
Abstract
Objectives:
The purpose of this study was to provide insights into which patient-level characteristics are associated with a positive treatment response among patients whose primary drug of choice was a psychostimulant with a particular emphasis on understanding the impact of age at first use and co-occurring psychiatric comorbidities.
Methods:
We used a cross-sectional study design and the 2019 US Treatment Episode Data Set: Discharges (n = 167 802) to identify outpatient treatment episodes for which the primary drug of choice was a psychostimulant. We defined a positive treatment response as (1) a reduction in drug use between treatment admission and discharge or (2) no use at both admission and discharge. Multivariable logistic regression was conducted, overall and stratified by presence of psychiatric comorbidity, to identify demographic, clinical, and treatment-level factors associated with positive treatment response.
Results:
Treatment episodes among patients 11 years and under at the time of first use had a 22% higher odds of having a positive response to treatment as compared to those treatment episodes in which the person was 30 years or older at the time of first use. The presence of psychiatric comorbidity resulted in substantial differences in direction and magnitude of the relationships between treatment response and covariates. Positive response to treatment was less likely for episodes among Non-Hispanic Black/African American persons, in detoxification settings, for unemployed individuals, or for individuals living in the South, but a positive response was more likely for episodes occurring in rehabilitation/residential settings.
Conclusions:
Race/ethnicity, geographic region, treatment setting, and employment status were the strongest predictors of response to treatment. Treatment programs should maximize treatment of psychiatric conditions, intensify support for persons of color seeking treatment in detoxification settings, and increase efforts to find adequate employment for patients.
Introduction
Use of psychostimulants (eg, cocaine, methamphetamine) is a growing epidemic in the United States.1 -3 Roughly 5 million Americans misuse psychostimulants each year; use of cocaine increased by 7% in 2016 alone. From 2009 to 2019, the number of stimulant overdose deaths rose 5-fold with 63% of all stimulant deaths also involving an opioid. 2 With no effective pharmacotherapies for stimulant use disorder, it is imperative we identify patient-level factors (eg, age of drug use onset, mental health comorbidities) that promote or inhibit a positive response to treatment for stimulant use disorders. 4 Factors identified may help inform interventions delivered by drug treatment programs and may elucidate key characteristics in resource allocation decisions.
Current evidence suggests that a person’s age at the time of first use of an addictive substance is an important factor in the development of substance use disorders, including stimulant use disorders. Analyses of data from the National Survey on Drug Use and Health indicate that adults who first tried cannabis at or below 14 years of age had a 6-fold increase in diagnosis of illicit drug dependence or misuse, compared to those who first used cannabis at or above the age of 18. 5 Moreover, initiating substance use during childhood or adolescence has been linked to substantial long-term health risks such as development of substance use disorder,6 -8 polysubstance use, 7 and developmental delays. 8 Age at first substance use may also be a powerful predictor of treatment response, utilization, and completion for patients suffering from substance use disorders, especially given that current, younger age is associated with shorter retention in treatment for opioid use disorder.9 -11 Thus, early, effective strategies for preventing substance use are urgently needed. 5
Psychiatric comorbidities may also impede treatment effectiveness for stimulant use disorders. Co-occurrence of psychiatric and substance use disorders is common, with half of those with a substance use disorder also experiencing a psychiatric disorder during their lives.12 -15 Persons with comorbid psychiatric disorders, such as attention deficit hyperactivity disorder (ADHD), generalized anxiety disorder (GAD), and bipolar disorder, have been found to have poorer treatment adherence and higher dropout rates than those without these disorders. 16 Co-occurrence of ADHD has been found to be associated with discontinuation of treatment for a substance use disorder, 17 and neuroimaging studies suggest ADHD may alter the brain circuits associated with drug cravings thereby decreasing the probability of treatment success.18 -20 Persons with GAD have indicated relief of their anxieties/worries provided by substance use may ultimately interfere with the effectiveness their substance use treatment. 21 Persons with bipolar disorder have the highest prevalence of substance use disorders as compared to persons with other comorbid psychiatric disorders. This is thought to be due to the shared characteristics of bipolar and substance use disorders, including impulsivity, poor modulation of motivation, and susceptibility to behavioral sensitization. In such persons with bipolar disorder, substance use disorder treatment may be most effective when addressing these shared mechanisms. 22
Unfortunately, there is limited knowledge on patient-level factors that are associated with a person’s response to treatment for a stimulant use disorder. Therefore, the purpose of this study was to identify patient-level factors associated with SUD treatment response among persons using psychostimulants. Previous studies have identified adolescence as a critical risk period for development of substance use disorders of alcohol and cannabis, and early onset of drug use has been shown to be predictive of long term impairments such as reduced educational and occupational attainment in adulthood. 23 Thus, we hypothesized that individuals who started substance use at a younger age (eg, adolescent years) would be more likely to have a non-positive response to treatment (ie, increased utilization, or same frequency of drug use [some or daily use] at treatment completion) than individuals initiating drug use later in life. We also hypothesized that persons entering SUD treatment with a co-occurring psychiatric disorder (eg, anxiety disorders, bipolar disorder) would less likely to demonstrate a positive treatment response than those without a co-occurring psychiatric disorder. By understanding the impact of personal, environmental, and social factors that positively or negatively affect treatment response in patients admitted for psychostimulant misuse, the findings from this study could be used by providers and population health management programs to identify additional treatment needs (eg, need to address comorbid psychiatric disorders) to improve treatment retention and outcomes.
