer life span in culture than BMSCs,10,54 and possess multi-lineage potential (eg, adipogenic, osteogenic, myogenic, cardiomyogenic, and neurogenic cell types).55–58 Adipose-derived stem cells also have a shorter doubling time and later in vitro senescence than BMSCs. 12
ADSC isolation and preparation
Adipose-derived stem cells are typically isolated from lipoaspirates obtained at liposuction procedures, of which, approximately 400 000 are conducted in the United States annually. Each procedure yields approximately 100 mL to 3 L of lipoaspirate, in which 90% to 100% of ADSCs are viable, which is usually discarded following routine liposuction. 40 To isolate ADSCs, adipose tissue is digested with collagenase, filtered, and centrifuged. The resulting cell pellet is the SVF, containing stromal cells, including ADSCs, which do not contain the lipid droplet in mature adipocytes and have a fibroblast-like morphology. 38 Other cell types present include endothelial cells, smooth muscle cells, pericytes, fibroblasts, and circulating cells such as leucocytes, haematopoietic stem cells, and endothelial progenitor cells. White adipose tissue (WAT) depots vary in stem cell content and properties depending on anatomical site. Adipose-derived stem cells of visceral origin have a higher self-renewal capacity 59 and ADSCs from abdominal superficial regions are more resistant to apoptosis than those from the arm, thigh, or trochanteric depots. 10 This is hypothesised to be secondary to different levels of apoptotic regulators within cells from different depots, such as the Bcl-2 family, in addition to variations in production of paracrine/autocrine factors, eg, insulinlike growth factor 1 (IGF-1). 60 A recent study demonstrated that superficial abdominal cells have higher G3PD activity, aP2, peroxisome proliferator–activated receptor γ (PPAR-γ), and C/EBP-α expression compared with other depots, which may contribute to their resistance to apoptosis. 61 However, the greatest numbers of stem cells are isolated from the arm when compared with depots such as the thigh, abdomen, or breast, postulated to be secondary to this depot having the highest PPAR-γ2 expression.61,62 The optimum WAT depot ADSC harvest and recovery has yet to be elucidated. 63
ADSC characteristics
The immunophenotype of ADSCs is >90% identical to that of BMSCs. 14 One significant difference between the cell types is the presence of the glycoprotein CD34 on the ADSC cell surface.63–65 Adipose-derived stem cells show uniformly positive expression for stem cell markers CD34, CD44, CD73, CD90, and CD105 12 and are negative for CD19, CD14, and CD45. They are positive for pericytic markers CD140a and CD14b and the smooth muscle marker α-smooth muscle actin. Adipose-derived stem cells secrete growth factors such as vascular endothelial growth factor (VEGF), hepatocyte growth factor, fibroblast growth factor 2 (FGF-2), and IGF-1, all of which are involved in angiogenesis and adipose tissue regeneration.54,64 As ADSCs exhibit a similar cell surface immunophenotype as pericytes, it is thought that ADSCs reside within the perivascular region of adipose tissue, between mature adipocytes and adipose extracellular matrix (ECM) near small capillaries.14,66
The transition of a multipotent ADSC into a mature adipocyte occurs in 2 stages. First, by determination and differentiation of the stem cell into a preadipocyte, with subsequent terminal differentiation into a mature adipocyte characterised by accumulation of a single lipid droplet within the cell. 54 This is regulated by the nuclear transcription factor PPAR-γ. The transcriptional programme activated by PPAR-γ is responsible for the regulation of expression of hormone-sensitive lipase, adiponectin, and fatty acid–binding protein 4 (FABP-4). 11 Insulinlike growth factor 1 stimulates the first stage of adipogenesis. Glucocorticoids, insulin, and growth hormone play a role in the stimulation of the early and late phases of adipogenesis. 40 Mature adipocytes are terminally differentiated cells with limited capacity for self-renewal and replacement of mature adipocytes. 63 The responsibility for tissue homeostasis and cell renewal as a result of cells lost due to maturation, damage, or ageing in mature adipose tissue lies with ADSCs. 67 As ADSCs originate from the SVF of digested adipose tissue, they also have the ability to differentiate into vascular endothelial cells and also produce the pro-angiogenic growth factor VEGF, which would be advantageous in the process of vascularising an engineered tissue construct. 10
Due to these characteristics, ADSCs hold considerable potential for the regeneration of fat tissue in reconstructive surgery and can be used as both autologous and allogenic grafts in this context.
