
Abstract
The molecular classification for breast carcinomas has been used in clinical studies with a simple surrogate panel of immunohistochemistry (IHC) markers. The objective of this current project was to study the molecular classification of commonly used breast cancer cell lines by IHC analysis. Seventeen breast cancer cell lines were harvested, fixed in formalin and made into cell blocks. IHC analyses were performed on each cell block with antibodies to estrogen receptor (ER), progesterone receptor (PR), HER2, EGFR, CK5/6, Ki-67 and androgen receptor (AR). Among the 17 cell lines, MCF-7 and ZR-75-1 fell to Luminal A subtype; BT-474 to Luminal B subtype; SKBR-3, MDA-MD-435 and AU 565 to HER2 over-expression subtype; MDA-MB-231, MCF-12A, HBL 101, HS 598 T, MCF-10A, MCF-10F, BT-20, 468 and BT-483 to basal subtype. MDA-MB-453 belonged to Unclassified subtype. Since each subtype defined by this IHC-based molecular classification does show a distinct clinical outcome, attention should be paid when choosing a cell line for any study.
Introduction
Breast cancer encompasses a group of very heterogeneous diseases, which can be demonstrated at the molecular, histopathologic and clinical levels. 1 The heterogeneity at the molecular level has been demonstrated by reproducible differences in the frequencies and magnitudes of genomic aberrations and by differential gene expression among breast carcinomas, even those with similar histology.2,3 Studies on whole-genome analysis using expression microarray have revolutionized our understanding of breast carcinomas, which has led to the discovery of 5 distinct subtypes of breast carcinomas (Luminal A, Luminal B, HER2 over-expression, Basal-like, Normal-like), each with unique recognizable phenotypes and clinical outcomes.4–8 Subsequent studies have shown that breast carcinomas can also be divided into 5 similar subgroups using immunohistochemical (IHC) analysis as a surrogate with a limited panel of antibody markers (including ER, PR, HER2, CK5/6 and EGFR).9,10 These subgroups have distinguishing features closely associated with subtypes defined by gene expression profiling, including distinct clinical outcomes, different responses to adjuvant therapy and different patterns of metastatic recurrence.11–14 Although molecular classification has been mainly used in clinical and translational research, many have suggested it may have utility in routine clinical practice in guiding individualized management for breast cancer patients.15–17
Breast cancer cell lines have been used extensively in basic research and have provided valuable insight into many aspects of breast cancer biology. Cell lines are one of the most critical components in studying tumor carcinogenesis,18,19 signal transduction pathways,20,21 and new therapeutic targets for breast carcinoma.22–24 However, a cell line chosen for a particular study is largely based on its unique biologic features and its availability, and often its ER, PR and HER2 status may not be known. If breast cancer represents a heterogeneous group of diseases, then cell lines derived from different patient's tumors should reflect this biologic diversity. The objective of the current project is to investigate the expression patterns of the clinically most critical molecules for breast cancer (ER, PR HER2, Ki-67, CK5/6, EGFR and AR) 14 by immunohistochemical (IHC) analysis in 17 commonly used cell lines and with this information determine the molecular classification of each cell line.
Methods
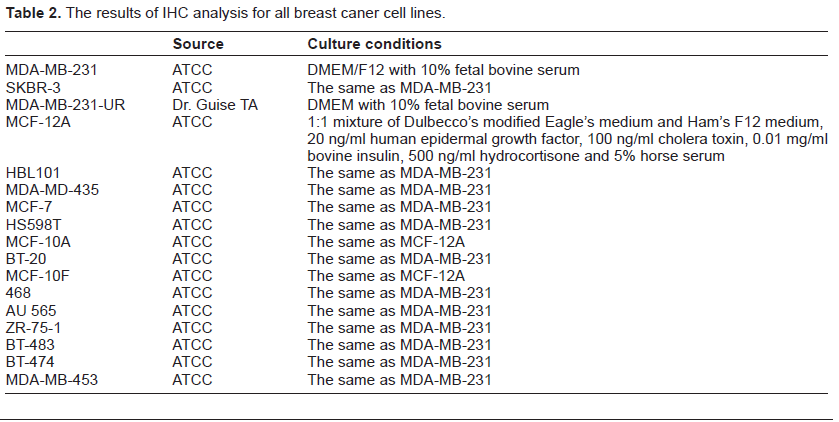
