
Abstract
Background:
Marijuana is the most widely used illicit drug worldwide. From an occupational perspective, its use is paradoxical in that although it can be harmful to health and has criminal consequences, it can also promote well-being. This study examined predictors of well-being to determine the effects of marijuana use and its prohibition on the daily lives of Brazilian adults.
Methods:
This cross-sectional study used an anonymous online questionnaire with a final sample of 2637 respondents. Utilizing logistic regression, variables were selected pertaining to use and prohibition risks, benefits of use, and harm reduction associated with the socioeconomic characteristics of the respondents.
Results:
Using marijuana for fun was most likely among those self-identified as male, trans/non-binary people, college graduates, and those with higher incomes. Living with family members and using less frequently proved to be protective against the adverse effect of “getting high.” Indigenous peoples and youth were more likely to report trouble with the police due to marijuana use; individuals with higher education and longer use of marijuana reported more frequent use of harm reduction strategies; people who identified their color as yellow were more likely to report daily use compared to people who identified their color as white; women and people with higher income were less likely to report daily use.
Conclusions:
Social class, race, gender, and generation were predictors of well-being associated with marijuana use and its prohibition, indicating an interaction between different dimensions involving the use of illicit substances. Identifying the effects of the use and prohibition of marijuana in promoting well-being, from the conception of drug use as a non-sanctioned occupation, can broaden the understanding of this complex human phenomenon, with health and criminal repercussions, subsidizing the development of approaches more equitable and adequate into occupational therapy to reduce personal and social harm.
Introduction
Cannabis sativa is a complex plant with multiple human uses, many of which were reported over 10 000 years ago by Indigenous, Indian, and Chinese peoples for spiritual, therapeutic, and everyday purposes. 1 Its medical properties were first recorded in the 18th century,1,2 and its therapeutic uses remain widely recognized, especially in the East. Since its inclusion as a concern of public order, expressed at the II International Opium Conference in Geneva by a representative, 2 Brazilian public policy proposals have been dominated by the negative effects of its use. These effects were later consolidated globally with its inclusion on the list of dangerous substances in the 1961 report of the Single Convention on Narcotic Drugs. 3
Concurrently, since the mid-1960s, advances and scientific findings have intensified debates on the use of the cannabis plant, especially after the isolation of its main active ingredients 4 and the identification of the endocannabinoid system 5 which has promoted the human dimension of solutions to their potential as health issues. These findings have highlighted the plant’s potential for promoting well-being with studies examining the effects of anxiolytic, antipsychotic, anti-inflammatory, and antiepileptic action on cognitive deficits as well as sleep, eating, and mood disorders. 6 Moreover, there are potential benefits in psychiatry, 7 in the control of nausea and vomiting induced by chemotherapy, 8 in the treatment of epilepsy,9,10 multiple sclerosis,11,12 Alzheimer’s,13,14 chronic pain, 15 among other neurological disorders. 16 Additionally, studies have reported its potential to reduce aggressiveness and hyperactivity, and aid in the treatment of seizures. With increasing reports of positive effects on well-being, prohibitionist and punitive models that guide current drug policies in the field of public safety are being questioned as they do not reduce the supply and demand for drugs, 7 limit access to health care due to the stigma associated with drug users, 17 or greatly impact the prison system, 18 and have an inequitable impact on specific population groups, such as migrants, blacks, women and the poor. 19
The illicit status of cannabis has been reviewed globally, demystifying the prohibitionist pillars that culminate in the incarceration and mortality of those involved in the so-called War on Drugs, 20 with disproportional impacts on some specific ethnic groups.21-24 This contradiction has become more evident due to changes in the legislation of some countries and the growth of scientific evidence, prompting the United Nations (UN) Commission on Narcotics Drug 25 to recommend reclassifying marijuana to remove it from the 1961 list of the most dangerous drugs. The non-medical use of marijuana has also been legalized in Uruguay, Canada, the Netherlands, some jurisdictions in the United States, and Mexico the debate on its legalization is well underway. Since 1830, when many elements of African culture were criminalized with strong racist and eugenicist biases, Brazil was one of the first nations to prohibit marijuana use.20,26,27 Despite efforts to legalize its medical use 28 and increasing movements of patients and their families to ensure its medical use, 29 the plant remains illegal in Brazil.
The III National Survey on Drug Use 30 carried out in large Brazilian cities, estimates the number of Brazilians, between the ages of 12 and 65 years, who use marijuana, hashish, or skank, to be more than 2 million, characterizing it as the most used illicit substance in the national territory. Additionally, 2.4% of respondents reported use in the 30 days prior to the survey. Recently, a Brazilian cross-sectional study of a non-probabilistic sample 31 involving more than 7400 adults (6620 recreational cannabis users and 785 non-users) assessed their quality of life, subjective well-being, anxiety, and depression with standardized scales using an online survey about cannabis and other substance use. The highest scores for quality of life were observed among habitual cannabis users, followed by occasional users, whereas both non-users and dysfunctional users presented less favorable scores. Subjective measures of well-being were higher among habitual and occasional users than non-users, whereas dysfunctional users were most adversely affected. Poor quality of life, depression, and anxiety were more prevalent among dysfunctional cannabis users, but non-users reported more depression or anxiety symptoms and a lower quality of life than occasional and habitual users. 31 The researchers highlighted that samples dominantly comprising most habitual cannabis users from the general population are rarely represented in surveys outside the clinical or medical context.
Well-being, occupational therapy, and drug use: Background
In 1946, the World Health Organization (WHO) defined health as a state of complete physical, mental, and social well-being, and not merely the absence of disease or infirmity. This definition recognized the concept of well-being as a key component of health of the individual in a comprehensive and holistic manner, influenced not only by individual characteristics but also by the social conditions in which people find themselves and the environment in which they reside. These determinants interact dynamically and may threaten or protect an individual’s mental health state. 32
Well-being is an important pillar of the Democratic State, which, according to the Brazilian Federal Constitution, “aimed at ensuring the exercise of social and individual rights, freedom, security, well-being, development, equality, and justice as supreme values of a fraternal, pluralistic, and unprejudiced society, founded on social and committed harmony, in the domestic and international order, with the peaceful settlement of disputes.” 33 Since the origins of occupational therapy, the concept of well-being has been present, whether as an objective of professional practice, through participation in significant occupations and meaningful activities that aim to restore or promote healthy conditions (occupational well-being), or as a state that can be determined by occupations.34,35 Occupational therapy is a client-centered health profession focused on promoting health and well-being through occupation, as shown in almost all definitions of the profession worldwide. 36 The term “occupation” not only refers to work but also to all activities that individuals wish to do, have to do, and are expected to do, including self-care, productivity, and leisure. 37 Law et al 38 reviewed research on the association between occupation, health, and well-being and concluded that occupation substantially affects human health and well-being. According to the World Federation of Occupational Therapists 36 “occupational therapists can use a community-centered approach to intervene and facilitate initiatives that promote community health, well-being, participation, and inclusion.” We recognize the inseparability of well-being and the guarantee of access to education, health, work, income, housing, and justice, among other elements of daily life that have a decisive impact on life satisfaction. 39
The dominant discourse in occupational therapy and occupational science literature on the relationship between occupation and health and well-being is positive.40-43 To Stewart et al,
44
“the discussion of the relationship between occupation and health and well-being as positive is so commonly found within the occupational therapy and occupational science literature that it could be considered as an a priori assumption.”
