
Abstract
The parent-infant relationship is critical for socioemotional development and is adversely impacted by perinatal substance use. This systematic review posits that the mechanisms underlying these risks to mother-infant relationships center on 3 primary processes: (1) mothers’ childhood maltreatment experiences; (2) attachment styles and consequent internal working models of interpersonal relationships; and (3) perinatal substance use. Further, the review considers the role of hyperkatifeia, or hypersensitivity to negative affect which occurs when people with substance use disorders are not using substances, and which drives the negative reinforcement in addiction. The authors performed a systematic review of articles (published 2000-2022) related to these constructs and their impact on mother-infant relationships and offspring outcomes, including original clinical research articles addressing relationships between these constructs, and excluding case studies, reviews, non-human animal studies, intervention studies, studies with fewer than 30% female-sex participants, clinical guidelines, studies limited to obstetric outcomes, mechanistic/biological studies, and studies with methodological issues precluding interpretation. Overall 1844 articles were screened, 377 were selected for full text review, and data were extracted from 157 articles. Results revealed strong relationships between mothers’ childhood maltreatment experiences, less optimal internal working models, and increased risk for perinatal substance use, and importantly, all of these predictors interacted with hyperkatifeia and exerted a marked impact on mother-infant relationships with less data available on offspring outcomes. These data strongly support the need for future studies addressing the additive impact of maternal childhood maltreatment experiences, suboptimal internal working models, and perinatal substance use, with hyperkatifeia as a potential moderator, and their interacting effects on mother-infant socioemotional outcomes.
Keywords
Introduction
The parent-infant relationship is critical because it relates directly to the future well-being of the child. 1 However, this relationship is highly vulnerable. In particular, maternal mental illness and substance use significantly increase risks to the integrity of this relationship.2 -4 This systematic review posits that the mechanisms underlying this risk center on 3 primary processes: (1) mothers’ childhood maltreatment experiences; (2) attachment styles and consequent internal working models of interpersonal relationships; and (3) perinatal substance use. When people experience maltreatment during childhood, including exposure to abuse, neglect or witnessed violence, 5 they are at higher risk for future use of substances early, often, and problematically.6 -10 Further, childhood maltreatment experiences, particularly at the hands of a caregiver, jeopardize the development of healthy relationships, 11 impacting internal working models, the templates which influence relationship formation across development.12,13 As maltreatment-exposed offspring enter adolescence and young adulthood, formation of partner relationships is influenced by suboptimal internal working models, increasing risk for exposure to intimate partner violence.14 -16 Additionally, the onset of substance misuse during adolescence interferes with development of adaptive coping strategies for regulating emotions and with formation of healthy interpersonal relationships, including parent-offspring relationships.17 -19 During the perinatal period, the tri-partite risks of maternal substance use, maternal childhood maltreatment experiences, and mothers’ associated internal working models of relationships converge, adding to common perinatal risks for mood disturbances and dysregulation associated with hormonal changes, increased stress, and poor sleep.20 -23
While pregnant people may consider reducing use of substances during the perinatal period,24,25 strong stigma hampers access to treatment including concerns of being reported to child protective services, and this stigma is worse in people of color and those experiencing lower socioeconomic status.26 -31 Further, the importance of these research questions is paramount given the closing of the gender gap in substance use, lower access to treatment in women, racial, ethnic, and socioeconomic disparities,32,33 lack of funding for substance use treatment, and the consequent (due to underfunding) lack of high-quality integrated programs for mothers and their infants despite encouraging clinical trial results of such interventions.34 -38 To summarize, in perinatal people with more severe maltreatment experiences and early substance use initiation, these stunted socioemotional growth trajectories lead to increased risks for two generations (parent and offspring), negatively impacting parental, dyadic, and infant socioemotional development.
When considering mothers with early life trauma and emotional dysregulation who are attempting to curtail substance use during the perinatal period, the concept of hyperkatifeia may be instructive. Hyperkatifeia is defined as greater negative affect and emotional dysregulation in the setting of withdrawal from substances and associated negative reinforcement, driving continued use to escape from negative affective tone. 39 A growing body of research highlights the key role of hyperkatifeia and negative reinforcement in the cycle of addiction, suggesting that addiction is a disorder not only of reward deficit but also of stress surfeit40 -43; thus, exposure to childhood maltreatment is not surprisingly noted as a risk factor for this phenomenon. 39 Specifically, more severe childhood maltreatment has been associated with early development of chronic negative affect and emotional dysregulation, increased risk of early-onset of substance use, and greater risk for hyperkatifeia.39,44 -46 Even without substance use, severe exposure to childhood maltreatment has been associated with chronic negative affect and emotional dysregulation.44,45,47,48 Further, substance use has worsened during the COVID-19 pandemic, with increasing number of overdoses, poorer access to care, and escalating morbidity and mortality, including in perinatal people.49 -52 More generally, the perinatal period is a stressful time and supportive interpersonal relationships are critical for new parents, putting parents who lack these supports and who use substances at greater risk for hyperkatifeia.53 -57 Thus, understanding the specific impact of hyperkatifeia in mothers whose emotional dysregulation and tonic negative affect pre-dated their substance use is critical for two reasons: (1) it can provide a window into the way that negative reinforcement, reward deficit, and stress surfeit processes act on the maternal brain; and (2) in understanding these reward deficits, we may determine how the presence of “natural rewards” like one’s infant or an increased sense of parenting competency can motivate the path to recovery and enhance engagement in substance use treatment.
