
Abstract
The “Severe Acute Respiratory Syndrome” (SARS), which has relation to the coronavirus-2 considered to be a major cause of the disease addressed by COVID-19. COVID-19 requires the angiotensin converting enzyme 2 (ACE-2), which is considered to be the target receptor of the host cells. The intention of this practical research study was to observe ACE I/D polymorphism association with COVID-19 and also the in-silico screening of potential phytochemicals against COVID-19. This study incorporated total of 320 blood samples; of which 160 were collected from COVID-19 patients and 160 were collected from healthy controls. DNA extraction was conducted from whole genomic blood and afterward, the banding patterns of ACE polymorphism were identified by the application of a nested polymerase chain reaction. A significant discrepancy was recorded in the frequency of insertion/deletion (ID) and homozygous deletion (DD) between controls and patients. The frequency reported for ID was just 10% and that of DD (genetic constitution) was 90%. Predictably, a 100% DD genetic constitution was shown by all the controls. The inference of this study was that the DD genotype has a greater prevalence in COVID-19 as compared to II and ID. In-silico screening of potential phytochemicals against COVID-19 is very effective in its concentrated form showing no or fewer side effects and can be used as a drug against COVID-19 spike protein blockage to inhibit the interaction between ACE-2 receptors. The highest affinity and lowest binding energy were observed by Dictaminine.
Introduction
Corona-viruses giving a positive sense with alternative genetically name RNA virus which is surrounded by an envelope, and the size of Coronaviruses ranges from 60 nm to 140 nm in diameter. It is called Coronavirus due to its spike-like protrusions on it’s outer surface, which gives it crown like look under an electron microscopy. 1 In December 2019, Chinese authorities informed the world that Novel virus was spreading through their communities. This novel virus was identified on 7 January 2020 as a Coronavirus that had more than (70%) homology with the SARS-CoV and more than (95%) similarity with the bat Coronavirus. In the months of January and February 2020, the virus spread to other countries, and the cases within China and around the world doubled within days. The most affected countries were China, Italy, America, Spain, other countries were also surrounded by its affect but to a minor extent, the virus also entered Pakistan during the early days of March 2020.1,2
This new virus had more than 40 mutated strains, half of which are present only on spikes protein. SARS-cov-2 variant is also known as variant of concern (VOC), and this name is given by World Health Organization (WHO). The actual name of omicron is (SARS-COV-2) B.1.1.529. In terms of rate of spreading, it was faster than any type in the SARS family. Its rate of spreading is three times higher than the Delta variant. More than 50 mutations have been discovered in the omicron variant. Now omicrons have been identified in more than 90 countries worldwide within very short period of its discovery. Its infection may be leading value of COVID patients. It was also observed that antibodies of recovered patients are not effective against other variants of the SARS family. But in case of omicron, they show unique response in being absorbed by cell showing that mutation in omicron is the result of surface variation by the virus. 3 This is the reason why omicron has doubling time of infection and spreading while in case of other variant they have effective response by antibodies. The booster with previously applied two doses of vaccination is compulsory for complete protection against omicron. It is experimentally observed that only two doses of vaccination are not enough to get protection against omicron, but booster is also required. The vaccine particularly stimulates the growth of T cells which help to protect the body against disease. The function of T cells is reorganization of antigen cells or foreign particles to protect the body. It was also found that T cells which recognize COVID virus are also working in reorganization of omicron virus which proofs that COVID and omicron has some same relation. A dominant delta virus form of COVID virus is equally working with lowest form of omicrons virus. It was also found that there is no chance of reinjection of delta variant after recovery from infection. The spreading rate of omicron is high. The S-gene is associated with omicron viral infection. Structurally omicron has three deletion and one insertion sequence in its protein. The chances of omicron infection are high among those who have COVID infection positive history. 2