Seventeen commonly used breast cancer cell lines (MDA-MB-231, SKBR-3, MDA-MB-231-UR, MCF-12A, HBL101, MDA-MD-435, MCF-7, HS598T, MCF-10A, BT-20, MCF10F, 468, AU 565, ZR-75-1, BT-483, BT-474, and MDA-MB-453) were cultured in appropriate medium (Table 2), harvested by cell scraper before reaching confluence, washed twice with PBS, and frozen as cell pellets at –80 °C. Once all cell lines were ready, they were thawed on ice, and fixed in 10% formalin for 16 hours. Each cell line was pelleted and made into a cell block. One H & E stain and 7 IHC stains were subsequently performed for each cell line. Pretreatments consisted of enzyme digestion, or other heat mediated retrieval methods. Sections were stained on a Dako Autostainer using either a Envision Plus–-HRP polymer (Dako, Carpenteria, Ca.) or Horse Anti-Mouse IgG-Biotin (Vector Laboratories, Inc. Burlingame, Ca), Streptavidin-HRP (Jackson Labs) and AEC (Dako, Carpenteria, Ca.), and counterstained in hematoxylin. ER (clones 1D5 and ER-2-123, Dako), PR (clone PgR 1294, Dako) and AR (clone AR441, Dako) were recorded as Allred scores; 25 HER2 (HercepTest, Dako) was scored as positive if >30% of tumor cells showed 3+ membrane staining; 26 EGFR (EGFR pharmDx, Dako) was designated as positive if any tumor cells showed 1+ positive stain; any strong cytoplasmic stain was considered as positive for CK5/6 (clone D5/16 B4, Dako); and Ki-67 (clone MIB-1, Dako) was scored as % of any intensity nuclear stain. The definition for each molecular subtype was based on the expression of ER, PR, HER2, EGFR and CK5/6 as previously described 17 (Table 1).
Definition of each subtype in molecular classification.

The results of IHC analysis for all breast caner cell lines.
Results (Table 3 and Figs. 1 and 2)

Representative staining results from H&E and IHC for ER, PR, HER2, EGFR, CK5/6, Ki-67 and AR (original magnification 400X). A) H & E stain for HS 598T cell; B) ER for MCF-7; C) PR for BT-474, D) HER2 for SKBR-3, E) EGFR for MDA-MB-231, F) CK5/6 for MCF-10F, G) Ki-67 for MCF-10A, and H) AR for ZR-75-1.

Examples of the subtypes of molecular classification. A-D) MCF-7 for Luminal A subtype with stains for ER, PR, HER2 and EGFR; E-H) BT-474 for Luminal B subtype with stains for ER, PR, HER2 and EGFR; I-L) SKBR-3 for HER2 overexpression subtype with stains for ER, PR, HER2 and EGFR; M-P) MCF-12A for Basal subtype with stains for ER, PR, HER2 and EGFR.
The results of IHC analysis for all breast caner cell lines.

Using the same antibodies, the same experimental conditions, and the same scoring systems that we use for our clinical specimens, we found that two cell lines MCF-7 and ZR-75-I were positive for ER; and three cell lines MCF-7, ZR-75-I and BT-474 were positive for PR. HER2 was found over-expressed in four cell lines. Of these four, SKBR-3, MDA-MD-435, and AU 565 were ER and PR negative, and BT-474 was ER negative and PR positive.
MCF-7 and ZR-75-1 fell within the Luminal A subtype; and BT-474 belonged to Luminal B subtype, which was repeatedly shown to be ER negative, PR positive, HER2 positive, CK5/6 negative and EGFR positive. Three cell lines (SKBR,-3, MDA-MD-435 and AU 565) fell within the HER2 over-expression subtype. Ten cell lines (MDA-MB-231, MDA-MB-231-UR, MCF-12A, HBL101, HS598T, MCF-10A, BT-20, MCF-10F, 468 and BT-483) belonged to Basal-like subtype due to their negativity for ER, PR and HER2 and positive for EGFR (10/10 cell lines) and/or CK5/6 (3/10 cell lines). MDA-MB-453 belonged to triple negative non-basal (Unclassified) subtype. Only three cell lines (MCF-12A, MCF-10A and MCF-10F) were positive for CK5/6. Of these, all belonged to Basal subtype. All but 2 cell lines were positive for EGFR; one (MDA-MD-435) belonged to HER2 subtype, and the other (MDA-MB-453) belonged to Unclassified subtype.
We found most of the cell lines expressed very high levels of Ki-67, ranging from 20% to 100%. MDA-MB-231 had 100% positive stain for Ki-67. Two cell lines expressed Ki-67 under 50%, SKBR-3 was 20% and MCF-10A was 30%. AR was expressed in 14/17 cell lines, and the three AR negative cell lines (HS598T, MCF-10F, MCF-10A) were also negative for ER and belonged to basal-like subtype.
