
Abstract
The dual pathway hypothesis of risk for substance use was tested by examining risk from symptoms of conduct problems and depressive symptoms in adolescence (from ages 10-11 to 17-18 years) to substance use—including tobacco, alcohol, cannabis, and other illicit drugs—in both early adulthood (approximately from ages 20 to 29 years) and middle adulthood (approximately from ages 29 to 38 years). Hypotheses were tested on a sample of boys who were at risk for conduct problems by virtue of the neighborhoods where they lived in childhood (the Oregon Youth Study; N = 206 at Wave 1). Dual-trajectory modeling (Latent Class Analysis) resulted in a 3-group solution of high, moderate, and low co-occurring symptoms. The latent class of boys with co-occurring symptoms in adolescence showed higher levels of substance use in adulthood; namely, higher levels of cannabis and illicit substance use during early adulthood compared to either of the moderate or low symptom classes, and higher use of cannabis in midadulthood than the low symptom class. Those with co-occurring symptoms also showed, overall, higher vulnerability to use of tobacco in these 2 periods, but not to higher use of alcohol. Regression analyses indicated that the higher substance use of the co-occur group of men was related to their adolescent conduct problems, but was not related to their adolescent depressive symptoms; however, these associations were nonsignificant when adolescent use of the respective substances were included in the models. Thus, the dual-trajectory hypothesis was not supported. However, the findings indicated that, as assessed in the present study, the psychopathology symptoms of boys with conduct problems in adolescence who show risk for later substance use may be complex, involving depressive symptoms.
Introduction
Co-occurring symptoms of internalizing and externalizing problems in childhood and adolescence, and comorbidity of disorders in these domains, have been researched since the 1980s,1,2 with studies focused largely on whether 1 symptom domain precedes and may cause the other,1,3,4 and the extent to which co-occurrence is associated more with detrimental outcomes in adolescence and young adulthood than symptoms in a single domain.5 -9 Early studies of boys in the Oregon Youth Study (OYS) assessing conduct problems and depressive symptoms concluded co-occurring symptoms in early adolescence (ages 11-12 years) were associated with substance use, 10 although this was not supported in the studies extending into mid and later adolescence. 5 Other studies have also found risks for substance use from both conduct problems and depressive symptoms in adolescence. 11 Given there is less evidence on the long-term risks in adulthood associated with co-occurring symptoms during adolescence, we examined this issue presently.
Previously, we examined prediction from levels of both conduct problems and depressive symptoms in early adolescence (from ages 11-12 to 13-14 years) to substance use in young adulthood at ages 18 or 21 years. 6 Early adolescent conduct problems, but not depressive symptoms, predicted more frequent and intense past-year substance use, while controlling for early adolescent substance use. Overall, there is considerable evidence that conduct problems in adolescence predict substance use in adulthood,12,13 but less support for additional risk from depressive symptoms. However, adolescents’ depressive symptoms may be associated with substance use later in adulthood. Motivations for alcohol and cannabis use change across early adulthood, including decreases in to experiment, fit in, and have a good time, and increases in to get high, relax, and sleep. 14 These latter motivations may be related to depressive symptoms. Motivations to use substances are also related life events that may also be related to increases in depressive symptoms, such as the ending of relationships and employment. 15 Thus, it is valuable to examine what the implications of conduct problems and depressive symptoms may be for substance use beyond young adulthood.
A number of studies have found associations between conduct problems and depressive symptoms in adolescence and substance use in adulthood. In 1 study, psychosocial factors assessed at ages 14, 19, and 24 years (including symptoms of anxiety and depression and antisocial behavior) were associated with higher risk for cannabis use disorder assessed at age 29 years. 16 In another study, comorbid substance use and mental health problems (symptoms of depression and anxiety) at ages 13 to 14 years predicted similar comorbid symptoms at age 33 years for the Seattle Social Development Project sample. 17 In the Victoria Healthy Youth Survey, an adolescent chronic cannabis use class (11% of the sample) had more problem behaviors, including conduct problems in both adolescence and young adulthood (ages 22-29 years), and more depressive symptoms in young adulthood than other classes. 18 Whereas these studies support an association of depressive symptoms, conduct problems, and substance use across adolescence and adulthood (through the early 30s), they did not specifically examine the association of depressive symptoms and conduct problems in adolescence to later substance use, while controlling for use in adolescence and alcohol use in adulthood.
The dual pathway hypothesis is an influential theory regarding risk for substance use in adulthood, which posits that substance use is related first to histories of conduct problems and second to histories of internalizing disorders including depressive symptoms.19,20 The key mechanism posited regarding risk from depressive symptoms is self-medication for such symptoms. 21 In a test of this hypothesis using data from the National Longitudinal Study of Adolescent Health (Add Health), 22 the authors found that conduct problems were related to use of most substances in adolescence and in early adulthood, whereas depressive symptoms showed little association with the outcomes in either period. However, outcomes were measured only to approximately ages 23 to 24 years, which is relatively young for making conclusions about associations having lifespan implications.
