
Abstract
Background
Postoperative risk stratification for severe acute kidney injury (AKI) can facilitate timely intervention and improve prognosis.
Objectives
This study aimed to evaluate the added predictive ability of urinary calprotectin for postoperative risk stratification of severe AKI in non-cardiac surgery patients.
Design
A total of 580 patients were enrolled, and 98 (17%) developed severe AKI with a median time of 12.8 hours after SICU admission.
Methods
In a prospective cohort of patients transferred to the surgical intensive care unit (SICU) after non-cardiac surgery, calprotectin was measured in urine samples collected 0, 6, and 12 hours after SICU admission. A clinical model for predicting severe AKI was established. We tested the ability of urinary calprotectin alone to predict severe AKI by area under the receiver operating characteristics curve (AUC) analysis. We further evaluated the improvement of the pre-diction ability after adding urinary calprotectin in the clinical model by the increment in AUC, relevant integrated discrimination improvement (IDI), and net reclassification improvement (NRI).
Results
Higher urinary calprotectin levels were observed in the severe AKI group at any time point (All P<0.001). In the entire cohort, the AUC of urinary calprotectin at SICU admission for predicting severe AKI was 0.701(95% CI, 0.649 to 0.754), and calprotectin ≥32.3 ng/ml was associated with increased risk (OR 6.119, 95% CI 3.259 – 11.488). The AUC of the clinical model increased from 0.693 (95%CI, 0.633 to 0.754) to 0.730 (95%CI, 0.677 to 0.784) upon adding urinary calprotectin, the NRI was 0.337 (P<0.001) and the IDI was 0.055 (P<0.001).
Conclusion
A combination of urinary calprotectin and clinical features could be useful for postoperative risk stratification of severe AKI in non-cardiac surgery patients.
Introduction
Acute kidney injury (AKI) represents a significant postoperative complication following non-cardiac surgery, occurring in 5.3% to 15.3% of patients.1-3 While AKI encompasses a wild severity spectrum, severe cases, typically defined as KDIGO stage 2 to 3, are associated with greater burden, including increased short-term mortality and elevated long-term risks of chronic kidney disease (CKD) and end-stage renal disease in the long term.3-6 Given the lack of effective treatments for established severe AKI, the early identification of patients at high risk is critical for guiding timely preventive strategies and optimizing resource allocation.
Traditional clinical risk models, such as those based on ASA score, effectively predict postoperative mortality but fall short in forecasting AKI. 7 In response, novel biomarkers like NGAL, 8 TIMP2*IGFBP7,9,10 and u-α-GST11,12 have been investigated for AKI prediction. However, their reported performance varied widely (AUC range: 0.52 - 0.83),and existing evidence predominantly comes from cardiac surgery populations.13-15 Since AKI after non-cardiac surgery differs in in pathogenesis, etiology, and severity, findings from cardiac surgery may not be directly transferable. Consequently, there remains a clear need for reliable predictors grounded in a more universal AKI pathophysiology and validated in diverse surgical cohorts.
Calprotectin (the calcium-binding protein S100A8/A9 complex) represents a candidate biomarker that meet this need. As a damage-associated molecular pattern primarily released by neutrophils, monocytes, macrophages, and kidney tubular epithelial cells,16-18 it triggers and maintains inflammation by activating toll-like receptor 4 (TLR4) and plays a significant role in AKI pathophysiology. While urinary calprotectin effectively differentiates between pre-renal and intrinsic AKI,19-22 its predictive potential remains underexplored. We previously found that macrophages with high expression of calprotectin (calprotectinhigh macrophage) were the earliest infiltrating inflammatory cells that exacerbated kidney injury in a mouse model of kidney ischemia-reperfusion injury; and urinary calprotectin levels correlated strongly with both calprotectinhigh macrophage infiltration density and the severity of kidney injury in AKI patients, suggesting superior temporal resolution. 23 These mechanistic insights position urinary calprotectin not merely as a diagnostic biomarker, but as a potential predictive biomarker for severe AKI, as it signals the early inflammatory response that can escalate into substantial kidney injury. This study therefore aims to evaluate the predictive value of urinary calprotectin—both alone and in combination with clinical variables—for severe AKI in patients admitted to surgical intensive care unit (SICU) following non-cardiac surgery.
