
Abstract
African-American adolescents experience disproportionate rates of negative consequences of substance use despite using substances at average or below-average rates. Due to underrepresentation of African-American adolescents in etiological literature, risk and protective processes associated with their substance use require further study. This study examines the role of parental support in adolescents’ conduct problems (CPs), depressive symptoms (DSs), and alcohol and marijuana use in a national sample and a high-risk sample of African-American adolescents. In both samples, parental support was inversely related to adolescent CPs, DSs, and alcohol and marijuana use. CPs, but not DSs, partially mediated the relation of parental support to substance use. Results were consistent across the national and high-risk samples, suggesting that the protective effect of parental support applies to African-American adolescents from a range of demographic backgrounds.
Introduction
African-American adolescents are exposed to disproportionate rates of known risk factors for substance use and mental health difficulties, particularly contextual risk factors such as poverty, discrimination, and neighborhood violence.1–3 Negative consequences of alcohol and marijuana use are amplified for African-Americans despite average or below-average prevalence of use among African-American youth. 4 Alcohol use and marijuana use are more strongly related to school dropout, substance use disorders, and physical health consequences among African-Americans versus White Americans, making substance use by African-American adolescents a serious public health concern.5,6 Despite disproportionate exposure to risk factors, the prevalence of substance use and mental health disorders among African-American adolescents is comparable to or lower than national averages,4,7 indicating the presence of protective factors to mitigate the impact of those risks.
Supportive parenting has been highlighted as an important protective factor for African-American adolescents.8,9 However, African-American adolescents are underrepresented in much of the extant substance use etiological literature, and the role of parenting in the development of mental health problems and substance use is unclear. Although the representation of African-Americans in the substance use etiological literature has steadily increased over the past two decades,10–12 they still remain underrepresented and considerable work remains to address the processes underlying the development of substance use by African-American adolescents and to identify potential avenues for prevention in this group. 13 The current study examines the role of parental support in African-American adolescents’ depressive symptoms (DSs), conduct problems (CPs), and alcohol and marijuana use.
Parental Support, Adolescent Mental Health, and Substance Use
Positive relationships with parents promote psychological well-being and protect against both substance use and mental health problems in African-American adolescents.9,14–17 Parental support, which refers to behaviors such as warmth and talking with the adolescent about his or her problems, may be particularly important for African American adolescents’ development as African American adolescents tend to maintain stronger ties with family members during adolescence and tend to be more parent- than peer-oriented compared to White adolescents.8,18,19 Parental support has been offered as one explanation for why African-American adolescents often use fewer substances despite relatively high rates of exposure to contextual risk factors. 8 Contextual risks such as exposure to violence and living in poverty are positively associated with adolescent alcohol and marijuana use.20,21 Similarly, prenatal exposure to substances, cocaine in the case of the current high-risk sample, is a biological risk factor for later use of a variety of substances, including not only cocaine but also alcohol and marijuana.22,23 In the face of these and other risks of substance use, parental support can function as a powerful protective factor; however, the mechanisms by which supportive parenting relates to reduced alcohol and marijuana use are unclear.
We examined whether supportive parenting exerts part of its protective association with alcohol and marijuana use via the lower levels of symptoms of two prevalent mental health problems, CPs and DSs. CPs refers to rule-breaking behaviors such as aggression and delinquency. DSs refers to symptoms such as sadness and hopelessness. CPs and DSs are known to relate to alcohol and marijuana use in the general adolescent population, although how these symptoms relate among African-American adolescents, particularly whether there is within-group heterogeneity in their effects, requires additional research.11,24–26
CPs and DSs typically precede substance use, emerging on average at least three to four years before alcohol and marijuana use in adolescence.27–29 CPs is a robust predictor of alcohol and marijuana use; adolescents with higher levels of CPs also tend to have higher levels of alcohol and marijuana use.24–26,30 The relation between DSs and alcohol and marijuana use during adolescence is less clear. Although some studies found a positive effect of DSs on alcohol and marijuana use,11,31 others failed to detect a significant effect.32,33 We chose to test DSs as a mediator of the association between parental support and alcohol and marijuana use based on the known association between parental support on DSs and the need for more research on the relation of DSs to alcohol and marijuana use, particularly among African-American adolescents.