Methods
Data and inclusion criteria
We used a cross-sectional study design and the 2019 US Treatment Episode Data Set: Discharges (TEDS-D) to identify discharges in 2019 from substance use treatment facilities in which the primary drug of choice upon admission was identified as a stimulant (ie, “Cocaine/crack,” “Methamphetamine/speed,” “Other amphetamines,” or “Other stimulants”). Managed by the Center for Behavioral Health Statistics and Quality of the Substance Abuse and Mental Health Services Administration (SAMHSA), TEDS-D is a national data system of annual discharges from substance use treatment facilities across the US that provides demographic, clinical, and substance use characteristics of persons admitted (people aged 12 years and older) to facilities for treatment of alcohol or drug use disorders. This publicly available data set and corresponding codebook were retrieved from the SAMHSA.gov website. Treatment episodes for which there were no data for frequency of drug use at admission or at discharge (used to define the outcome variable) were excluded from the sample (N = 13 254; 4.15%). Since TEDS-D is publicly available, IRB approval was not warranted, and therefore, informed consent was not obtained.
Outcome: Response to treatment
The outcome of interest was a binary indicator of positive or non-positive response to treatment. Treatment response was defined as change, or lack of change, in drug use from admission to discharge; for each episode, response was determined from the TEDS-D variable of “frequency of drug use in the past month” (daily use, some use, or no use). As outlined in Pro et al, positive response to treatment was defined as (1) a reduction in use between admission and discharge (daily use to some use, daily use to no use, or some to no use) or (2) no use at both admission and discharge, under the assumption that not relapsing is a positive response for someone in treatment. No use at admission and discharge is considered a positive treatment episode in this paper and in Pro et al to recognize the substantial efforts, challenges, and successes of persons with substance use disorders on their path to recovery. Non-positive response to treatment was defined as (1) increased use from admission to discharge or (2) same level of use (some or daily use).24,25
Main independent variable: Age at first use
The primary independent variable of interest was age at first use for the primary drug upon admission (denoted in 2019 TEDS-D as column “FRSTUSE1”). This variable is broken into 7 groups by TEDS-D: 11 years and under, 12-14 years, 15-17 years, 18-20 years, 21-24 years, 25-29 years, and 30 years and over. This variable was used to test the hypothesis that initiation at an earlier age is associated with a non-positive response to treatment.
Covariates
Inclusion of each covariate was driven by findings from previous studies that evaluated substance use disorder treatment response.26 -29 Covariates included demographic, clinical, and healthcare utilization information. Demographic characteristics included gender (male or female), age at the time of treatment admission (not age of initiation of drug use) as categorized by TEDS-D (12-17 years, 18-24 years, 25-34 years, 35-44 years, 45-54 years, and 55 and over), race/ethnicity (non-Hispanic White; non-Hispanic Black/African American; non-Hispanic Alaskan Native/Native American; non-Hispanic Asian/Pacific Islander; non-Hispanic, other race(s); Hispanic, any race), geographic region of treatment (Northeast, South, Midwest, West), employment status at admission (full-time, part-time, unemployed, not in labor force), marital status at admission (never married, married, separated, divorced/widowed), and educational level at admission (middle school or less, some high school, high school/GED, some college, 4-year college/university/postgraduate study or more).