ADSCs and Breast Surgery
Fat grafting
Autologous fat grafting has been successfully used in the clinical setting for breast augmentation, filling small-volume defects post–breast-conserving therapy68–72 and contour defects in implant-based breast reconstructions.73,74 Although promising aesthetic outcomes have been demonstrated in this setting, the larger volume of adipose tissue required to reconstruct the breast mound post-mastectomy is more challenging. 75 Autologous fat grafting has had limited success in breast reconstruction with resorption rates ranging from 25% to 80% and complications such as fat necrosis, oil cyst formation, and microcalcifications in patients receiving autologous fat transfer in addition to a primary reconstructive procedure, eg, LD flap 76 or as a filler for small-volume defects post-BCS.77–79 In an attempt to reduce the rate of resorption, cell-assisted lipotransfer, first described by Matsumoto et al 80 in 2006, involves enrichment of autologous lipoaspirates with ADSCs prior to grafting. Enrichment of autologous fat lipoaspirates with ADSCs which have been expanded ex vivo has had more successful outcomes in terms of volume retention, likely as a result of superior graft maintenance due to increased vascularisation and collagen synthesis within the graft. 14 Kolle et al demonstrated residual fat volume of >80% in 10 patients over 121 days using abdominal lipoaspirate enriched with ADSCs that had been expanded ex vivo for 14 days prior to reimplantation into the upper posterior arm. Compared with controls, there were higher amounts of adipose tissue, less necrotic tissue, and newly formed connective tissue in grafts enriched with ADSCs. 81 Yoshimura et al conducted a study in 40 healthy patients undergoing cosmetic breast augmentation, where a mean volume of 270 mL of ADSC-enriched fat was injected into the breast. They reported minimal post-operative atrophy of the injected fat which did not change significantly more than 2 months. Small cystic formations and microcalcifications were observed in some cases; however, the microcalcifications were readily distinguished as benign radiologically. Post-operative computed tomographic and magnetic resonance imaging images showed that transplanted fat tissue survived and breast volume stabilised 2 to 3 months post-operatively. These data indicate that cell-assisted lipotransfer is effective for small-volume breast defects. 82
Tissue-engineered constructs
Recreating the breast mound post-mastectomy is likely to require long-term maintenance of larger tissue volumes in engineered grafts supported by a biocompatible scaffold. 28 There has been limited success with ‘scaffold free’ techniques. This approach involves inducing ADSCs to differentiate into adipocytes and supplementation of culture media with ascorbic acid, to stimulate the production and organisation of ECM to form manipulatable sheets which can be assembled into thicker adipose constructs. Such constructs produced a thickness of 140 ± 14 µm after superimposing 3 adipose sheets. 83 For scaffold-based tissue-engineered constructs, correct scaffold material and design selection will be paramount in overcoming the obstacles of volume retention and vascularisation. Current tissue engineering strategies involve 2-dimensional or 3-dimensional (3D) natural or synthetic scaffold biomaterials that may or may not be seeded with MSCs. 54
Scaffolds allow for the culture of cells in a 3D microenvironment, more accurately mimicking native tissue in vivo. The ‘ideal’ scaffold is one that allows for the production of ‘native-like tissue’, with similar physical and biochemical properties of the tissue it is replacing. Choice of scaffold material is a key consideration in the regeneration of specific tissue types (Table 2). Biomaterials act as the biochemical and biophysical environment to tune the cell response for the specific tissue engineering requirement. The properties of biomaterials (eg, mechanical and chemical functionality) affect phenomena such as cell adhesion, proliferation, and differentiation. 54 The ideal scaffold is also biocompatible, preventing the occurrence of a long-term immune reaction. A highly porous structure is required for vascular ingrowth and cell differentiation. Adipose-derived stem cells undergo morphologic alterations during differentiation to mature adipocytes which includes an increase in diameter from approximately 10 to 100 µm. 84 Pores within the scaffold must be of adequate size to accommodate changes such as these. A scaffold’s stiffness is an important consideration, in that it must be capable of maintaining its structural integrity despite handling during surgical insertion and physiological forces in vivo, yet flexible so that ingrowth of new tissue and vascular structures is possible. In addition to this, biomaterial stiffness influences ADSC differentiation, eg, when stem cells are encapsulated in polycaprolactone (PCL), they are more likely to differentiate towards bone, tendon, and cartilage over other tissue types. 85 Biomechanical properties of the biomaterial must be adjustable to regulate the cellular microenvironment. Degradation properties of a biomaterial are imperative; an ideal scaffold should remain intact for sufficient time for new tissue to form but degrade at a sufficient rate that new ECM can be formed and tissue regenerated. 86 Generally, scaffolds are composed of biomaterials in the form of sponges, hydrogels, 3D or bioprinted constructs, and electrospun scaffolds (Table 2).
Biomaterials can be naturally or synthetically derived. Natural biomaterials used in adipose tissue engineering include collagen, silk, alginate, and gelatin (Table 1). The principle advantage of these biomaterials is their biocompatibility. There are significant differences in the biochemical properties of these biomaterials, eg, collagen, a major component of in vivo microenvironments, is capable of interaction with ADSCs via integrins, unlike alginate, as it does not exist in native ECM and thus does not interact with stem cells. 85 Von Heimburg et al investigated freeze-dried collagen sponges seeded with preadipocytes. These were implanted into immunodeficient mice and preadipocytes differentiated to mature adipocytes in vivo. The constructs were explanted at 3 and 8 weeks and histologic analysis revealed adipose tissue with rich vascularisation attached to the scaffold beneath a thin capsule layer of fibrovascular tissue. This study highlighted the need for the correct scaffold pore size as scaffolds with smaller pore sizes were unable to support preadipocytes differentiation to mature adipocytes. Developing adipocytes have the potential to grow to a diameter of 100 µm. A narrow pore size can restrict growth and differentiation of preadipocytes. 87 A study on HYAFF11 sponges, a derivative of hyaluronic acid, concluded that these were superior to collagen sponges regarding cellularity achieved in adipose tissue engineering. 88 This has been identified as a suitable scaffold material for the culture and in vivo differentiation of ADSCs.89,90
Natural biomaterials previously studied as scaffolds in adipose tissue engineering.