Within-Group Approach
A common criticism of research on racial and ethnic minorities is the tendency to compare their development and outcomes to a racial majority reference group. An alternative approach is to perform a within-group study.34,35 Within-group research focuses on defining a psychological process within one racial or ethnic group without comparing to another group or relying on previously defined frameworks based on other racial or ethnic groups. Within-group studies are the opposite of racial/ethnic comparative studies, which highlight differences between racial and ethnic groups but generally do not explain within-group heterogeneity in outcomes or in the developmental processes that lead to them. 36 Within-group research does not assume that psychological processes operate equivalently among all racial and ethnic groups; instead, it tests empirically how psychological processes occur within nonmajority groups. 37
The advantages of within-group research are best realized with a sample whose characteristics other than race are diverse. Maximal variance in characteristics that may impact psychological processes will help to reveal those characteristics that differentiate outcomes within a particular group. Given that such information does not always exist within a single dataset, another option is to combine multiple, complementary datasets to achieve heterogeneity in predictors of interest. Here, we combined a nationally representative sample and a high-risk sample to enable within-group analysis of racially homogeneous but otherwise diverse samples.
Two research questions were tested: (1) Do CPs and DSs mediate the impact of parental support on alcohol and marijuana use in African-American adolescents? (2) Do the relations between parental support, CPs and DSs, and alcohol and marijuana use vary between a high-risk and a national sample of African-American adolescents? We hypothesized that CPs would mediate the impact of parental support on alcohol and marijuana use in both samples. No hypothesis was formulated regarding the mediation by DSs due to the unclear nature of the relation between DSs and alcohol and marijuana use in the extant literature. It was expected that the relation of parental support to alcohol and marijuana use and the mediation by CPs would operate similarly in the high-risk and national samples, despite differential individual characteristics and exposure to risk factors, based on previous research that documented the strong roles of parental support and CPs in predicting alcohol and marijuana use.
Method
Sample
Data are drawn from two studies. The first sample consisted of participants in the School-Based Evaluation Study (SCHOO-BE), a prospective longitudinal investigation of long-term effects of prenatal cocaine exposure. 38 In this study, African-American mothers were recruited prospectively from prenatal care clinics in a large Midwestern city over a 24-month period, 1988–1991, during the crack cocaine epidemic. Those who had engaged in prenatal alcohol and drug use were oversampled; 34% of the children in the current sample were prenatally exposed to cocaine. Given high rates of prenatal exposure to substances and of risk factors such as childhood poverty and violence exposure, SCHOO-BE adolescents are at high risk for substance use. Data were collected prenatally, at birth, and when the child was at the age of 7 and 14. The current study used data from the age 14 wave, which were collected from 2003 to 2005 (N = 432). Additional information regarding the study protocol is available in the literature.22,38,39
The second sample was drawn from the Monitoring the Future (MTF) study. MTF conducts annual nationally representative, cross-sectional surveys that track behaviors and attitudes of American youth, with a primary focus on substance use and its predictors. 4 Approximately 17,000 eighth grade students in 150 public and private schools are surveyed each year. The sample for the current study was selected to match the age and data collection year of the SCHOO-BE study participants. Therefore, the MTF study sample included all the African-American eighth graders (modal age 14 years) who participated in the MTF surveys conducted from 2003 to 2005 (N = 2123).
Integrative data analysis
Integrative data analysis (IDA) was used to generate comparable measures of the constructs of interest across the two samples. IDA is a method of combining data across multiple datasets when measures are similar but not exactly the same.40,41 IDA operates on the measurement side of an analytic model to identify like measures, scale them equivalently, and test whether they function similarly across samples. IDA can be used to combine studies that measure the same constructs in samples of different ages or the same constructs in multiple reporters, and it can also be used to combine samples to increase the heterogeneity of a study sample.42,43 Here, we apply IDA to facilitate within-group analysis by increasing the heterogeneity of an African-American adolescent sample.