Clinical characteristics included primary psychostimulant of use at admission (cocaine/crack, methamphetamine/speed, other amphetamines, other stimulants), co-occurring mental and substance use disorders (yes/no; as defined by PSYPROB), secondary substance of use at admission (depressants, cannabinoids, opiates, hallucinogens, other drugs, no secondary drug), and route of administration for primary substance of use at admission (oral, smoking inhalation, injection, other). The healthcare utilization characteristic was service setting (detoxification, rehabilitation/residential, ambulatory). Only covariates with less than 10% of data missing in the original dataset were included in the model.
Analyses
R software (version 4.2.1) was used to conduct all analyses. Bivariate descriptive statistics were estimated for the main independent variables of interest and for all covariates (see section 2.4) in relation to the treatment outcome (ie, positive or non-positive response to treatment). Chi tests of independence were used for each covariate to assess the strength of bivariate associations between each independent variable and treatment outcome. We used multivariable logistic regression to model (1) the association between each group for age at first use and response to treatment, (2) the association between age at first use and treatment response, adjusting for all other covariates (including the presence of psychiatric comorbidity), and (3) the association between age at first use and treatment response stratified by the presence of psychiatric comorbidity, adjusting for all other covariates. We fit the model using all categories for age at first use from the TEDS-D, as well as for collapsed age groups (less than 18 years, 18-24 years, and 35 years and older), due to small sample size among some of the age groups. Treatment episodes in which any of the covariates or primary outcome of treatment response were missing data were excluded from the analyses.
Sensitivity analysis
To gain insight on the impact of different treatment settings in substance use treatment, we conducted 2 sensitivity analyses: (1) including only treatment episodes from outpatient/ambulatory treatment settings and (2) excluding treatment episodes where individuals maintained no use at both admission and discharge. We chose these 2 sensitivity analyses as treatment episodes in outpatient/ambulatory treatment settings and treatment episodes where no use is maintained at both admission and discharge may differ substantially from other treatment episodes. After restricting to only episodes from outpatient/ambulatory treatment settings or excluding those episodes where no use was maintained, we refit our overall model using the same specifications noted in section 2.5.
Results
A total of 167 802 treatment episodes were included in our final sample. Table 1 provides descriptive statistics for each demographic and clinical characteristic among individuals with positive versus a non-positive treatment response (Table 1). Roughly 57% and 67% of all treatment episodes were for males and persons who identified as non-Hispanic White, respectively. Methamphetamine was the most common (59%) primary psychostimulant used at admission, and smoking was the most prevalent (almost 52%) route of administration. The most common range for age at first psychostimulant use was 18 to 20 years of age (20.6%), and slightly fewer than half of the treatment episodes were among individuals whose highest level of education was a high school diploma or GED.
Demographic and clinical characteristics of psychostimulant treatment episodes.

Overall, 54% (N = 91 020) of persons entering treatment had a positive treatment response (ie, abstinence was maintained, or drug use reduced from treatment entry to discharge). Bivariate comparisons for all demographics included in Table 1 were significantly different between episodes with a positive response to treatment and those with a non-positive response to treatment. Notable bivariate differences include use of methamphetamine or speed as the primary psychostimulant of choice at admission (54.30% had a positive response and 45.70% had a non-positive response), geographic region of residence (70.39% had a positive response and 29.61% had a non-positive response for the Northeast region), and employment status at admission (48.15% of those unemployed had a positive response while 51.85% of those unemployed had a non-positive response).
Figure 1 provides the multiple logistic regression analyses of the data sample examining the relationship between response to treatment and patient characteristics, particularly age at first use. Treatment episodes among patients 11 years or under at the time of first use were 22% more likely to result in a positive response to treatment, as compared to treatment episodes in which the person was 30 years or older at the time of first use (adjusted odds ratio [aOR] = 1.22, 95%CI: 1.11, 1.34). A positive response to treatment was less likely for Black/African American patients (ie, 22% lower odds of having a positive treatment response), Southern patients (60% lower odds), patients being treated in detoxification settings (79% lower odds), and unemployed patients (29% lower odds). Alternatively, the odds of a positive response to treatment was higher for treatment episodes among Alaskan Native/Native American (22%) and Asian/Pacific Islander patients (30%), patients whose primary stimulant of use at admission was methamphetamine/speed (20%), and patients being treated in rehabilitation or residential settings (41%). Those without a comorbid mental health condition were found to have a 22% higher odds of having a positive treatment response compared to those with a psychiatric comorbidity.