Omicron infection is directly associated with substantial ability to evade immunity. New variant of is B.1.1.529 which was recognized in last of year 2021. Worldwide vaccinated population from COVID virus is not 100% which is also alarming to cause re-infection of omicrons. Those who are COVID vaccinated may have lower chance of omicron infection as compared to the non-vaccinated. It is also observed that this variant is partially resistant to previous immunity but not completely. Some of the variants of omicron have additional spike protein, which is almost more than 30, as compared to COVID, which has no effect with medicine and has the capacity to escape from host immunity due to alpha and beta variants with S gene target failure and S gene dropout. That’s why RT-PCR test is not enough to confirm presence of omicron in patient, but sequencing is also compulsory for complete confirmation. To get epidemiological data about transmission of omicron will be too early. Post fusion and past fusion spikes play major role in helping omicron infection in severe cases particularly N_RBD and C_RBD region. 3
The virus may survive on surfaces for days, provided it receives favorable atmospheric conditions. However, it remains uncertain how long the virus can survive under proper atmospheric conditions. Incubation period ranges from 2 to 14 days. When people cough and touch their nose, or rub the eyes with contaminated hands, the virus starts its journey and penetrates deeper into the body. Its destinations are the intestine, the lungs, and the spleen where it can have the most devastating effects. The lining of lungs is comprised of billions of epithelial cells. Covid-19 begins its damaging effect by connecting to specific receptors (ACE) on the host membrane and injects its genetic material. The host cells get new instructions that are copied and reassembled. Lungs get filled up with an increasing amount of these copies of parental virus until they reach the critical order of self-destruction. Afterward, the host cells release new corona particles and are ready to infect more host cells. In such conditions, the immune system protects us which can be dangerous for ourselves. 4 Thus, tight regulations are required; reason being is that when the cells of immune system get into the lungs to combat against Coronavirus; the virus infects many given amounts of these cells too, prompting misunderstanding. Coronavirus causes infected cells in the immune system to overreact and ultimately burst. Every immune reaction is regulated by a protein known as cytokine. The immune system will send more soldiers, thus wasting its resources and as a result causing more damage. Two kinds of immune cells are involved; one is neutrophil that releases several enzymes to kill the virus, and the second is killer T cells which get an order to kill the infected cells. These confused immune cells are siphoned away from killing the virus, and, instead, kill the healthy cells. In other words, the more immune cells arrive, the more harm to the lung tissue occurs. Coronavirus sometime cause irreversible damages, which may even cause lifelong disabilities. On the other hand, if the humoral and cellular immunity clears up, the battlefield recovery begins. 5
Majority of the patients have marked symptoms like headache, dry cough, fever, flu, fatigue, myalgia, and breathlessness but in some cases this gets increasingly severe; the marker of this severity is the epithelial cell death has increased and the protective lining of the lungs are gone. Coronaviruses are often compared with the flu, but it is in fact much more dangerous than flu as it is more contagious. 6 Alveoli can be co-infected by bacteria and may even cause patients to contract pneumonia; respiration gets difficult and even fails, such patients require a ventilator for survival. The immune system makes antiviral weapons, but as bacteria become overwhelmed it may enter the blood; this can cause death. In such conditions, antibiotics or antifungals are required for the treatment of co-infections. WHO suggested that initial mild symptoms might case of omicrons viral attack especially for travelers should diagnose it immediately. 7
Vaccination trial against COVID was developed in 2021, but these vaccination trials against omicron are not clear yet. More observation and trials need to be done for further confirmation. 8 While unvaccinated community is seeming to be more effective and high hospitalization report than vaccinated. Major error while producing vaccination against COVID and omicron is phase variation and secondly viral escaping ability from host immune system is also remarkable error. The companies Moderna, Pfizer and Jonhson have strong trust on vaccines produced by them and according to their statement given to public that their produced vaccines have ability to not only protect against virus but also against many other disease. 9 The WHO and CDC (Centers For Disease Control) has imposed restrictions on travelers and asked them to lemmatize their international traveling activity. Further strict SOPs are also imposing to be in quarantine for 1 or 2 weeks immediately after traveling either having negative PCR COVID report or completer health medical history. It is also advised to old people to stay at home and do avoid international traveling to avoid new variant of COVID (omicron). There are different types of variants that are affecting people. The most prominent variants are from different regions of the world, which are (B.1.1.7) this variant is found in the United Kingdom, the second variant is (B.1.1.351) this variant is found at south Africa region of world, third is (P.1) this variant is considered as gamma variant and found in Brazil region, and fourth and last one is delta variant which found in India, neighboring country of Pakistan and have huge population over countrywide, the variant structure is (B.1.627.2). 