According to the developmental psychopathology framework, a thorough understanding of risk processes results from the study of both high-risk populations and large-scale epidemiological studies, which together yield complementary knowledge regarding processes that underlie both typical and atypical development.44–47 While this has traditionally been accomplished through separate studies or through parallel analyses of separate samples within one study, a next logical step is to integrate multiple data sources. Compared to a traditional parallel analysis approach, IDA offers the advantage of an empirical test of whether the process is the same across studies after equating measurement to ensure that observed similarities or differences are not attributable to between-study differences in the measurement.
Following the standard IDA procedures, 40 potential items were selected from each study based on face validity in assessing the construct of interest and use in previous research to represent the construct of interest. The pool of potential items from each study was then reduced by identifying the most similar items across the two studies, based on the comparability of the item text and measurement scale. Table 1 contains the original text and scales of measurement of the selected items. Item scales were harmonized to create an equivalent scale of measurement for each construct across the two samples. Harmonization occurs by identifying like points on the measurement scales of the items across studies, collapsing categories as needed until the items can be scaled comparably.40,48
Original and harmonized items from the SCHOO-BE and MTF samples.

Measures
Parental support was measured via one item in each study. In SCHOO-BE, adolescents were asked to respond to one item from the Survey of Children's Social Support 49 using a scale of 1–5 (1 = “always,” 2 = “most of the time,” 3 = “sometimes,” 4 = “hardly ever,” and 5 = “never”): “Some kids can count on their family for help or advice when they have problems, but other kids cannot. Can you count on your family for help or advice when you have problems?” In MTF, adolescents were asked, “If you were having problems in your life, do you think you would talk them over with one or both of your parents?”, on a scale of 1–3 (1 = “no,” 2 = “yes for at least some of my problems,” and 3 = “yes for most or all of my problems”). Responses of 1 in the MTF sample and 4 or 5 in the SCHOO-BE sample were coded 1, indicating little or no parental support. Responses of 2 in the MTF sample and 3 in the SCHOO-BE sample were coded 2, indicating some parental support. Responses of 3 in the MTF sample and 1 or 2 in the SCHOO-BE sample were coded 3, indicating high levels of parental support.
CPs were measured in SCHOO-BE by adolescents’ reports of their engagement in behaviors that are part of the diagnostic criteria for conduct disorder in DSM-IV on a scale of 0 = “never or rarely,” 1 = “sometimes,” 2 = “often,” and 3 = “very often” by four items: “initiates physical fights,” “has been physically cruel to people,” “stolen items of nontrivial value without confronting a victim,” and “has deliberately destroyed others’ property (other than by fire setting).” In MTF, CPs was measured via four items on a scale of 1 = “never,” 2 = “once,” 3 = “twice,” 4 = “3 or 4 times,” and 5 = “5 or more times”: “In the past twelve months, how often have you… (gotten into a serious fight at work or school, hurt someone badly enough to need bandages or a doctor, stolen something worth $50 or more, damaged school property on purpose)?” SCHOO-BE responses of 1 or higher and MTF responses of 2 or higher were coded 1, indicating any endorsement of that behavior; remaining responses were coded 0, indicating no endorsement of that behavior.
DSs were measured in SCHOO-BE via three items from the Child Behavior Checklist 50 on a scale of 0 = “not true,” 1 = “somewhat or sometimes true,” and 2 = “very true or often true”: “there is very little he/she enjoys,” “unhappy, sad, or depressed,” and “feels worthless or inferior.” In MTF, DSs was measured by three items on a scale of 1 = “disagree,” 2 = “mostly disagree,” 3 = “neither,” 4 = “mostly agree,” and 5 = “agree”: “I enjoy life as much as anyone,” “It feels good to be alive,” and “I feel I am a person of worth, on an equal plane with others.” Items were reverse coded such that higher scores indicated greater levels of DSs. Responses of 1 or 2 on SCHOO-BE items and 4 or 5 on MTF items were coded 1, indicating any endorsement of the symptom. The remaining responses were coded 0, indicating no endorsement of the symptom.
