
Abstract
The activity of Na+-K+ ATPase is altered in sickle cell disease (SCD), which affects serum electrolyte levels. This alteration is associated with several complications in sickle cell patients. This study evaluated the serum levels of sodium, potassium, and chloride in patients with SCD. The study was a case-control cross-sectional study involving 120 SCD patients in the steady state and 48 ‘healthy’ controls. The SCD patients were made up of 69 HbSS patients and 41 HbSC patients. Serum electrolyte levels (Na+, K+, and Cl−) were measured using a Flame Atomic Absorption Spectrometer (Variant 240FS; Varian Australia Pty Ltd). Serum sodium levels were significantly lower in the sickle cell patients, compared with their ‘healthy’ counterparts (P = .0001). Although the study found significantly higher serum levels of potassium in the SCD patients (P = .0001), there was no significant difference in serum chloride levels between patients with SCD and the controls (P = .098). Serum sodium and chloride levels were not significantly different in both HbSS and HbSC patients (P = .197 and P = .553, respectively). The level of serum potassium in the HbSS patients was, however, significantly higher compared with those with the HbSC genotype (P = .0001). There is higher efflux of K+ from the intracellular into the extracellular space in HbSS patients, which may lead to red cell membrane dysfunction and associated complications.
Introduction
Sickle cell disease (SCD) is a group of haemoglobinopathies characterized by the inheritance of two abnormal haemoglobin genes in which at least one is the Haemoglobin S gene. The synthesis of Haemoglobin S is a result of a point mutation in the beta-globin gene resulting in the substitution of glutamic acid for valine in the beta-globin protein. Homozygous form of the SCD, which is commonly termed as sickle cell anaemia, is a combination of two forms of the Haemoglobin S genes, while a combination of another variant haemoglobin gene (HbC) with the Haemoglobin S gives the heterozygous form. About 20 million people are affected by the disease worldwide, with a high prevalence, especially of the homozygous form, living in Africa. 1
Sickling, which is associated with Haemoglobin S and erythrocyte haemolysis, affects the overall electrolyte balance in sickle cell patients and may lead to increased cell dehydration.2,3 Electrolytes such as sodium (Na+), potassium (K+), and chloride (Cl−) play various vital roles in the body and are required for optimal functioning of cells and organs. Sodium is one of the major cations and functions in regulating the total amount of water in the body. It also plays a vital role in electrical communication in many systems especially the nervous and muscular systems. However, potassium is responsible for regulating heartbeat and muscle function and is important for the overall functioning of the cell. Chloride helps maintain a normal balance of body fluids. Alteration of these electrolytes could, thus, lead to detrimental effects.
In SCD, commonly encountered events, such as intravenous potassium administration and blood transfusion, can lead to increased serum potassium level and can also affect the levels of other electrolytes.4,5 This may consequently put SCD patients at risk of experiencing fatal outcomes including episodes of vaso-occlusion.
Abnormal activation of the potassium chloride (K+-Cl−) co-transport system and the Gardos channel has been proposed to be involved in intra-erythrocytic shift of potassium. 6 In most cases, the deoxygenation of sickle cell promotes cation permeability of electrolytes including potassium and calcium. 3 These processes may consequently lead to increased cell dehydration in the sickle cell patients, with aggravated clinical complications. Previous studies have been conducted mainly to determine the levels of electrolytes in patients with sickle cell anaemia (HbSS),7-10 as well as other sickle cell genotypes other than HbSC. 11 In Ghana, no single study has been done to determine and to compare the relative levels of electrolytes in patients with HbSS and HbSC genotypes. In most cases, clinical characteristics are inferred from studies involving only HbSS. Meanwhile, the clinical presentations of these two genotypes (HbSS and HbSC) have been shown to be different, 12 with the latter being less severe. In this study, serum levels of some major electrolytes were determined in sickle cell patients (HbSS and HbSC genotypes) and compared with ‘healthy’ controls in Ghana.
Methods
Study site
The study was conducted at the Korle-Bu Teaching Hospital (KBTH) in the Greater Accra Region of Ghana. The hospital is a 2000-bed facility and the leading tertiary facility in the country. The sickle cell unit, wherein this study was carried out, forms part of the departments of the facility. The controls were recruited from the Accra Southern Area Blood Centre, Korle-Bu. These were voluntary blood donors who consented to partake in the study. The haemoglobin electrophoresis was used to confirm the absence of sickle cell trait in all the control group.
Study design, subject recruitment, and data collection
This was a cross-sectional study, involving 120 sickle cell patients (in the steady state) with HbSS and HbSC genotypes, and 48 HbAA ‘healthy’ individuals as controls. Steady state was defined as a period where patients are not in crisis for at least 1 month. The patients were recruited from the sickle cell unit of the KBTH from the period of May 2018 to August 2018. Patients with comorbidities such as coronary artery disease, diabetes mellitus, hypertension, renal failure, pregnancy, and recent blood transfusion (3 months prior to the study) were not included in the study. The genotype of the study participants (HbSS, HbSC, and HbAA) was determined using haemoglobin electrophoresis. A volume of 5 mL of venous blood sample was collected from each of the study participants into plain test tubes for serum sodium, potassium, and chloride analysis.