10 This entire variant has most transmissible properties as compared to another virus which is drastic situation over the other region of world also. More than 300 cases have been reported to European Center for Disease Control all over the world. In Pakistan, 2289 patients were admitted in hospitals within 24 hours due to omicron attack. Punjab and Sindh were affected majorly. Two big cities Karachi and Lahore having high ratio of affected patients. 8 It is also considered that immunity against COVID was developed cannot be developed even against omicron. It will keep threatening our immunity. As Dr. Olivier le Polain, an epidemiologist with the World Health Organization (WHO) told that “Reaching a theoretical threshold beyond which transmission will cease is probably unrealistic given the experience we have had in the pandemic.” 11 In case of omicron, the booster vaccination will only reduce the infection severity, but it will not destroy the infection from the body. “As long as population immunity holds with this variant and future variant, we’ll be fortunate and the disease will be manageable,” said Dr. David Heymann, a professor of infectious disease epidemiology at the London School of Hygiene and Tropical Medicine. 12 The COVID vaccine was not designed to cure the patient infected with COVID, but to reduce the infection rate and death rate among the people. This omicron virus has ability to quickly elucidate from host immunity by creating mutation in its behavior that host immunity becomes unable to recognize the antigen (omicron) inside the body. A Francois Balloux, professor of computational systems biology at University College London, told Reuters said that we may get herd immunity after 60% of vaccination all over the world, and if we are not getting herd immunity the we need to enhance vaccination percentage up to 80% which will develop herd immunity, but in case of failure we need to increase percentage of vaccination among people to protect them and to stop death rate. 11 The CDC has taken step to surveillance the data analyzing SARS-CoV-2 load circulating among the United State. This system will be systemized by getting genomic data and information from all over the world to manage surveillance data against SARS-CoV-2. 13 As concern with effective vaccine primarily it was calculated that BNT162b2 and ChAdOx1 with two connective week follow-up BNT162b2 booster may immunize the person against COVID variant. 14
Chloroquine is a therapeutic agent as it acts as a prophylactic drug against COVID-19; sister to SARS-Coronavirus. It functions in three ways: one by increasing the pH of endosome (by acting on the host respiratory cells) which is required for the fusion of the virus and host cells. The impacts of this increase are that normal viral functions are disrupted by increase in the pH. Second, the drug interferes with the glycosylation pathway present in the cellular receptors of the virus. COVID-19 requires ACE-2 receptors for attachment to the host cell and chloroquine results in disablement of terminal glycosylation of ACE-2 receptor, which leads to change in its morphology and interferes in the association between the host cell and the virus. 15 The overarching objective of this study is to discern the extent to which there might be a relation between ACE polymorphism (I/D) and COVID-19 as well as in-silico screening of potential phytochemicals against COVID-19.
Material and Methods
This study on COVID-19 patients related to ACE polymorphism was conducted from Lahore. Sampling of blood was done from the National Hospital, Lahore. Coronavirus was diagnosed in the 160 blood samples and another 160 samples were included as controls. Among those 160 patients, 104 were males and 56 of were females. A proforma was designed to collect the information from the patients and endorsement of the participants (for the research purpose) was taken on consent form. During diagnosis special importance was given to the travel history as well. DNA was extracted from whole genomic blood by utilizing kit method (Fermentas). For detection of the isolated DNA, agarose gel electrophoresis was carried out and then the nested PCR was done by employing three specific primers for Intron 16 region of ACE gene in order to detect polymorphism. The ID and DD genetic constitution were identified by agarose gel electrophoresis. If the band was of 190 bp, it was considered as DD genotype; 190 bp + 287 bp, ID genotype; 287 bp + 464 bp, II genotype. The collected data were then statistically analyzed by using the chi-square test to check the significance. If the probability is <.05, then it is not reflected to be statistically significant.