Alcohol use was measured via two items assessing frequency of alcohol use in each sample. In SCHOO-BE, the adolescent was asked about drinking beer and wine versus hard alcohol in two separate items from the Child Health and Illness Profile (CHIP) 51 on a scale of 1 = “never,” 2 = “more than a year ago,” 3 = “in the past year,” 4 = “in the past month,” and 5 = “in the past week”: “When was the last time you drank [beer or wine/hard liquor]?” The higher of the two responses was used to represent last alcohol use. In MTF, the adolescent was asked, “On how many occasions have you had alcoholic beverages to drink – more than just a few sips – in the past 12 months?”, on a scale of 1 = “never,” 2 = “1–2,” 3 = “3–5,” 4 = “6–9,” 5 = “10–19,” 6 = “20–39,” and 7 = “40 or more.” A second MTF item regarding lifetime prevalence of alcohol use was used to identify adolescents who had never used alcohol during their lifetime. Those who indicated no lifetime use in MTF and those who responded “never” in SCHOO-BE were coded 0, indicating they had never used alcohol. Those in MTF who indicated they had used during their lifetime but not within the past year and those in SCHOO-BE who responded they had last used “more than a year ago” were coded 1, indicating the alcohol use more than one year ago. Those in MTF who indicated using alcohol 1–2, 3–5, or 6–9 times within the past year and those in SCHOO-BE who indicated they had last used alcohol “within the past year” were coded 2, indicating the last alcohol use occurred within the past year. Those in MTF who reported using alcohol 10–19 or 20–39 times in the past year and those in SCHOO-BE who indicated they had used “in the past month” were coded 3, indicating the alcohol use within the past month. Finally, those in MTF who indicated they had used alcohol 40 or more times during the past year and those in SCHOO-BE who indicated they had last used alcohol “in the past week” were coded 4, indicating the alcohol use within the past week.
Marijuana use was assessed via one item in each sample. In SCHOO-BE, the adolescent was asked “When was the last time you used marijuana?”. This item from the CHIP was measured on the same scale as alcohol, ranging from 1 = “never” to 5 = “in the past week.” In MTF, the adolescent was asked, “On how many occasions (if any) have you used marijuana (weed, pot) or hashish (hash, hash oil) during the last 12 months?”, on the same 1–7 scale as alcohol use. As with alcohol, a second item regarding lifetime use of marijuana was used to identify those who had not used marijuana in their lifetime. The scales were harmonized in the same manner as the alcohol scales, described above, yielding a 5-point scale ranging from 0 = “never” to 4 = “in the past week.”
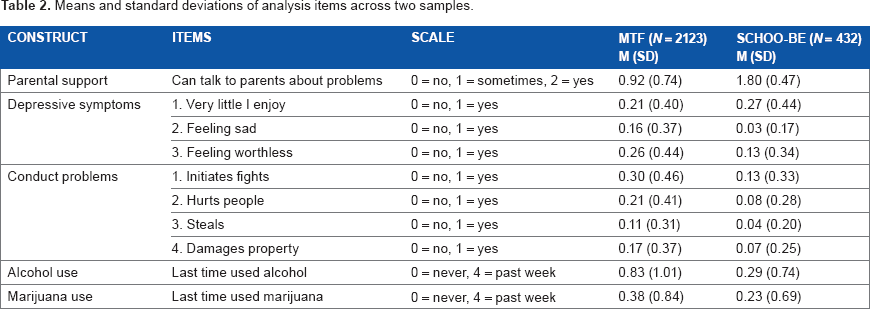
Table 2 contains the means and standard deviations of all analysis variables on the harmonized scales. All data were self-reported except adolescent DSs in the SCHOO-BE sample, which were reported by the parents.
Means and standard deviations of analysis items across two samples.
Preliminary analyses
Bivariate correlations among the harmonized study variables are presented in Table 3. Preliminary analyses using the harmonized variables were conducted as part of the IDA, following the guidelines of Bauer and Hussong. 40 First, exploratory factor analyses were conducted to ensure unidimensionality of the CPs and DSs factors in each sample separately. Both factors were found to be unidimensional in each study. Next, a measurement model was fitted to test for measurement invariance across the two studies. Separate measurement models were specified for alcohol and marijuana use. The measurement models were specified as multiple group models, with study as the grouping variable. All factor loadings were constrained to be equal across study. Factor means and variances were free across study. Both measurement models fit well (CFI > 0.99, TLI > 0.99, RMSEA < 0.03), indicating measurement invariance across the two studies. Factor loadings were thus constrained to be equal across studies in subsequent analyses.
