
Abstract
Background:
The study aims to evaluate the current state and tendencies in multiple primary breast cancer incidence, behavior, and treatment in Ukraine.
Methods:
A total of 2032 patients who received special treatment at the Department of Breast Tumors and Reconstructive Surgery of the National Cancer Institute from 2008 to 2015 were included in the study. Among them, there were 195 patients with multiple primary malignant neoplasms: 54.9% patients with synchronous cancer and 45.1% patients with metachronous cancer. The average age of patients was 46.6 years, and the percentage of postmenopausal women was 63.1%. Among patients with synchronous cancer, there were 56.1% patients with only breast localizations and 43.9% with combination of breast and other localizations, and among patients with metachronous cancer, there were 46.6% patients with only breast localizations and 53.4% with combination of breast and other localizations. All the patients were evaluated in terms of aggressiveness of the disease, survival rates, as well as risk factors and treatment options.
Results:
A more aggressive course of breast cancer is observed in patients exposed to radiation from the Chernobyl accident under the age of 30 years (P < .01). The clinical course of disease in patients with synchronous cancer is worse and prognostically unfavorable compared with metachronous cancer (P < .01). The course of the disease in patients who underwent mastectomy is worse compared with patients who underwent breast-conserving surgery (P < .01). Plastic and reconstructive surgery in patients with synchronous cancer was proven to be reasonable in terms of increase in survival (P < .01).
Conclusions:
The patients with multiple primary breast cancer should have attentive management and treatment. Multidisciplinary team should concern all the risk factors and provide the most sufficient option of management. This is crucial to continue research in this oncological area.
Introduction
Breast cancer (BC) constitutes 30% to 50% of all other primary malignant growths of women who had primary BC (PBC). The risk is 2 to 6 times more that they will have new primary cancer in contralateral breast during their lifetime,1–3 which constitutes 0.3% to 1% annually.2,4
In current structure of cancer diseases of women in Ukraine, BC takes the first place (19.5%) which causes 20% mortality of all malignant growths. Reproductive organ cancer (corpus uteri and cervix) is among the 6 mostly widely spread nosological forms of women’s cancer. However, the intensity of these diseases among Ukrainian women is almost the same as that in the post-Soviet European countries, and the level of BC (41.7 per 100.00 women, 2014 in Ukraine) is even lower than in some industrialized European countries, such us United Kingdom (95 per 100.00 women, 2012), Germany (91.6 per 100.00 women, 2012), and France (89.7 per 100.00 women, 2012). 5 The latter can be connected with the fact that more women are covered with preventive examination and better quality medical diagnostics in these countries.
Two or more unrelated primary malignant tumors that originate from different organs and occur simultaneously or one after another are called multiple primary malignant neoplasms (MPMNs). They fall into 2 main categories: synchronous MPMNs (SMPMNs) and metachronous MPMNs (MMPMNs). The SMPMNs are defined if the tumors occur simultaneously or within 6 months of one another. If the interval time is more than 6 months, such tumors are called MMPMNs.
Clinically, MPMNs are often confused with metastasis or recurrence of malignant tumors. However, metastatic tumors are derived from the primary lesion, with both showing the same pathological characteristics and similar developmental processes. Conversely, MPMNs refer to the development of a new malignant lesion de novo; their characteristics are completely different from those of the original tumor lesions. 6
The occurrence of MPMN has increased in recent years. Breast cancer represents 30% to 50% of all second primary malignant tumors in women affected by PBC. They have 2 to 6 times higher risk of developing a new primary cancer in the contralateral breast during their life,1–3 corresponding to a risk of 0.3% to 1.0% per year.2,4 There is uncertainty in the literature regarding the prognosis and survival of patients with primary MPMNs compared with primary unilateral BC (UBC).7–12 Debates are held over whether prophylactic bilateral mastectomies are reasonable. Given the importance of this issue, we investigated the clinical features and patterns of occurrence, prognosis, and consequences of MPMNs in patients with breast tumors.