Methods
Study Design and Participants
This observational, single-center, prospective cohort study was conducted at the Peking University First Hospital, China. All adult patients (aged≥18 years) transferred to SICU immediately after non-cardiac surgery from May 20, 2019, to November 24, 2020, were enrolled. Patients were excluded if they (1) had CKD stage 5 or undergoing long-term dialysis; (2) received surgery involving the kidney; (3) patients who satisfied the diagnostic criteria for AKI before SICU admission and the urine output diagnostic criteria for AKI within the first 6 hours of SICU admission were defined as having developed AKI before SICU admission 24 ; (4) without an indwelling urethral catheter; (5) without informed consent. This study was registered at https://ClinicalTrials.gov (NCT03880110). Ethical approval (2019-075) was granted by the Clinical Research Ethics Committee of Peking University First Hospital, and written informed consent was obtained from all participants.
Urinary Calprotectin Quantification
Urine samples were collected at 0, 6, and 12 hours after SICU admission, centrifuged, and stored frozen at -80°C. The storage duration prior to measurement ranged from 3 to 6 months. Urinary calprotectin was measured by enzyme-linked immunosorbent assay (ELISA) using a human calprotectin quantikine kit (R&D, USA, DS8900). Samples were diluted 1:100 according to the manufacturer’s instructions and measured in duplicate using a 96-well microplate reader (BioRad, Hercules, CA). Urinary creatinine (Cr) was measured in parallel using a validated enzymatic assay kit (BioAssay Systems, USA, DICT-500) on a regularly calibrated Promega GloMax® Discover Microplate Reader. Quality control included validating a fresh standard curve (R2 > 0.99), verifying low- and high-concentration controls provided by manufacturer, and duplicate measurement of all samples (mean value used). The calprotectin/Cr ratio was calculated to account for urine dilution.
Data Collection
Clinical information was collected prospectively by a prespecified case report form, including demographic characteristics, comorbid conditions, surgery type, and preoperative laboratory values (the most recent values available before surgery), Sequential organ failure assessment (SOFA) score, 25 acute physiology, and chronic health evaluation II (APACHE II) score 26 were collected within 24 hours of SICU admission. Risk factors for AKI (blood transfusion, hypovolemia, vasopressors, nephrotoxin exposure) and postoperative complications (bleeding, infection, sepsis, acute heart failure, and acute respiratory failure) were assessed by an independent researcher. We defined hypovolemia as systolic blood pressure (SBP) <90mmHg or decreased by >30% from the preoperative SBP; pyuria as more than 10 white blood cells per high-powered field; macroscopic hematuria as urine that is visibly tea-colored, cola-colored, pink, or even red 27 ; and anuria as urine output of less than 100ml per 24h. The baseline SCr was defined as the lowest SCr value from 3 months before admission to the time of surgery.
Outcome
Patients were followed until discharge, death, or 30 days after surgery, whichever came first. Urine output was monitored every 4 hours, and SCr values were measured daily at 6 a.m. AKI was diagnosed and staged according to Kidney Disease Improving Global Outcomes (KDIGO) criteria, defined by an increase in SCr of ≥26.5 μmol/L within 48 hours, a ≥50% increase in SCr within 7 days, or urine output <0.5 ml/kg per hour for 6 hours. 28 The primary outcome was severe AKI within 7 days after surgery, defined as AKI stage 2 or 3. AKI stage 1 and non-AKI were defined as no-severe AKI.