Discussion
There are many breast cancer cell lines available and used in various studies. Like primary breast carcinomas, these cell lines can be very different from one to another.27,28 Although breast cancer cell lines have always been a critical tool for most of the basic research, they are rarely studied with methods similar to those that are used for a routine clinical work up for primary breast cancer, such as IHC.
We were surprised to see that only a few cell lines express ER (MCF-7 and ZR-75-1) and PR (MCF-7, ZR-75-1, and BT-474) with IHC analysis that is routinely used for primary breast cancer. BT-483, a cell line which was reportedly positive for ER, 29 failed to showed a positive ER staining in our study. One explanation for this could be the different experimental methods and conditions. We have confirmed that SKBR-3, AU 565 and BT-474 overexpress HER2, 30 and found that another cell line, MDA-MD-435, also over-expresses HER2.
Molecular subtypes, originally identified by gene expression profiling,4–6 were then confirmed by IHC analysis.9,10 Numerous studies have shown that Luminal A subtype has better differentiated tumors, is often seen in older patients and has the best prognosis compared to other subtypes; Luminal B subtype has higher expression of proliferation associated genes and a worse prognosis than Luminal A; HER2 subtype is often associated with nodal metastasis; and Basal subtype often occurs in younger patients, is more frequently associated with visceral organ metastasis, and has a poor prognosis.11–13 Since molecular classification has been shown with important clinical implications for breast cancer patients, it would be important to understand the molecular subtypes of commonly used breast cancer cell lines. Most cell lines in the current study are Basal subtype, which is not surprising, since Basal subtype tumors are more aggressive and poorly differentiated, and thus are more likely to be established as a cell line compared to better differentiated ER positive Luminal subtypes. MDA-MB-231 was obtained from MD Anderson Cancer Center; and MDA-MB-231 UR was a bone specific cell line obtained from University of Rochester (UR, a gift from Dr. Guise TA from university of Indiana), which may explain the different expression level of EGFR. It is important to understand that although IHC-based molecular classification has been used in numerous studies, there is still lack of uniform definition for each subtype, and the definitive role of molecular classification in guiding clinical decision making remains to be confirmed. 17
Besides ER, PR and HER2, Ki-67 has become a very important predictive and prognostic marker for breast cancer.14,31,32 Using the same conditions and scoring system for IHC analysis used in breast cancer, we found most of the cell lines expressed a very high level of Ki-67, ranging from 20% to 100%. The very aggressive cell line MDA-MB-231 33 had 100% cells positive for Ki-67, and only two cell lines expressed Ki-67 under 50% (SKBR-3 20% and MCF-10A 30%). One explanation for the dramatic difference between cell lines and primary tumors (often under 50%, with most ranging from 2%–40% in our experience) is that these tumor cells were harvested at their growth phase, while only a very small fraction of primary tumor cells would be at the growth phase at any given time.
The results from studies using breast cancer cell lines may not be clinically relevant to the general breast cancer population. The breast cancer metastasis suppressor 1 (BRMS1) is one of a growing number of genes that have the ability to suppress metastasis without affecting tumorigenicity in experimental in vivo models. 34 Transfection of BRM1 into MDA-MB-435 and MDA-MB-231 has been shown to significantly decrease the metastatic potential of both cell lines in animal models. 35 An examination of BRMS1 in a large clinical cohort of breast cancer cases showed no correlation between loss of BRMS1 expression by IHC and cumulative disease-free survival. 36 However when stratified by ER negative, PR negative or HER2 positive subsets of patients, the BRMS1-negative subgroups had significantly reduced disease-free survival compared with BRMS1-positive cases. 36 Interestingly, the two cell lines used in the initial cell-line studies of BRMS1 were both ER, PR negative; and MDA-MB-435 was HER2 positive in the current study. These finding highlight the importance of taking the molecular subtype into consideration when attempting to translate findings from breast cancer cell lines into a clinical context.
AR has been shown to be an important prognostic marker, and associated with better prognosis.37,38 AR may also be used as a therapeutic target, especially in ER negative breast cancer. 39 We have previously demonstrated the possible role that AR might play during the transition from high grade in situ to invasive ductal carcinoma. 40 In the current study, we did confirm that MCF-10F is ER negative, but did not confirm that it is AR positive, as it has been previously reported. 41
In conclusion, the clinical and biologic heterogeneity in breast carcinomas revealed by gene expression profiling is also present among the different breast cancer cell lines, and can be detected by IHC analysis. Attention to these differences should be paid when choosing a cell line for any study and attempting to translate in vitro data into a clinical context.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.