Laboratory analysis
The blood samples in the tubes were spun in a centrifuge at 2500 r/min for 10 minutes. The sera were kept in Eppendorf tubes at −20°C before analyses. Full blood count was determined using Labsystems Multiskan MS (Amersham Biosciences Ltd, Chalfont, UK) within 2 hours of sample collection. Sodium, potassium, and chloride levels were quantified using a Flame Atomic Absorption Spectrometer (Variant 240FS; Varian Australia Pty Ltd, VIC, Australia) described by Meret and Henkin. 13
Data analyses
Microsoft Excel 2010 was used for data entry, and analysis was done using SPSS version 20. Mean ± standard deviation and frequencies were used to represent nominal data (the age of the study participants and the number of participants with regard to sex, respectively). The analysis of variance (ANOVA) was used to compare the mean values between the study participants, followed by the Tukey post hoc analyses, and P-values less than .05 were considered significant.
Ethical statement
Ethical approval for the study was sought from the Ethical and Protocol Review Committee of the College of Health Sciences, University of Ghana, with protocol identification number: CHS-Et/M.8-P2.13/2017-2018. The consent of participants was sought before questionnaire was administered and blood samples were taken.
Results
Demographical and clinical characteristics of the study participants
A total of 168 participants were recruited into the current study, involving 120 SCD patients with HbSS and HbSC genotypes and 48 ‘healthy’ controls (HbAA). The mean age of SCD patients and the ‘healthy’ controls was 27.66 ± 10.57 years and 31.67 ± 9.48 years, respectively.
The gender difference among the study participants was not significant (P = .440). The general demographic characteristics of the study participants are presented in Table 1.
Demographic characteristics of the study participants.

P < .05 is significant.
The mean age of the HbSS and HbSC patients was not significantly different (P = .382). The ratio of the HbSS patients to the HbSC patients was 1:1. The demographic features of the HbSS and HbSC SCD patients are presented in Table 2.
Demographic features of HbSS and HbSC patients.

P < .05 is significant.
Level of haemoglobin and serum electrolytes in SCD patients and the controls
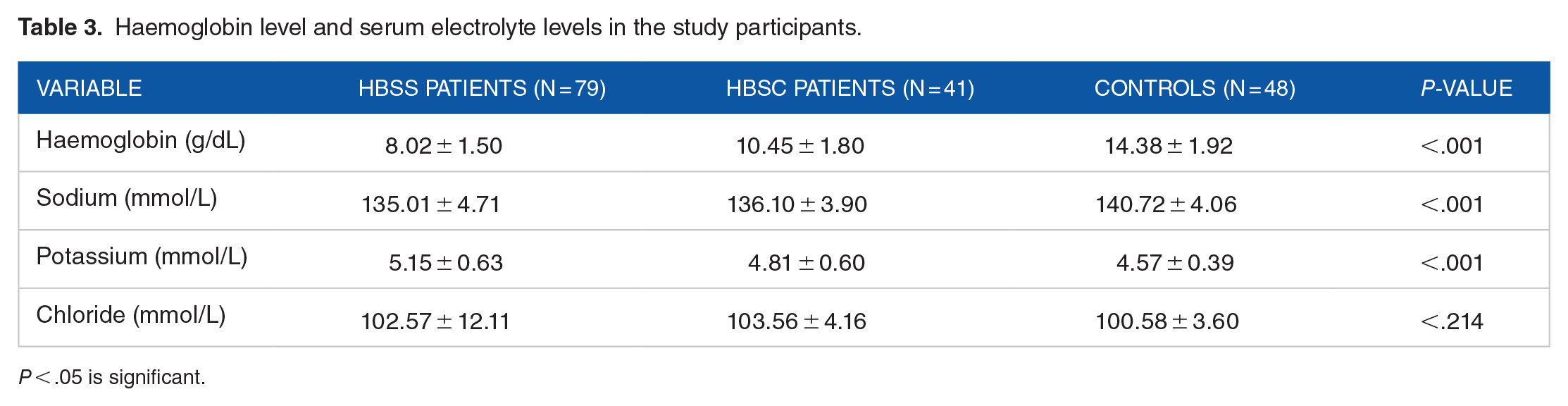
It was observed that, levels of haemoglobin were significantly lower in the sickle cell patients, especially those with the HbSS genotype (P < .001). The mean serum level of sodium was significantly lower in the SCD patients compared with the HbAA ‘healthy’ controls (P < .001). There was no significant difference in the levels of sodium between HbSS and HbSC sickle cell patients (P = .400). However, potassium level was observed to be significantly higher in the SCD patients (P < .001). Although potassium levels were significantly higher in the HbSS patients, compared with the HbSC patients (P = .006), there was no significant difference in the levels of potassium between HbSC and HbAA patients (P = .082). Meanwhile, potassium levels were significantly higher in HbSS patients, compared with the controls (P < .001). The mean serum level of chloride between the SCD patients and the controls was not significant (P = .098). There was no significant difference in chloride levels between HbSS and HbSC patients (P = .824), HbSS and HbAA patients (P = .386), as well as HbSC and HbAA patients (P = .220). Serum electrolyte levels and levels of haemoglobin in the study participants are shown in Table 3.