Conversely, discussions on the potential negative health or well-being implications of occupational engagement remain vague and limited. These authors proposed that occupations should be conceptualized as neutral, and that the health-promoting and illness-producing aspects are dependent on the physical, cultural, social, historical, and political contexts in which an individual engages in an occupation and the meaning that individual assigns to that occupation. Kiepek et al 43 identified occupations as discursively “positive” and focused on how the relationship between occupational engagement and improved health and well-being can result in the implicit exclusion of activities considered “negative,” “unhealthy,” or “deviant,” with the potential to stigmatize and marginalize individuals or groups. “This has effectively silenced a significant realm of human experience, namely, occupations that are considered within dominant worldviews and societal groups to be unhealthy, illegal, and/or deviant.” 45 Some authors have argued that drug use46-50 or addiction46,51,52 is an occupation. Looking critically at the realm of healthcare, drug use and drug abuse have been deemed undesirable behaviors by society, 46 and typically labeled as problematic. 49 Thus, they are almost always viewed as an object of intervention and remediation in occupational therapy, with healthcare professionals eager to help clients abandon it. 46
According to Kiepek and Magalhães, 51 activities classified as addictions and impulse-control disorders meet the criteria of occupation given that they give meaning to life, are significant determinants of health, well-being, and justice, organize behavior, develop and change over a lifetime, shape and are shaped by environments, and possess therapeutic potential. Stewart and Fischer 47 acknowledged the complexity of occupation and the possibility of engaging in a profession that can affect the lives and well-being of individuals both positively and negatively through occupations, such as drug use. However, they believe that addiction is not an occupation in and of itself, but rather describes the nature of a person’s involvement in an occupation. The focus of the occupational therapist would then shift from addiction to the client’s health and well-being, as well as the occupations they perform. To Chang, 46 people’s needs and wants frequently determine their choice of daily occupations. Thus, even for individuals with drug addiction, time spent in occupations that support the need to acquire drugs can create a role, a sense of identity, and organize their lives, allowing them to connect with, adapt to, and feel in control of their surroundings.
In the occupational science field, studies have pointed out that viewing drug use as distinct from substance abuse, problematic use, dependence, or addiction, focusing on occupation can (a) stimulate new ways of understanding substance use and its relationship with the quality of life and meaningful experiences 50 ; (b) facilitate a better understanding of how people employ alternatives to achieve desired occupational outcomes 49 ; and (c) help identify factors that encourage and constrain use, expanding approaches to addressing substance use that go beyond the individual to social and institutional contexts. 48 Attention to non-sanctioned occupations may be vital to diversify perspectives on occupation, emphasizing a critical reflection on underlying disciplinary assumptions, decrees of social power and values, and moral viewpoints that inform the production of knowledge in science. This attention can help to diversify the understanding of the occupation itself to challenge dualisms, given the politically constructed nature of all occupations. 45 In Brazil, from the critical occupational therapy perspective, cotidiano 53 is a Portuguese word that means what is common to everyday life, banal, which has been adopted as a concept that can be translated as a resource used to understand the different ways of thinking, acting, and feeling of individuals and groups, analyzing living, social, ethnic, sociocultural, economic, and generational conditions. It also becomes an intervention tool centered on the needs of individuals, groups, and collectives, seeking to promote greater participation and autonomy, expressing the construction and transformation of concrete reality, encompassing adversities, decision making, and forging ways of being, living, and acting. 53
This study aimed to identify (a) the effects of marijuana use and its prohibition on the daily lives of adults in Brazil, recognizing different types, justifications, and motivations for use, and (b) to examine the predictors of well-being for the characteristics of marijuana users.
Methods
Study design, sample, and ethics
In this exploratory cross-sectional study, an anonymous online questionnaire was used on a non-probabilistic sample. The analytical sample comprised 2637 respondents. The socioeconomic characteristics of the respondents were used to select variables pertaining to the risks of use and prohibition, the benefits of use, and harm reduction. An analysis of logistic regression was performed. The Federal University of São Paulo Ethics Committee approved the study after ensuring all ethical procedures were followed.
Procedures
Tool construction and validation
In collaboration with 12 specialists, including researchers in the fields of drugs and occupational therapy as well as representatives of organized social movements, an online and anonymous questionnaire was developed for data collection. This technique is used to establish consensus when no unanimity of opinion exists on a given topic or innovative topics, being used in health research, for clinical decisions, and to support decisions in the daily practices of health services. 45 Based on the expertise of the panel, it was possible to qualify the instrument before its wide availability, also supporting the management of biases.
The expert panel was comprised of all who were invited and was recorded through the Google Meet platform. The consensus meeting was conducted by the primary researcher together with the assistant researcher, a scientific initiation student, an occupational therapist in the role of observer and annotator, and a researcher in the field. Panel experts were presented with the study’s objectives and general design, as well as an outline of the survey form that had been prepared in advance and was open for consideration by each expert.
The experts’ contributions were fundamental to the construction of the questionnaire, which was divided into the following sections: (a) characterization of respondents, which asked questions on socioeconomic, demographic, and cultural information; (b) information on the use of marijuana, which contained aspects related to use and frequency, motivations for use, and associated use with other substances; (c) access to marijuana, which reported on the mechanisms of how the substance is obtained, the origin, and which health problems are intended for this use; and (d) the repercussions of marijuana use in daily life, addressing how prohibitionism affects the daily lives of users and identifying the individual and collective consequences of this use.
Sample size
Considering that the marijuana user population can be criminalized in Brazil, insufficient information exists from which to draw an accurate sample. However, despite acknowledging the limits and restrictions on generalizability, probabilistic analyses were performed with the aim of seeking possible predictors of marijuana use to promote well-being for the characteristics of marijuana users. For the sample calculation, the variable marijuana use to promote well-being was used, with an expected prevalence of 32.9% in the target population. This prevalence was based on a characterization of participants in an online harm reduction course carried out by the Study, Research and Extension Group: DiV3rso of the Federal University of São Paulo, Campus Baixada Santista. In this course, 47.4% of participants were marijuana users, and 32.9% used it for the purpose of promoting well-being. Considering a confidence level of 95%, a sampling error of 2%, and that there were approximately 2 million individuals who regularly use marijuana in Brazil, when a population survey was carried out, in 2017 21 the estimated sample size should be 2121 respondents.