Zero-order correlations of study variables.

P < 0.05.
Analysis
Analyses were conducted in Mplus Version 6.152 using weighted least squares with robust standard errors to account for categorical indicators of factors and full information maximum likelihood (FIML) to account for missing data. With the use of FIML, <1% of available cases (21 of 2555, all from the MTF sample) were excluded due to missing data. MTF data were weighted to account for sampling probabilities. Structural equation models were used to examine parental support as a predictor of CPs, DSs, and alcohol or marijuana use, with CPs and DSs as mediators of the relation of parental support to alcohol and marijuana use. Models were estimated separately for alcohol and marijuana use. Differences in structural parameters across the two studies were tested using multiple group models. Measurement parameters (factor loadings, item means, and variances) were constrained to be equal across the two studies. Factor means and variances were allowed to vary across study if freeing them resulted in significant improvement in model fit (Table 4). Mediation was tested using the test of indirect effects in Mplus.
Estimates and equivalence of variable means and variances in multiple group structural equation models.

Estimates were significantly different across groups, P < 0.01.
Results
Alcohol use
As hypothesized, in both samples, parental support was inversely related to adolescent CPs, DSs, and alcohol use (Fig. 1). Also in both samples, the relation of parental support to alcohol use was partially mediated by CPs (MTF: Z = -4.23, P < 0.05; SCHOO-BE: Z = -2.49, P < 0.05) but not DSs, indicating that the effect of parental support with lower levels of adolescent alcohol use was partially explained by its negative effect on CPs and the subsequent association of lower CPs with lower alcohol use. In MTF, the mediation by CPs explained 54% of the direct effect of parental support on alcohol use. In SCHOO-BE, it explained 33% of the direct effect. The model explained significantly more variance in alcohol use in the MTF than SCHOO-BE sample (MTF: R2 = 0.21, SCHOO-BE: R2 = 0.06).
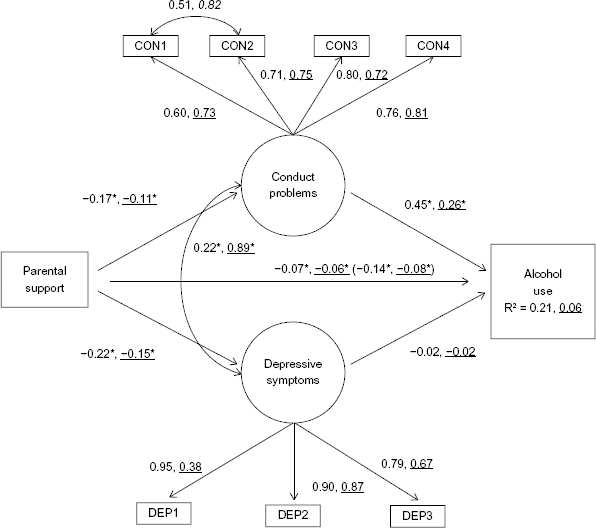
Multiple group structural equation model testing mediation of the association of parental support with alcohol use among African-American adolescents. N = 2102 (MTF), N = 432 (SCHOO-BE), X2(55) = 101.9, P < 0.001, CFI = 0.99, TLI = 0.99, RMSEA = 0.03. Underlined coefficients refer to the SCHOO-BE sample; Roman font coefficients refer to the MTF sample. Standardized coefficients are presented. Numbers in parentheses indicate the direct effect of parental support on alcohol use before adding mediators to the model. All factor loadings and all path coefficients with the exception of conduct problems to alcohol use are constrained to be equal across datasets at the unstandardized level; apparent differences are due to standardization. *P < 0.05.
Marijuana use
The results for marijuana use were similar to those for alcohol use (Fig. 2). In both samples, parental support was inversely related to adolescent CPs, DSs, and marijuana use. Also in both samples, the relation of parental support to marijuana use was partially mediated by CPs (MTF: Z = -4.42, P < 0.05; SCHOO-BE: Z = -2.23, P < 0.05) but not DSs. The effect of parental support on lower levels of marijuana use was partly mediated by parental support's negative association with CPs and the subsequent association of lower CPs with lower alcohol use. In MTF, the mediation by CPs explained 56% of the direct effect of parental support on marijuana use. In SCHOO-BE, it explained 35% of the direct effect. After accounting for the mediation, the direct association of parental support with marijuana use was no longer significant in either sample. The model explained significantly more variance in marijuana use in the MTF than SCHOO-BE sample (MTF: R2 = 0.15, SCHOO-BE: R2 = 0.06).