The present study is particularly timely as prevalence of daily cannabis use in the U.S. more than doubled from 2005 to 2017; furthermore, prevalence of daily use is higher and increased more over time among depressed (from 2.5% to 6.7%) than nondepressed (1.4% to 2.9%) individuals. 23 Thus, it is critical to learn more about developmental risk factors for cannabis use, as well as for other substances. In addition, the study involves men in the OYS, who in childhood lived in lower-income neighborhoods; there is evidence that this population is particularly vulnerable to substance use and associated health risks in adulthood. 24
Several factors were considered in selecting the approach for examining the co-occurrence of conduct problems and depressive symptoms at adolescence. In studies of co-occurrence of symptoms assessed across the full range (ie, that do not involve clinical diagnoses), there are disadvantages to selecting a cut point to define 4 groups. First, such an approach does not utilize or characterize the full range of individual experiences of symptoms. Second, cut points based on sample distributions (eg, 0.5 standard deviations above the mean) 10 are relatively arbitrary and subject to being affected by sample characteristics. Thus, in the present study, continuous measures in each domain were modeled simultaneously from ages 10-11 through 17-18 years using dual-trajectory growth modeling to examine heterogeneity in latent trajectories of co-occurring symptoms. This approach was expected mainly to provide descriptive information regarding co-occurring symptoms at adolescence, as it was unlikely that the modeled groups would fall into the 4 distinguishable patterns of symptoms that were co-occurring, conduct problems only, depressive symptoms only, or low levels of both problems. Thus, in addition to examining substance use outcomes for the modeled trajectory groups, regression analyses considered adolescent conduct problems, depressive symptoms, and their interactive effects as predictors of substance use in adulthood, adjusting for use of the same substance in adolescence.
Hypotheses
First, it was hypothesized that the classes modeled across adolescence would include a group experiencing relatively high symptoms of both conduct problems and depression, a group that would show low levels of symptoms in both domains, a group experiencing moderate-to-high conduct problems but low depressive symptoms, and a group with moderate-to-high levels of depressive symptoms but with low levels of conduct problems. Next, mean levels of cannabis, alcohol, tobacco, and any use of other illicit drugs were examined separately within early adulthood (approximately from ages 20 to 29 years) and within middle adulthood (approximately from ages 29 to 38 years) for the groups that were modeled. It was predicted that men who had experienced higher and co-occurring symptoms in adolescence would show significantly higher use of each type of substance in both adult periods than men who had experienced low levels of each type of symptoms. Based on the dual-trajectory hypothesis regarding risks for substance use in adulthood, it was hypothesized that a group experiencing higher levels of depressive symptoms but lower levels of conduct problems in adolescence would show higher levels of substance use in both early and middle adulthood than a group experiencing low symptoms in each area. Given that there was not a substantial justification for hypothesizing differential findings for the different forms of substances used, these analyses were considered exploratory. Follow-up regression analyses were then conducted to formally test the prediction from adolescents’ conduct problems and depressive symptoms to their substance use in adulthood.
Methods
Design
The OYS was a longitudinal study initiated in order to assess prospective predictors, particularly family and peer group factors, related to the onset and course of conduct problem behaviors, particularly delinquency and substance use in adolescence, for boys. The study initially involved 9- to 10-year-old boys and their families who were living in higher-delinquency neighborhoods (determined by density of adolescent offenders residing in the area) in a medium-sized metropolitan area in the Pacific Northwest. The study started in 1984 and ended in 2013, and involved 24 annual assessment waves from ages 9-10 to 31-32 years—except for no assessment at ages 26 to 27 years (22 assessments)—with 2 further assessments at ages 35 to 36 and 37 to 38 years. As is typical for such long-term studies, the specific hypotheses and analyses of the present study were not part of the initial study plan.
Participants
All families with fourth-grade boys in schools in selected at-risk neighborhoods were eligible to participate (except 31 families who could not speak English or were planning to move out of state within 6 months). Families were recruited via an initial letter from the school announcing the study and asking them to withdraw their names if they did not want to be contacted by study staff (very few families withdrew their names). Families then received a phone call to schedule a home visit in which study participation was described. The recruitment rate of eligible families was 74% (N = 206 25 ). Participation rates were high through young adulthood (202 of 206—98% at ages 20-21 years) and lower but still high, considering the length of the study, in midadulthood (176 of 200 living men (88%) at ages 37 to 38 years, or 85% of the original sample of 206).
Consistent with regional demographics at the time, participants were primarily White (n = 185 of 206: 90%) and from lower- and working-class families (n = 154-155; 75%). 26 In the first year of the study, 69 of 206 (33%) of the families received welfare or food stamps. Forty percent (n = 89 of 205) of the families involved 2 biological parents; 25% were 2 parent, including a stepparent; 30% were single-mother families; and (n = 10 of 205) 5% were single-father families. Sixteen (n = 23 of 142) percent of participating fathers and 8% of mothers were college graduates.
Procedures
OYS parents and sons completed in-person interviews and questionnaires separately, with each interview lasting 45 minutes to 1 hour. They were compensated for their time. Adults provided written informed consent and all procedures were approved by the Institutional Review Board of the Oregon Social Learning Center.
Measures
Measures are described briefly below and in more detail in the online Supplemental Material (Supplemental Table 1) where the number of items per scale, sample items, and reliability information are provided.