Recruitment, data collection, and respondents
The link to the survey form was widely disseminated on social media networks, including groups on WhatsApp, university student groups on Facebook, groups for the legalization of marijuana, and Instagram stories. In addition, researchers and partner organizations were provided with the survey link and asked to disseminate it broadly, ensuring a good reach. The survey form was made available for 1 month, which was enough time to reach the minimum sample calculation. A total of 2777 responses were obtained.
The respondents resided in Brazil, and were 18 years or older, used marijuana—whether for their well-being or medical/clinical indication—and voluntarily participated in the study. There were no exclusion criteria. Two respondents who did not meet the inclusion criteria were excluded because they did not use marijuana.
Data analysis
Viewing marijuana use for well-being as a complex and significant occupation, in interaction with the set of forces present in various daily lives, we chose 6 response variables: (a) 2 variables about the effects of use; (b) 2 variables about what we consider the effects of prohibition; and (c) 2 variables about harm reduction. In addition to the effects of use, 2 additional variables were added: (a) “feeling high and not being able to comply with your tasks” (response: yes or no) as an adverse effect, 54 to recognize possible occupational performance impacts of cannabis use; and (b) “having fun” (response: yes or no) to indicate a positive effect. These variables are viewed as important dimensions of well-being, and relevant to the goals of occupational therapy, whose significance and experience are always in relation to the forces of power and social hierarchy. The variables “problems with the police” (response: yes or no) and “dangerous and illegal method of obtaining it” I (response: yes or no) were selected as the effects of prohibition, and addressed some of the problems that the international process of cannabis regulation is trying to resolve.18,19,55
To address harm reduction strategies, we selected the variables “use at strategic times for better results” (response: yes or no) and “daily” (response: yes or no), with the former indicating a lower-risk marijuana use and the latter a higher-risk use. 47 The independent variables considered for the associations were sociodemographic characteristics, such as color, II age group, gender, schooling, region of residence, income, religion, who they live with, frequency of use, and age at first use.
For the statistical analysis, the categorical variables were described by their absolute and relative frequencies. To study these associations, univariate logistic regression models were first performed, and then multivariate logistic regression models were fitted. Variables without statistical significance were excluded, one by one, until the final model included only statistically significant variables. The significance level considered in the entire analysis was 5%. The R Core Team 56 software was used. For the purposes of the subsequent statistical analyses, individuals were excluded if they did not respond to one or more questions (including the sociodemographic characteristics) and or stated that they did not use marijuana (n = 2), leaving 2637 individuals. The qualitative variables were summarized as absolute and relative frequencies in the descriptive analysis.
Results
The respondents’ sociodemographic characteristics indicate that most respondents were white, were currently between 18 and 29 years, had completed or partially completed higher education and graduate studies, had no religious affiliation, had an income between 1 and 5 minimum wages (between US$203 and US$1018.99 per month), and lived with family members. Most respondents had used marijuana for 1 to more than 20 years, regularly and daily, and started using marijuana at approximately 16 to 20 years of age (Table 1).
General characterization of the sample.

Despite the small number of self-declared Indigenous peoples among the respondents, we believe it is important to maintain a separate category for them in this work, as such information was not included in the previous study on marijuana use for recreational purposes in Brazil. We emphasize that the small sample size had no impact on the estimates of the effects of the logistic regression models used in the data analysis.
Almost 20% of respondents named their use as casual; that is, they use it only when the substance is available in the environment where it is; 70.75% claimed their use as intentional, where they searched for and obtained it for their use, and 45.16% claimed their use as therapeutic. Some respondents chose more than 1 category. Therapeutic use was justified either through personal recognition of the benefits, reports of benefits by friends, or referrals from medical and non-medical professionals. More than 93% of the respondents said that they smoked marijuana, 26% ingested it, and 21% vaped it.
Of all the respondents in the present study, 7% reported that their use of marijuana was medically prescribed, with more than 76% using it by personal decision or from personal experience. Twenty-seven percent of users indicated that they used marijuana to reduce the consumption of alcohol or other licit substances, 21.20% to reduce the use of psychotropic drugs, and 5% to reduce the use of other illicit substances. Regarding other reasons for use, almost 50% reported using it to stimulate creativity, more than 52% to manage stress, 55.6% to sleep better, 63.3% to promote well-being, 66.8% to have fun, and over 83% to relax. Regarding health problems, the respondents reported using marijuana to alleviate anxiety (45.92%), insomnia (30%), depression (27.27%), menstrual cramps (15.51%), headaches (15%), chronic pain (11.34%), attention-deficit hyperactivity disorder (8.49%), chemical dependency (3%), and muscle spasms (2.43%).
Effects of use
In the multivariable logistic regression model, users aged 18 to 29 years and 30 to 45 years had higher odds of using marijuana for recreational purposes than those over 60 years (OR = 9.08; 95%CI [5.47; 15.10, P < .001] and OR = 2.52; 95%CI [1.60; 3.95, P < .001], respectively; Table 2). Male gender users and users who identify with other genders (transgender; non-binary) had higher odds of using for recreational purposes compared to feminine gender, OR = 1.50 (95%CI [1.21; 1.85, P < .001]) and OR = 2.31 (95%CI [1.10; 5.49], P = .038). For users with a postgraduate degree, there was a greater chance of using it for recreational purposes than for users who did not study or only attended elementary school (OR = 3.06, 95%CI [1.16; 7.74], P = .020). Users who follow any religion or have no religious affiliation are less likely to use marijuana for recreational purposes than atheist/agnostic users. In relation to income, the higher the income range of users, the greater the chance of using it for recreational purposes compared to users who earn less than 1 minimum wage (less than US$203 per month). Finally, users who had used marijuana for a longer period were more likely to use it for fun than those who had used it for less than a year.
Univariate and multivariate logistic regression for the association between the characteristics of marijuana users and use for fun (n = 2637).