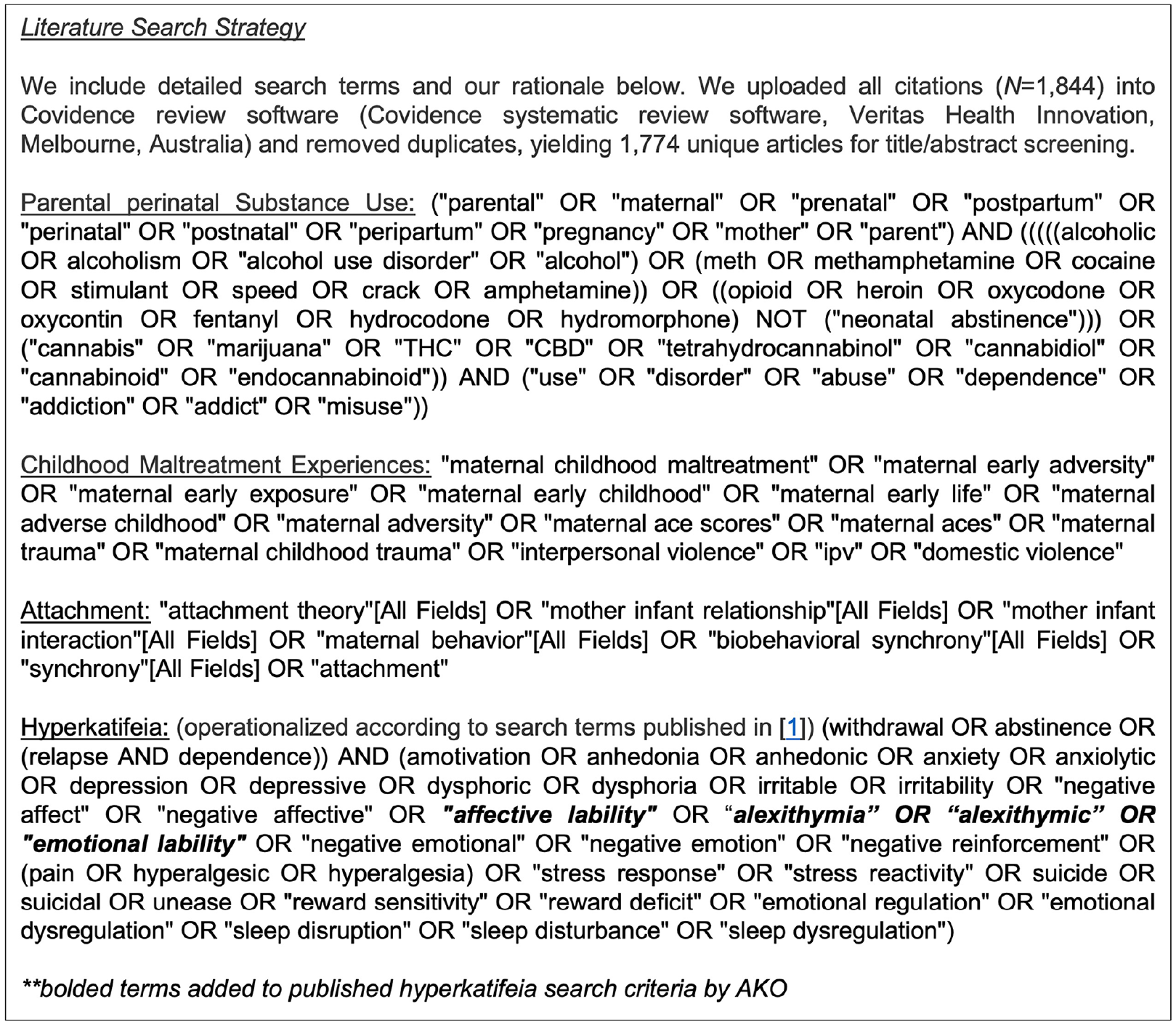
This manuscript presents data from a systematic review of hyperkatifeia and its relationship with 3 constructs (1) mothers’ childhood maltreatment experiences; (2) attachment styles and consequent internal working models of interpersonal relationships; and (3) perinatal substance use. Hyperkatifeia is operationalized according to previously published search criteria 58 (Figure 2). The goal of this review is to understand how this triad of risks impacts mothers, infants, and mother-infant dyads during the perinatal period. Additionally, this review employs a developmental approach, considering the impact of early adversity across adolescence into the mid-adult lifespan, along with tandem risks of substance use and less adaptive internal working models. The conceptual model (Figure 1) outlines the relationships between mothers’ early maltreatment experiences and their impact on relationship formation, as well as how maltreatment history and relational difficulties both predispose people to perinatal substance use. In turn, the model outlines how these constructs impact mother-infant relationships and offspring development, both via direct pathways, as well as indirectly via interactions of these 3 constructs with hyperkatifeia as a potential moderator of their effects.