Statistical Analysis
Categorical variables were expressed as frequencies, and Chi-square or Fisher exact test was used to compare groups. Whereas continuous variables were expressed as mean±SD or medians (interquartile range) depending on whether data were normally distributed, non-parametric tests were used for group comparisons. Shapiro-Wilk test was conducted to test for normality. Missing values of urinary calprotectin due to anuria were not imputed. The receiver operating characteristic (ROC) curves were plotted to evaluate the prediction performance of urinary calprotectin and calprotectin/Cr at SICU admission (0h). The raw value of urinary calprotectin and calprotectin/Cr were used. The area under the curves (AUCs) values with 95% confidence intervals (95%CI) were calculated through the method of DeLong, and the optimal cutoff was defined based on the Youden index.
Given the sample size constraints, candidate variables for the clinical model of severe AKI were pre-selected based on established clinical relevance and prior literature, rather than on statistical criteria alone, including demographic characteristics (age, male, body mass index [BMI]), comorbid conditions (hypertension, diabetes, coronary heart disease, chronic heart failure, chronic hepatic disease, chronic pulmonary disease, cerebrovascular disease, cancer, and chronic kidney disease), surgery type, preoperative laboratory values (hemoglobin [Hb], albumin [Alb], blood urea nitrogen [BUN], and B type natriuretic peptide [BNP]), APACHE II score, and conventional risk factors prior to AKI (transfusion, hypotensive, vasopressors, and nephrotoxic agents), were evaluated first by univariate analysis and then by multivariate analysis. A stepwise forward selection was performed for multivariable analysis, starting with all the variables identified by the univariate analysis as potential predictors at P <0.10. The internal validation was performed using a regular bootstrap procedure with 1000 times, and bootstrap-estimated corrected AUC value was calculated by apparent - optimism. Model calibration was assessed by using calibration plots and Hosmer-Lemeshow goodness-of-fit statistic. The decision curve analysis (DCA) was used to evaluate the net benefit of the predictive model.
The improvement in prediction performance after adding urinary calprotectin into the clinical model was evaluated using increment in AUC, relevant integrated discrimination improvement (IDI), and net reclassification improvement (NRI). 29 For categorical NRI, we prespecified three risk categories (<3%, 3-10%, and >10%) adapted from prior postoperative AKI prediction studies. 30 Because clinically validated decision thresholds for severe AKI risk in SICU patients are not established, these categories were used to facilitate methodological comparison of reclassification rather than to define actionable clinical cut-offs. The confidence intervals for relevant NRI and IDI were computed by bootstrapping with 10000 replications.
The potential confounding effect of pyuria or macroscopic hematuria on urinary calprotectin levels (due to neutrophils release16-18) was prespecified for assessment; accordingly, the observed improved model performance in patients without these conditions is presented as an exploratory finding. Test for interaction was performed by including an interaction term (urinary calprotectin at SICU admission × pyuria or macroscopic hematuria) in a multivariable logistic model. If a significant interaction effect was found, subgroup analyses were performed. Two additional sensitivity analyses were performed. First, the clinical model was developed using only variables available at SICU admission, including patient characteristics, comorbid conditions, surgery type, and preoperative laboratory values, with variables selected through univariate and multivariate analyses. Second, least absolute shrinkage and selection operator (LASSO) regression was applied for variable selection to assess the robustness of the forward stepwise selection model and to mitigate the risk of overfitting. All candidate clinical variables were entered into the LASSO model, and the optimal penalty parameter λ was determined via 10-fold cross-validation. The λ value corresponding to the minimum binomial deviance was selected. Variables with non-zero coefficients at this λ value were retained for constructing the clinical model, after which a logistic regression model was built using the selected variables.