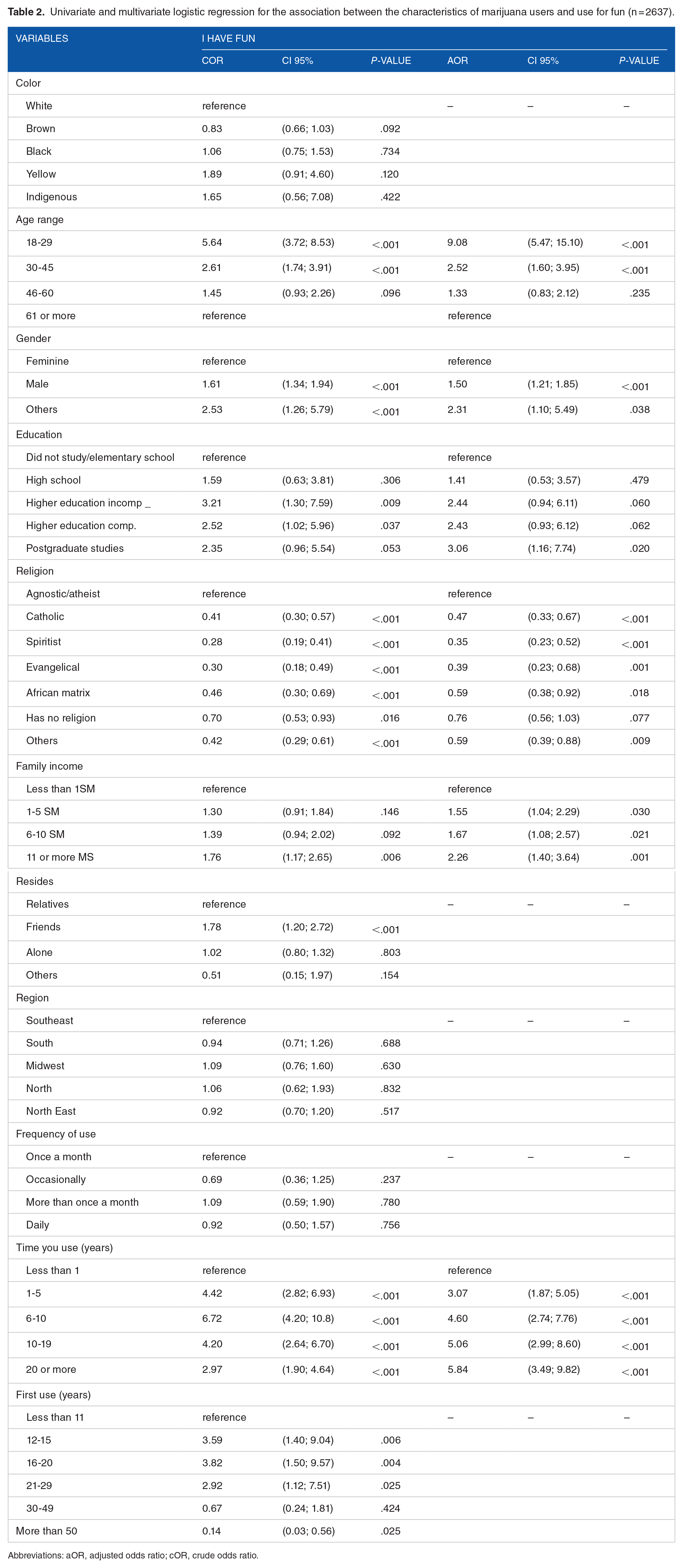
Abbreviations: aOR, adjusted odds ratio; cOR, crude odds ratio.
In the multivariable logistic regression model (Table 3), users who self-identified as brown or black were less likely to use marijuana and feel “high” to the point of not being able to perform their tasks compared to white people (OR = 0.77; 95%CI [0.63; 0.95, P = .014]; OR = 0.59 (95%CI [0.43, 0.80, P = .001]). Regarding age group, users aged 18 to 29 and 30 to 45 years old have higher odds of using marijuana and feeling “high,” unable to perform their tasks compared to people aged 61 and over (OR = 8.09; 95% CI [4.7;17.46, P < .001] and OR = 3, 28; CI 95% [1.98;5.67, P < 0.001], respectively. Regarding education, individuals with incomplete, complete and postgraduate higher education have higher odds of using marijuana and feeling “high” compared to individuals who did not study or attended until high school. Regarding religion, Catholics and Evangelicals were less likely than atheists and agnostics to fail at their jobs due to substance abuse.
Univariate and multivariate logistic regression for association between characteristics of marijuana users and feeling stoned (n = 2637).

Abbreviations: aOR, adjusted odds ratio; cOR, crude odds ratio.
People who live with friends or alone were more likely to experience feeling stoned than those who lived with family members. Residents of the south and northeast regions had lower odds of feeling “high” and unable to perform their tasks than those of the Southeast (OR = 0.76 (95%CI [0.59; 0.98, P = .038]; OR = 0.71 [0.55; 0.91, P = .007]). People who use it more than once a month and for more than a year were more likely to feel stoned and unable to fulfill their tasks than those who used it for less than a year, once a month, or occasionally.
Effects of the prohibition
The factors associated with the response variable “problems with the police” referred to color, age group, gender, region, frequency, and time of use, as shown in Table 4.
Univariate and multivariate logistic regression for association between characteristics of marijuana users and problems with the police (n = 2637).

Abbreviations: aOR, adjusted odds ratio; cOR: crude odds ratio.
In terms of color, Indigenous peoples were 3 times more likely to have problems with the police than white people (OR = 3.03; 95% CI [1.16; 8.37], P = .026). The younger they were, the higher the odds for problems with the police, with the emphasis on the range between 18 and 29 years (OR = 10.32; 95% CI [5.89; 18.64, P < .001]). The findings indicate an increase of approximately 10 times compared to the age group of 61 years and older of having problems with the police. Regarding gender, compared to the feminine, users who self-identified their gender as masculine have higher odds. Residents in the northeast region (OR = 0.73; 95% CI [0.56; 0.95], P = .021) were less likely to have problems with the police than those in the southeast region of the country. As for the time of use, the more time spent using marijuana, the greater the chance of having problems with the police than for users with less than a year of use. Likewise, individuals who used marijuana more than once a month or daily had higher odds than users who used it less than once a month.
The factors associated with the response variable “dangerous way of obtaining” were color, age group, gender, religion, frequency, time, and age of first use, as shown in Table 5. For the response variable “dangerous way of obtaining” when we analyzed data referring to color, there was a lower chance of dangerous acquisition among brown people than white people (OR = 0.62; 95% CI [0.47, 0.81], P = .001). Regarding age groups, the associations were inversely proportional; the greater the age range, the lower the chance of acquiring marijuana dangerously, compared to people over 61 years old, reaching 6 times greater among people aged 18 to 29 years (OR = 6.74; 95% CI [3.73; 12.16], P < 0.001). Male sex had higher odds than female sex (OR = 1.79; 95% CI [1.41, 2.29], P < 0.001). Religion was also associated with dangerous ways of obtaining, appearing as protective factors for those with Catholic, Spiritist, and Evangelical religious affiliation, compared with agnostics/atheists. Belonging to the northeast region was a protective factor for the dangerous and illegal way of obtaining marijuana in relation to the southeast region (OR = 0.67; 95% CI [0.49; 0.94], P = .017). An association was also observed in relation to time of use, such that the longer the use, the greater the odds of dangerous acquisition compared to those who use it for less than 1 year. The age of first use was associated in all age ranges, decreasing, with the mode of obtaining marijuana in a dangerous way, compared with those who used it for the first time under the age of 11, meaning the higher the age of first use, the less dangerous the way used to obtain it.