In-silico screening of potential bioactive chemicals to block COVID-19 spike protein, this approach gives a clue to step forward toward drug discovery to cure COVID-19. In which special computational tools were used to predict possible therapeutic agents in plants by protein-ligands interactions. The 3D structures of ligands were retrieved from different chemicals data bases like PubChem, ChEMBL and Zinc 15 while COVID-19 spike protein in complex with ACE-2 receptor was retrieved from PBD (NCBI) with ID 7FEM. The SDF format of ligands was converted into PDB format by using online SDF to PDB convertor. Then, PDB ligands were changed into PDBqt format in Auto Dock Vina and saved into the drive C. The active site of the spike protein was observed in PyMol, and additional water and ligands were removed. Then, the spike protein was converted into PDBqt format in Auto Dock Vina and saved into the folders with ligands into the drive C. The active site was fixed within the grid box by in Auto Dock Vina and command was run within command prompt.
Results
Gender distribution among COVID-19 patients
320 blood samples were collected of which included 160 COVID-19 patients and 160 healthy controls. Among the 160 patients, males were 104 (65%) of the patients and females were 56 (35%), making the ratio of male to female is 13:7 (Figure 1).

Gender distribution among COVID-19 patients.
Symptoms observed among COVID-19 patients
The most common symptoms found in COVID-19 patients were headache (100%), fever (100%), flu (50%), dry cough (50%), breathlessness (20%), and myalgia (10%) (Figure 2).
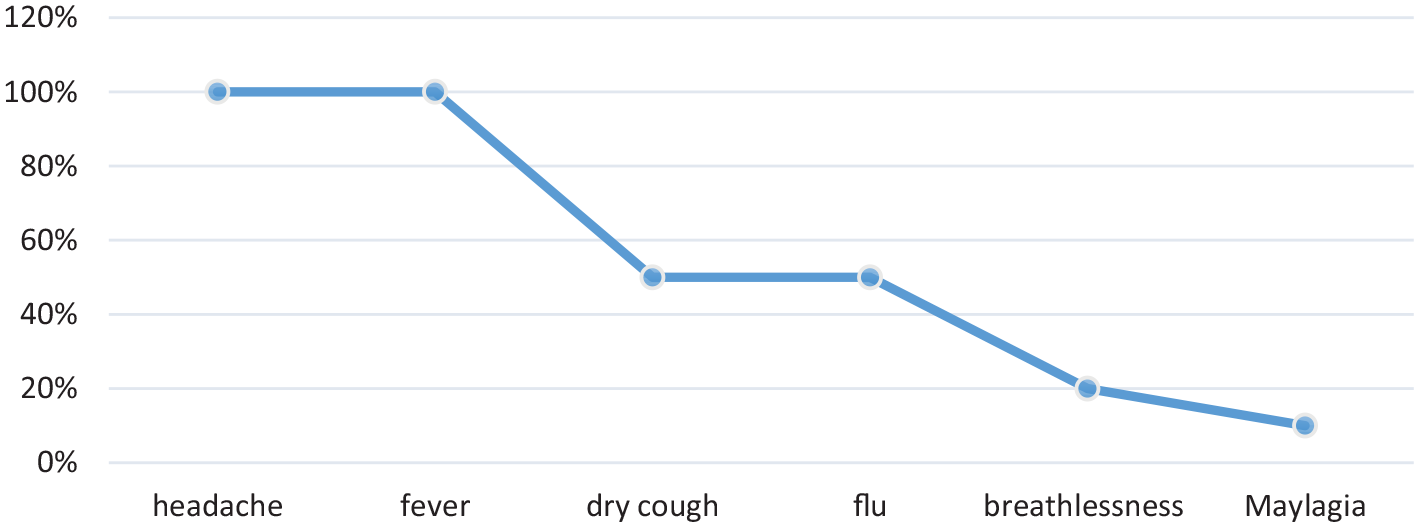
Symptoms observed among COVID-19 patients (n = 160).