Conceptual model graphic.
Methods
A detailed and systematic approach was utilized to search PubMed and PsycInfo databases for all articles published between January 2000 and October 2022 relevant to the 3 constructs (parental perinatal substance use, maternal childhood maltreatment experiences, and attachment/early life relationships) in tandem with one another and with hyperkatifeia (as defined by the search terms in Figure 2 below).
Literature search criteria.
[(perinatal substance use OR childhood maltreatment experiences OR attachment) + hyperkatifeia] OR (perinatal substance use + childhood maltreatment experiences) OR (childhood maltreatment experiences + attachment) OR (perinatal substance use + attachment)
Literature search criteria
Inclusion Criteria: articles published between January 2000 and October 2022 related to the intersection between the construct of hyperkatifeia and at least 2 of the following 3 constructs: (1) mothers’ childhood maltreatment experiences; (2) attachment styles and consequent internal working models of relationships; (3) perinatal substance use.
Exclusion Criteria: case studies; review papers; randomized controlled trials or other intervention studies; significant problems with study quality/methodology (eg, studies with N < 10 participants/cell or which use complex mediational models in cross-sectional studies); case reports; practice parameters; clinical guidelines; studies focused solely on biological males or with <30% of research population of biological female sex; toxicological studies; qualitative studies without post-analysis; pharmacological studies (treatment); biological effects of prenatal substance exposure; limited to obstetric outcomes; limited to perinatal mental health; limited to school age/latency; solely addressing factors influencing intimate partner perpetration; mechanistic studies (ie,—neuroimaging, physiology); and non-human animal studies.
Rationale for Inclusion/Exclusion Criteria: Due to this review’s focus on postnatal implications of substance use, articles solely focusing on prenatal exposure were excluded, of course while acknowledging here the impact of prenatal exposure. Due to the focus on pregnancy and the postpartum period, studies with <30% females were excluded. The extant literature on parents and children has primarily focused on cis-gender heterosexual females and thus the review focuses on this population, while acknowledging the importance of research across parental populations. Studies solely focused on domestic violence perpetration without considering victimization were excluded, as they were outside the scope of this review regarding biological females, given sex and gender patterns in perpetration. Studies solely focused on children of school-age/latency were excluded due to not falling within the intergenerational focus (ie,—early life and adolescent/adult parenthood). To be more specific with respect to this exclusion criterion, we included studies of adolescents which were relevant to them becoming parents or partnered, and we included studies of young children (infancy-toddlers) which were relevant to the relationship between maternal childhood maltreatment experiences, perinatal substance use, mother-infant relationships, and offspring outcomes. The authors added relevant terms to the published hyperkatifeia search language (italicized/bolded in search terms) 58 (see Figure 2), to capture affective lability. Non-human animal and biological mechanistic studies were excluded as they were outside the scope of this review and would merit a separate review.
Review process
For reference, number of articles by topic in the original search (N = 1844) are reported below (Figure 3). The search yielded 1844 articles, 70 of which were duplicates, leaving 1774 articles for initial screening of titles and abstracts (AKO). Next, 1397 articles did not meet inclusion/exclusion criteria. Subsequently, 377 articles underwent full text screening (AKO), with 220 excluded, and data extracted from 157 articles (see Figure 4). Next, a panel of reviewers (IC, DA, HC, BB, KK, LS, AKO) who were trained by Dr. Olsavsky on the Covidence software (Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org) extracted data from the articles using a data extraction template in which reviewers reported data from the article, coverage of various themes (whether substance use, childhood maltreatment experiences, race/ethnicity, sex as a biological variable were addressed in the articles), as well as identifying quality issues with data collection, analyses, or interpretation. Each extraction was performed by one reviewer and checked by a second, with either Dr. Olsavsky serving as the final or initial reviewer on each article.

Literature search results by topic.

PRISMA flow diagram.