Univariate and multivariate logistic regression for association between the characteristics of marijuana users and dangerous way of obtaining (n = 2637).
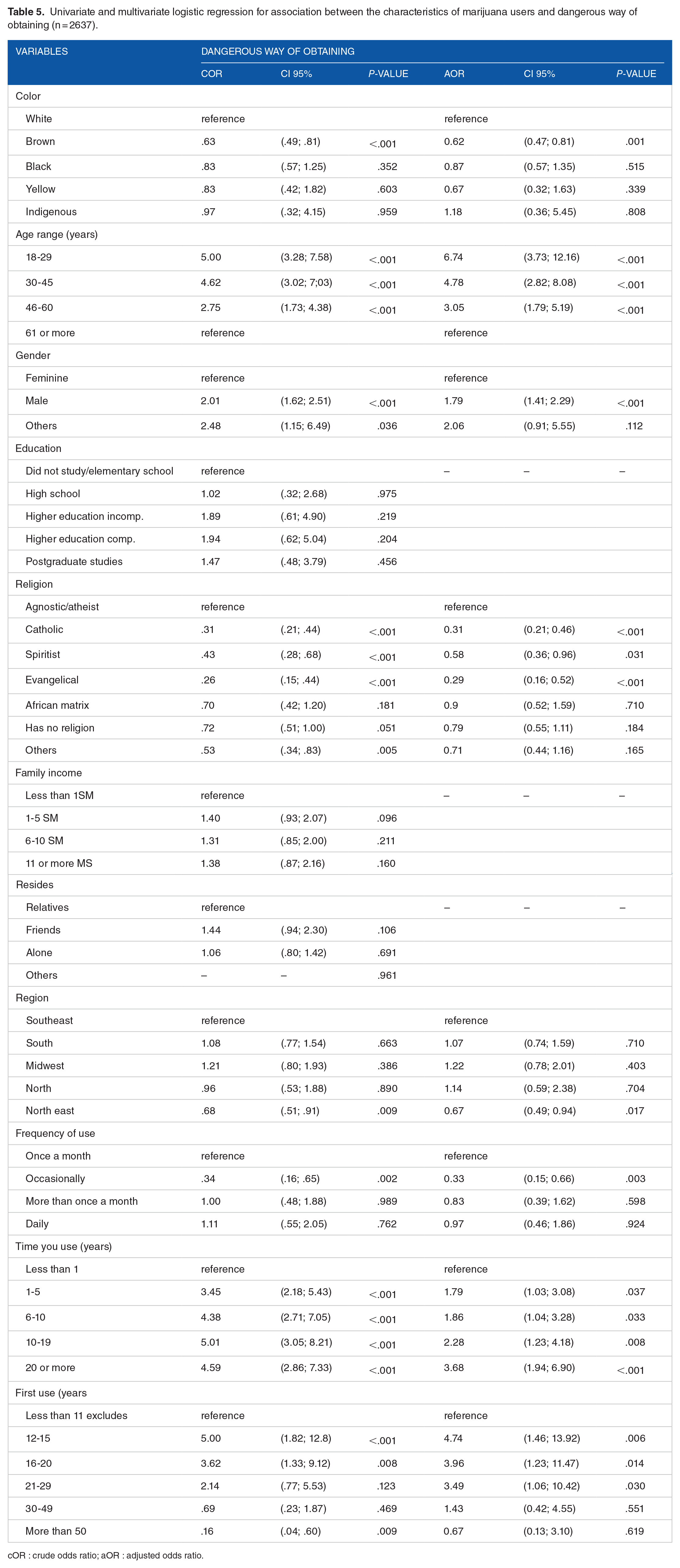
cOR : crude odds ratio; aOR : adjusted odds ratio.
Harm reduction
The choice of the response variable “use at strategic times” starts from the recognition of the potential of harm reduction strategies that can guide health education actions related to the knowledge arising from the experience of drug use. The factors associated with this variable were age, education, frequency, and duration of use, as shown in Table 6.
Univariate and multivariate logistic regression for association between characteristics of marijuana users and use at strategic times (n = 2637).

Abbreviations: aOR, adjusted odds ratio; cOR, crude odds ratio.
Level of education was shown to be positively associated with use at strategic times, with those who had completed high school more likely to use at strategic times than users who did not study or who only completed elementary school. For frequency of use, users with more intense use (using it more than once a month or daily) were more likely to use marijuana at strategic times compared to those who used it only once per month. Regarding lifetime use, users who used marijuana for 1 to 5 years and 6 to 10 years are more likely to use this harm reduction strategy than those who have used marijuana for less than 1 year.
The characteristics associated with the response variable “daily use” were color range, gender, income, time of use, and age at first use, as shown in Table 7. For the response variable “daily use,” those who self-declared yellow race had higher odds of using daily than white people (OR = 1.91; 95% CI [1.06; 3.65]; P = .039). Those users who self-identified their gender as feminine had lower odds of daily use compared to who self-identified as masculine. Regarding family income, people who earned 11 or more minimum wages (more than US$2298.34 for month) were less likely to use it daily compared to those who earned less than 1 minimum wage (less than US$203 per month; OR = 0.52; 95% CI [0.35; 0.76]; P = .001).
Univariate and multivariate logistic regression for association between characteristics of marijuana users and daily use (n = 2637).

Abbreviations: aOR, adjusted odds ratio; cOR: crude odds ratio.
Regarding the length of time using marijuana, all those who used it for more than 1 year had greater odds of using it daily compared to those who used it for less than 1 year, and those who used it for more than 20 years had 3 times more chance of daily use (OR = 3.14; 95% CI [1.94, 5.14], P < .001). As for the age at first use, people who started using marijuana between the ages of 16 and 29 were less likely to use it daily.
Discussion
The majority of respondents were white between the ages of 18 to 29 years with higher education and graduate studies, no religious affiliation, incomes between US$203 and US$1018.99 per month, living with family, and using marijuana on a regular and daily basis. Using marijuana for fun was most likely among those self-identified as male, trans/non-binary people, college graduates, and those with higher incomes. Living with family members and using less frequently proved to be protective against the adverse effect of “getting high.” Indigenous peoples and youth were more likely to report trouble with the police due to marijuana use; individuals with higher education and longer use of marijuana reported more frequent use of harm reduction strategies; people who identified their race as yellow were more likely to report daily use compared to people who identified their race as white; women and people with higher income were less likely to report daily use.