Raised laboratory parameters observed among COVID-19 patients
Different laboratory parameters were noted such as the 50% of the COVID-19 patients who were reported low WBCs count, raised inflammatory markers like erythrocyte sedimentation rate (ESR 100%) and C-reactive protein (CRP 100%) were also observed among COVID-19 patients (n = 160) (Figure 3). Among hospitalized patients, hypertension was one of the most common problems observed and 75% of the patients had a travel history.

Raised laboratory parameters (low WBC count, raised CRP and ESR) observed among COVID-19 patients (n = 160).
Detection of the (I/D) Polymorphisms in COVID_19 Patients using Polymerase Chain Reaction (PCR)
DNA extracted from the whole genomic blood and then the nested PCR was done to detect the ACE polymorphism (I/D) banding patterns. A stark statistical difference was observed between the frequency of insertion/deletion (ID) and deletion (DD) of controls and patients. The frequency reported for ID was just 10%, and that of DD genotype was 90% in the COVID-19 patients. In all, 100% DD genetic constitution was reported in all the controls (Figure 4).

PCR gel picture representing DD and ID genotype.
Types of ACE polymorphism observed in COVID-19 patients
By the application of chi-square test the association between the ACE polymorphism and the controls cases were tested. The DD genotype showed significant relation in both the patients as well as in the controls (Table 1). As the value of P is < .05, therefore, the result was found significant. Indicating that there is strong correlation between COVID-19 and ACE I/D polymorphism. Figure 4 showed DD genotype represented by a banding pattern of 190 bp, ID genotype (190 bp + 287 bp). Distribution of DD genotype in COVID-19 patients in relation to COVID symptoms are shown in Tables 2 and 3.
Types of ACE polymorphism observed in COVID-19 patients.

