
Abstract
Equity in pandemic planning and response for First Nations peoples in Australia requires a deeper understanding of sociocultural realities to determine appropriate public health actions. First Nations community panels were held in three locations across Australia between September 2020 to December 2020 to make decisions on how government authorities should help First Nations peoples keep safe from COVID-19. Twenty-two First Nations peoples participated in online panels. Panels heard from public health experts, examined the evidence and deliberated on the issues. All panels highlighted that embedding First Nations worldviews into health policy was important. First Nations peoples must be supported and resourced to enable self-determination in preparation for future infectious disease emergencies, otherwise their health could be negatively impacted if they are not intentionally considered or actively engaged.
Introduction
The coronavirus pandemic (COVID-19) inequitably impacted the lives of many Aboriginal and Torres Strait Islander peoples of the lands now called Australia (respectfully hereafter First Nations). First Nations peoples globally and in Australia experience health inequities and disadvantages due to ongoing colonisation, systemic and structural racism (Mashford-Pringle et al., 2021; Paradies, 2016), culturally unsafe health services (Durey & Thompson, 2012), higher rates of chronic conditions (Australian Institute of Health and Welfare, 2011), and reduced access to appropriate and timely health care (Nolan-Isles et al., 2021).
Public health measures to prevent spread of infectious diseases in response to a disease threat, like physical distancing and quarantine, often fail to account for the lived experiences of First Nations peoples. This failure to account for lived experiences reflects an inappropriate one-size-fits-all approach, that reinforces ongoing colonisation and does not include culturally appropriate and targeted strategies (Miller & Durrheim, 2010). The pandemic exposed gaps in implementing public health actions to mitigate against infectious disease transmission with First Nations communities and also highlights the importance of understanding community preferences, needs and priorities (Crooks et al., 2022; Fredericks et al., 2024; Health Protection NSW, 2019).
First Nations worldviews are intrinsically linked to the interconnectedness of people, experiences, environment, culture and spirituality (Sherwood, 2010). Knowledge is transferred through storytelling and yarning, focusing on collective health and well-being of individuals, families and communities (Verbunt et al., 2021). These worldviews often contrast with dominant ideologies, which are more individualistic and biomedical (Terare & Rawsthorne, 2020). Recognising these differences are important for designing and implementing culturally relatable and appropriate and equitable public health strategies for First Nations peoples, while privileging cultural knowledge and practices.
This study builds on deliberative democratic methods and Indigenist methodologies (Bessarab & Ng’Andu, 2010; Miller et al., 2015; Street et al., 2014). Deliberative approaches, like citizen juries, emphasise participatory decision-making, emphasise diverse perspectives to address complex public health problems (Degeling et al., 2017), while Indigenist methodologies prioritise self-determination, relationality, and collective decision-making (Smith, 2021). This model enables First Nations peoples to critically examine evidence, engage in challenging discussions, and recommend culturally relevant public health strategies (Crooks et al., 2022).
This study aimed to engage First Nations peoples to make decisions on how public health authorities and government departments should support First Nations families and communities during COVID-19. Although the questions for these panels focused on COVID-19, the principles, and arguments presented are applicable for other infectious disease emergencies.
Methods
Study setting
First Nations community panels were convened and framed from the deliberative decision-making citizen juries approach but informed and modified through First Nations knowledges and practices (Crooks et al., 2022; Degeling et al., 2021). Three separate and independent panels occurred, each located in a different Australian state: New South Wales (NSW), Western Australia (WA) and Queensland (QLD). The study sites were selected because of the contrast of the locations, including large regional towns and regional city, existing relationships and previous work on other projects (Crooks et al., 2023). Each panel met for a total of 16 hours over 4 weeks, consisting of eight 2-hr sessions. Panels were convened between September 2020 and December 2020 via Zoom due to travel restrictions during the COVID-19 pandemic.
Community panel recruitment and process
First Nations participants were purposively recruited through local community, cultural and professional networks specific to each region to ensure local voices and perspectives reflected their communities.
A five-step approach was used to engage First Nations peoples in deliberative decision-making which is described elsewhere (Crooks et al., 2022, 2023). Panels commenced with an introduction to the process, questions and expectations, and participant consent. Participants received an information booklet outlining the process and expert biographies. First Nations researchers designed the panel questions, in collaboration with non-First Nations public health experts.