Conduct problems were assessed yearly from ages 10-11 to 17-18 years (8 occasions). Conduct problems at each of the 8 time points were assessed by mother and father reports (32 items each; mean Cronbach’s alphas across waves were .93 and .92, respectively) on the externalizing scale of the Child Behavior Checklist (CBC-L 27 ).
Depressive symptoms were assessed by self-report using 18 items from the Child Behavior Rating Scale (CBRS 28 ) in the first 4 years (ages 10-11 to 13-14 years) and 20 items from the Center for Epidemiologic Studies Depression Scale (CES-D 29 ) in the last 4 years (ages 14-15 to 17-18 years; mean Cronbach’s alphas across waves were .76 and .84, respectively).
Adult substance use—comprising tobacco, alcohol, cannabis, and other illicit drug use—was assessed 8 times across early adulthood (from ages 20-21 to 28-29 years) and 5 times across midadulthood (from ages 29-30 to 37-38 years). At each wave, tobacco, alcohol, and cannabis use scores were calculated as the log of the volume of use, which consisted of the number of times the substance was used in the previous year multiplied by the amount of use. Tobacco use volume was scaled in milligrams of nicotine (estimated from reported number if cigars, cigarettes, and chews). Alcohol use volume was in ounces determined from the number of drinks, equalized to 1 ounce of alcohol per drink. Volume of cannabis use in grams was estimated from reported number of joints, bong hits, pipefuls, grams, or portion of ounces typically used.30,31 For other illicit drug use, the variable was the log of the mean across waves of a dichotomous score of any use of cocaine, hallucinogens, opiates, uppers, downers, or other tranquilizers versus no use (1 vs 0). Finally, the early and midadulthood substance use outcomes were calculated for each substance type (tobacco, alcohol, cannabis, and other illicit drug use) as the mean of the annual scores within each period.
Adolescent substance use was assessed yearly on 7 occasions (from ages 11-12 to 17-18 years) and involved separate measures of tobacco, alcohol, cannabis, and other illicit drug use. Each was used as control variables in the regression analysis for the corresponding substance use outcome. The scores were calculated in the same way as for adult substance use.
Analytic plan
The first part of the analyses involved a dual-trajectory latent class growth analysis based on trajectories of conduct problems and depressive symptoms across adolescence. Trajectories were modeled using Mplus. 32 The approach assumes the study population is comprised of classes with differential growth patterns and creates classes of individuals sharing similar growth parameters. Nested single-class dual-trajectory models were initially estimated to determine the shape of growth. Although separate conduct problem and depressive symptoms growth models may have had different shapes, we constrained the growth parameters to the same type for both in order to ensure 1 domain did not overly affect the modeling by having a different number of growth parameters, in this case including linear and quadratic growth with the intercept fixed at ages 13 to 14 years. Classes were then added until the model best fit the data based on minimizing the Bayesian information criterion statistic, and with a significant Lo-Mendell-Rubin likelihood ratio test, 33 indicating the model with that number of classes was a significant improvement in fit versus the model with 1 less class. Trajectory modeling was based on latent growth analyses using only the means, because estimation of subgroup variances for the growth parameters produced inadmissible model results—likely due to lack of large enough class sizes to reliably identify this information. Additionally, the purpose of the latent class growth analysis was to identify co-occur classes; thus, the variances were of little relevance to the main hypotheses. Missing data were accounted for by using robust maximum likelihood estimation. To avoid local minima in the solution, 400 random starts were used with 50 final iterations.
Equality of means tests for substance use in both the early and midadult period between classes were modeled in the analysis that defined the classes, using the Bakk and Vermunt 34 and Bolck et al 35 option of the auxiliary variable command, which is preferred for continuous distal outcomes (p. 617 32 ).
For any case where the dual-modeled trajectory classes were found to be associated with use of a particular substance in early or midadulthood, follow-up regression analyses were conducted to probe whether the mean of conduct problems alone, mean of depressive symptoms alone (each calculated across adolescence), additive effects (models including both), and/or interactive effects were associated with each substance use outcome separately (adding a control for adolescent use of the equivalent substance in the final model). These provided further insight into whether any risk for future substance use was conferred from either psychopathology domain alone or from co-occurring effects.
Results
Descriptive statistics
Shown in Table 1 are descriptive statistics for the 4 types of substances (cannabis, alcohol, tobacco, and illicit drugs) in both early and midadulthood. Almost all of the men used some alcohol in each period. Any use of cannabis, tobacco, and illicit drugs was also relatively high, and in each case was lower in midadulthood than in early adulthood. Even in midadulthood, however, close to 1 half of the men reported some use of cannabis and/or illicit drugs. Shown in Table 2 are Pearson correlations among all the timepoint estimates for conduct problems and depressive symptoms and each of the 4 substances for both the early adult and midadult period. Across all measures, on average 87% of men had full data, with a minimum of 163 of 197 (83%) for all measures in midadulthood and a high of 190 of 206 (92%) for adolescent alcohol use.
Cannabis, alcohol, and tobacco use in early and midadulthood.

Illicit use does not include alcohol or tobacco use by minors, or cannabis use.