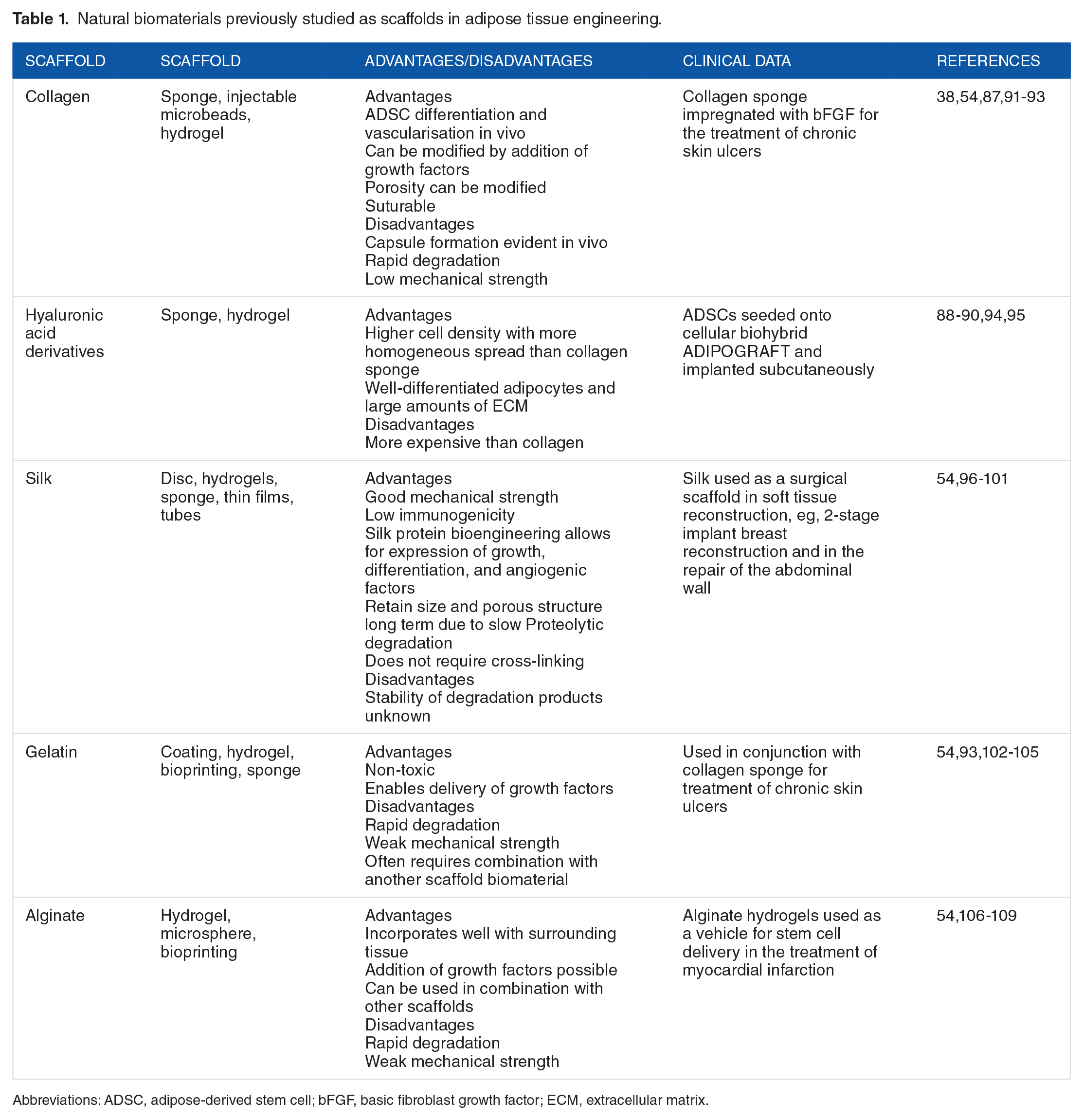
Abbreviations: ADSC, adipose-derived stem cell; bFGF, basic fibroblast growth factor; ECM, extracellular matrix.
Synthetic scaffolds studied in this field include polyglycolic acid (PLGA), polyethylene glycol, PCL, and poly-
Synthetic biomaterials previously studied as scaffolds in adipose tissue engineering.

Abbreviations: 3D, 3-dimensional; ADSC, adipose-derived stem cell.
More recently, biological scaffolds such as decellularised ECM (dECM) have been studied (Table 3). They generate a minimal immunologic and inflammatory response and provide an accurate mimicry of the native tissue microenvironment by preserving the structure of organised tissue and acting as a natural template for the remodelling of regenerated tissue. Scaffolds exist in different biomaterials and different formats based on the individual requirements of the tissue to be regenerated. Pati et al 127 successfully bioprinted a 3D cell laden construct with dECM that showed high cell viability and functionality. A similar biomaterial adipose tissue construct was implanted into a mouse model, which demonstrated positive tissue infiltration, constructive tissue remodelling, and adipose tissue formation. Decellularised adipose tissue (DAT) also holds promise as an adipogenic bioscaffold. One study seeded ADSCs onto DAT bioscaffolds and implanted them into female Wistar rats. At explantation at 12 weeks, 56.1% ± 9.2% of the ADSC-seeded DAT had been remodelled into mature adipose tissue. There was a higher density of blood vessels within the areas of the implant that had been remodelled into mature adipose tissue. 128
Biological scaffolds previously studies as scaffolds in adipose tissue engineering.

Abbreviations: 3D, 3-dimensional; ECM, extracellular matrix.