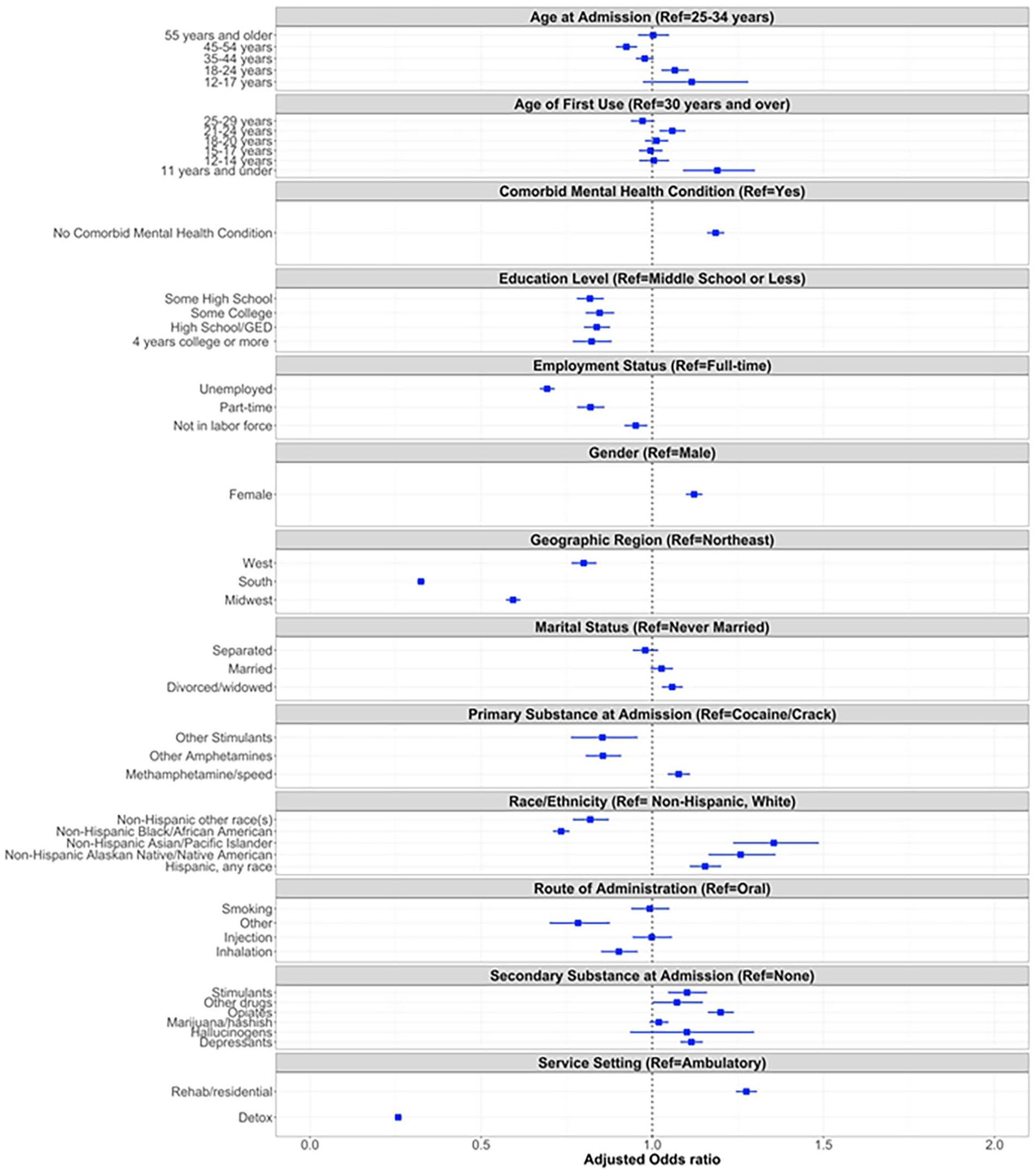
Forest plot of the results of the multiple logistic regression model with outcome as response to treatment.