Matrix of Pearson Correlations among adolescent depressive symptoms, adolescent conduct problems, early adult substance use, and midadult substance use.
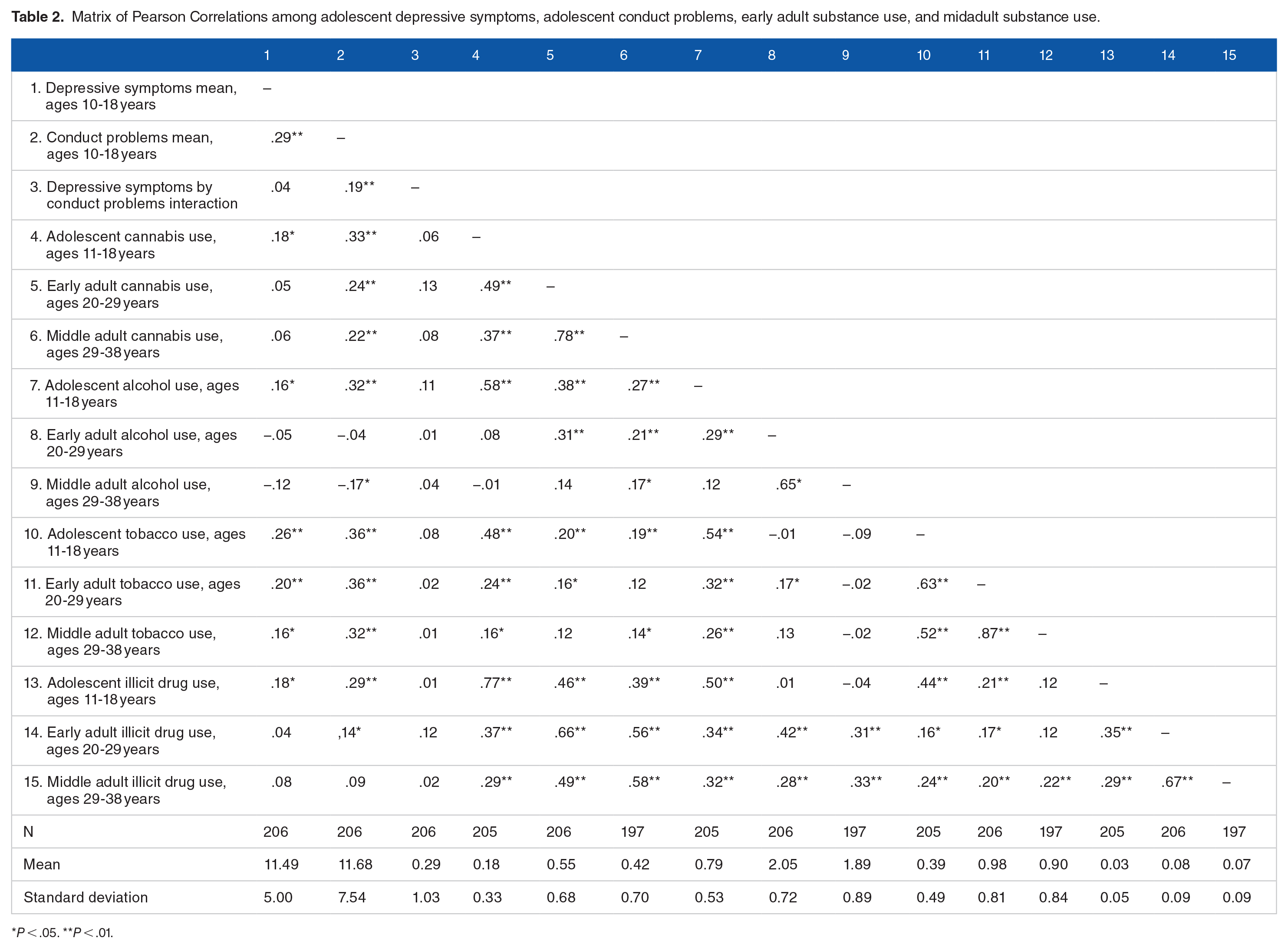
P < .05. **P < .01.
Dual-trajectory modeling
Findings for the dual-trajectory modeling latent classes indicated that the 3-class solution showed a significant improvement in model fit compared with the 2-class solution according to the Bootstrap Likelihood Ratio Test (LRT) and Vuong-Lo-Mendell-Rubin LRT tests. In addition, the fit of the 3-class model exhibited good entropy (model fit comparisons are shown in Supplemental Table 2 of the online Supplemental Material). Trajectories of conduct problems and depressive symptoms across adolescence for the 2 models are shown in Figure 1. Note that the classes represented greater heterogeneity for conduct problems than for depressive symptoms. The first class (High Co-occur) was relatively small (10.6% of the sample) and included boys who reported high levels of both conduct problem and depressive symptoms. The second class (Moderate Co-occur) represented 42% of the sample and were boys who had moderate symptoms in both domains. The third class (Low Symptoms) represented 47.5% of the sample and had low symptoms in both domains.