Results
Overall results are first described utilizing a developmental framework. Next, interactions between each of the primary 3 predictors in the conceptual model are reported (Figure 1): (1) mothers’ childhood maltreatment experiences; (2) attachment styles and consequent internal working models of interpersonal relationships; and (3) perinatal substance use. In the sections addressing interactions of perinatal substance use and childhood maltreatment experiences with internal working models, impact on mother-infant relationships and offspring outcomes (as well as on partner relationships) is discussed. Subsequently, relationships of these constructs with hyperkatifeia will be discussed, with respect to hyperkatifeia’s role as a potential moderator of the effects of these 3 primary constructs.
Overall summary and placing findings within developmental framework
With respect to geography, of the 157 studies included, 63% were performed in the United States, 4% were performed across multiple countries, 6% in Canada, 5% in Australia, 5% in the United Kingdom, 3% in South Africa, 3% in Brazil, 3% in South Africa, 2% in Switzerland, 2% in New Zealand, 1% in Mexico, and the remainder split across various European countries. With respect to developmental stage, of the 157 articles included (Please reference Table 1 for summaries of all articles), 83 addressed the perinatal period, 38 addressed infancy, 28 addressed toddlers/young children, 42 addressed adolescence, and 133 reported data on adults of reproductive age. Of the studies included, 111 (71%) studies reported on substance use, 10 (5%) excluded participants based on substance use, and 37 (24%) neither reported on substance use nor noted it as an exclusion criterion. Reporting patterns for substance use overall were similar to those for perinatal studies, with 59 (71%) reporting on substance use, 6 (7%) excluding based on substance use, and 18 (22%) neither reporting on substance use nor listing it as an exclusion criterion. Substance use data quality varied widely, with some studies collecting self-report scales, timeline followback, or urine toxicological data, while others assessed with one yes/no question regarding amount or any use (ie, —as in large epidemiological studies), or divided groups based on substance use disorders or enrollment in treatment programs (+/– use patterns).
Summary of Relevant Articles.

Perinatal substance use and childhood maltreatment experiences
Of the included articles, 40 addressed exposure to childhood maltreatment experiences and their relationship with substance use in people of reproductive age, including adolescence through adulthood.6,8,9,33,59 -94 With respect to the 15 articles addressing the perinatal period,65 -77,94 11 articles supported associations between maternal childhood maltreatment experiences and higher risk for perinatal substance use or cravings for substances.65 -75 Of the 17 studies focused on adolescents,6,9,65,67,72,78 -87,94,95 13 supported a relationship between childhood maltreatment experiences and increased risk for substance use in adolescence and transitional age youth.6,9,78 -87,95 Of 14 studies specifically in young adults of reproductive age (which did not relate to adolescent or perinatal periods), all of these studies supported a relationship between childhood maltreatment experiences and substance use.8,33,59 -64,88 -93 The impact of each of these two domains on mother-infant relationships and offspring outcomes is addressed in the sections including interactions with internal working models, as these effects are likely mediated via this mechanism.
Childhood maltreatment experiences and impaired internal working models
The relationship between impaired internal working models with childhood maltreatment manifests across the female reproductive lifespan in 2 major ways: (1) relationships with partners; (2) relationships with offspring.
Childhood maltreatment experiences and impaired internal working models: Relationships with partners
Of the 26 papers addressing the relationship between childhood maltreatment experiences and risk for difficulties with partner relationships, 24 supported a relationship between exposure to childhood maltreatment and increased risk for intimate partner violence victimization14 -16,61 -64,67,78,80,81,83,89,91,93,96 -106 and early sexual initiation, 94 including 6 supporting these increased risks during the perinatal period,67,94,97,98,105,106 8 in adolescents and transitional age people,15,16,67,78,80,81,83,94 and 16 in adults of reproductive age.14,61 -64,89,91,93,96,99 -105
Childhood maltreatment experiences and impaired internal working models: relationships with offspring and offspring outcomes
With respect to the impact of maternal exposure to interpersonal violence (including childhood maltreatment experiences +/− intimate partner violence), out of 29 relevant articles, 25 reported on early mother-child relational outcomes.107 -109 Of these studies, 19 reported on mother-child attachment or relationship quality,14,105,110 -125 10 on maternal sensitivity or responsiveness,107,108,110,112,113,121,122,126 -128 one on maternal reflective function, 128 one on maternal structuring, 129 four on maternal intrusiveness,110,119,126,128 one on parenting competence, 130 two on harsh parenting,110,119 two on negative infant emotionality,107,108 two on child internalizing symptoms,111,115 three on child externalizing symptoms,111,115,121 and one reporting on total child psychiatric symptoms. 131 Overall, less optimal internal working models and severity of maternal mood or PTSD symptoms and alexithymia were associated with more negative parenting behaviors, lower reflective function, and negative offspring outcomes.105,110,112,113,119,122,126 -128 Further, in families impacted by intimate partner violence, children had more insecure and less stable attachment styles and male offspring were more likely to exhibit aggressive touch.120,121,123,125 By contrast, more secure maternal adult attachment style was associated with better child outcomes across multiple studies.111,115,117 Further, though substance use was not assessed in this particular study, multiple separations or losses of caregivers were associated with less optimal offspring socioemotional development. 114 Finally, maternal depressive symptoms worsened and more optimal parenting buffered against effects of childhood violence exposure.107 -109
Perinatal substance use and impaired internal working models
As referenced previously, the relationship between impaired internal working models with substance use manifests in 2 major ways in the context of this review: (1) relationships with partners; (2) relationships with offspring.