Epidemiological data from the Third National Survey on Drug Use in Brazil 30 revealed that the highest prevalence of regular marijuana use was among 18- to 24-year-olds with a postgraduate degree or higher residing in the capitals of the southeast region. Similarly, in the first Brazilian study on the recreational use of marijuana, 31 regular users, those with religious affiliation, those with a higher level of education, those residing in the south, southeast, and midwest, and those with a monthly household income between US$515 and US$2560.00 had a greater presence.
Although the level of education of the respondents is comparable to that of other studies, none of the cited studies disaggregates the data by race/color, which has been considered essential to identify and face the inequalities.23,24,57,58 Therefore, we question whether the preponderance of white people indicates that the disproportionate criminalization of racialized populations for drug use can influence the greater difficulty in participating in research identifying themselves as drug users, or whether marijuana is used by black people for other motivations.
A study on cannabis use frequency and use-related impairment among African American and white users supports that although participants did not differ in their cannabis use frequency or cannabis-related impairment, they appeared to use cannabis for different reasons. More specifically, social motives were differentially associated with cannabis-related impairment as a function of race. 59 The results from the 2018 National Survey on Drug Use and Health demonstrated that the lifetime prevalence of cannabis use was lower in black (45.3%) than in white (53.6%) adults aged 18 years or older. 60
According to Kiepek and Beagan, 48 Kiepek et al,49,50 and Kiepek and Magalhães, 51 drug use can be labeled as an addiction or impulse control disorder, typically portrayed as problematic, but is related in complex ways to health, well-being, and social justice.45,49,50 In the process of decriminalizing or legalizing marijuana, researchers and social movements have pointed out the disproportionate impact of the drug war on blacks and other minorities, including prisons, reduced access to therapeutic use, lower participation in legal retail, and abuse in police approaches.22,24,58,61,62
Although almost half of the respondents claimed their marijuana use was therapeutic, only a few had a medical prescription, even if the marijuana use was being reported to alleviate health problems like anxiety, insomnia, depression, chronic pain, and addiction. In another survey of marijuana associations, specifically focused on medical use, 29 the main reported treatment for similar problems added Alzheimer’s, Parkinson’s different types of cancer, and multiple sclerosis. In the current study, we identified a therapeutic use of marijuana that went beyond the medical indications for marijuana use, including menstrual cramps, headaches, ADHD, and muscle spasms. Reducing the consumption of alcohol, other licit substances, and psychotropic drugs are among the motivations for use.
Harwick et al 63 argue that the binary distinction of substances by medical/non-medical use served as a conceptual basis that directed public policy regulation on the use of marijuana without critiquing its consequences. The authors maintain that such separation has created a division that does not correspond to the experience, meaning, and function of drug use by the different people living in diverse contexts and cultures.
Morais et al 31 had purposed that “a non-stigmatizing approach to the use of cannabis, as well as the possibility of understanding the use of cannabis as an alternative strategy of self-care,” may help us optimize treatment for those who might be using cannabis as a self-medication tool. We agree with Kiepek and Magalhães 51 who defined occupation with therapeutic potential as “engaging in an activity that has the potential to improve health and well-being, outside the guidance of a health professional.” This definition helps us understand the changes and overlaps that marijuana use can have in a care relationship with health professionals over the course of a person’s lifetime.
Having fun
The concept of occupation must expand to include complexities experienced in daily life, such as engaging in the activities with which people occupy themselves as well as those they are prevented from doing. It must also include an understanding of the social places people occupy or are prevented from occupying. 64 In this way, drug use can illuminate aspects of experience, existence, resistance, practices, and scenarios, as well as potential obstacles.
Considering marijuana as an occupation, we recognize its potential for multiple meanings that are socially constructed and influenced by individual processes. We emphasize the importance of the generational factor, which indicates those over the age of 30 are nine times more likely to use recreational marijuana than those over the age of 60. Although epidemiologically, marijuana use is more related to young people, some reported experiences seem to indicate that low-income young people may not have access to other recreational activities that do not involve drug use. 65
An analysis of the scientific literature on the use of psychoactive substances among older adults revealed that alcohol is the most commonly used psychoactive substance in this age group, followed by drug use and a gradual increase in the use of illicit substances. In this study, older adult users of psychoactive substances were predominantly male, had low levels of education and income, were unemployed, unmarried, lived alone, and had organic and psychological comorbidities. 66 In 1 study, 67 older adults who used drugs were categorized as “survivors,” referring to those who began using drugs in their youth and have a long history of consumption, or “reactive,” referring to those who began using drugs later in life and whose use is related to lifelong problems. Another study that sought to comprehend the significance that older adults ascribe to drug use and was limited to older adults being monitored by health services for people with drug problems identified the need to form relationships or occupy space as a motivation for drug use, such as voids resulting from effectual losses. 68
Longer duration of marijuana use was significantly associated with recreational use compared to participants with less than 1 year of marijuana use, likely corroborating the findings of Harwick et al 63 and Kiepek et al 50 that the types of drug use changed over the course of a lifetime. Respondents reported using marijuana to stimulate creativity, manage stress, sleep better, promote well-being, and relax, among other reasons identified as positive effects by the researchers. Kiepek and Beagan 48 investigated the motivations for substance use among professionals and students in professional programs in Canada who used 1 or more non-prescription psychoactive substances and discovered that substance use was advantageous for relieving pain, enhancing sleep, supplying energy, and engaging in daily activities. Some individuals discovered that substance use reduced anxiety, allowing them to better manage occupational demands, enhance performance, or served as a reward for completing tasks. Kiepek et al 49 identified that psychoactive substance use, even those framed as unhealthy, illegal, and deviant, may be used to enhance mood, cognition, occupational performance, and/or experience. Sometimes, substance use is an occupation in and of itself, such as drinking alcohol or going out for coffee. Occasionally, a substance is used to enhance the performance of another occupation, such as taking erectile dysfunction medication to enhance sexual performance or amphetamines to enhance academic performance. 49 According to Chang, 46 drug users may find a sense of control, temporary relief from emotional and physical pain, acceptance, peer interaction, a role, and a sense of identity through their occupation of “drug use.” They can do so on purpose. The author argued that even for people with drug addiction, the activities associated with use can “sustain them, organize their lives, and enable them to connect with, adapt to, and have a sense of control in their environment,” as with other occupations, allowing them to express themselves and provide a sense of who they are, regardless of whether it is deemed good or bad, or socially acceptable.