Vascularisation of regenerated tissue is one of the primary challenges of tissue engineering. Several methods of providing these constructs with adequate blood supply have been investigated. The scaffold within regenerated tissue can play a prominent role in this regard, as scaffold stiffness and porosity are known to influence angiogenesis. 133 In addition, ADSCs themselves are implicated in the regulation of neovascularisation through their modulation of the ECM, or scaffold, by matrix metalloproteinases (MMPs). 134 Some studies have sought to aid vascularisation by the addition of HUVECs to ADSC and scaffold constructs.135,136 Chhaya et al seeded HUVECs onto their adipose tissue construct prior to implantation into a murine model. They observed a 62.3% increase in adipose tissue with the formation of a functional capillary network within the tissue. 113 Vascular pedicles have been used as additional support for an engineered adipose construct within a chamber to facilitate large-scale adipose tissue engineering. 137 In this setting, a chamber allows the vascular pedicle to induce intense vasculogenesis to maximise cell survival. 84 Dolderer et al 138 demonstrated a 10% to 15% increase in adipose tissue volume over a 20-week period using this approach; there was no evidence of hypertrophy, fat necrosis, or atypical changes in the regenerated tissue. Findlay et al 114 was successful in generating up to 56.5 mL of adipose tissue by implanting bilateral 78.5-mL chambers subcutaneously in the groin of a pig which enclosed a fat flap based on the superficial circumflex iliac pedicle for 22 weeks. Implantation of a scaffold prior to ADSC/adipose tissue to allow for ingrowth of new vessels among the scaffold has been investigated. ‘Additive biomanufacturing’ used delayed fat injection into a custom-made scaffold implanted in minipigs for 24 weeks after a period of prevascularisation. The prevascularisation + lipoaspirate group had the highest relative area of adipose tissue on explantation (47.32% ± 4.12%) which was similar to native breast tissue (44.97%±14.12%). 122 These studies represent the largest volumes of adipose tissue engineering in vivo.
The transition to large animal studies and the generation of larger, more clinically relevant volumes of adipose tissue present an exciting prospect for translation of a tissue-engineered breast reconstruction to the clinical setting. However, the evidence for the oncological safety of using ADSCs in patients who have been treated for breast cancer is limited and requires further investigation before the knowledge and techniques generated through these studies can be considered for application in post-mastectomy reconstruction. 39
Oncologic Safety Considerations
Despite the promising early results of ADSCs in breast lipofilling and small-volume reconstruction, its application towards post-oncologic reconstruction should be approached with caution. The concern regarding use of autologous ADSCs in this setting stems from the very same characteristics which make them so attractive for tissue regeneration. Adipose-derived stem cells may potentially contribute to stromal support for cancer cells and deliver locally inflammatory cytokines and/or growth factors, thus facilitating residual cancer cell survival and growth.
Tumour microenvironment
Breast cancer grows in close anatomical proximity to adipose tissue. The ‘tumour microenvironment’ consists of a complex signalling network which influences the behaviour of both resident stem cells and tumour cells. 46 It is composed of all cells surrounding the tumour including endothelial, inflammatory and immune cells, adipocytes, myoepithelial cells, and fibroblasts in conjunction with their ECM.139,140 Understanding the complexity of tumour-stromal interactions will enhance our understanding of how ADSCs may interact with the tumour microenvironment. Numerous autocrine, paracrine, and exocrine pathways in this environment have been described as a role-playing factor in breast cancer. 47
A subset of adipocytes known as ‘cancer-associated adipocytes’ (CAAs) have been shown to play an active role in tumour progression and metastasis. 141 Cancer-associated adipocytes are mature adipocytes that have dedifferentiated into preadipocytes through loss of their lipid droplet and adopted a fibroblastic morphology. 11 This cell type increases tumour growth, tumour invasion via greater epithelial-mesenchymal transition (EMT) 14 and results in a radio-resistant breast cancer phenotype. 13 Several inflammatory cytokines are thought to be involved in this process, eg, tumour necrosis factor α (TNF-α), interleukin (IL)-1, IL-6, IL-11, leukaemia inhibitory factor, IFN-γ, oncostatin M, and ciliary neurotrophic factor. They have been observed to both inhibit stem cell commitment and differentiation towards adipogenesis and may be implicated in adipocyte dedifferentiation. 67
In order for cancer to progress, it requires stem cells and partly differentiated progenitor cells to be recruited from local and distant sites and angiogenesis, both of which occur due to release of factors by the inflammatory and hypoxic tumour microenvironment. 142 Adipose-derived stem cells have a role in angiogenesis and localise to sites of injury and contribute to revascularisation. 64 Epithelial-mesenchymal transition plays a major role in tumour development and benign resident and stromal cells recruited to the area are implicated in early cancer development and metastasis. 39 These stromal cells within the tumour microenvironment are collectively known as ‘cancer-associated fibroblasts’. They secrete pro-angiogenic and anti-apoptotic factors, contributing to tumour development. Zhang et al 59 demonstrated that ADSCs mobilise and migrate through the systemic circulation to distant tumours resulting in acceleration of tumour growth. This action appears to be unique to ADSCs and is not observed in similar models using bone marrow-derived or lung-derived MSCs. 143 It remains unclear whether ADSCs used in wound repair are capable of migration to distant tumours. Altman et al investigated whether ADSCs had any effect on the growth and progression of distant tumours when applied to a skin wound; comparing tumour growth in vivo (murine model) when breast cancer cells and ADSCs were co-injected and when the ADSCs were introduced on an ADM at a distant skin wound. Although there was an increase in tumour volume when ADSCs were co-injected, there was no such effect observed in cases where the ADSCs were introduced at the skin wound, indicating that that the wound microenvironment is capable of retaining ADSCs and preventing their migration to distant malignant sites. 144
Adipose-derived stem cells, both local and those recruited to a breast tumour site, are capable of dedifferentiation into CAAs. Several genes involved in cell growth, ECM deposition/remodelling, and angiogenesis are expressed at higher levels in local breast ADSCs than those isolated from adipose tissue or bone marrow, suggesting that the breast adipose depot plays a more intimate role in breast cancer progression. 145 Coculture of breast cancer cells and preadipocytes prevents adipogenic differentiation, supporting the hypothesis that ADSCs are part of the CAA population within breast cancer tumours. 146
Extracellular matrix secreted by adipocytes also has a role in breast cancer progression.147–150 Adipose tissue ECM is rich in collagen VI, 151 which is upregulated in tumorigenesis and promotes GSK3β phosphorylation and increased β-catenin activity in breast cancer cells. Breast tumour growth has been shown to be reduced in a collagen VI–deficient murine model. Breast cancer cells cocultured with adipocytes and injected subcutaneously in the mammary fat pad of a nude mouse resulted in larger tumours than breast cancer cells cocultured with fibroblasts and Matrigel. 152 Matrix metalloproteinases are enzymes involved in the degradation of ECM proteins during growth and tissue turnover. Higher levels of MMP-11 are expressed by adipocytes at the invasive front of human breast cancers secondary to ECM remodelling in this area. MMP-11 is a negative regulator of adipogenesis and may be responsible in part for the ‘dedifferentiation’ of adipocytes. 13 Certain cell surface markers, eg, CD44, mediate reorganisation of ECM components, by anchoring MMPs to the cell surface. Therefore, ADSCs play a direct role in ECM remodelling occurring during tumour growth. 12 Adipose-derived stem cells are involved in the desmoplastic reaction occurring within tumours through their involvement with MMPs. Desmoplasia results in the recruitment of myofibroblasts, a cell type frequently detected in breast cancer tumour stroma. Adipose-derived stem cells express α-smooth muscle actin, a marker for myofibroblasts, suggesting that ADSCs are a source of tumour myofibroblasts. 14 These intricate interactions within the tumour microenvironment illustrate how ADSCs may create a favourable milieu for tumour growth.