Perinatal substance use and impaired internal working models: Relationships with partners
Much like childhood maltreatment experiences, exposure to intimate partner violence has been associated with increased risk for perinatal substance use, though the directional relationship is unclear. Of the 31 studies reporting relevant data67,68,70,76,79,96,132 -156, 29 demonstrated associations between exposure to intimate partner violence and substance use.67,68,70,76,79,96,132 -154 Of these studies reporting higher co-incidence of intimate partner violence with substance use, two longitudinal studies reported increased substance use in women following exposure to intimate partner violence96,148, four studies reported associations between intimate partner violence and partner substance use,149 -152 one study in young adults from 25 countries highlighted relationships between alcohol use and sexual assault, 132 and another study noted racial/ethnic disparities, with African American and Hispanic but not White women exhibiting increased risk for substance use with intimate partner violence. 135 Other associated risk factors were noted in several studies, including unintended pregnancy, lower level of education, younger age, and history of military sexual trauma.138,142,145,146,153,154 These data regarding co-occurring risk factors are in line with the 19 studies reporting on early initiation of sexual intercourse (⩽15 years old in most of these studies)81,83,101,132,146,147,157 -160 and unintended pregnancy,83,133,138,146,150,153,161 -164 all of which support relationships between these reproductive risks, intimate partner violence, and/or substance use.
Perinatal substance use and impaired internal working models: Relationships with offspring and offspring outcomes
Of the 54 articles pertinent to associations between impaired internal working models and early parent-child relationships and offspring outcomes,14,59,62,63,71,72,76,77,92,107 -124,126 -130,134,139,147,156,165 -182 28 reported on substance use,59,62,63,71,72,76,77,92,134,139,147,156,165 -180 8 studies excluded for substance use,110 -113,126 -128,130 and 18 did not report whether it was exclusionary or measured.14,107-109,114-124,129,181,182
Of these 54 relevant articles, 41 addressed mother-infant or mother-toddler relationships,14,59,71,76,77,92,107,108,110 -117,119 -124,126 -130,139,147,166 -170,172,174,176 -180 with 18 addressing substance use. Of these 18 articles, eight focused on cocaine +/− other drugs/alcohol,59,71,166,167,169,170,172,174 two focused on alcohol,178,179 three on opioids,92,176,177 and five focused either on cravings, multiple substances, or “illicit drugs.”76,77,134,147,168 Approximately two-thirds of these pertinent studies addressed mother-infant relationships and one-third addressed mother-toddler relationships, reporting decreased maternal sensitivity,59,92,166,167,169,172,177,178 more neutral maternal affect, 178 lower structuring and higher intrusiveness, 170 more harsh parenting,170,179 higher maternal rigidity, 174 lower reflective function, 77 and high rates of parent-child separation. 134
Of the articles relevant to relational and child outcomes which reported on substance use, four addressed offspring outcomes,62,147,171,175 with two reporting on child socioemotional development,62,171 one reporting on child temperament, 147 and another reporting on child internalizing symptoms. 175 Given study heterogeneity and the low number of studies, it is difficult to make definitive conclusions, though one longitudinal study reported that prenatal substance use mediated the relationship between maternal childhood maltreatment experiences and young child internalizing symptoms. 175
Hyperkatifeia as a potential moderator
Perinatal substance use and childhood maltreatment experiences
With respect to hyperkatifeia as a potential moderator of the relationships between perinatal substance use and childhood maltreatment experiences, a total of 18 articles, including 6 with perinatal participants, 67,69 -72,76 6 including adolescents,6,78 -81,83 and 6 studies including females of reproductive age (not in perinatal or adolescent categories)8,59 -63 supported this relationship. Findings in people exposed to early adverse experiences included earlier initiation of substance use (⩽14yo), “use to cope” in adolescents, increased rates of depression and suicidal ideation, 8 higher rates of early sex or pregnancy, 67 depressive symptoms partially the moderating dose-response relationship between adverse early experiences and perinatal substance use in a longitudinal cohort, 69 the role of PTSD symptoms in the cycle of substance cravings, use, and withdrawal during pregnancy in 2 studies using ecological momentary assessment,70,76 interaction of interpersonal sensitivity and maternal stress with perinatal cocaine use, 71 and associations of maternal early adversity, perinatal substance use, and depression with offspring internalizing and externalizing symptoms. 72 Of note, these data included several population-based or longitudinal studies, with some noting even higher risk in females, which is particularly relevant for perinatal populations.78 -81,83 Further, in two additional studies with higher-risk mother-toddler dyads (mothers using cocaine and mothers experiencing homelessness), adverse childhood experiences were associated with maternal depression, substance use, and lower sensitivity, which were, in turn, related to impaired toddler socioemotional development.59,62 Thus, the negatively valenced processes associated with hyperkatifeia may be transmitted to the next generation.