Getting high
The variable “getting high and not being able to fulfill your tasks” was chosen as an adverse effect, recognizing the possible impacts of marijuana use on occupational performance17,69 although other findings have reported marijuana use as a strategy to attenuate impairments in performance.46,48,50,70 When examining education and noting that university enrolment increased the likelihood of these experiences, is it possible to link them to academic activities that generate greater cognitive demand? Furthermore, the adverse effects of marijuana use are poor educational outcomes and cognitive impairment.17,69 Living with family members and using them less frequently appeared to be protective factors against feelings of being high and inability to complete tasks.
Observing that white people were more likely than black and brown people to experience of the “getting high and not being able to fulfill your tasks” in their daily lives, we can formulate some hypotheses. Considering the racist social context of Brazil and that vulnerable populations, such as those with lower socioeconomic status, mental health problems, and minority populations, are more likely to experience the severe negative consequences of substance use, could whites face less stigma or repercussions if they are permitted to withdraw from their duties when they are ill? Other analyses that verify job placement, income, and other potential protective factors can help to expand this discussion.
Effects of the prohibition
The factors associated with the response variable “problems with the police” were color, age group, gender, region, frequency, and time of use. Indigenous peoples were 3 times more likely to have problems with police than white people; those aged 18 to 29 had approximately 10 times the likelihood of those aged 61 and older; and men were more likely to have problems with police than women. Similarly, users who used it more than once a month or daily were more likely to encounter the police than those who used it less frequently.
Color, age group, sex, religion, frequency, time, and age of first use were the factors associated with the response variable “dangerous way to obtain.” The likelihood of dangerous acquisition was lower among black people compared to whites; 6 times greater among those aged 18 to 29 compared to those aged 30 and older; the longer the duration of use, the greater the likelihood of dangerous acquisition; and males were more likely than females. Catholic, Spiritist, and Evangelical religious affiliations, living in the northeast, and older age at first use were identified as protective factors.
In Brazil, marijuana became prohibited in the colonial period and was directly related to the enslaved black population. Pointing to the racist heritage that the country carries, marijuana descends from black culture, which led to the stigmatization that black people who used the weed were lazy, rowdy, and savage. Thus, a eugenics hygiene process prohibited marijuana from being circulated and preached as a degenerative element to health. 11 Currently, in Brazil, marijuana continues to be obtained through illegal means, fueling trafficking and leading to the third largest prison population in the world, 32.6% of which are linked to the crime of drug trafficking. 62 Problems with the police are some of the risks of prohibition that, in our country, have resulted in state violence that has mainly killed and imprisoned the most oppressed sections of the population, with a strong racial marker.71,72
As the findings on the indigenous population demonstrate, we refer to the work of Barreto, 65 who focused on the sociocultural issues associated with the use of coca leaves in the Andes and Amazon regions and historically reconstructed a tendency to indiscriminately link coca to cocaine and, consequently, to drug trafficking, demonstrating a bias of denial of the historical and cultural roots of the age-old use of this plant by traditional communities. According to this author, efforts to break the silence surrounding indigenous issues are due to science. We emphasize that the inclusion of Tupi Guarani indigenous people in our research group III seems to have favored access to information about this population to think about care policies.
According to Carneiro 20 the youth are punished the most for their everyday recreational activities, making police violence more devastating for these age groups. The results indicate that users with longer use histories are more likely to be associated with this adverse effect, possibly indicating how the War on Drugs is perpetuated on a daily basis and predicting that at some point in their lives, they will encounter issues with the police.
We are aware that the illegality of marijuana does not prevent its use, but rather exposes its consumers to danger on a daily basis, such as by requiring them to engage in risky behavior to obtain the drug. Thus, we question what it means for self-identifying as white to be more associated with exposure to risky means of obtaining while being less associated with issues with the police. Especially vulnerable populations, such as poor young people, blacks, and residents of the periphery, are more susceptible to incarceration as a result of prohibitionist policies,73,74 it appears that for whites, exposure to dangerous modes of shopping does not necessarily correlate with problems with the police, an institution that has historically operated on the basis of racial bias and for which the importance of anti-racist educational processes has been indicated. 62 Problems with the police can impact people’s civil rights, such as parental rights, immigration status, education, social security benefits, and prevention of access to public housing programs. Respondents living in the northeast were less likely to have problems with the police, which may be a result of the high concentration of cannabis associations in the region, which accounted for 23% of all cannabis associations in the United States in 2020. In the process of regulating marijuana use, the prior distension of police forces in the face of ongoing decriminalization 62 has been highlighted.
Harm reduction strategies
The “use at strategic moments” variable is interpreted here as a harm reduction strategy for marijuana consumption so that adverse effects cause less individual and collective harm. This strategy was more prevalent among individuals with postgraduate and graduate degrees, who use it more frequently and for longer durations, indicating that this type of information can reach experienced marijuana users more easily. In a study that explored the different meanings of substance use and associated occupations, Kiepek et al 50 found similar strategies among marijuana users. Incorporations into people’s days and weeks were reported, providing meanings associated with routine and ritual, from uses that meant a clear demonstration between work and leisure, “any activity that you do of this type of shutting down your brain or sort of putting it into a non-working mode” or as a “weekend treat.” As this study was carried out in a country where marijuana is legal, the participants shared a legacy of stigma and misunderstandings that created apprehension about disclosing or concealing the use of a substance that was once considered harmful.
Given the reflection on the critical perspectives of occupation that aim to overcome dualisms, recognizing that its social validation takes place in the context of power struggles, social values, and moral points of view, and that its nature is politically constructed, 45 we agree that the concept of negative consequences is correlated with social marginalization and oppression. 51 According to the Drug Policy Alliance, 75 an American non-governmental organization dedicated to building alternatives to current drug policies, Harm Reduction “is a set of ideas and interventions that seek to reduce the harm associated with the use of drugs and racialized and ineffective drug policies,” in contrast to the punitive approach to problem drug use. Harm Reduction focuses on the prohibitionist gap in information about drugs and users’ rights, developing care and reception strategies that make drug use as least harmful as possible to the individual and society, always based on horizontality and collectivity. 75
The response-variable “daily use” was selected given that it is considered a higher-risk use, as mentioned by 59% of the respondents. In our study, those who identified as yellow had a higher chance of using it on a daily basis than those who identified as white; those who used the substance for more than 1 year had a higher chance of using it on a daily basis than those who used it for less than 1 year, and those who used it for more than 20 years had a threefold higher chance of using it on a daily basis. Women-gender people had lower odds of using it daily compared to men. People who received 11 or more minimum wages (more than US$2298.34 per month) were less likely to use it daily compared to those who earned less than 1 minimum wage (less than US$203 per month); and people who began using marijuana between the ages of 16 and 29 were less likely to use it daily.