Relation of ACE I/D polymorphism with the symptoms of COVID.

Multiple Regression, impact of age and fever/flu.

Where Z1 is unknown value.
If age increases, for example, Z1 = 50
Then,
We can see that by increasing age, COVID cases increase. The same is true for other symptoms like fever/headache/flu.
Phytochemicals against COVID-19
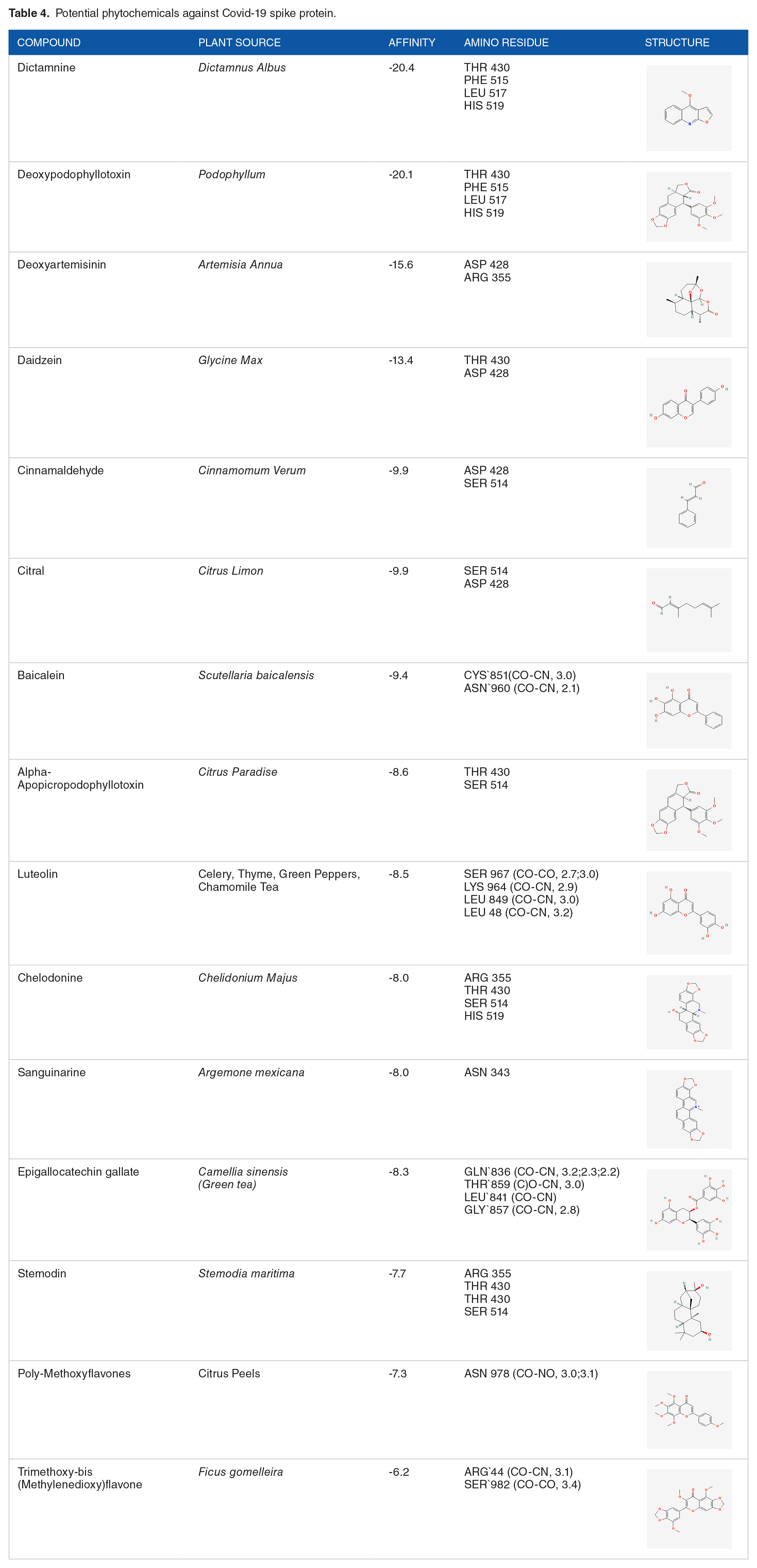
Although chloroquine is being considered as potential treatment of COVID-19 that alters ACE-2 receptor structure and interferes glycosylation process of COVID-19 to prevent host-pathogenic interaction. There are some potential phytochemicals that block spike proteins of COVID-19. These spike proteins (S protein) bind to ACE-2 receptors to get entry into the host cells. If these S proteins are blocked by these phytochemicals, entry of COVID-19 into host cells can be inhibited. Some potential phytochemicals which have been screened in-silico are given in Table 4.
Potential phytochemicals against Covid-19 spike protein.
ADME properties.

To screen potential spike protein inhibitors in-silico, a variety of phytochemical structures were downloaded from PubChem in SDF format, then converted into pdb format by application of online SDF to PDB convertor. After that pdbqt format in Autodock Vina and results were observed in PyMol. Lipinski’s rule of five to evaluate drug likeness was applied by submitting canonical smiles of phytochemicals on SwissADME platform. COVID-19 spike protein structure was retrieved from PDB and PHE 429, THR 430, PHE 515, GLU 516 and LEU 517 residues were targeted to block spike protein.
ADME Properties of Compounds
ADME stands for absorption, distribution, metabolism, and excretion of a chemical, a chemical to behave as a drug and bioavailability (Figure 5). These properties are validated by applying Lipinski’s rule of five. If a chemical follows these rules, that chemical may show as drug likeness and might be used as drug (Figure 6).