In the modern era, where breast-conserving surgery (BCS) is a viable alternative to mastectomy, patients with BC and their health care providers have to consider the issue of quality of life regarding the type of surgery. The choice of surgical procedure should consider the perceptions of women diagnosed with BC as well as their functional and emotional well-being. A more holistic approach to the patient should be implemented with proper psychological evaluation before and psychological support after the crisis. 13 However, appropriateness of BCS in patients with MPMNs was not studied.
In the literature, there is uncertainty as to the prediction and survival of the sick with metachronous cancer processes compared with primary one-side BC. In view of this, regularities of the occurrence of metachronous processes of the patients with breast tumors are studied in this article, their consequences are estimated and predictions are suggested.
The development of multiple processes can be connected with radiation contamination as a result of the disaster at Chernobyl nuclear power station (ChNPS). Extra radiation-induced cases of PBC were recorded among irradiated woman after atomic bombing of Hiroshima and Nagasaki. 12
The development of the cancer location depended on the age of this population group at the moment of irradiation. Higher tumor incidence was observed among the individuals irradiated at the age of 10 to 19 years. Primary breast cancer incidence was lower among the irradiated people at the age of 20 years. Average latent period, followed by BC, did not depend on the dose and was about 18 years. World literature confirms that BC among women irradiated at the age 19 to 20 years was higher than among those older than 30 years.7–12
In Ukraine, as well as in most industrialized countries, the main cause of women’s mortality from cancer diseases is cancer of reproductive system organs. Besides direct losses of women, including fertility cohort, indirect losses occur—unborn children because of permanent or temporary loss of reproductive function as a result of the disease of this location. In view of this, it is important to study the trend of cancer incidence of reproductive organs of women in Ukraine and their survival, in particular, of the consequences of the disaster of ChNPS, and to determine the volume of indirect demographic losses due to cancer incidence of women of reproductive age.
For a short period of time (2003-2015), the level of cancer incidence of women of reproductive age was constantly growing in Ukraine. The frequency of preliminary BC increased more than by 9% (0.8% annually), reproductive organs depending on localization by 7.5% (ovary cancer) and by 21.3% (corpus uteri), respectively. However, the largest number of malignant growths identified for the first time included BC. The coefficient of disease incidence in this localization exceeded 3 times similar indicators of the 3 main localizations of a reproductive system (cervix cancer, corpus uteri, and ovary).
Objective of the study
To evaluate the predictive impact of adverse factors, optimize approaches to diagnosis and treatment of BC associated with MPMNs, improve life quality and increase life expectancy of such patients, and to estimate the volume of indirect demographic losses due to cancer diseases of women of reproductive age.
Materials and Methods
Diagnostic criteria
We considered synchronous cancer located in the contralateral breast or other sites occurred within 6 months from the first diagnosis. We considered metachronous cancer located in the contralateral breast or other sites occurred after 6 months from the first diagnosis. Patients were divided into 4 groups: (1) with synchronous BC (SBC), (2) with SBC and cancer in other sites, (3) with metachronous BC (MBC), and (4) with MBC and cancer in other sites (MBCOs).
The study is conducted according to the ethics principles of Helsinki Declaration, GCP (Good Clinical Practice), and Law of Ukraine “On medications” approved by the Commission on issues of ethics of the National Cancer Institute (Minutes No. 7 of April 8, 2010) and the Commission on issues of ethics of the Bogomolets National Medical University (Minutes No. 71 of April 10, 2013).
Data analysis
The study included 2032 patients who received special treatment at the Department of Breast Tumors and Reconstructive Surgery of the National Cancer Institute (Oncology Department Bogomolets National Medical University) from 2008 to December 2015 within an open randomized controlled trial to study objectification criteria for selection of operative intervention scope in patients with BC. In total, 195 (9.6%) patients constituted a group with MPMNs; treatment results for these patients are presented in the article.