ADSC secretome
Adipose-derived stem cells possess tumour-supporting functions through provision of migratory cells which secrete trophic factors, increasing vascularisation and contributing to survival and proliferation of malignant cells. 140 Adipose tissue secretes cytokines known as adipokines, eg, TNF-α, IL-6, IL-8, PAI-1, MCP-1, adiponectin, resistin, leptin, insulin growth factor, and steroid hormones, some of which have been studied in relation to cancer, 142 eg, leptin upregulates activity in signalling pathways in breast cancer tumours that play a role in proliferation (Figure 1). 13

Adipogenesis in tissue-engineered adipose construct and produced adipokines. ADSC indicates adipose-derived stem cell; FGF, fibroblast growth factor; IGF, insulinlike growth factor; IGFBP, IGF-binding protein; IL, interleukin; MMP-1, matrix metalloproteinase 1; NF-κB, nuclear factor κB; PDGF, platelet-derived growth factor; TGF-β, transforming growth factor β; TNF-α, tumour necrosis factor α; VEGF, vascular endothelial growth factor.
Many adipokines are pro-inflammatory, are secreted in increasing amounts in obese individuals, and are involved in the promotion of tumour growth, locally at the tumour site and, via communication with distant sites, in particular TNF-α, IL-6, IL-8, and MCP-1.11,13,59 Factors known to play a significant role in tissue regeneration, neovascularisation, carcinogenesis, and tumour progression found in high-risk patients, expressed by MSCs and ADSCs, include FGF, ILs, IGF-binding protein, platelet-derived growth factor, transforming growth factor β (TGF-β), TNF-α, and VEGF. 39
Adipokines induce transcriptional programmes implicated in promoting tumorigenesis which include increased cell proliferation through IGF-2, FOS, JUN, and cyclin D1; invasive potential through MMP-1 and AFT3l; cell survival via A20 and nuclear factor κB; and angiogenesis. 152
Adipose-derived stem cells may also influence tumour growth and progression through exertion of immunomodulatory effects on T cells within the tumour microenvironment due to the secretion of cytokines such as prostaglandin E2, TGF-β1, indoleamine 2,3-dioxygenase, hepatocyte growth factor (HGF), and inducible nitric oxide synthase. Adipose-derived stem cells may be responsible for abnormal CD4+ T-cell activation and function. 15 Razmkhah et al investigated the expression of IL-4, IL-10, and TGF-β1 in ADSCs isolated from breast tissue in patients with cancer and healthy controls and whether these cytokines had an influence on peripheral blood lymphocytes. Messenger RNA expression of IL-10 and TGF-β1 in ADSCs from patients with cancer was higher than those isolated from healthy patients. The conditioned media from ADSCs of patients with stage III disease was used to culture ADSCs from healthy patients and caused IL-4 and IL-10 expression to increase. Therefore, ADSCs may assist in protecting the breast cancer from anti-tumour immune responses by providing a source of anti-inflammatory cytokines within the tumour microenvironment and their potential to act as regulatory T cells. 15
Breast adipose tissue functions in oestrogen biosynthesis and high local levels of oestrogen are related to breast cancer development and progression. 153 Oestrogen upregulates growth factors such as epidermal growth factor receptor and Akt phosphorylation, sustaining breast cancer growth. 154 Oestrogen plays a role in the increased aggressiveness of breast cancer in obese individuals. 155 Adipose-derived stem cells isolated from abdominal adipose tissue of those with a body mass index >30 enhance breast cancer cell line proliferation and tumorigenicity in vitro and in vivo. Changes in the oestrogen receptor alpha and progesterone receptor gene expression profile correlated with these changes. Obesity caused changes in several adipogenic genes including leptin, and women with ER+/PR+ tumours that had high leptin expression had a poorer prognosis. 156
The effect of ADSCs on breast cancer: in vitro and in vivo evidence
As discussed above, ADSCs have the potential to influence the behaviour of breast cancer cells due to secreted adipokines and their effect on the tumour microenvironment. However, there are conflicting reports on the manner in which this influence is exerted.
The role of adipokines was demonstrated by Dirat et al 141 who reported increased invasiveness of both human and murine breast cancer cells associated with overexpression of proteases, including MMP-11, and pro-inflammatory cytokines (IL-6, IL-1β), when cocultured with adipocytes. Zhang et al 157 demonstrated that ADSCs increased the motility of MCF-7 breast cancer cells in vitro through the secretion of the chemokine CCL5.