Five experts, including First Nations and non-First Nations people, were invited to present balanced factual evidence supporting different perspectives on the topics. Experts included a public health physician, Indigenous Health academics, a paediatrician, and a social scientist. Expert presentations ran for 20mins to 30mins and were pre-recorded or presented live. After each presentation, the expert was available by videoconference for participants to ask questions or clarify the evidence. After each presentation and question and answer session, panel members participated in online activities to promote discussion and debate.
The presented evidence covered three topics: (1) COVID-19 actions to keep families safe, (2) COVID-19 and education settings, and (3) COVID-19 communication and governance (Figure 1).
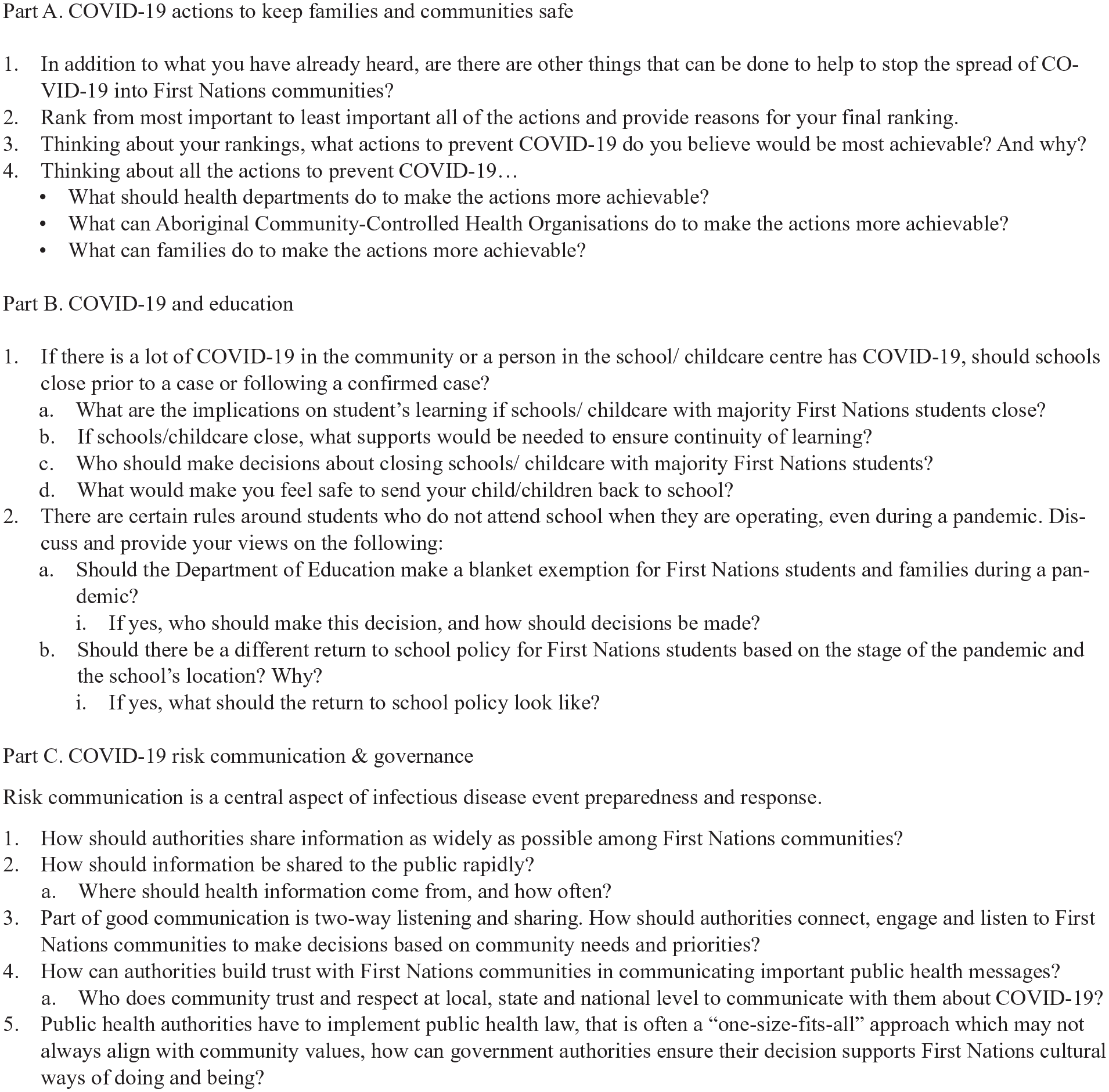
Questions for the First Nations community panels.