The analyses of relevant IDI and NRI (R package Hmisc), bootstrap validation, calibration plots (R package rms), Hosmer-Lemeshow goodness-of-fit statistic (R package ResourceSelection), DCA (R package rmda), and LASSO regression (R package glmnet) were performed using R software, version 4.1.0. All other data was analyzed using SPSS 26.0 software (SPSS Inc., Chicago, IL, USA), and P < 0.05 was considered statistically significant. We followed the TRIPOD statement (Supplementary Table 1).
Results
Clinical Characteristics
During the study period, 580 patients were finally enrolled, with a median age of 70 years (range: 20 - 96). The flow chart of the study selection was presented in Figure 1. Among the enrolled patients, 219 patients developed AKI within 7 days after surgery. Of those, 121(55%), 89(41%), and 9(4%) were classified as AKI stage 1, stage 2, and stage 3, respectively. Severe AKI occurred in 17% (98/580) of the enrolled patients at a median time of 12.8 (8.0, 19.3) hours after SICU admission. Table 1 summarizes the baseline demographic and clinical characteristics of the study population. Compared with no severe AKI patients, severe AKI patients were older, had a higher BMI, and presented with a higher prevalence of cancer history. They also had lower baseline eGFR levels, higher APACHE II scores, and higher nonrenal SOFA scores. Flow chart The Baseline Demographic and Clinical Characteristics of the Study Population AKI, acute kidney injury; BMI, body mass index; CHD, coronary heart disease; CHF. Chronic heart failure; CVD, cerebrovascular disease; CKD, chronic kidney disease; SCr, serum creatinine; eGFR, estimated glomerular filtration rate; Hb, hemoglobin; Alb, Albumin; BUN, blood urea nitrogen; BNP, B type natriuretic peptide; ACEI/ARB, angiotensin converting enzyme inhibitors/angiotensin receptor blocker; NSAIDs, non-steroid anti-inflammatory drugs; SOFA, sequential organ failure assessment score; APACHE, acute physiology and chronic health evaluation.