Follow-up
Overall survival and median survival were used as indicators to assess survival time. Overall survival was calculated from the tumor diagnosis date to the death or last follow-up date; if the patient was lost, the last follow-up date was defined as the study end point.
For patients with MPMN, the survival time was calculated according to the confirmed date of the first tumor, whereas for patients with MPMN, survival time was calculated from the confirmed date of the last diagnosis of the tumor.
Survival rates of 195 patients were evaluated according to the data of National Cancer Registry of Ukraine.
Statistical analysis
The methodological basis of the study consisted of the descriptive statistics methods and specific methods of statistical analysis that laid the basis for the statistical conclusion. For general characteristics of patients group that formed the sampling frame, methods of summarizing and grouping, construction of series of distribution, methods of absolute, relative and average values, and tabular and graphical methods were used.
The analytical basis for statistical conclusion was formed by special methods of in-depth statistical analysis. Thus, for the survival analysis based on incomplete (censored) data, the survivorship function was constructed, which characterizes the probability that the subject will survive longer than t. Also, the life tables were constructed and survival distribution was adjusted with simultaneous survival function assessment using the Kaplan-Meier procedure to compare survival in 2 or more groups.
To test the hypothesis about the difference between the average periods of metachronous cancer development before and after 2008, the analysis was performed using the Student t test, and to test the hypotheses that their variances are unequal, using the Levene criterion and the Brown-Forsythe criterion were performed, which are more resistant to possible deviations of the normal distribution. Values of P < .05 were considered to be significant.
To estimate how big indirect demographic losses can be, the number of unborn children because of new cases of malignant growths among women of a reproductive age, a multiple index model of hypothetic number of unborn children was used, taking into consideration cancer incidence of women of a reproductive age, their age-specific fertility rates, and age structure.
The standard data model was created in Excel. The analytical data models were created in Statistica application. All calculations and graphs were made in Statistica application.
General characteristics of morbidity
According to the data of the National Cancer Registry of Ukraine during the past 10 years, the highest intensity of BC and that of corpus uteri and cervix was observed among women of older than reproductive age (60-69 years). At the same time, in 2004 to 2014, age structure of malignant growths among reproductive female population became worse slightly. For instance, in the structure of BC incidence, the proportion of young and average age groups (25-39 years) increased by 4 percentage points; they have shown high birth activity in recent years. Women of an early age (15-19) and those of an early reproductive age (25-29) contributed to ovary cancer incidence, with its indicator increasing by 3.7 percentage points. However, malignant growths of the mentioned organs did not result in permanent loss of reproductive function, which can be restored provided proper treatment is given. On the contrary, other 2 localizations (corpus uteri and cervix cancer) lead to permanent loss of the childbearing ability. In Ukraine, 52.8% of the sick with cervix cancer are women of average and older reproductive age (35-39 and 40-44 years), and fertility of this age groups increased by 2.3 and 2.5 times in 2004 to 2014, respectively. In total, in 2004 to 2014, the annual number of new incidence of reproductive organ cancer increased by 3.5%, and within the compared territory of Ukraine (including annexed and temporarily occupied regions), this indicator increased by 4% in 2003 to 2013, ie, 0.39% annually.5,14
Tumor distribution
The sample included 195 patients, of which 105 persons (53.9%) presented synchronous processes. Distribution of synchronous processes by localization is as follows: 55.2%—BC and 44.8%—combination of cancer in breast and other sites. The percentage of metachronous processes is 46.1%, of which 47.8% present BC and the rest 52.2% present a combination of cancer localizations.
The most frequent secondary localization of tumors was breast (79.5%) and female reproductive system (12.3%) making together 91.8% of the cases.
Distribution of patients by territorial basis
Most patients (83.1%) were urban dwellers, and the remaining 16.9% were rural dwellers. However, the reason of such distribution could be not only eventually worse ecology in big cities but also less healthy lifestyle of urban citizens and other possible factors which differ in city life from life in small villages. We consider also that primarily this could be also due to better access for health care, predominance of the urban population of Ukraine, better awareness, and higher social status of patients.