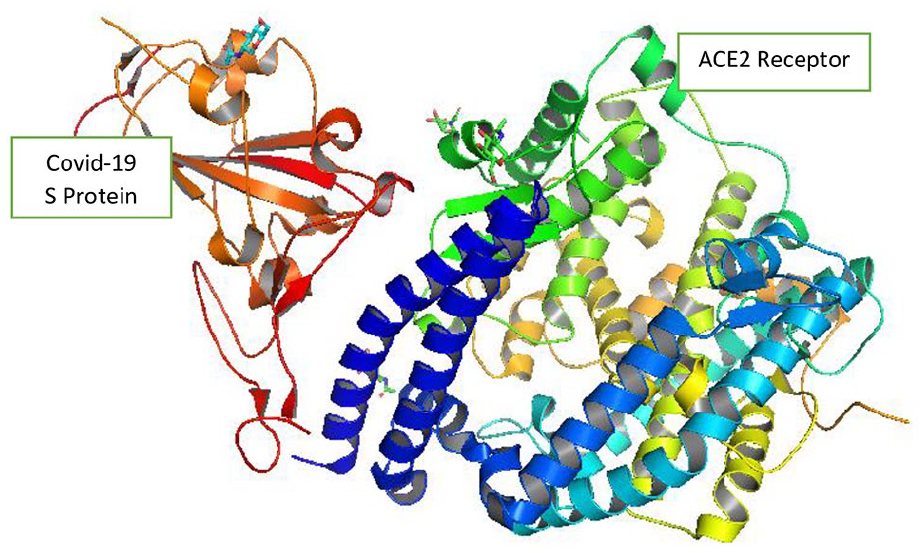
Interaction between Spike Protein (left) and ACE2 receptor (right).

Phytochemicals binding energies with COVID spike protein.

Phytochemicals affinity with spike protein: dictaminine(A), baicalein(B), epigallocatechin gallate(C), citral(D), Luteolin(E), and poly-methoxyflavones(F).
Discussion
ACE-2 receptors aid the coronavirus in its attempt to infect human cells; such receptors are expressed mainly on the lungs but are also present within the tissues of the patients. ACE-2 helps in brisk viral replication, while ACE-2 reduction from cell membrane facilitates in deteriorating effectively of angiotensin II inside the lungs. The ACE-1 I/D polymorphism (in intron 16) are related with variations in tissue concentration and circulation of ACE. The deleted material is linked with decreased expression of ACE-2.16,17 Since this polymorphism is found in a non-coding (Intron) region, this activity cannot be contemplating a functional variant, but second one I/D polymorphism can influence both plasma and tissue levels of ACE. 13 The data propose that the ACE1 D/I polymorphism may be considered as perplexed aspect in the COVID-19 spread, and consequently infection in several European communities. These outcomes suggested that in pulmonary infections the role of ACE is due to coronaviruses. The ACE D/I genotype may impact infection clinical course. 7 In this study, association of ACE I/D polymorphism was studied with COVID-19 infection as ACE polymorphism (I/D) may be involved in process of pathogenic of COVID-19.
RNA-sequence analysis indicated that higher expression level of tissue ACE2 in comparison to their ethnic counterparts. In the present study, more males (65%) were affected with COVID-19 infection than females (35%). However, people of all ages are prone to COVID-19 infection. Children within ages of 6 months to 17 years, also have higher level of ACE-2 than adults. The mean age of the participants was 37 years ± 1.56. It was also proved that younger animals are resistant to SARS-CoV infection than in comparison to older animals. Females in the third trimester have high level of ACE-2 in urine and plasma which is later transferred to the baby through the placenta. 17
Symptoms of COVID-19 have an interlinking relationship with the level of expression of ACE-2 enzyme in different body tissues; moreover, the circulatory or unattached ACE-2 has role in potentially restricting the corona virus gateway to the pulmonary epithelium as compared to attached ACE-2. 18 In the plasma of COVID-19 patients, elevated level of Ang-II depicted linear association with lung damage and viral load. 19 The affinity of virus binding to ACE2 on alveolar pneumocytes leads to reduction of these cells, contributing to decrease in secretion of surfactants, also declining the capacity to repair the damaged tissues and ultimately leading to worsening of lung injury in serious COVID patients.20,21 Consequently, all these findings evidently suggested that the disease severity of viral infection can be provoked by the regulation of ACE2 and subsequently have part in the pathogenesis of COVID-19.