The Ability of the Urinary Calprotectin Alone to Predict Severe AKI
As shown in Figure 2, the urinary calprotectin concentration increased over time both in severe AKI and no severe AKI groups. Compared with no severe AKI, the severe AKI group presented significantly higher median urinary calprotectin values and calprotectin/Cr ratios at any time (0, 6, and 12 hours, all P < 0.001). Urinary calprotectin and calprotectin/creatinine (Cr) levels in severe AKI and no severe AKI groups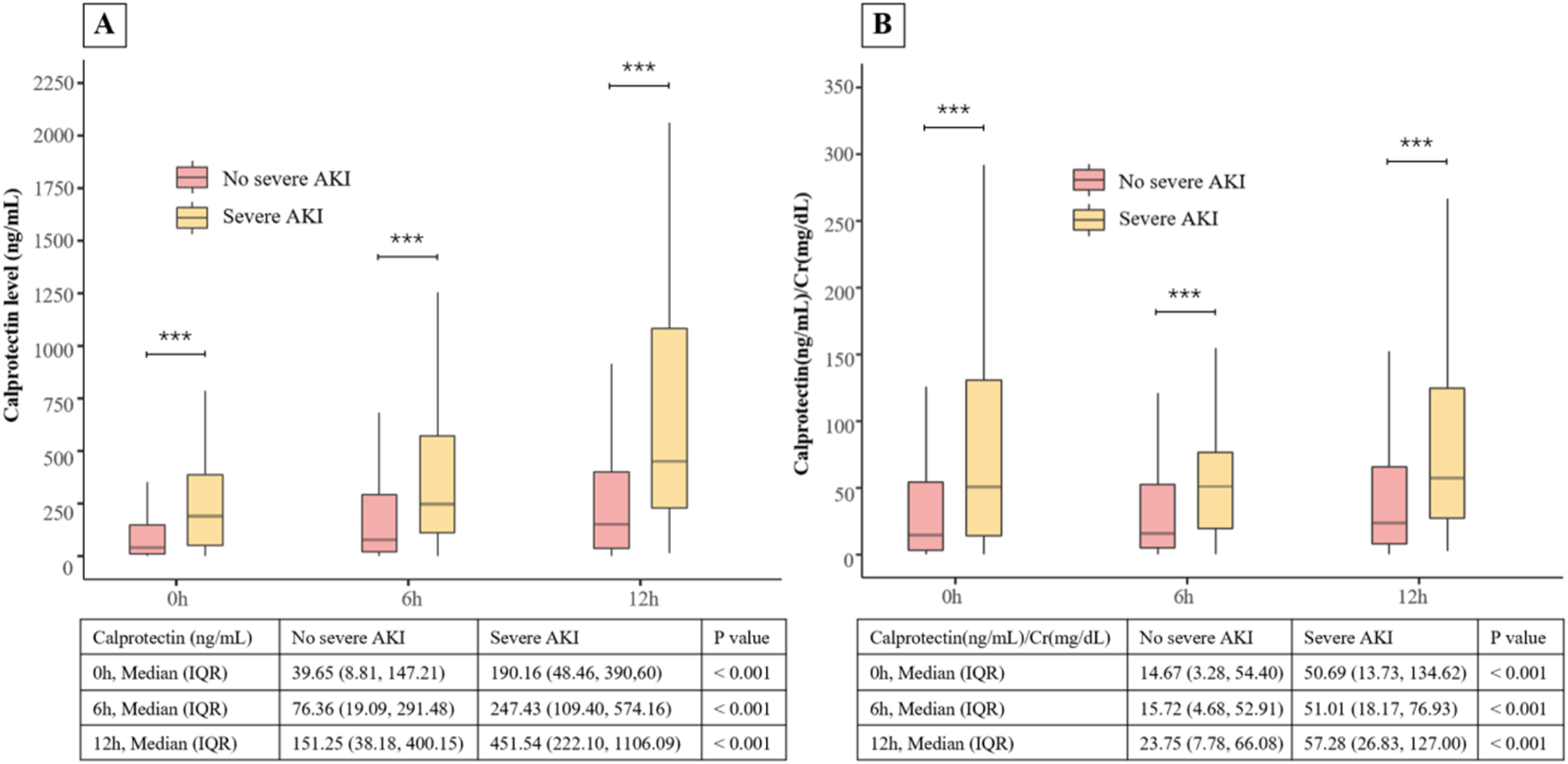
The AUC of urinary calprotectin at SICU admission (0 h) to predict severe AKI was 0.701 (95% CI, 0.649 to 0.754), and urinary calprotectin at 0 h ≥ 32.3 (ng/ml) was associated with an increased risk of severe AKI (OR 6.119, 95% CI 3.259-11.488). Meanwhile, the AUC was 0.684 (95% CI, 0.628 to 0.741) for urinary calprotectin/Cr ratio at 0 h, and urinary calprotectin/Cr at 0 h ≥ 28.6 (ng/ml)/(mg/dl) was also associated with an increased risk of severe AKI (OR 3.941, 95% CI 2.468-6.292).
The Ability of the Urinary Calprotectin With the Clinical Model to Predict Severe AKI
Univariate and Multivariable Logistic Analysis of Factors With Severe AKI in Clinical Model

AKI, acute kidney injury; BMI, body mass index; eGFR, estimated glomerular filtration rate; Hb, hemoglobin; Alb, Albumin; BNP, B type natriuretic peptide; ACEI/ARB, angiotensin converting enzyme inhibitors/angiotensin receptor blocker; APACHE, acute physiology and chronic health evaluation; OR, odds ratio.