Childhood maltreatment experiences and internal working models of relationships
Seventeen of the studies addressing the relationship between childhood maltreatment experiences and internal working models had a relationship with hyperkatifeia-related phenomena.14,15,62,67,78,80,81,89,91,93,97 -101,104,106 Seven studies reported on factors such as mood, anxiety, PTSD symptoms, or suicidal ideation/self-injurious behaviors67,78,81,96 -98,106, 10 reported a relationship with substance use62,67,78,80,81,89,91,93,96,97, four studies reported associations with insecure adult attachment or disengaged coping strategies,14,99,100,106 while one negative study failed to link anxious attachment and increased risk for intimate partner violence. 101
Perinatal substance use and internal working models of relationships
A relationship between perinatal substance use, suboptimal internal working models of relationships, and hyperkatifeia-related constructs was present in 12 articles,67,79,133,139,140,142,144,145,147,151,154,155 noting depressive symptoms,67,79,142,144,145 higher distress,140,155 perception of infants as dysregulated, 147 increased substance use after experiencing reproductive coercion, 133 use of substances to cope,139,151 or mothers being unable to stop use during pregnancy. 154
Discussion
Hyperkatifeia during the perinatal period—the negative reinforcement cycle
To our knowledge, this is the first systematic review to examine the relationships of maternal childhood maltreatment experiences, internal working models of relationships, and perinatal substance use, with hyperkatifeia as a potential moderator, and to assess their collective impact on mother-infant relationships and offspring outcomes. As previously stated, hyperkatifeia is characterized by hypersensitivity to negative affect and dysregulation associated with not using substances—a key component of the negative reinforcement cycle of addiction. 39 Importantly, hyperkatifeia does not simply constitute withdrawal, but rather, relates to brain plasticity underpinning addiction, via which a new (lower) hedonic set point is established. 41 Thus, even in the absence of acute withdrawal, associations between relief from negative affect and prior substance use constitute a powerful ongoing motivationally salient stimulus for continued use.183,184 Given this notion of addiction as both a reward deficit and stress surfeit problem, it is highly likely that both childhood maltreatment experiences and subsequent intimate partner violence further impact this process.39 -42 To the extent that these traumatic experiences pre-date substance use initiation, people may experience more brittle affect and emotional dysregulation at baseline.44,45 When substance use begins in adolescence, people using substances do not develop the coping skills to regulate their emotions without using substances.185 -187 Thus, once the cycle of intoxication, withdrawal, and planning to obtain substances ensues, the person is “stuck,” attempting to cope with tonic negative affect and emotional dysregulation at baseline in the absence of use. 39
Hyperkatifeia, early adversity, and substance use—beyond trauma-related and depressive DSM diagnoses
These associations between trauma exposure, negative affect, and substance use are not a novel concept. In one of the first studies of Adverse Childhood Experiences (ACEs) from 2001, a relationship between suicide attempts and ACEs across the lifespan was partially mediated by 3 factors: depressive symptoms, illicit drug use, and ‘alcoholism’, 8 with ACEs being similarly associated with substance use disorders in a parallel Canadian study. 88 Additionally, the current recommendations of the necessity to treat co-morbid conditions associated with negative affective tone (eg, depression and anxiety) simultaneously with substance use disorders underscores the importance of these relationships.188 -191
However, these phenomena go beyond the need to treat comorbid psychiatric disorders in people with problematic substance use. This work is particularly relevant to the population of pregnant people who have experienced chronic trauma starting in childhood, and who use substances to cope with affective dysregulation, as childhood trauma has been identified as an important risk factor for hyperkatifeia in people using substances.39,192 Further, given the attachment disruptions in populations living with the sequelae of severe childhood abuse or neglect, associations between mothers’ childhood maltreatment experiences and later exposure to intimate partner violence may compound affective dysregulation and negative mood at baseline in this population.44,193 -199 Additionally, certain personality traits are independent risk factors for hyperkatifeia in people using substances, which may explain to some degree the more enduring nature of this problem, and which likely relates to the lack of development of healthy coping strategies during adolescence when use often begins. 39 Relationships between partner substance use, maternal substance use, and intimate partner violence even further worsen affective dysregulation in the setting of continued trauma. 200 This relationship between suboptimal interpersonal relationships and emotional dysregulation is of particular importance during the perinatal period, as coping with changes in relationships and role function are critical during this time, and not surprisingly, one of the most supported interventions for preventing perinatal depression is interpersonal therapy.201,202 Thus, when substance use is involved in mothers who have experienced childhood trauma, risk is compounded—with the increased response to distress and emotional dysregulation at baseline which pre-dated onset of substance use, 203 now overlaid with the addiction-related synaptic plasticity underlying hyperkatifeia. 183 These processes, in turn, relate to the pharmacological downregulation of brain reward function in response to substance use, exacerbating pre-existing trauma-related vulnerability.40,41,204 Further, these phenomena jeopardize relationships with infants, who are a “natural reward” for many parents.205,206 Importantly, although the detailed mechanisms are outside the scope of the current review, the mesolimbic dopaminergic pathway undergirds motivated maternal behaviors, interacts with oxytocinergic pathways, and the oxytocin system has previously been identified as a potential clinical intervention target for substance use disorders.207 -209