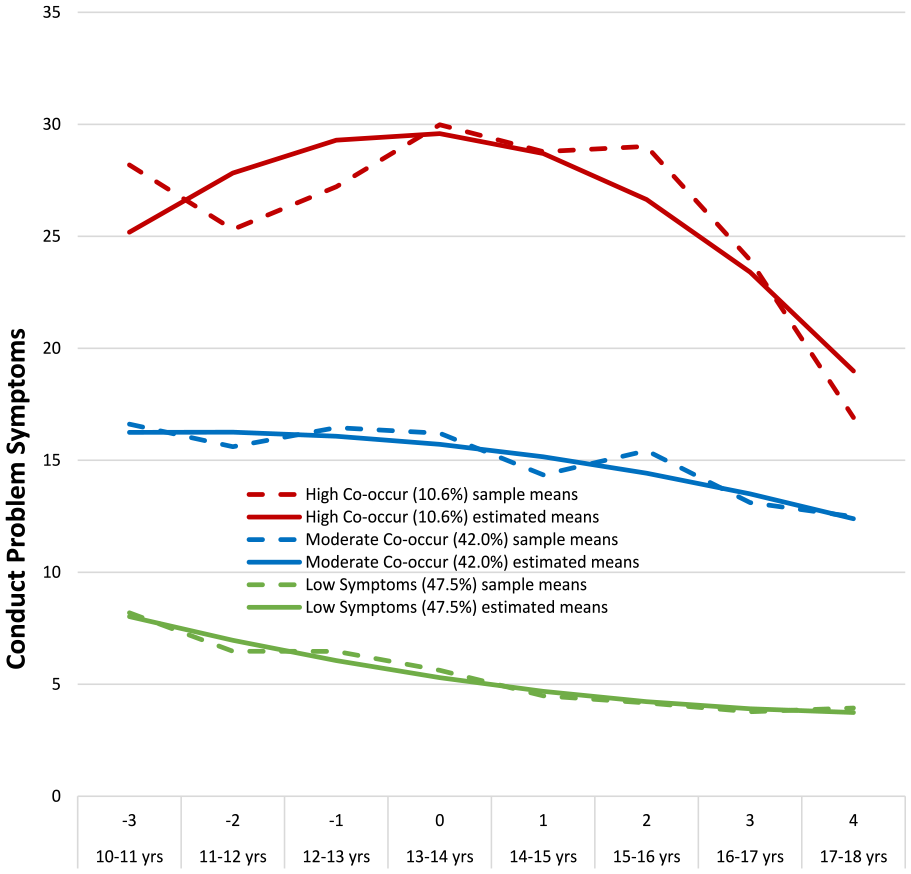
Means for conduct problem symptoms and depressive symptoms by co-occur group.
Association of trajectory class membership with clinical cutoff levels of symptoms
The number of waves at which boys’ scores were above the clinical cutoffs for depressive symptoms and conduct problems within each of the 3 trajectory classes was examined. Cutoffs were based on a score of 15 or higher on the CDRS, 20 or higher on the CES-D, and T-score of 64 or higher on the CBC-L externalizing scale. The High Co-occur group (N = 21) was above the cutoff for depressive symptoms a mean of 1.81 times (SD = 1.69) and above the cutoff for conduct problems a mean of 6.05 times (SD = 1.43). The respective statistics for the Moderate Co-occur group (N = 88) were 0.80 (SD = 1.83) and 1.90 (SD = 1.52), and for the Low Symptoms group (N = 97) were 0.52 (SD = 0.95) and 0.09 (SD = 0.36).
Analyses of variance indicated significant differences among the trajectory groupings for both depressive symptoms (F[2,203] = 12.50, P < .001) and externalizing symptoms (F[2,203] = 254.60, P < .001). Note also that the number of waves in which the boy was above the clinical cutoff for depressive symptoms and externalizing symptoms, respectively, were associated (r = .248, P < .001, n = 206). Thus, if they met clinical criteria on multiple occasions for conduct problems they were likely to meet clinical criteria on multiple occasions for depressive symptoms.
Associations of co-occurring symptom classes in adolescence with substance use in early and midadulthood
Shown in Table 3 are the findings for class associations with substance use in early adulthood (Column I) and midadulthood (Column II). In early adulthood, the classes were significantly associated with cannabis use, tobacco use, and illicit substance use but not with alcohol use. Specifically, participants in the High Co-occur class had significantly higher levels of cannabis use and illicit substance use in early adulthood compared to either of the other 2 classes, and higher use of tobacco relative to those in the Low Symptoms class.
Equality tests of means for early and midadulthood substance use across latent co-occur classes.