However, it has been suggested that ADSCs may only promote the growth and progression of active breast cancer cells and do not activate dormant residual breast cancer cells; therefore, the use of ADSC regenerative therapies should therefore be delayed until there is no evidence of active disease. 158
Indeed, there is a lack of consensus on the reported effects of ADSCs on tumour behaviour as some studies have demonstrated an ability by ADSCs to inhibit tumour growth in vitro. Adipose-derived stem cells are capable of inducing cell death in pancreatic adenocarcinoma, hepatocarcinoma, colon, and prostate cancers.159,160 Adipose-derived stem cells cultured at high density and their conditioned media have been shown to be capable of suppressing the growth of MCF-7 cells in vitro, as a result of IFN-β expression by ADSCs in high-density culture. 161
There is a similar discordance in results from in vivo studies. Increased tumour growth and metastasis in a murine model was observed when ADSCs from WAT were co-injected with triple-negative human breast cancer cells. Tumour progression was similar in the groups that were co-injected with human breast cancer cells and unprocessed lipoaspirate and those co-injected with human breast cancer cells and purified CD34+ WAT ADSCs, suggesting that most of the tumour progression effects of human WAT are due to the ADSC fraction. A follow-up metastasis study demonstrated that mice which had a primary breast cancer tumour removed and were injected with ADSCs alone had a higher rate of axillary and lung metastasis than mice which had CD34− cells injected post-resection. Immunohistochemistry revealed that human cells generated from ADSCs were incorporated into the tumour vasculature. These effects have never been observed using bone marrow–derived stem cells, suggesting that these functions are unique to ADSCs. 53
Conversely, the ability of ADSCs to inhibit MDA-MB-231 breast adenocarcinoma cells was demonstrated by Sun et al. 162 The authors using a murine cancer model similar to prior studies demonstrated that ADSCs did not appear to increase tumour progression or metastasis and actually had the effect of inhibiting breast cancer cells by apoptosis.
Experimental data, both in vitro and in vivo, are conflicting regarding the effect of ADSCs on breast cancer, and there is a lack of consensus on this subject. Data from their use in the clinical setting must also be considered when evaluating the oncological safety of their use in patients with breast cancer.
ADSCs – Clinical Use in Patients With Breast Cancer
As outlined above, the properties of ADSCs which are advantageous tissue regeneration, including immune-modulatory, pro-survival, pro-angiogenic, and anti-apoptotic effects, immunosuppression, tissue growth, and cellular homing are also dysregulated in tumour progression and metastasis, thus raising questions regarding the oncologic safety of these cells in breast reconstruction post-mastectomy.39,163,164 In addition to experimental mechanistic data, the clinical evidence relating to the safety of ADSC use in patients with breast cancer has been assessed in both retrospective and prospective series of patients undergoing ADSC-enhanced fat grafting (Table 4).
Studies of breast cancer recurrence post-autologous fat grafting procedures.

The oncological safety of autologous fat grafting has been assessed in multiple prospective and retrospective series of patients who had undergone BCS or mastectomy (Table 4). Petit et al reported local recurrence rates of 1.35% for the mastectomy group and 2.19% in the BCS group. Only patients with intraepithelial neoplasia (n = 37) who underwent autologous fat grafting demonstrated an increased rate of local recurrence (10.8%). 165 A follow-up–matched cohort study investigating fat grafting in 59 patients with intraepithelial neoplasia concluded that there is a higher risk of local recurrence in this patient cohort compared with age-matched and stage-matched controls (n = 118). 166 Although the results of these studies are significant, they are retrospective series in a single centre with small numbers of patients. Several other explanations may exist for this increased rate of recurrence: there was a higher rate of recurrence in those patients with close or positive surgical margins in the study group, and there was an increased rate of recurrence in those with a higher grade tumour. There is no other published study that reports such an increased rate of breast cancer recurrence after autologous fat grafting. Further prospective investigation of the risk that intraepithelial neoplasia poses in autologous fat grafting is required, in larger numbers of patients with longer follow-up. The largest retrospective study to date which focused on ADSCs use in patients with a history of breast cancer was conducted by Kronowitz et al. The authors conducted a retrospective matched controlled study of 719 patients undergoing lipofilling of the breast post-tumour resection. There was no increase in locoregional or systemic recurrence or of a second breast cancer.167,168 In a separate retrospective study conducted by Petit et al, 169 which focused on local recurrence consisted of 370 patients who underwent mastectomy (1.35%) and 143 patients who underwent BCS (2.19%), the authors concluded that there was no difference in recurrence rate of either group when compared with controls. Several other studies showed similar rates of recurrence in patients who solely underwent BCS when compared with controls. 170 Therefore, there does not appear to be any difference in the rate of recurrence in patients undergoing autologous fat grafting post-BCS or mastectomy and reconstruction.