The addition of urinary calprotectin or the calprotectin/Cr ratio measured at SICU admission to the clinical model significantly improved the AUC by 0.037 (from 0.693 to 0.730; 95% CI, 0.677–0.784) and by 0.063 (from 0.693 to 0.756; 95% CI, 0.697–0.815), respectively. At the optimal risk thresholds of 17.2% and 19.2%, the models achieved sensitivities of 78.6% and 69.4%, and specificities of 62.4% and 76.4%, respectively (Figure 3). The urinary calprotectin at 0 h ≥ 32.3 (ng/ml) (adjusted OR [aOR], 4.943; 95% CI, 2.590-9.434) and calprotectin/Cr ratio at 0 h ≥ 28.6 (ng/ml)/(mg/dl) (aOR, 3.468; 95% CI, 2.133-5.638) remained independently associated with a higher risk of severe AKI Receiver operating characteristic (ROC) curve of urinary calprotectin for severe AKI in patients after non-cardiac surgery
Using the prespecified risk categories (<3%, 3–10%, >10%) adapted from previous studies, adding urinary calprotectin also significantly improved the reclassification for severe AKI with categorical NRI of 0.337 (95% CI, 0.111% to 0.427%; P<0.001) and IDI of 0.055 (95% CI, 0.036 to 0.073; P < 0.001). Similar findings were observed when adding urinary calprotectin/Cr with categorical NRI of 0.197 (95% CI, 0.019 to 0.363; P = 0.024) and IDI of 0.059 (95% CI, 0.037 to 0.081; P < 0.001). The DCA was performed (Figures S3–S4), demonstrating that the models incorporating urinary calprotectin or the calprotectin/Cr ratio at 0 hours provide a higher net benefit compared to the clinical model alone, across risk threshold probability ranges of 3%–35% and 7%–42%, respectively. Two sensitivity analyses were conducted to evaluate the impact of different variable screening strategies on the clinical model. The results of these sensitivity analyses were consistent with those of the main analysis
Subgroup Analyses
The effect of the interaction between urinary calprotectin at SICU admission and pyuria or macroscopic hematuria was examined for severe AKI, and the interactive effect was significant (P for interaction = 0.009). Therefore, a subgroup analysis was performed in patients without pyuria and macroscopic hematuria to evaluate the predictive ability of urinary calprotectin for severe AKI. Among the 438 patients without pyuria or macroscopic hematuria, 158 developed AKI within 7 days after surgery, and 71 experienced severe AKI (16.2%). The AUC to predict severe AKI was 0.729 (95%CI, 0.670 to 0.791) for urinary calprotectin, 0.696 (95%CI 0.628 to 0.763) for urinary calprotectin/Cr, and 0.693 (95%CI, 0.626 to 0.761) for the clinical model. Adding urinary calprotectin to the clinical model improved the AUC from 0.693 to 0.832, with NRI of 0.413 (95% CI, 0.126 to 0.537; P < 0.001) and IDI of 0.082 (95% CI, 0.056 to 0.107 P < 0.001). Moreover, adding urinary calprotectin/Cr to the clinical model also improved the AUC from 0.696 to 0.818, with NRI of 0.176 (95% CI, 0.005 to 0.420; P = 0.098) and IDI of 0.086 (95% CI, 0.052 to 0.119; P < 0.001).
Discussion
This study provides the first evaluation of urinary calprotectin for predicting severe AKI in non-cardiac surgerical patients. We found that urinary calprotectin alone showed moderate predictive performance (AUC of 0.701), but its combination with a clinical model significantly enhanced predictive performance, improving the AUC from 0.693 to 0.730. The NRI indicates that 33.7% of patients were correctly reclassified, and the IDI reflects a modest but significant improvement in discriminative ability. The integrate model shows good calibration, higher net benefit and robustness in internal validation. Notably, urinary calprotectin demonstrated superior predictive capability in patients without pyuria or macroscopic hematuria, substantially increasing the AUC from 0.693 to 0.832, with an NRI of 0.413 and an IDI of 0.082.