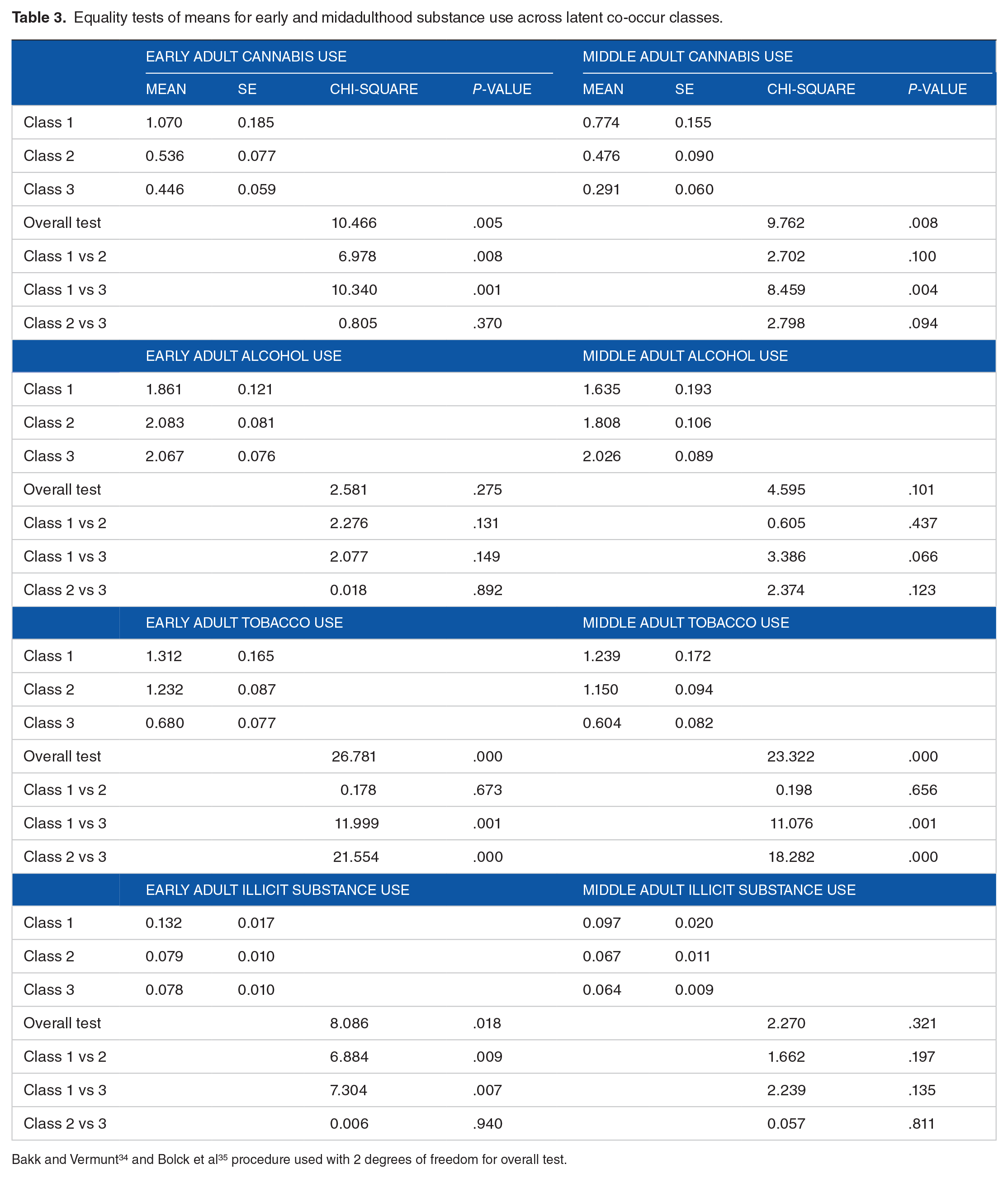
Findings for associations of the adolescent co-occurring symptom classes with substance use in midadulthood indicated that, relative to the Low Symptoms class, the High Co-occur class had significantly higher levels of cannabis and tobacco use, but not alcohol or illicit substance use. Thus, findings for early adulthood and midadulthood were similar with respect to cannabis, tobacco, and alcohol use, but differed for illicit substance use.
Independent and interacting effects of adolescent symptom domains on later substance use
Departing from the latent class approach, we next used regression analyses to predict substance use in both early and midadulthood from conduct problems and depressive symptoms during adolescence, with a focus on substance use outcomes that showed a significant association with the classes in the prior analyses (Table 4). For each substance, 4 models were tested. Model I involved 2 separate regression analyses from depressive symptoms and conduct problems, respectively. Model II included both predictors. Model III added the interaction between depressive symptoms and conduct problems to the model. Finally, Model IV included a control for adolescent use of the outcome substance.
Regression models (standardized estimates) of early and middle adult substance use on adolescent depressive symptoms and conduct problems.