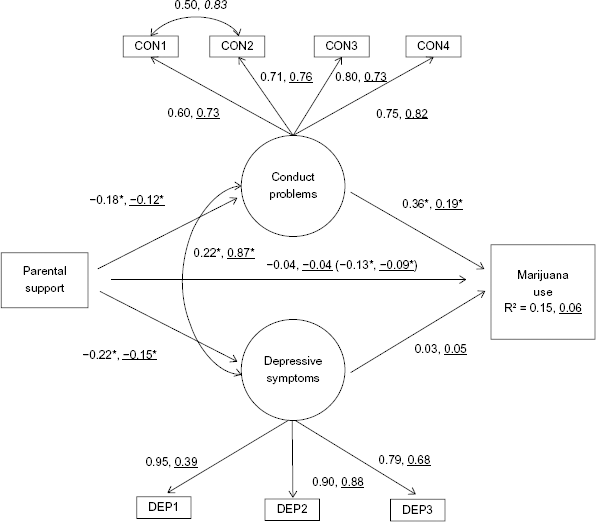
Multiple group structural equation model testing mediation of the association of parental support with marijuana use among African-American adolescents. N = 2117 (MTF), N = 432 (SCHOO-BE), X2(55) = 94.6, P < 0.001, CFI = 0.99, TLI = 0.99, RMSEA = 0.02. Underlined coefficients refer to the SCHOO-BE sample; Roman font coefficients refer to the MTF sample. Standardized coefficients are presented. Numbers in parentheses indicate the direct effect of parental support on marijuana use before adding mediators to the model. All factor loadings and all path coefficients with the exception of conduct problems to marijuana use are constrained to be equal across datasets at the unstandardized level; apparent differences are due to standardization. *P < 0.05.
Discussion
This study demonstrated that African-American adolescents who report more supportive parenting experience lower levels of DSs, CPs, marijuana use, and alcohol use. This was equally true in the SCHOO-BE sample, who are at high risk for mental health and substance use problems due to high rates of prenatal substance exposure, poverty, custodial changes, and violence exposure, and in the national sample of African-American adolescents from the MTF study. Our findings are consistent with previous work that has demonstrated the power of supportive parenting for high-risk African-American adolescents and with studies that have found that CPs but not DSs are associated with alcohol and marijuana use.32,33
Our findings add to the literature in two respects. First, they demonstrate the role of reduced CPs as a mediator of the previously identified protective effect of parental support on adolescent alcohol and marijuana use. Adolescents who feel more supported by their parents have lower levels of CPs, and those who have lower levels of CPs use less alcohol and marijuana. Second, our results provide further evidence that parental support is protective against mental health problems and alcohol and marijuana use even in families that face high levels of familial and contextual risk. Thus, parental support is an important target for preventive interventions with African-American adolescents, including high-risk samples. 14 Several authors have highlighted the need to identify mediators of the effects of culturally relevant variables on developmentally important outcomes, such as alcohol and marijuana use,54,55 particularly existing protective processes, such as supportive parenting, which can be leveraged in prevention programs. 56 Leveraging the family may be particularly important given that African-American adolescents are less likely than White adolescents to receive school-based substance use prevention. 57 Successful prevention will help to reduce more serious consequences in adulthood, including substance abuse disorders, criminal involvement, and financial instability in adulthood.56,58 Prevention programs for African-American adolescents are more important than ever because the prevalence of marijuana use by this population has increased in recent years, while the overall national prevalence of marijuana use by eighth graders has decreased. In 2003, the first of the three years included in the current study, 13.0% of African-American eighth graders reported marijuana use during the past year, a prevalence comparable to the overall national prevalence of 12.8% among all racial and ethnic groups. In 2014, the prevalence of marijuana use among African-American eighth graders had risen to 13.2%, while the overall national prevalence of marijuana use among eighth graders had dropped to 11.7%. The prevalence of alcohol use among African-American eighth graders has historically been and remains lower than the national average (17.8% and 20.8%, respectively). 4 Additional research on the effects of parental support in the current context of more prevalent marijuana use is warranted.