Figure 2 provides the results of the multiple logistic regression model stratified by treatment episodes with psychiatric comorbidity (N = 96 610; 57.57%) and without psychiatric comorbidity (N = 71 192; 42.43%). Figure 2 provides results of the model, inclusive of the covariates, with all categories for age at first use. Table 2 provides the results only for age at first use, with age categories collapsed into 3 groups (less than 18 years, 18-24 years, and 25 years and older). Overall, the odds of experiencing a positive response to treatment was 12% higher (aOR = 1.12, 95%CI: 1.05, 1.20) for treatment episodes in which the patient had no psychiatric comorbidities and the age at first use was 12 to 14 years (as compared to those in which the age at first use was 30 years or older and had no psychiatric comorbidities). The odds of experiencing a positive response to treatment was 9% lower (aOR = 0.91, 95%CI: 0.86, 0.96) for treatment episodes in which the patient had a psychiatric comorbidity, as compared to treatment episodes in which the age at first use was 30 years or older and the patient had a psychiatric comorbidity. The odds of experiencing a positive response to treatment was 23% higher (aOR = 1.23, 95%CI: 1.07, 1.42) for treatment episodes in which the patient had no psychiatric comorbidities and the age at first use was 11 years and under, as compared to those in which the age at first use was 30 years or older and had no psychiatric comorbidities. For treatment episodes in which the age of first use was between 12 and 17 years, the presence of psychiatric comorbidity decreased the odds of a positive response by an average of 18%.

Forest plot of the results of the multiple logistic regression models with outcome as response to treatment, stratified by psychiatric comorbidity.
Distribution of adjusted odds ratios of age at first use predicting response to treatment for treatment episodes as stratified by the presence of psychiatric comorbidity (N = 167 802).

Abbreviations: aOR, adjusted odds ratio; CI, confidence interval.
P < .1. **P < .05. ***P < .01. ****P < .001.
Results of the multiple logistic regression model adjusted for all covariates, stratified by those with and without psychiatric comorbidities, are compared in Figure 2. Many of the relationships demonstrated in Figure 1 stayed the same as stratified by treatment episodes with and without psychiatric comorbidities. For example, treatment episodes among persons who are Black/African American, as compared to treatment episodes among persons who are non-Hispanic White, had a lower odds of having a positive response to treatment, among both those with and without psychiatric comorbidities; however, the association is of higher magnitude among those without psychiatric comorbidities (No Psychiatric Comorbidities: aOR = 0.67, 95%CI: 0.63, 0.70; with Psychiatric Comorbidities: aOR = 0.80, 95%CI: 0.77, 0.84). Treatment episodes in the South had a lower odds of having a positive response to treatment among individuals with (aOR = 0.29, 95%CI: 0.28, 0.30) or without (aOR = 0.38, 95%CI: 0.36, 0.40) psychiatric comorbidities. Being treated in rehabilitation or residential settings increased the odds of having a positive response relative to being treated in an ambulatory setting among individuals without psychiatric comorbidities (aOR = 1.27, 95%CI: 1.23, 1.32) as well as those with psychiatric comorbidities (aOR = 1.24, 95%CI: 1.20, 1.28). Methamphetamine or speed as the primary stimulant of use at admission (as compared to cocaine/crack as the primary stimulant of use at admission) had a positive association with a positive treatment response among individuals without psychiatric comorbidities (aOR = 1.28, 95%CI: 1.22, 1.34), but was not statistically significant for those with psychiatric comorbidities (aOR = 0.99, 95%CI: 0.95, 1.03). Being female had no association with positive treatment response in episodes with psychiatric comorbidity (aOR = 1.02, 95%CI: 0.98, 1.05); however, among the model including individuals with psychiatric comorbidity, females had a 20% higher odds of having a positive treatment response compared to males (aOR = 1.20, 95%CI: 1.17, 1.23).