Among recreational marijuana users in Brazil, those who sought treatment were predominantly between 12 and 25 years old (72%), single (78%), male (72%), with high school or higher education (53%), with a family income of up to US$2560.00 (94%), and 30% used other associated substances. 31 A systematic review of high-quality evidence on behavioral factors that determine adverse health outcomes from marijuana use revealed that informed behavioral choices among users may substantially reduce an increase in the risk of adverse health outcomes from cannabis use. 56 The authors developed the Lower-Risk Cannabis Use Guidelines (LRCUG) as a targeted prevention tool to improve public health outcomes with 10 recommendations, including avoiding high-frequency (daily or near daily) cannabis use and preventing early age initiation of cannabis use—definitively before the age of 16 years. 56 Drug use should also be considered a public health issue, targeting the reality of those who use marijuana to improve their health and quality of life, as well as those who favor access as a treatment resource for a variety of health problems. 71
Implications for occupational therapy practice
In Occupational Therapy, everyday life has been defined as “a space-time in which the subject, individual or collective, immediately and not always consciously, accesses opportunities and resources, faces adversities and limits, makes decisions, adopts mechanisms of resistance and invents new ways of being, being, live and do.” 53 When occupations are viewed as entirely promoting health or disease, the various aspects or nuances of the occupation that have the potential to influence health and well-being positively or negatively are neglected or inadequately addressed, thereby limiting the practice of occupational therapy and preventing the assessment of clients’ complete occupational repertoires. 47
Occupations such as sex work, engaging in crime, selling or using drugs, panhandling, and vagrancy are often judged as poor choices or evidence of a poor moral character. This perspective assumes that agency occurs at the individual level and that all potential options are equally available to all people; it fails to unearth the social forces that shape occupations. 45
Thus, drug use can result in varied daily lives, which can be evaluated from the standpoint of occupational engagement. Drug use, whether problematic or not, is a human activity that must be considered if it gains prominence in people’s lives and enhances their well-being. In addition to having therapeutic potential, drug use can play a role in determining health, articulating or not well-being, justice, the organization of behaviors, and being forged together with various lifestyles and contexts.
Kiepek et al 45 took the construct of resistance as a lens for analyzing how non-sanctioned occupations defy prevailing expectations and may not fail attempts to meet expectations, but rather active practices of transgression—everyday acts of resistance that oppose power relations that validate certain ways of doing things, thereby generating opposition to occupational inequities. Non-sanctioned occupations as forms of resistance can contribute to the development of a knowledge base regarding the transformative potential of occupation, while avoiding the danger of perpetuating the marginalization of private and collective actions.
As predictors of well-being, whether impediments or facilitators of its reach, the following factors stand out: (a) the greater chance of using marijuana for recreational purposes among men and trans/non-binary people, graduates, and with higher incomes; (b) living with family members and using them less frequently as protective factors for the adverse effects of “getting high”; (c) more likely to have problems with the police due to marijuana use among Indigenous peoples (3 times more likely) and people aged 18 to 29 years (10 times more likely); (d) use at strategic moments more frequently among individuals with postgraduate studies and higher education, those who use marijuana more frequently, and those who use it longer; (e) greater chance of daily use among self-declared yellow people and those who have used it for more than 20 years, with protective factors being female and having a higher income. Maximino and Tedesco 76 recognized the dialectic of everyday life that, while materializing what oppresses us, also makes micro-resistance present, resulting in “subtle shifts in the borders of domination.” When confronted with the fact that nearly 60% of respondents use marijuana on a daily basis, to the detriment of prohibition, we are made aware of the potential harm caused by consumption while facing an act of resistance to prohibitionism. We then recover well-being within the scope of occupational therapy, as a goal of interventions and as a state that can be determined by occupations,34,35 when the research begins with a non-stigmatizing approach to drug use to highlight the dynamic interaction between the highlighted predictors, which can then provide the desired well-being and/or exposure to higher risk situations related to use.
With the aim of promoting self-care and establishing new political, cultural, and economic relationships, we posit that harm reduction, as a reference for occupational therapists in caring for people who use drugs, can anchor actions to value the diversity of bodies, knowledge, and cultures, directing efforts toward care in freedom with the goal of social transformation of those who experience process addiction. 77
As a matter of social justice and contributing to social legitimacy, occupational science can play a significant role in developing a critical understanding of the social construction of occupations as moral or immoral, deviant or normal, and healthy or unhealthy, as well as different ways of acting and being.
Study limitations
Consideration is given to the study’s limitations. The probabilistic analyses conducted using non-probabilistic sampling, and the use of a closed online survey. In addition to being criminalized in Brazil, the population of interest is not listed so that an accurate sample can be drawn; therefore, the sample size was used as a strategy to qualify our efforts but does not permit generalizability of the results presented. The configuration of the sample by individuals who agreed to complete the online questionnaire, despite being a strategy widely employed by online recruitment studies, also limited the information derived from the respondents’ comprehension. Nonetheless, despite these limitations, the results shed light on a subject that has been inadequately explored and on which further research is required.
This exploratory study aimed to provide a general and descriptive overview of the findings, requiring further studies to deepen the highlighted aspects. The exploratory study allows for a descriptive approach to prevalence with less generalization ability due to the biases of the respondents.
Future research
We highlight some findings that caught our attention and warrant further exploration, such as “having fun” being cited by interviewees as a positive effect of use; investigating whether the lower use of entertainment among these populations may be related to the overload of the women’s occupational roles 78 ; if gender differences exists in the motivation for using marijuana 7 ; whether restrictions on the use of entertainment among people with higher income may be related to class inequalities in access to leisure, with less use of spaces and entertainment strategies by the low-income population 68 ; and, finally, whether trans people would have more enjoyable experiences associated with the consumption of psychoactive substances. 69 Future studies guided by the human experience of drug use are desirable, in addition to the damage caused by its consumption, to better understand its meanings, risks, and potential, and then to plan an action that broadens participation and protects individual, collective, and citizenship rights.
Conclusion
This is the second study conducted in Brazil involving a non-clinical population of marijuana users and the first from an occupational perspective to examine predictors of well-being among the effects of marijuana use and its prohibition on the daily lives of adults. Social class, race, gender, and generation were predictors of well-being associated with marijuana use and its prohibition, indicating an interaction between different dimensions involving the use of illicit substances. Identifying the effects of the use and prohibition of marijuana in promoting well-being from the conception of drug use as a non-sanctioned occupation can broaden the understanding of this complex human phenomenon, which includes health and criminal repercussions that can subsidize the development of approaches more equitable and adequate in occupational therapy to reduce personal and social harm.
Footnotes
Acknowledgements
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Luciana Togni de Lima e Silva Surjus was responsible for the conceptualisation, study design, literature search, data interpretation, writing and review.
Natalia Cavalcante Dainesi was responsible for the study design, data collection, data interpretation and writing.
Felipe Granado de Souza was responsible for data design, data analysis, writing and review.