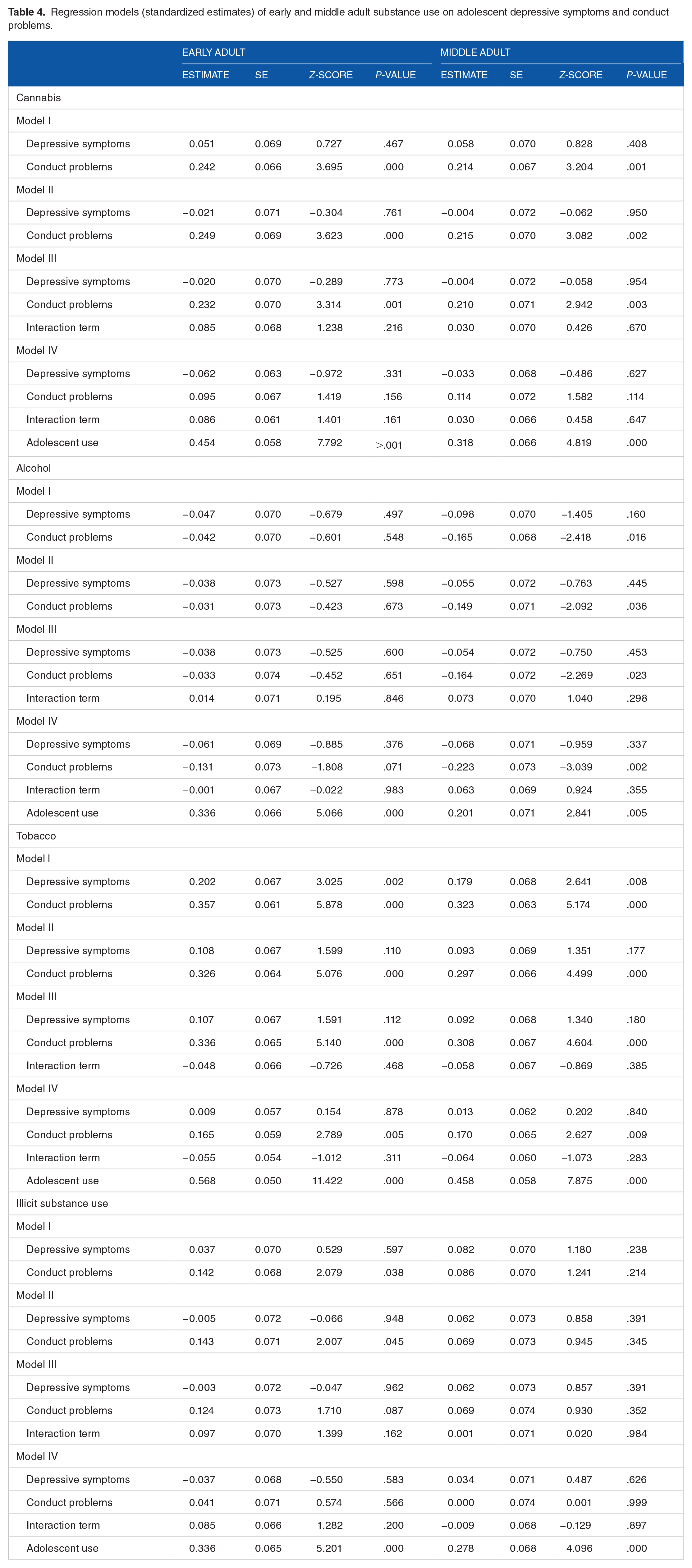
As shown in Table 4, findings indicated that only adolescents’ conduct problems were associated with cannabis use in both early and midadulthood in Models I through III. When cannabis use during adolescence was added in Model IV, adolescents’ conduct problems were no longer a significant predictor of their adult use. For tobacco, when conduct problems and depressive symptoms in adolescence were modeled separately (Model I), they were associated with tobacco use in both adult periods. In Model II, however, only conduct problems were significantly associated with tobacco use in the adult periods, and the Model III interaction terms were not significant. Adolescents’ conduct problems remained a significant predictor of their early and midadult tobacco use in Model IV, controlling for tobacco use in adolescence.
Finally, conduct problems in adolescence were significantly associated with illicit drug use in early adulthood in Model I and when depressive symptoms were controlled (Model II); adolescents’ depressive symptoms did not predict their later illicit drug use in either model, and neither predictor was significant in Model III. Neither forms of symptoms of psychopathology in adolescence were predictive of illicit substance use in midadulthood.
Discussion
As hypothesized, a dual-trajectory model of symptoms during adolescence identified latent class of boys with high, moderate, and low levels of co-occurring conduct problems and depressive symptoms. The High Co-occur class of boys showed higher levels of cannabis and illicit substance use during early adulthood than either of the Moderate Co-occur or Low Symptoms classes, and higher use of cannabis than the Low Symptoms class in midadulthood. Adolescents with co-occurring symptoms also showed overall higher vulnerability to use of tobacco in these 2 periods, but not to higher use of alcohol. However, higher levels of substance use during adulthood was only predicted by boys’ adolescent conduct problems and not by their adolescent depressive symptoms. Thus, no independent pathway to adult substance use via adolescent depressive symptoms was identified, and findings were not supportive of the dual-trajectory hypothesis 19 that both conduct problems and depressive symptoms are pathways to adult substance use—at least in men from at-risk backgrounds. Furthermore, associations of boys’ conduct problems with their cannabis, alcohol, and illicit drug use in adult periods were accounted for by their use of the respective substances in adolescence; only adult tobacco use remained associated with earlier conduct problems when tobacco use during adolescence was controlled. It is well established that conduct problems in youth predict substance use in adolescence. 36 For this sample of men, it seems that this association was sufficiently robust that no independent association remained between conduct problems in adolescence and later substance use in adulthood once adolescent substance use was considered.