Sensitivity analysis
Results of the sensitivity analysis, which included only episodes occurring in outpatient/ambulatory treatment settings, were similar to those of the primary analysis. Of importance, the relationship between positive treatment response and age of first use was such that individuals with age of first use at 11 years or younger had a 37% higher odds of having a positive treatment response (aOR = 1.37, 95%CI: 1.21, 1.54), compared to 19% among all settings (aOR = 1.19, 95%CI: 1.09, 1.30 in all settings). Additionally, individuals with a primary stimulant of methamphetamine/speed had an increased odds of having a positive response in ambulatory settings (aOR = 1.25, 95%CI: 1.21, 1.30). Only one association changed in direction of effect; among episodes from all treatment settings, patients living in the West had a 20% lower odds of having a positive treatment response as compared to patients living in the Northeast (aOR = 0.80, 95%CI: 0.76, 0.84). However, among only ambulatory settings only, patients living in the West had a 56% higher odds (aOR = 1.56, 95%CI: 1.47, 1.65) of having a positive treatment response as compared to patients living in the Northeast. Full model results are available upon request from the corresponding author.
Results of the sensitivity analysis when excluding treatment episodes in which persons maintained no psychostimulant use throughout their treatment were similar to those of the primary analysis. Primary psychostimulant of choice at admission was the sole covariate to change direction of effect, with methamphetamine/speed, other amphetamines, and other stimulants being more likely to be associated with not achieving a positive treatment response when compared to crack/cocaine. The rates of changes in frequency of use from admission to discharge are available in Table 3. Full model results are available upon request from the corresponding author.
Distribution of change in frequency of primary stimulant use from admission to discharge.

Discussion
To the best of our knowledge, this is the first national-level study assessing predictors of positive response to treatment among treatment episodes in which the primary drug of choice was a stimulant. This study adds to the literature by assessing factors associated with a positive response among individuals with and without psychiatric comorbidities. Our findings indicate that, among the covariates examined, race/ethnicity, geographic region, treatment setting, and employment status were the strongest predictors of response to treatment. Positive responses to treatment were significantly less likely for treatment episodes among the following groups of patients: Black/African Americans, non-Hispanic individuals of other races (eg, Pacific Islanders), those who live in the South, those in detoxification settings, and unemployed persons. We also found that the association between age at first use and positive response to treatment differed for those with and without psychiatric comorbidity. Specifically, individuals who were first-time users during adolescence who had psychiatric comorbidities were less likely to have a positive response to treatment than were their counterparts with no psychiatric comorbidities.
A novel finding of this study is that Black/African American persons are less likely to have a positive response to treatment for stimulant use disorders. Related to these results reported here, another study showed non-Hispanic Black/African American persons with opioid use disorder are more likely to be criminalized for opioid use disorder, and therefore, are less likely to seek treatment. 30 In addition, Black Veterans have been found to be more likely to discontinue treatment for opioid use disorder. 31 Our findings show that the higher likelihood of a non-positive response to treatment for Black/African American persons extends beyond opioid use disorder to also include stimulant use disorders. These results are consistent with findings from previous studies investigating healthcare disparities in substance use treatment among Black/African American persons compared to non-Hispanic White persons. Specifically, Black adolescents in substance use treatment were shown to receive less specialty and informal care compared to non-Latino White adolescents. 32 Socioeconomic factors such as employment status and housing stability, insurance coverage, and federal/state healthcare policies affecting access to substance use care or mental health care were identified as significant drivers causing these disparities.33,34 Because of its positive effect on treatment completion among Black patients with opioid use disorder, short-term residential addiction treatment may also help mitigate negative responses to stimulant use disorder treatment for minorities. 35
A second novel finding from this study is we found a lower probability of positive response to treatment for persons with substance use disorders in the South, as compared to other regions of the US. The southern US has higher proportions of patients residing in rural communities, which may help explain the reduced rate of positive response to treatment—patients in rural communities have limited availability of additional behavioral health services (eg, adequate treatment of psychiatric comorbidities),36 -38 lower rates of completing treatment, 39 higher financial burden of services,40,41 and greater stigma surrounding substance use and treatment.42 -44 Stigma, in particular, may play a substantial role in the observed lower positive response to treatment in the southern US. 45 These differences could also be linked to religiosity, which is more common in the South, given a large proportion of substance use treatment in the U.S. is somewhat religious in nature and religious belief and practice may influence attitudes toward substance use and its treatment. 46