Most of the patients (69.2%) were residents of central regions and the city of Kyiv: 13.3%—eastern regions and 11.8%—western regions. This could be also due to better access for health care in big cities, especially in Kyiv, and close to Kyiv territories.
Age characteristics of patients
The average age of patients with MMPMNs was 46.6 years. The distribution of patients by age is as follows: women of reproductive age—72 (37%) and postmenopausal women—123 (63%).
Development of MPMNs is possibly associated with the consequences of the Chernobyl accident. The excess cases of BC due to radiation were identified among women exposed to radiation following the atomic bombings of Hiroshima and Nagasaki.12,15 The development of this type of cancer in this population group depended on age at the time of radiation exposure. The highest frequency of tumors was in patients exposed to radiation at the age of 10 to 19 years. A lower incidence of BC was in case of exposure at the age of 20 years and at older ages. The average latency period for BC was independent of dose and approximated 18 years. It was also determined that the BC incidence in patients exposed to radiation at the age of 10 to 29 years was higher than in patients exposed after the age of 30 years.12,15
While analyzing patients with MBCs and MBCOs, namely, the interval time between the first and the second occurrences of disease, the following data were obtained. The median interval time with MMPMNs in patients first diagnosed with BC before 2009 was 605 weeks, whereas after 2009, this median interval time was already 104 weeks (P = .000001). Reduction in the interval between the second disease occurrence after 2009 is explained by the fact that the average age of patients with BC before 2009 at the time of the Chernobyl accident was 30.5, and after 2009 was 25.5 (P = .000798). These data may indicate that BC is more aggressive in patients exposed to radiation from the Chernobyl accident under the age of 30 years.
Most patients with MPMNs had A (II) and O (I) blood type representing 145 cases, and 84.1% had Rh+, confirming the population sample distribution.
The sample included patients with BC with stages I to IIIC. The distribution by BC stage is as follows: T1-2N0M0 process was observed in 114 cases (58.5%), T1-2N1M0 in 17.9%, and T1-4N1-3M0 in 46 patients (23.6%). The above distribution demonstrates the aggressiveness of these variants of BC.
Treatment
All patients received special treatment in accordance with the National Standards for diagnosis and treatment of oncologic patients. The systemic polychemotherapy was applied in 82.2% of patients but its regimens and variants are not discussed herein.
As for surgery, we perform BCS or modified radical mastectomy with or without breast reconstruction. Our conception of choice among these options goes to the following: if the tissue volume we want to delete does not exceed 25% of the whole breast volume, the conservative surgery is performed. And if necessary, the correction of size and form of the contralateral breast also could be performed. But when the volume to delete exceeds 25% of the whole breast tissue volume, mastectomy is performed. The breast reconstruction with patient’s own tissues could be performed in case there are enough tissues in donor site. In case the donor site does not have enough own tissues for the reconstruction, it could be performed either with prosthetics or with combination of prosthetics and own tissues. And if necessary, we may also make the correction of the other breast as well.8–11
The overwhelming number of patients in our study had mastectomy—114 cases (58.5%). Breast-conserving surgery had 38.5%; we had 6 cases of BCS followed by mastectomy.
We divided our patients into core and control groups. Patients of the core group underwent simultaneous oncoplastic and reconstructive surgery, whereas control group patients had special oncological treatment only. Distribution of patients to the core and control groups was 1:3. In all, 46 patients (23.6%) were in the core group and 149 patients were in the control group (76.4%).
Distribution of patients to the core and control groups by operative intervention scope was nonrandomized. Thus, in the control group, mastectomy was performed in 93 cases (62.42%) and BCS in 53 cases (35.57%), whereas in the core group, mastectomy was performed in 21 cases (45.65%) and BCS in 22 cases (47.83%), respectively.