Prevention implications of the study would indicate that the chief target for programs in adolescence aimed at preventing longer-term substance use should be conduct problems rather than depressive symptoms, at least for boys from at-risk backgrounds. However, the observation that these men as adolescents also showed higher levels of depressive symptoms indicates a relatively complex picture of psychopathology. Thus, also addressing adolescent boys’ depressive symptoms may provide better leverage on their conduct problems and on later substance use via this route, as well as preventing other threats to adult health and adjustment associated with early depressive symptoms. 37
In a recent study with the OYS men of long-term risks of adolescent substance use, 38 it was found that cannabis use across adolescence and early adulthood was associated comprehensively with more detrimental psychosocial adjustment in early adulthood and midadulthood, respectively, in models that controlled for a number of early risk factors, including prior levels of the outcome variable where appropriate. Along with the findings of the present study, this indicates a high priority for public health should involve early prevention and treatment—at least for at-risk boys—that focuses on adolescents’ conduct problems and substance use, including cannabis use.
Rather surprisingly, the High Co-occur class of adolescents that was identified presently did not show higher levels of alcohol use in early or midadulthood. Alcohol use has a high prevalence overall in the U.S. population (with 69.5% of adults age 18 years and older reporting drinking in the past year, according to the National Survey on Drug Use and Health) 39 and also for the OYS men. 30 Thus, it is a relatively normative substance use behavior, which may relate to a rather different etiological pattern.
The present study addressed longer-term risk of co-occurring symptoms for substance use in both early and midadulthood for at-risk men, thus extending examination of such risk further into adulthood than prior studies. However, the contributions of more proximal symptoms of conduct problems and depression (ie, during early and midadulthood) was not tested. The question of how much continuity of symptoms into adulthood, or newly developed symptoms, may relate to substance use across adulthood should be examined.
This study made novel contributions to our understanding of longer-term risk for substance use related to adolescent psychopathology symptoms for men from at-risk backgrounds. However, there were some study limitations. First, the sample size was relatively small, affecting both power to detect effects and possibly the generalizability of findings. Relatedly, there were relatively few observations in the High Co-occur group (n = 21), resulting in uneven sizes across groups, affecting power to detect effects. If there were relatively few men at the high end of the distribution of depressive symptoms, this may relate to why men in the High Co-occur group were above the clinical cutoff for such symptoms at relatively few waves. Second, these hypotheses should be tested for women and in more ethnically diverse samples. The dual hypothesis regarding risk for substance use from both conduct problems and depressive symptoms may be more applicable to women, for whom depression is more prevalent than men, estimated at 2:1. 40 Third, the measure of conduct problem symptoms in adolescence involved only parental reports. Mitigating this limitation, however, the summary measure included both maternal and paternal reports assessed yearly for 8 years. It is possibly that findings may have differed if other measures of conduct problems had been used (eg, self-report delinquency or official arrest records).
Findings of the present study indicated that boys from at-risk backgrounds with higher levels of co-occurring conduct problems and depressive symptoms in adolescence were at risk for higher levels of use of a number of substances in adulthood, including cannabis. However, this risk did not extend to higher use of alcohol in adulthood, and the overall effects on substance use were largely accounted for by use of the equivalent substance in adolescence. Although conduct problems showed stronger prediction to adult substance use than did depressive symptoms, the complex psychopathology of vulnerable at-risk boys should be taken into account in prevention and treatment programs.
Supplemental Material
sj-docx-1-sat-10.1177_11782218231204776 – Supplemental material for The Co-Occurrence of Conduct Problems and Depressive Symptoms From Childhood to Adulthood for Men: Stability Over Time and Prediction to Substance Use
Supplemental material, sj-docx-1-sat-10.1177_11782218231204776 for The Co-Occurrence of Conduct Problems and Depressive Symptoms From Childhood to Adulthood for Men: Stability Over Time and Prediction to Substance Use by Deborah M Capaldi, Stacey S Tiberio, David CR Kerr and Lee D Owen in Substance Abuse: Research and Treatment
Footnotes
Author Contributions
Deborah M Capaldi: Conceptualization, Writing original draft - Review and Editing, Funding acquisition; Stacy S. Tiberio: Conceptualization, Methodology, Writing - Review and Editing; David C. R. Kerr: Conceptualization, Writing - Review and Editing, Funding Acquisition; Lee D. Owen; Methodology, Formal Analyses, Writing Measures Section, Table and Figure Preparation, Review and Editing.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Health (NIH), U.S. PHS to Drs. Capaldi and Kerr: Award Number R01 DA 015485 (Intergenerational Studies Consortium: Understanding Mechanisms of Family Substance Use Transmission and Effects of Marijuana Legalization) from the National Institute on Drug Abuse (NIDA). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or NIDA. NIH and NIDA had no further role in study design; in the collection, analysis, and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication. We thank Shivan Tucci and the Oregon Youth Study—3 Generational Study team for high-quality data collection. Sally Schwader (Oregon Social Learning Center) provided editorial assistance with this manuscript and is submitting on behalf of the authors. Sally Schwader was supported by grant number R01 DA015485. The authors approved Sally Schwader as submitter of the manuscript on their behalf, and all aspects of the submitted document. The authors have authorized the submission of the manuscript via third party and approved statements and declarations of conflicting interests and funding.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.