Haemoglobin level and serum electrolyte levels in the study participants.
P < .05 is significant.
Discussion
The result from this current study highlights the potential use of electrolyte levels as biomarkers of SCD. Imbalance homeostasis of electrolytes including sodium, potassium, and chloride has been described in relation with sickling and increased dehydration in sickle cell patients outside Ghana,7,8,11 with very few studies in Africa.9,10 The sodium-potassium ATPase activity has been shown to be more active in sickle cell and contributes to cell dehydration. 14 This may consequently lead to frequent crises and associated painful episodes due to vaso-occlusion of the sickle erythrocytes, as observed in sickle cell patients. This is mainly as a result of the sustained and rapid polymerization of the Haemoglobin S molecule, where intracellular concentrations (of the HbS molecules) are increased in sickle cell patients.15,16 Prevention of cell dehydration is, thus, important, as it can help reduce the painful crises associated with SCD, 17 as well as aid in the management of the disease.
The serum level of sodium was significantly lower in the SCD patients, compared with the controls. This is in line with other studies7-11 conducted elsewhere, which reported low serum levels of sodium in the sickle cell patients, compared with their ‘healthy’ counterparts. The reduced serum level of sodium in the SCD patients may be due to at least, in part, a possible loss of some body fluids and electrolytes, as well as inflammation and the underlying chronic condition. 18 Although serum sodium levels were significantly higher in the control group, no significant difference was observed between HbSS patients and those with the HbSC genotype. The reduced serum sodium levels in the HbSS patients, compared with the HbSC patients (although not significantly different), partially agree with Aluoch. 19 It seems likely from the current study and the work of Aluoch 19 that, alteration of serum sodium levels in HbSS patients is similar to those with HbSC genotype.
Potassium alteration in sickle erythrocytes is also associated with cell dehydration and sickling. 17 The significantly higher levels of serum potassium in the sickle cell patients as compared with the controls agree with previous studies.10,11,20 Cell dehydration and hypoxia usually encountered by sickle cell patients might have caused the loss of potassium from the cell into the extracellular fluid,21,22 thus increasing the concentration of potassium in the serum. Consequently, blood flow will be slower than normal, as a result of the dehydrated sickled erythrocytes, leading to vaso-occlusion in most cases. Consequently, there may be ischaemia reperfusion as well as inflammation in such patients when blood flow is restored, 23 which may further intensify the clinical presentations. Even though the current study reports no significant difference in serum levels of sodium between HbSS and HbSC patients, it appears that, potassium levels are higher in HbSS patients. 19 Meanwhile, the Gardos channel implicated in the efflux of potassium has been shown to be very active in HbSS compared with HbSC. 12
In sickle cell, chloride and water movement from the intracellular fluid is observed when calcium is increased in the red cells.24,25 In a previous study, a rise in the erythrocyte concentration of calcium levels (although not reported in the current study) in the sickle cell patients contributed to higher efflux of potassium accompanied by chloride. This is as a result of the abnormal activation of the Gardos channel and the K-Cl co-transport (which is increased in HbSC) and, thus, may lead to cell dehydration. 25 Thus, erythrocyte calcium levels may play a role in chloride homeostasis. 26 In this study, serum chloride level was higher in the sickle cell patients, although not significantly higher than the controls. Howbeit, significant changes in chloride levels in sickle erythrocytes may influence cell dehydration and provoke certain clinical presentations of SCD. It is worth mentioning that, the results from this current study arise from patients in Ghana (sub-Saharan Africa). As such, the results may be different from sickle cell patients in other countries. The main limitation of the study was the small sample size as well as the inability to assess severity of the SCD. We could also not determine glucose levels, renal function, as well as treatment in the study participants. Further studies with all the confounding factors are needed to confirm findings from this current study.
Conclusions
This study concludes that, unlike serum sodium levels, serum levels of potassium are significantly higher in sickle cell patients. Intra-erythrocytic shifts of potassium are pronounced in HbSS patients, compared with HbSC patients. The associated clinical complications may include increased intravenous haemolysis, as a result of augmented cell dehydration and rapid auto-polymerization of the Haemoglobin S. Thus, blockade of potassium loss from sickle erythrocytes would reduce sickling, for better clinical outcomes in sickle cell patients. Lower serum sodium levels are generally linked with SCD.
Footnotes
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
CA-B conceived the idea, designed the study, and revised the drafted manuscript; YAK-M did clinical characterization, recruited the patients, and collected data; RA drafted the first manuscript; ES-D, EO-D, and CH-B supervised the collection of data and revised the drafted manuscript; GBD, RA, and FAB collected data and did the major laboratory analysis; and KLA entered data and interpreted the data collected. All authors read and approved the final version of the manuscript.
Data Availability
The data are stored electronically with all the results from the analysis and available from the corresponding author upon reasonable request.