Patients of the core group in 18 cases (69.2%) underwent skin-sparing mastectomy with immediate prosthetic replacement and in 7 cases (26.9%) underwent mastectomy (or biquadrantectomy) with immediate breast reconstruction using the transverse rectus abdominis flap or thoracodorsal (TDL) flap.
Breast-conserving surgeries were performed in accordance with the oncoplastic surgery principles under the Clough approach. 16 Thus, level I envisaged the replacement of breast defect by mobilized skin flaps or mobilized flaps of breast parenchyma from other quadrants. Level II envisaged mastopexy or reduction mammoplasty. Level III envisaged replacement of the removed breast segment by TDL flap and others.
Results
Assessment of survival in patients with synchronous and metachronous processes was made. Thus, the chance to live 3.5 years in patients with SMPMNs was 0.73, whereas in patients with MMPMNs was 0.92 (P = .002). Thus, the clinical course of disease in patients with SMPMNs is more aggressive and prognostically unfavorable.
Modeling the survival character of cancer sick women requires preliminary estimation of their survival, taking into account the fact that patients have SMPMN and MMPMN processes of cancer development.
According to the data of sample studies, the probability to live another 125 months for patients on SMPMNs was 0.73, whereas for patients on MMPMNs, it was 0.92 (P = .002). Thus, disease development of the patients with synchronous cancer is more aggressive and diagnostically unfavorable.
When analyzing time interval between the occurrence of the first and the second diseases, it was found that median of the patients with the first diagnosis of BC before 2009 was 605 weeks, and after 2009, it decreased to 104 weeks (P < .001). The interval decrease between the occurrences of the second disease after 2009 is explained by the fact that the average age of patients with BC was 30.5 years before 2009 at the time of the disaster at ChNPS and after the year of 2009 was 25.5 years (P < .001). The presented data can confirm more aggressive disease development of patients with BC who received radiation at the age of 30 years when the disaster happened at ChNPS.
It has been statistically proved that recent years show the decrease in the period between the first and the second disease occurrences (Table 1). Thus, the period between diagnoses when identifying the first incidence before 2008 was 605 weeks (more than 11 years), and beginning from 2008, it decreased by 6 times and was 94 weeks (1 year and 9 months). Such drastic changes are the grounds for unfavorable prognoses for potential enhancement of the mentioned processes in Ukraine in the near 10 to 15 years.
Time between the first and second disease appearances (before 2008—group 1 and after 2008—group 2).
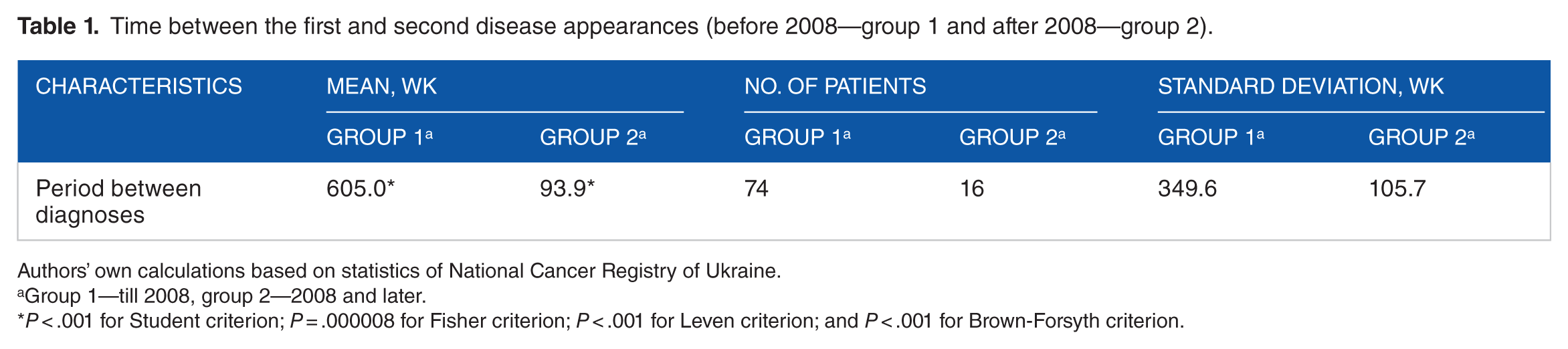
Authors’ own calculations based on statistics of National Cancer Registry of Ukraine.