The RESTORE-2 trial prospectively assessed the oncological safety of ADSC-enriched fat grafting in patients undergoing BCS with defects of up to 150 mL. In total, 67 patients reported high levels of satisfaction with the cosmetic outcomes. No incidences of local recurrence were reported within 12 months of the procedure; however, this is not a sufficient follow-up time to adequately investigate the oncologic safety of this technique. 121
Delay et al analysed outcomes in 880 patients in a retrospective review, who underwent fat grafting. This review of the practice of 4 surgeons demonstrated that after 10 years of follow-up, there was no increased risk of cancer recurrence or new cancer development. 77 They also reported that the radiological appearance of the breasts post-lipofilling was usually of normal breast tissue; however, some images showed fat necrosis, which was easily distinguished from neoplastic lesions. Systematic reviews on the topic conclude that autologous fat grafting appears to be oncologically safe with low rates of complications and satisfactory patient and surgeon satisfaction.186–189 However, questions remain with many of these previous mentioned studies as limited information is given about tumour size, lymph node status, and chemotherapy regimens, all of which would affect the locoregional recurrence (LRR) rate. Another key factor is the follow-up time, which varied considerably between studies. The largest study published by Kronowitz et al had a follow-up time of 5 years; in comparison, Petit et al reported a follow-up time of a little more than 2 years.167,169 The timing of the autologous fat grafting after surgery is another area for consideration; deciding on an optimal time point post primary surgery for autologous grafting with ADSCs may indeed be the primary decision in preventing recurrence. It is due to these issues that all authors call for well-designed randomised controlled trials with adequate follow-up to adequately address these issues and to exercise caution in performing these procedures in high-risk patients. A phase 3 multicentre randomised controlled trial is currently underway in France with the goal of investigating this issue (GRATSEC NCT01035268).
One further suggested explanation for the discrepancies between basic science and clinical studies in relation to oncological safety is the higher concentration of ADSCs used in vitro than clinically, which raises further concerns for the use of ADSCs in tissue engineering strategies which would require high concentrations of ADSCs to generate large volumes of adipose tissue.75,186,189–191
Adjuvant Therapy Considerations
If ADSC-based breast reconstruction/regeneration approaches are to be translated to the clinical setting for patients with breast cancer, in addition to addressing oncologic safety, the potential effect of tissue regeneration using ADSCs on the efficacy of adjuvant therapy and the effects of adjuvant therapy on the success of tissue regeneration and breast reconstruction also require investigation.
Cytotoxic chemotherapy
After neoadjuvant chemotherapy for breast cancer, poor wound healing is a significant problem for patients undergoing subsequent tumour resection and reconstruction. It is postulated that chemotherapy influences ADSC’s ability to function effectively. Charon et al were the first to investigate the effect of paclitaxel on ADSCs. They found that paclitaxel inhibits proliferation and differentiation of ADSCs and can induce apoptosis. Paclitaxel can also impair wound healing in chemotherapy patients due to its inhibition of endothelial differentiation in ADSCs. 192 Harris et al treated ADSCs isolated from human periumbilical fat with paclitaxel at various concentrations in vitro. Adipose-derived stem cells from rats treated with paclitaxel were also investigated. Paclitaxel treatment resulted in increased ADSC apoptosis and decreased cell proliferation and migration and inhibited ADSC multipotent differentiation in both human and rodent cell populations. However, human and rodent ADSCs recovered differentiation abilities after cessation of paclitaxel treatment. 193 Chen et al 194 demonstrated that ADSCs induce doxorubicin resistance in MDA-MBA-231 triple-negative breast cancer cells through IL-8 secretion. However, ADSCs are shown to cause increased chemosensitivity to doxorubicin and 5-flourouracil in SKBR3 Her2 breast cancer cell lines. 195 Beane et al discovered that vincristine, cytarabine, and etoposide all inhibited the proliferative ability of ADSCs, although the authors did note that variability did exist between drug type and concentration. In direct comparison, it was found that ADSCs’ growth or viability was not inhibited by any concentration of methotrexate. 196
Overall, it would appear that each chemotherapeutic agent interacts with ADSCs in a distinct manner and each would warrant investigation. What is clear, however, is that harvesting and storing ADSCs prior to beginning any chemotherapeutic regime may be the best approach to maximise their benefit in terms of adipose regeneration.
Targeted therapies
Trastuzumab
An in vitro coculture study and in vivo analysis of Her2 breast cancer found that adipocytes play a role in resistance of Her2-overexpressing breast cancer cells to trastuzumab. Whether this effect is exclusive to mature adipocytes or whether ADSCs are capable of similar promotion of breast cancer cell resistance to trastuzumab requires further investigation. 197
Hormonal therapy
Tamoxifen is the most widely used adjuvant hormonal therapeutic agent for the treatment of breast cancer. 198 Pike et al isolated human ADSCs and treated them with various concentrations of tamoxifen. This resulted in increased apoptosis, decreased proliferation of human ADSCs, and a decrease in differentiation capability into adipocytes and osteocytes and inhibited ability to form cords in Matrigel, suggesting that patients treated with tamoxifen may have decreased ADSC graft survival. 199 This is a cause for concern and could potentially mean women may not be suitable for ADSC-based tissue regeneration while being treated with tamoxifen. In the clinical setting, Kronowitz et al 167 showed a significant increased risk of LRR in patients who received hormonal therapy after autologous fat grafting. Although it is unclear what this increased risk is due to, Waked et al 47 hypothesised that it may be due to a stimulatory effect of hormonal therapy on the communication between breast cancer cells and ADSCs or more worryingly that hormone receptor–positive patients with breast cancer may be at increased risk of LRR post-autologous grafting. This is a hypothesis that also requires further investigation.