Implications of perinatal substance use for mother-infant relationships
In considering relationships between substance use and maternal behaviors, there are several points which should be highlighted. First, several studies suggested that ongoing postnatal substance use versus exclusively prenatal use contributed to lower levels of mother-infant reciprocity166,170,174,176; thus, while many have emphasized the primacy of prenatal exposure, the postnatal period is also crucial for mother-infant relationship development. Additionally, in a study of mothers on medication-assisted treatment, whether mothers responded contingently to infants explained more variance in mother-infant relationships than substance use. 177 One study found not as many differences between mothers using substances compared to other high-risk samples (eg, —mothers with lower income), 92 suggesting that social determinants of health, including structural racism, should receive consideration, which is in line with previous studies.155,210,211 Lastly, the impact of the separation/loss of caregivers on offspring socioemotional development cannot be overstated. 114 With the share of US children entering foster care due to parental substance use increasing from 15% in 2000 to 36% in 2017, 212 these data collectively underscore three relevant points: (1) attachment relationships are disrupted by separation of parents and children as well as substance use itself; (2) integrated services to address mother-infant relationships, maternal substance use, and co-morbid mental health conditions are often unavailable; and (3) stigma is enormous for mothers with substance use as they seek care. The inordinate focus on prenatal substance use may drive separations of families and decrease mothers’ propensity to seek treatment for their substance use, resulting in a missed opportunity to modify mother-infant relationships in the postpartum period with appropriate and integrated treatment.
Developmental approaches for early intervention, prevention, and perinatal substance use treatment
The roles of early life caregiving, adversity, and sources of resilience are critical to consider, as they affect the relationships between mothers’ experiences of childhood maltreatment, less optimal internal working models of interpersonal relationships, and perinatal substance use. Childhood traumatic experiences and negative internal working models of relationships have reverberating effects across the lifespan for interpersonal relationships and health behaviors.213,214 Although assessing the teratogenic outcomes of prenatal substance use exposure was outside the scope of this review, it has been shown to increase risk for substance use in the subsequent generation.215 -218 Additionally, during adolescence, the life course of potential mothers is profoundly affected by early sexual initiation, substance use, peer interactions, and choice of romantic partners.219,220 Collectively, these adolescent developmental processes alter the balance between mothers’ vulnerability and resilience, impacting the perinatal period, whether or not people become parents during adolescence. When we consider the discourse in the literature surrounding “deaths of despair, 221 ” which occur across multiple racial and ethnic groups during midlife,222,223 the antecedents clearly do not start in midlife. Importantly, investigators have reported changes in infant and adolescent health during the opioid crisis.224,225 Further, social determinants of health and their impact upon young families cannot be ignored, including housing availability, 226 the impact of discrimination and structural racism on perinatal and young child health,227 -229 less supportive social policies for young families in the US (eg, —decreasing access to contraception and lack of paid family leave), 230 as well as inequalities based on race, ethnicity, and socioeconomic status in reporting of putative neglect for maternal substance use in the US. 231
The perinatal period represents an important time in life where women expecting a child may seek to improve their life circumstances and health habits including reducing substance use, although women with undertreated and more severe mental health symptoms are less likely to do so. 232 Lifecourse events including traumatic experiences such as intimate partner violence and exposure to structural racism, demographics, social determinants of health, and type of substance used influence mothers’ ability to reduce their use or to engage in treatment during the perinatal period.24,144,151,154,156 To the extent that substance use, maternal exposure to early adversity, and attachment vulnerabilities interact, in substance use treatment, providers should consider not only co-morbid mental health conditions, but also the interaction of trauma exposure, relational problems, and substance use in women during the perinatal period.