The search for predictive biomarkers for AKI following non-cardiac surgery remains an area of active investigation. Compared with the more established evidence in cardiac surgery, 31 validated biomarkers for this specific population are lacking. To date, only a limited number of studies have evaluated promising candidates with varying reported performance—for instance, an AUC of 0.85 for urinary TIMP-2•IGFBP7 in one cohort, 32 and 0.74 for plasma NGAL in another. 8 This scarcity of consistent evidence underscores the need to explore novel biomarkers with a strong pathophysiological rational.
Our findings introduce urinary calprotectin as one such candidate. Mechanistically, as a damage-associated molecular pattern (DAMP) protein released early by innate immune cells and injured renal tubules, it engages TLR4 and RAGE to trigger oxidative stress and inflammatory cytokine production- a central pathway in AKI.33,34 Beyond its established role for predicting disease activity in other inflammatory conditions such as rheumatoid arthritis, 35 inflammatory bowel disease, 36 and COVID-19, 37 calprotectin has been specifically implicated in AKI. Fujiu et al. first demonstrated the involvement of calprotectin in AKI in a unilateral ureteral obstruction mouse model. 38 Our prior work established that calprotectinhigh macrophages infiltrated the kidney within hours of ischemic insult, and that urinary levels correlated with histological damage and clinical AKI severity.22,23 This provides a direct biological basis for its predictive capacity, positioning it as an indicator of the incipient inflammatory cascade that precedes significant functional decline.
Given the heterogeneity of severe AKI, a single biomarker is unlikely to capture all clinical characteristics. Even promising biomarker panels, TIMP2*IGFBP7, have shown only displayed modest predictive ability (a pooled AUC of 0.74) for severe AKI in cardiac surgical patients. 39 Consequently, integrating novel biomarkers with readily available clinical variables has emerged to improve risk stratification and early detection.40,41 In line with this approach, we previously developed a practical clinical model using four routine variables. The addition of urinary calprotectin significantly enhanced the predictive performance of this model (AUC 0.730. Nevertheless, given its modest sensitivity and specificity, its clinical utility is primarily for risk stratification—for example, helping to identify patients who might benefit from closer monitoring or preventive measures upon SICU admission. In contrast, notably, our exploratory subgroup analysis revealed a substantially higher AUC of 0.832 among patients without pyuria or macroscopic hematuria, suggesting greater clinical utility in this specific population and highlighting the complementary value of combining urinary calprotectin with clinical data. To clarify the practical timing of this risk stratification approach, our clinical model incorporates the 24-hour APACHE II score, which is assessed within the first 24 hours of SICU admission. As such, it represents an early postoperative risk stratification window rather than a prediction strictly at admission—a reflection of real-world clinical assessment. Importantly, our sensitivity analysis using only admission-day variables confirmed that urinary calprotectin retains its utility for very early risk assessment upon SICU entry.
Our study has several notable strengths. To our knowledge, this is the first prospective evaluation of urinary calprotectin specifically for predicting severe AKI in non-cardiac surgical patients, addressing a clear evidence gap. The work is grounded in prior mechanistic research from our group. Methodologically, we implemented rigorous quality control for biomarker assays and conducted performed internal validation using bootstrap resampling. We further assessed the biomarker both independently and in combination with a practical clinical model, and examined its performance in key clinical subgroups, offering a comprehensive and clinically relevant assessment.
Our study has several limitations. First, as a single-center investigation focused on SICU patients, the generalizability of our findings may be limited. Second, the low mortality rate and short follow-up period precluded evaluation of calprotectin’s ability to predict patient survival or long-term kidney recovery. Third, the subgroup without pyuria or macroscopic hematuria had limited sample size, few event, and potential selection bias; these findings are hypothesis-generating and require external validation. Fourth, because SCr was measured only once daily in routine practice, the onset of AKI may have been recognized later than its true occurrence, potentially exaggerating the apparent lead-time advantage of early urinary calprotectin testing. Fifth, as a nonspecific marker of inflammation, urinary calprotectin levels can be elevated in systemic conditions, which may affect its specificity for predicting AKI. Sixth, although stepwise regression was pragmatic given our sample size, this approach carries a risk of overfitting. Finally, the proposed cutoff values for urinary calprotectin should be considered exploratory at this stage and require external validation before clinical implementation.