Radiotherapy
Post-mastectomy radiotherapy can result in complications such as recurrent infection, impaired healing, fibrosis, contracture, and lymphoedema. Adipose-derived stem cells display an element of radio-resistance in comparison with other components of the SVF. 200 This may be secondary to a superior ability of MSCs to retain their proliferative capacity due to their enhanced repair mechanisms for damaged DNA compared with terminally differentiated cells. Lower metabolic demands of ADSCs compared with mature adipocytes result in protection from hypoxia and apoptosis, preserving them to perform regenerative functions. 200 There are several possible mechanisms by which injection of ADSCs into a previously irradiated area can overcome radiation-induced injury: ADSC adipogenic differentiation; increasing perfusion of injured tissues through induction and paracrine promotion of angiogenesis; exerting an anti-oxidant effect against hypoxia, ischaemia reperfusion, and reactive oxygen species–induced damage by adipokine release; modulating immune responses, inflammation, and improving wound healing; modulating granulation tissue, fibrosis, ECM remodelling, and improve epithelialisation; secreting lymphangiogenic factors, improving or reversing lymphoedema in damaged tissues; and recruiting endogenous stem cells via a homing chemokine gradient. 200 A study of cocultured ADSCs and normal human fibroblasts (NHF) exposed to radiation shows promise for the use of ADSCs in breast reconstruction. Monocultures of ADSCs and NHFs showed reduced cell proliferation after radiation exposure; however, reduced impairment of cell proliferation was seen in the cocultured cells after radiation exposure. Gene expression of MMPs was also improved in the cocultured group. 201 Microvascular endothelial cells were then added to the coculture. The levels of cytokines and adhesion molecules, IL-6, bFGF, ICAM-1, and VCAM-1, in the coculture supernatants were significantly less affected by irradiation than monocultures. 202
Adipose-derived stem cells improve graft retention in irradiated scalps of mice. Fat grafts supplemented with ADSCs demonstrated superior volume retention, structural qualities, and vascularity. 203 In a study of the effect of ADSCs on flap survival in irradiated tissues in rats, increased flap viability was observed in the ADSC-injected irradiated group compared with the control radiation only group. The mechanism may be both neovascularisation and vasodilation in addition to endothelial repair. 204 A clinical study of the treatment of radiotherapy-induced injury by lipoaspirate-containing ADSCs showed improved outcomes for 20 grade 3 or 4 patients on the Late Effects Normal Tissue Task force - Subjective, Objective, Management, Analytic (LENT-SOMA) scale measuring severity of radiation effects, with improvement or remission of symptoms in all 20 patients. 205
Further investigation of the effects of adjuvant cancer therapies, both cytotoxic and targeted on ADSC-based tissue regeneration, is required before this method of breast reconstruction can be considered for translation into the clinical setting.
Future Direction
Although there has been significant advancement made in the field of adipose tissue engineering, and in the use of ADSCs as a cell source in this regard, there are several outstanding issues that need to be addressed before adipose tissue engineering can be used to its full potential in breast reconstruction. Most basically, the isolation techniques used to produce lipoaspirate require refinement to optimise cell yield, survival, and viability. Investigation of this has thus far revealed that high-speed centrifugation is harmful to lipoaspirates and that washing the adipose tissue to separate it from blood and infiltration solutions may improve outcomes. 206 However, as of yet, there is no consensus on the protocol for adipose aspiration. 207 The optimal adipose depot also needs to be identified. First, as the source of greatest ADSC cell yield, and second, as the one that is oncologically safe. As previously discussed, several genes involved in cell growth, ECM deposition, or remodelling and angiogenesis are expressed at higher levels in local breast ADSCs than those isolated from adipose tissue or bone marrow, suggesting that the breast adipose depot plays a more intimate role in breast cancer progression.
The question of oncological safety of ADSCs needs to be definitively answered through investigation of the adipokines produced by this cell type and elucidating the role that these adipokines play in EMT and the tumour microenvironment. The role of ADSCs in stromal support for tumours will also require scrutiny in future experiments. Patient factors will also influence the oncological safety of ADSCs. Many adipokines are pro-inflammatory and are secreted in increasing amounts in obese individuals and are involved in the promotion of tumour growth, which begs the question, whether ADSCs are used in breast reconstruction, are obese individuals are greater risk of cancer recurrence? In addition, are there any other patient characteristics that place them at a greater recurrence risk?
Timing of reconstruction with ADSCs also requires careful consideration. It has been suggested that ADSCs may only promote the growth and progression of active breast cancer cells and not dormant residual breast cancer cells. Therefore, should the use of ADSC regenerative therapies be delayed until such time that there is no evidence of active disease, and what is the optimal time point post-curative surgery for reconstruction with ADSC technology to prevent recurrence?
Several clinical studies and systematic reviews have concluded that reconstruction techniques using autologous fat and ADSCs are oncologically safe with no increased rate of LRR. However, data such as tumour size, lymph node status, and adjuvant therapy regimens are scant. These factors are highly influential on the rate of recurrence and so need to be studied in greater detail in clinical trials of breast reconstruction techniques involving ADSCs.
Finally, there has been limited investigation of the relationship between ADSCs, adjuvant therapies, such as chemotherapy and radiotherapy, and cosmetic and oncological outcomes. The potential effect of tissue regeneration using ADSCs on the efficacy of adjuvant therapy and the effect of adjuvant therapy on the success of tissue regeneration and breast reconstruction requires elucidation.
Conclusions
With rates of mastectomy showing no sign of decline, novel, safe, functional, and cost-effective methods of breast reconstruction are required. Adipose tissue has been shown to be a valuable source of MSCs that hold immense potential for modern tissue engineering strategies in the field of breast reconstruction. However, there are still several pertinent research questions outstanding regarding the best adipose tissue depot from which to isolate ADSCs and how to generate and sustain volumes of mature adipose tissue to reconstruct the breast mound. Furthermore, the oncological safety of implanting ADSCs into patients with breast cancer due to the risk of cancer recurrence and what effects do adjuvant therapies have on ADSC isolation and their function on implantation remain to be fully elucidated. Well-designed randomised controlled trials will be required to accurately answer these issues. However, it is currently widely believed that ADSCs will be central to the development of novel future techniques in adipose tissue engineering.
Footnotes
Peer Review:
Three peer reviewers contributed to the peer review report. Reviewers’ reports totalled 487 words, excluding any confidential comments to the academic editor.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
All authors have made substantial contributions to the drafting or critical revision of this manuscript and have given final approval of the version to be published.