Group 1—till 2008, group 2—2008 and later.
P < .001 for Student criterion; P = .000008 for Fisher criterion; P < .001 for Leven criterion; and P < .001 for Brown-Forsyth criterion.
The described situation definitely influenced the patients’ survival (Figure 1).5,14,17–19 It was statistically proved that the probability to live through another 39 months after 101 months for the group of patients whose first diagnosis was made before 2008 was 0.959 and for those whose first diagnosis was made beginning from 2008 was 0.552.

Cumulative share of survived patients depending on the moment when the first diagnosis was made according to Kaplan-Meier (before 2008—group 1 and after 2008—group 2). P = .032.
Apparently, the prediction that the situation with cancer incidence in the near 20 to 25 years will worsen appears to be true. However, the cause of the aggravated situation is to be searched in a complex effect of the factors: not only the consequences of the disaster at ChNPS but also worsening of the characteristics of life quality which can be seen in decreasing living standards, environmental pollution, and poor health care system. All this taken together leads to the situation when a person is in permanent continuous stress which results in cancer incidence, in particular, if someone is inclined to it (the availability of the first cancer diagnosis).
Besides, a more detailed disperse analysis between the periods of cancer incidence in 2 groups of the sick confirms that these 2 groups of the sick is a sample of 2 different general complexes which are characterized by variations. The exceeding of the variation coefficient by 100% in the group of the sick whose diagnosis was made in 2008 and later proves the availability of latent factors of subjective order which will further classify disease occurrence of Ukraine’s population into primary and secondary cancer incidences.
The survival of patients by subgroups was assessed, and the clinical course in patients with SBCs was reliably proved to be worse compared with other groups of patients. Also, the difference in survival in patients with MBCs and MBCOs was not reliably proved.
The worst clinical course of the disease by stage was observed in patients with MPMNs, stage III; however, there is no significant difference in survival among patients with early stages and stage IIB (Figure 2).

Cumulative share of overall survived patients depending of the stage according to Kaplan-Meier. P = .013.
In addition to stage, the survival in patients is influenced by receptor status of the tumor and expression of Her2neu and Ki-67. Metachronous breast cancers presented higher grading and lower hormone receptors expression than UBCs. Meanwhile, SBCs presented higher hormone receptors expression than UBCs and lower grading than MBCs. The higher prevalence of estrogen receptor positivity in SBCs is also confirmed by the literature. 20 Anyway, both MBCs and SBCs had higher incidence of histologically negative prognostic factors (lobular invasive histology, high grading, multifocality, and lymph node extracapsular invasion).
The clinical course of disease was also assessed by primary localization, type of settlement, blood group and Rh factor, type of special treatment, and age. The influence of these factors on the overall survival in patients with SMPMNs and MMPMNs was not statistically proven (P = .46). There was no significant difference in survival in patients with SMPMNs and MMPMNs who received only surgical treatment compared with those who received also radiotherapy or chemotherapy.
The impact of operative intervention scope in patients with SMPMNs compared with patients with MMPMNs was statistically proven (Table 2). Thus, the course of the underlying disease in patients who underwent mastectomy is worse compared with patients who underwent BCS. Also, plastic and reconstructive surgery in patients with SMPMNs was statistically proven as reasonable according to survival rates (Table 3).
Survival in patients by operative intervention scope.

Abbreviations: BCS, breast-conserving surgery; MMPMNs, metachronous multiple primary malignant neoplasms; SMPMNs, synchronous multiple primary malignant neoplasms.
P < .001; **P = .13.
Survival in patients by operative intervention type (reconstructive and oncoplastic surgery).