Conclusions
In this cohort of non-cardiac surgical patients, urinary calprotectin demonstrated modest stand-alone ability for predicting severe AKI. Its predictive performance was meaningfully enhanced when integrated with readily available clinical variables, particularly among patients without pyuria and macroscopic hematuria. Our findings support the potential role of urinary calprotectin, as part of a combined risk-assessment strategy, in helping clinicians identify high-risk surgical patients who may benefit from early preventive measures.
Supplemental Material
Supplemental Material - Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study
Supplemental Material for Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study by Weijian Yao, Lingyi Xu, Nan Li, Jinwei Wang, Qingqing Zhou, Linger Tang, Xizi Zheng, Shuangling Li, Li Yang in Biomarker Insights
Supplemental Material
Supplemental Material - Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study
Supplemental Material for Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study by Weijian Yao, Lingyi Xu, Nan Li, Jinwei Wang, Qingqing Zhou, Linger Tang, Xizi Zheng, Shuangling Li, Li Yang in Biomarker Insights
Supplemental Material
Supplemental Material - Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study
Supplemental Material for Urinary Calprotectin Predicts Severe Acute Kidney Injury After Non-cardiac Surgery in Surgical Intensive Care Unit: A Prospective Cohort Study by Weijian Yao, Lingyi Xu, Nan Li, Jinwei Wang, Qingqing Zhou, Linger Tang, Xizi Zheng, Shuangling Li, Li Yang in Biomarker Insights
Footnotes
Acknowledgements
We thank the authors of all included studies cited in this study.
Ethical Considerations
Ethical approval (2019-075) was granted by the Clinical Research Ethics Committee of Peking University First Hospital.
Consent to Participate
written informed consent was obtained from all participants.
Authors’ Contributions
Li Yang, Shuangling Li and Xizi Zheng came up with the study concept; Weijian Yao, Lingyi Xu and Xizi Zheng developed the study design and protocol; Lingyi Xu, Weijian Yao and Nan Li collected the study data; Lingyi Xu, Jinwei Wang, Weijian Yao, Qingqing Zhou and Linger Tang were involved in the analysis and interpretation of the data. Li Yang, Shuangling Li and Xizi Zheng provided input and a critical review of the manuscript leading to the final version. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: National Natural Science Foundation of China (82130021, 82300759, 82300764); Beijing Nova Program (2021051); the Fundamental Research Funds for the Central Universities, Peking University Clinical Scientist Training Program (BMU2023PYJH023); the Capital’s Funds for Health Improvement and Research (CFH2022-1-4071); the Beijing Young Scientist Program (BJJWZYJH01201910001006); Clinical Medicine Plus X - Young Scholars Project, Peking University, the Fundamental Research Funds for the Central Universities (PKU2023LCXQ002); National High Level Hospital Clinical Research Funding, Interdisciplinary Research Project of Peking University First Hospital(2023IR14, 2022CR83); Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-046); the Fundamental Research Funds for the Central Universities, Peking University Medicine Sailing Program for Young Scholars’ Scientific & Technological Innovation (BMU2024YFJHMX003), Young Elite Scientists Sponsorship Program of the Beijing High Innovation Plan (20250908).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Data and Code Sharing
Due to the private and sensitive nature of the data, we are unable to publicly share the dataset or the full analysis code. However, we can provide a detailed description of the data-processing and analysis workflow upon reasonable request to support transparency and reproducibility.
AI Tool Declaration
We confirm that no scientific data was generated or modified using AI. An AI language model (ChatGPT by OpenAI) was used exclusively for polishing the English language and grammar in the revised manuscript’s text. The scientific content, data, analysis, and conclusions remain entirely our own.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.