Previously ACE-2 was found to be a significant biomarker for blood pressure. However, this study also indicated that ACE-2 can be used as prognostic marker in monitoring COVID-19 infection. The ACE I/D polymorphism do not show any direct relation regarding increased susceptibility to SARS-CoV infection. 22 In the present study, comparison between cases and controls were made for ACE I/D polymorphism and the results found were significant. In both the cases and controls, the frequency of DD genotype of ACE I/D polymorphism were contrarily found higher. The solemnity of the coronavirus patients may hinge on age, hypertension, diabetes, and ACE gene polymorphism. These findings suggest that there is a significant relationship between COVID-19 and ACE I/D polymorphism. Thus, it can be concluded that DD genotype is predominant in COVID-19 as compared to ID and II. There is still a need to understand the mechanism of the ACE polymorphism in the infection of COVID-19 patients, particularly because of its potential to further help in its therapy responses. ACE I/D polymorphism can be used as a beneficial tool to anticipate development of disease and may have an impact on treatment results against the COVID-19 to demonstrate a population-based therapeutic relationship.
If we discuss about chemotherapy of COVID-19, plants have a variety of potential bioactive compound which might be used as drugs to inhibit interaction between ACE2 receptor and COVID-19 spike proteins. Phytochemicals show no or less side effects as compared to synthetic drugs. These phytochemicals showed highest affinity having lowest binding energy to the target protein. This binding energy shows suitable interactions of ligand to the target protein active site.
The highest affinity and lowest binding energy were observed by dictaminine (-20.4). Dictaminine phytochemical is present in Dictamnus albus species which belongs to family Rutaceae. It is also famous as Burning Bush, Dittany, Gas Plant or Fraxinella. More than 100 chemicals have been extracted from this species like alkaloids, flavonoids, phenylpropane, limonoid triterpenoids and coumarins. In Pakistan, it is found in Western Himalaya. 23 Its side effects include cytotoxicity in women cervix, colon, and oral carcinoma. Despite of all these harmful side effects, it has an ability to fight bacteria and fungi like Saccharomyces cerevisiae, with a very low inhibitory concentration.
The second highest affinity and lowest energy was shown by deoxypodophyllotoxin (-20.1). Deoxypodophyllotoxin is extracted from Podophyllum species belonging to Berberidaceae family. It is native to Eastern United States and Southeastern Canada. The whole plant is very toxic except its ripened fruit that is nontoxic. Deoxypodophyllotoxin is a lignin type chemical which has a potential to treat tumors and inflammation. It is also used as purgative and cytostatic. Due to its high toxicity, it has not yet been used clinically. 18 Deoxyartemisinin is isolated from Artemisia annua species belonging to Asteraceae family. It has been found that it can block the replication of the SARS-CoV-2 virus along with its recent variants. This plant species also has flavonoids which also inhibits the replication of SARS CoV-2. It has anti-malarial, anti-scabies, anti-Candida albicans infections, anti-bacterial capabilities like E. coli, Salmonella, and other bacterial infections along with plasmodial parasites including Schistosomas. 19 Poly-methoxyflavones are found in peels of citrus fruits like oranges, lemon, and so on, which are common plants in subcontinent. Baicalein is a potential flavonoid extracted from Scutellaria baicaleinsis that has anti-inflammatory, anti-cancerous, antibiofilm against Candida-resistant species, as drug for cardiovascular disorders and reduce oxidative stress.23,24 It is also used in hepatitis and kidney problems. Citral is extracted from Citrus limon having anti-inflammatory, anti-cancerous, antioxidant, antimicrobial that shows long-term bioavailability with low side effects. 21 The above-mentioned phytochemicals are present in plants which can be easily found, and extraction can be done. They showed very low toxic effects and may be used as drugs against COVID-19 by optimizing their bioavailability.
Footnotes
Acknowledgements
I particularly would like to acknowledge the National Hospital how the ways they facilitate us with the working facilities and COVID-19 patients without them this research study qould bw impossible. I’d also like to acknowledge the principal editor of this paper, Aizaz Bokhari.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Ethical Approval
This project has been evaluated by Departmental Research Ethics and Bio-safety Committee. The committee could not find any Biosafety and Ethical concerns related to the proposed work during whole research work and its execution at the Department of Microbiology and Molecular Genetics, University of the Punjab, Lahore.