Abbreviations: MMPMNs, metachronous multiple primary malignant neoplasms; SMPMNs, synchronous multiple primary malignant neoplasms.
P = .015; **P = .36.
In this study, the influence of local recurrence on overall survival was analyzed. It was statistically proven that the worse course of the disease was in patients with SMPMNs, ie, the reduction in overall survival by 71%. However, the influence of local recurrence on life expectancy in patients with MMPMNs was not statistically proven.
The question arises: how big indirect demographic losses can be—the number of unborn children because of new cases of malignant growths among women of a reproductive age. To find the answer, a multiple index model of hypothetic number of unborn children was built, taking into consideration cancer incidence of women at a reproductive age, their age-specific fertility rates, and age structure for the years 2004 to 2014.
Table 4 shows a relative change of hypothetic number of unborn children taking into account new cases of malignant growths of all nosological forms, concerning a reproductive system, including BC, and also excluding it, ie, only reproductive organs.
Dynamics of hypothetical number of unborn children because of cancer in women of reproductive age in Ukraine in 2004 to 2014, %.

In 2004 to 2014, total hypothetic losses of childbirth due to unrealized reproductive functions by cancer sick women increased by 89.2%. If to exclude women diagnosed with BC whose reproductive ability can be restored after long-term sever therapy, the scope of hypothetic losses would be increased by 80.6%. However, such high growth rates are mostly associated with general tendency of age fertility increase, typical for all Ukrainian women (+62.9%); it is during the last 11 years that reproductive activity of women at the age of 30 to 40 years has increased by 2 times. The change in the age structure of a women’s reproductive cohort caused the increase in potential childbirth and also hypothetic losses (+2%). Primary cancer incidence of women at a reproductive age led to the increase in hypothetic losses by 11.8%, in general, and with permanent loss of reproductive functions because of cancer of a reproductive system, the number of unborn children increased by 8.7%. However, a mentioned index model enables to make rough estimation of hypothetic losses of childbirth based on the statistics of the annual number of identified new cases of disease.
Discussion
It was shown that the clinical course of disease in patients with SMPMNs is more aggressive and prognostically unfavorable compared with patients with MMPMNs. These results are different compared with the results obtained by Xu and Gu. According to their results, there was no significant difference in survival time between SMPMN and MMPMN (P = .81). However, the structure of localizations was different in this research: among 344 tumor lesions, there were 161 located in the digestive system, 48 in the respiratory system, only 63 in the breast, 7 in the reproductive system, 30 in the urinary system, 23 in the head and neck, and the other 12 occurred in the brain, blood system, and soft tissue. 6
In patients with cancer, the risk of developing second cancers varies from 1% to 10%, which is significantly higher than the risk among healthy individuals. In this study, the incidence of MPMNs was 9.6%. The incidence of SBCs was higher than the incidence of MBCs, at the ratio of 1.2:1. In addition, the incidence of MPMNs increases with age. 21 Thus, the average age of patients was 46.6 years, and the number of postmenopausal women was 63%.
Variability of the second tumor localization depends on the prevalence in a particular geographic region. Thus, in Japan, diseases of the gastrointestinal tract prevail, especially stomach cancer; in China, nasopharyngeal cancer; and in Ukraine, BC (incidence of 39.9 per 100 000 population). 22 In this study, most of the cases included BC (79.5%) and reproductive system cancer (12.3%). Among patients with SBCs, SMPMNs were observed in 60 cases.
Causes of MPMNs have not been studied; however, causal relationships with the following factors are possible. The first cause is linked with endogenous factors such as abnormal embryonic development, immunity-related diseases, and endocrine diseases affecting sensitivity to carcinogens. 23
The second cause is linked with environmental and lifestyle exposures, including long-term effects of radiation and industrial pollution. The study statistically proves the possible impact of radioactive contamination following the Chernobyl accident on possible MPMNs development. However, no difference was identified in the incidence of MPMNs among the urban and rural populations.