A notable strength of this study is its integration of two complementary data sources to explore potential within-group heterogeneity in the association of parental support with mental health and alcohol and marijuana use by African-American adolescents. This integrative approach offers at least two important advantages. First, it addresses criticisms that many social science research findings may be spurious due to lack of replication59–61 by testing a built-in replication of research findings across two independent samples. Second, it allows for increased heterogeneity of the study sample. The composition of a study's sample directly affects the inferences drawn from that sample. Using IDA to combine diverse datasets enables the researcher to exploit real population diversity for explanatory purposes in identifying those within-group characteristics that matter most in the development of the behaviors of interest, alcohol and marijuana use in this case.
There were several limitations to the study. First, the cross-sectional data do not permit causal inference. They are self-reported data and represent broad measures of the constructs of interest. Second, parental support, alcohol use, and marijuana use were measured by one item each, and in the SCHOO-BE sample, adolescent DSs were reported by the parents, not the adolescents. Parent–adolescent agreement on reports of mental health symptoms can be low. 62 Adolescents tend to report higher levels of internalizing and externalizing symptoms for themselves than their parents report for them, and parents’ reports of their adolescents’ symptoms tend to correlate positively with their own levels of symptomatology. This may have influenced the results of the current study, particularly with regards to the association of DSs with alcohol use and marijuana use; we may have observed stronger associations if DSs had been reported by the adolescent. As it represents a smaller association than that of CPs with alcohol use and marijuana use, this association may have been more vulnerable to measurement concerns. Additionally, due to data limitations, we were unable to examine other potential mediators of the association between parental support and lower levels of alcohol and marijuana use, including lower levels of anxiety symptoms among adolescents and less affiliation with deviant peers, which are also linked to supportive parenting and lower levels of alcohol and marijuana use.63–66 We were limited by the measures that were available in the datasets, a common occurrence in secondary data analysis that is often viewed as an acceptable trade-off.67,68 Future research examining the extent to which reduced anxiety and affiliations with deviant peers help to explain the association between parental support and alcohol and marijuana use is warranted.
Finally, the wording of the parent support items varied slightly across the two samples, with the MTF item referring to support from parents specifically and the SCHOO-BE item referring to support from family members including parents. It may be, then, that SCHOO-BE participants reported support from other caregivers, such as grandparents or older siblings, in addition to parents. However, our analytic strategy, IDA, demonstrated that the two items performed equivalently in measurement models across the two samples, alleviating some concerns that the items measured vastly different constructs across the two samples. Moreover, formal and informal kinship care, where a nonparent relative functions in a parental role, are common among African-American families such as some of those in the SCHOO-BE sample who struggle with drug use and abuse.69–71 This item may therefore capture an ecologically valid source of parent-like support coming from a figure other than a biological parent.
Conclusions
This study illustrates that parental support protects against early alcohol and marijuana use via its role in lower CPs in African-American adolescents in both a national sample and a high-risk sample. There appears to be a broadly applicable protective association of parental support with mental health (lower levels of CPs and DSs) and alcohol and marijuana use, even in high-risk conditions.9,14,72 Thus, parental support may be an important target for preventive interventions with African-American adolescents, including urban and high-risk samples.14,54
Author Contributions
Conceived and designed the study: JM. Analyzed the data: JM. Wrote the first draft of the manuscript: JM. Contributed to the writing of the manuscript: JM, JS, LMC, JHH, MKG, JJ, RJS, VDB. Agreed with manuscript results and conclusions: JM, JS, LMC, JHH, MKG, JJ, RJS, VDB. Jointly developed the structure and arguments for the paper: JM, JS, LMC, JHH, MKG, JJ, RJS, VDB. Made critical revisions and approved final version: JM, JS, LMC, JHH, MKG, JJ, RJS, VDB. All the authors reviewed and approved the final manuscript.