Limitations
Many articles either did not report on substance use or excluded people using substances. This is problematic due to the importance of considering substance use and trauma together since co-exposure is highly likely. Furthermore, the lack of inclusion of substance use measures may be at least partially due to the way that perinatal substance use is treated clinically in terms of reporting to child protective services, which is often not linked to immediate referral to high-quality substance use treatment. While exposure to substances is an important risk, the way that cannabis and other illegal substances are treated is largely different than alcohol. Additionally, there are known disparities in reporting to child protective services based on race, ethnicity, and socioeconomic status. All these factors may influence both research groups and participants as they decide whether to either include substance measures in projects or whether for participants, they will take part in research. This issue likely worsens both health disparities as well as disparities in research participation. In addition, since most parent-child perinatal work has been conducted in cis-gender heterosexual females, when referring to differences based on sex in pregnant or postpartum people, the words “females,” “women,” or “mothers” were used in this study. Many articles confounded sex and gender, as many did not collect data on gender identity. There is limited literature on people identifying as fathers and extremely sparse literature on LGBTQ+ parents. Expanding the research framework and parental populations studied is of critical importance for understanding these phenomena in families of all compositions, including addressing differences related to biological sex (based on chromosomal status), sexual orientation, and gender identity in future research. Additionally, only 63% of the articles included in this review which addressed offspring outcomes considered sex differences in these outcomes. Race and ethnicity were reported in only 71% of articles. In the remaining 29% either no breakdown was provided, nationality alone was provided, or investigators reported dichotomously (White/Caucasian vs not White/Caucasian). Given migration, health inequities, increasing heterogeneity of populations, and the importance of understanding the impact of structural racism on mother-infant dyads, more consistent reporting methodology would be beneficial. Despite well-known limitations associated with retrospective reporting of childhood maltreatment experiences233 -235 and lack of assessment of the impact of developmental timing and heterogeneity of adverse early experiences,236,237 many papers included in this review used longitudinal cohorts, which helped to mitigate this problem. The quality of any review depends on the quality of the underlying studies, which had considerable limitations, particularly in some of the dichotomous measures of substance use, lower frequency of articles considering gold standard measures of use patterns (ie, —timeline followback), and very low inclusion of biological measures of substance use.
Gaps in literature and future directions
Although many investigators study the impact of early adversity and substance use, it is important to account for each of these factors when considering the other, as both affect maternal and child health. In our review 29% of articles considered trauma alone (ie, —including childhood maltreatment +/− intimate partner violence exposure), 24% of articles considered maternal substance use alone, while only 47% addressed both phenomena. Given the impact of perinatal substance exposures and the relationship between maternal mental health and less optimal mother-infant relationships (even in studies where substance use was an exclusion criterion), it is critical that more in-depth perinatal studies of mothers and their offspring are performed for understanding the important impact of these phenomena on two generations. Further, studying the dynamic between one of the more potent natural rewards (babies) and hyperkatifeia in mothers during the perinatal period, may lead to treatment innovations, with goals of treating maternal substance use, decreasing parent-child separations, and improving mother-infant outcomes.
Footnotes
Author Contributions
Conceptualization: AKO, PR, KH, NT, CZ, CNE; Data curation: AKO, IC, DA, HC, BB, LS, KK; Formal analysis: AKO; Methodology: AKO, CNE Interpretation of data: AKO, IC, DA, HC, BB, LS, KK, KH, CZ, NT, PR, CNE; Writing—original draft: AKO; Writing—review and editing: AKO, IC, DA, HC, BB, LS, KK, KH, CZ, NT, PR, CNE. All authors have read and agreed to the published version of the manuscript.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Aviva K. Olsavsky receives funding from NIDA and the American Academy of Child and Adolescent Psychiatry as a NIDA/AACAP K12 awardee (K12DA031794 – PI Gray), the American Heart Association as a Consultant, and the NIMH Loan Repayment award. Dr. Diab Ali receives funding from the American Academy of Child and Adolescent Psychiatry (AACAP Pilot Award) and his research time during residency is funded by NIMH (R25MH125758). Dr. Kent Hutchison receives funding from NIAAA (R01AA029606, 75N94021D00016-759402100001), NIDA (R01DA048069), and NIA (R01AG079502). Dr. Charles Zeanah receives funding from NIMH (R01MH091363). Dr. Nim Tottenham receives funding from the NIMH (R01MH074374). Dr. Paula Riggs receives funding from NIDA (R01DA053288). Dr. C. Neill Epperson receives funding from NIMH (R25MH125758) and NICHD (R01HD105771).
Declaration of Conflicting Interests:
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.The authors report the following disclosures which are unrelated to this work: disclosures, Dr. Aviva K. Olsavsky serves as a Consultant to the American Heart Association, has received speaking Honoraria from (HMP Global), and her spouse is employed by Thermo Fisher Scientific. Dr. Charles Zeanah has received royalties from Guilford Press and Harvard University Press as well as periodic honoraria for speaking engagements to professional groups. Dr. C. Neill Epperson is a Consultant to Asarina Pharma and Sage Therapeutics, has received research funding from Sage Therapeutics and HealthRhythms, and is a Scientific Advisor for Babyscripts.