Third, genetic determinants may influence MPMN occurrence. In patients with BC and ovarian cancer, positive family history is observed, which is transmitted through autosomal dominant inheritance. 24 In the study, only 9 patients had a family history of breast and ovarian cancers. Thus, the presence of BRCA1/2 mutations in young patients with simultaneous BC was proved. 25
Finally, MPMN is caused by iatrogenic effect, especially radiation therapy and drug therapy. Carcinogenic effect of radiation therapy can be produced by DNA damage and oncogene activation. Thus, patients with BC are continuously treated with polychemotherapy and hormone therapy that suppress the immune system thereby increasing the probability of cancer occurrence. 26 The study did not reliably prove the increased overall survival from radiation therapy and drug therapy, especially in patients with SMPMNs.
There is currently no consensus for the method of calculating the survival rate of MPMN. Many researchers recommend basing the rate from the final diagnosis of the malignancy tumor, whereas others suggest calculating survival from the diagnosis of the first tumor to take into account the increased risk of malignancy tumor occurrence during the prolonged survival period. We recommend using the last cancer diagnosis to calculate the survival rate for determining the prognosis of MPMN. Because MMPMN has a relatively longer interval, which can possibly result in a bias, it is suggested that the calculation of survival time that is based on the last tumor diagnosis is more reasonable. In a study of the survival time of MPMN, second primary small-cell lung cancer (SCLC) was compared with first primary SCLC, and no significant differences were found in efficacy and median survival time.27,28
Although there is not yet a consensus of prognostic factors of MPMN, several studies have shown consistent prognostic factors, including the MPMN occurrence interval, earlier or later stage of the disease and tumor type, biological characteristics, and whether or not diagnosis and correct treatment are applied in a timely manner, including radical surgery, adjuvant chemotherapy, and radiotherapy. The definition of SMPMN and MMPMN is the starting point to achieve accurate comparisons, and 6 months is the standard criterion used in most previous studies. According to the biological characteristics of tumors, malignant tumors must be present for a certain period of time before showing clinical manifestations; therefore, if the interval time between tumors is too short, MMPMN might be equivalent to SMPMN so that the designation of simultaneous or metachronous is merely relative.
The survival rate of SMPMNs was lower compared with those of MMPMNs and UBCs, and SMPMNs was also associated with a higher risk of distant metastasis. In this study, overall survival in patients with SMPMNs was lower than in patients with MMPMNs being 0.73 and 0.92, respectively; similar results were obtained by British researchers. 29
At present, reconstructive and oncoplastic surgery is an integral part of surgical treatment. However, many unresolved issues remain regarding the choice of a particular type of surgery, and in patients with MPMN, this issue was never studied. The data obtained that are based on large clinical material prove the need to implement modern approaches in this patient population. Thus, using BCS is more appropriate in patients with MBCs, and in patients with SBCs, mastectomy with simultaneous breast reconstruction is deemed more preferable.
Conclusions
A more aggressive course of BC is observed in patients exposed to radiation from the Chernobyl accident under the age of 30 years. With probability P < .001, it was proved that the formation factors of patients’ survival before and after 30 years differed greatly, which requires separate studying.
The clinical course of disease in patients with SMPMNs is worse and prognostically unfavorable as compared with MMPMNs (P = .002). The course of the underlying disease in patients who underwent mastectomy is 3 times worse compared with patients who underwent BCS (P < .001). Plastic and reconstructive surgery in patients with SMPMNs was statistically proven in this study as reasonable, increasing overall survival by 29% (P = .015). Appearance of local recurrence reduces the overall survival by 71% (P = .033). However, the influence of local recurrence in patients with MMPMNs was not statistically proven.
Unfortunately, the lack of the information about age structure of all registered cancer sick women of a reproductive age does not allow estimating a true number of unborn children. While estimating the losses of childbirth, it is advisable to consider age survival probability of the women with malignant growths of reproductive organs. Hence, the next step is to identify the survival parameters of cancer sick women of a reproductive age.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.