Consistent with our findings, previous studies have shown patients with concomitant substance use disorders and other psychiatric comorbidities are more resistant to treatment than are patients with either disorder alone.13,47 However, our report is among the first to show response to treatment, where the primary drug of choice is a stimulant, is mediated by psychiatric comorbidities. Co-occurring psychiatric conditions are common among adolescents with substance use disorders: previous estimates have shown over 60% of adolescents in community-based treatment programs had co-occurring psychiatric conditions. 48 This high prevalence of co-occurring psychiatric conditions and our findings that psychiatric conditions are a mediator in the relationship of positive response to treatment underscore the urgency behind the statement from the U.S. National Institute on Drug Abuse that integrated approaches are needed that accurately identify and treat each disorder.49 -51
Our findings have important implications for treatment programs and policymakers. First, treatment programs should integrate treatment of psychiatric conditions as psychiatric conditions seem to mediate the relationship between a positive response to treatment and age at first use. 13 As noted in a prior study, integrating treatment for psychiatric comorbidities in substance use treatment settings may be beneficial, particularly among those who initiate use of drugs at a young age. 52 Second, further research is needed to understand why persons of color or those seeking treatment in detoxification settings have very low probabilities of a positive response to treatment. As noted above, increasing short-term residential addiction treatment among minorities may improve rates of positive responses to treatment. 35 Lastly, treatment programs and policymakers need to increase efforts to find adequate employment for patients seeking treatment and struggling with stimulant use disorders; employment can provide social support that likely underlies the increased likelihood of a positive response to treatment among those who are employed.53 -55
Limitations
These findings should be interpreted in light of several limitations. TEDS-D treatment episodes are derived from providers who receive federal funding 56 ; therefore, caution must be used when extrapolating our findings to treatment episodes among those treated in non-federally funded programs. Relatedly, TEDS-D data do not include treatment episodes from facilities operated by federal agencies that include the Department of Defense, Department of Veterans Affairs, and the Bureau of Prisons so our findings may not be generalizable to those settings. Second, our definition of a positive response to treatment was adapted from that of Pro et al, which was used in the setting of heroin and opioid treatment and has not been validated. 24 Third, TEDS-D discharges represent treatment episodes rather than individuals; therefore, we cannot determine if a discharge occurred multiple times for the same individual. Relatedly, length of treatment was not available in the TEDS-D data; therefore, we cannot include a variable measuring length of treatment for the episodes in this study. Fourth, our outcome of positive treatment response includes reduction in use (ie, either reduction in the frequency of use or complete cessation of use) and persistent no use at both admission and discharge. As such, there could be substantial heterogeneity between these groups; however, our sensitivity analysis excluding those with no use at both admission and discharge did not reveal substantial differences in the overall findings. Fifth, we did not conduct sample size calculations for this study since we used publicly available data. Lastly, primary, secondary, and tertiary substances of misuse are those substances that led to the treatment episode, and therefore, do not necessarily represent all drugs in use at the time of admission. 57
Conclusions
It is imperative we understand factors associated with a positive response to treatment so that we can help improve outcomes for this high need population. This study showed that age at first use of a psychostimulant is strongly mediated by psychiatric comorbidity and that race/ethnicity, geographic region, treatment setting, and employment status were the strongest predictors of positive response to treatment. These results indicate that treatment programs should maximize treatment of psychiatric conditions, intensify support for persons of color and for those seeking treatment in detoxification settings, and increase efforts to find adequate employment for patients.
Footnotes
Acknowledgements
The manuscript was edited by the Science Communication Group at the University of Arkansas for Medical Sciences. We would like to thank the Science Communication Group for their assistance.
Author Contributions
Dana Abulez: Conceptualization, Data curation, Visualization, Formal analysis. Clare Brown: Conceptualization, Methodology, Writing-Review & Editing. Michael Cucciare: Writing-Review & Editing, Methodology. Corey Hayes: Supervision, Conceptualization, Resources, Project administration, Writing-Original Draft.
Funding:
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Ms. Abulez was supported by the National Institute on Drug Abuse under the Translational Training in Addiction grant [1T32 DA 022981]. Dr. Brown was supported by the National Institute on Minority Health and Health Disparities under a K01 grant [K01MD018072]. Dr. Hayes was supported by VA Health Services Research and Development under a Career Development Award-2 grant [IK2HX003358].
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
Since this study involves publicly available data, no institutional review is required.
Informed Consent/Patient Consent
Informed patient consent was not feasible or required for this study.
Trial Registration Number/Date
N/A