Data collection and analysis
After each session, participants received a Yarning with the Mob booklet to facilitate discussions with their families and households. Later in the week, participants reconvened for a 2-hr deliberation session. In the first hour, the panels reflected, discussed, and debated the evidence, aided by the researchers. In the second hour, participants deliberated without the researchers, to reach consensus and present their final decisions. Online surveys helped rank preferences, generate discussion and frame decisions with justifications. Follow-up sessions checked for changes in positions and sought feedback on the process. Sessions were audio recorded and transcribed. Researchers developed the final report in collaboration with participants. The findings presented reflect the panel discussions, which were analysed using content analysis approach to identify key issues and experiences, decisions and recommendations. The panels final decisions and justifications are the units of analysis for this study. Key learnings were shared with policy makers and included in national pandemic guidance.
This study was approved by Hunter New England Local Health District (2018/ETH00547); Far North Queensland HREC (HREC/2019/QCH/54524); Western Australia Country Health Service (RGS 3367); New South Wales Aboriginal Health and Medical Research Council (1543/19); Western Australian Aboriginal HREC (959); Charles Darwin University HREC (H19056); and Wuchopperen Health Service. Informed consent was obtained from each participant in the study.
Findings
We purposively recruited twenty-two First Nations peoples in three Australian locations, in QLD (n = 7), NSW (n = 7) and WA (n = 8). All panels included participants from varying age groups and male and female genders however, there were more female (n = 16) than male participants (n = 6; Table 1). All participants were members of the local community, some were Elders or leaders in their community and families, and some held professional positions in government and nongovernment health and nonhealth-related organisations.
First Nations community panel characteristics 2020.
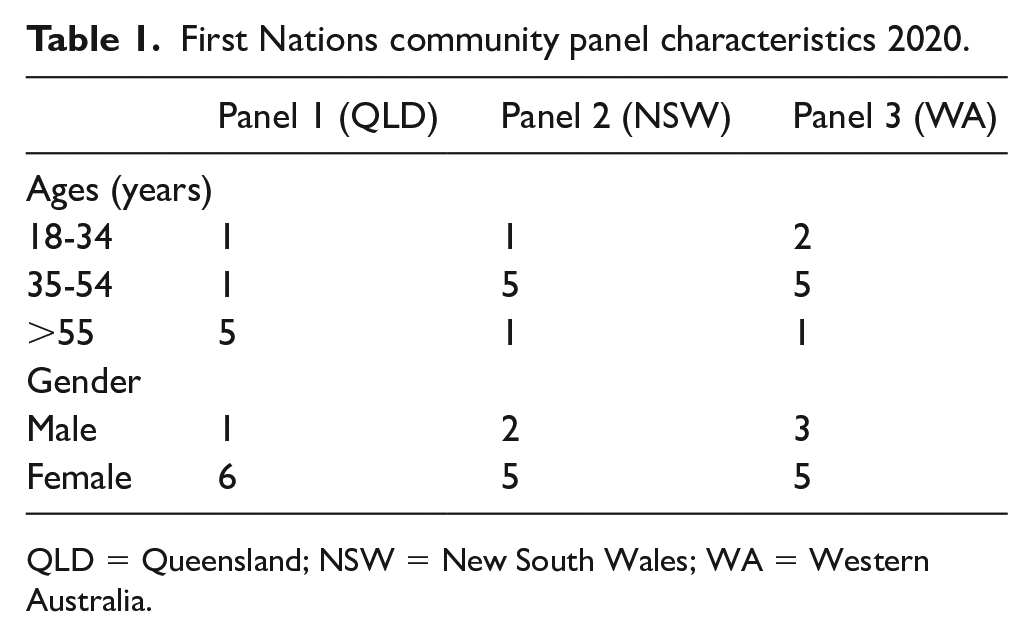
QLD = Queensland; NSW = New South Wales; WA = Western Australia.
Context
Participants shared experiences of systemic racism in the health system and government legislative practices, highlighting the power-imbalance between First Nations health system end users and policy makers:
We are still stuck in policies around assimilation . . . policies are [not] reflective enough, of the [First Nations] context or experience. There needs to be some exclusivity for Aboriginal people in recognition of our first nations status as the First Nations people of this world. (participant 1, female)
Community panel decisions and recommendations
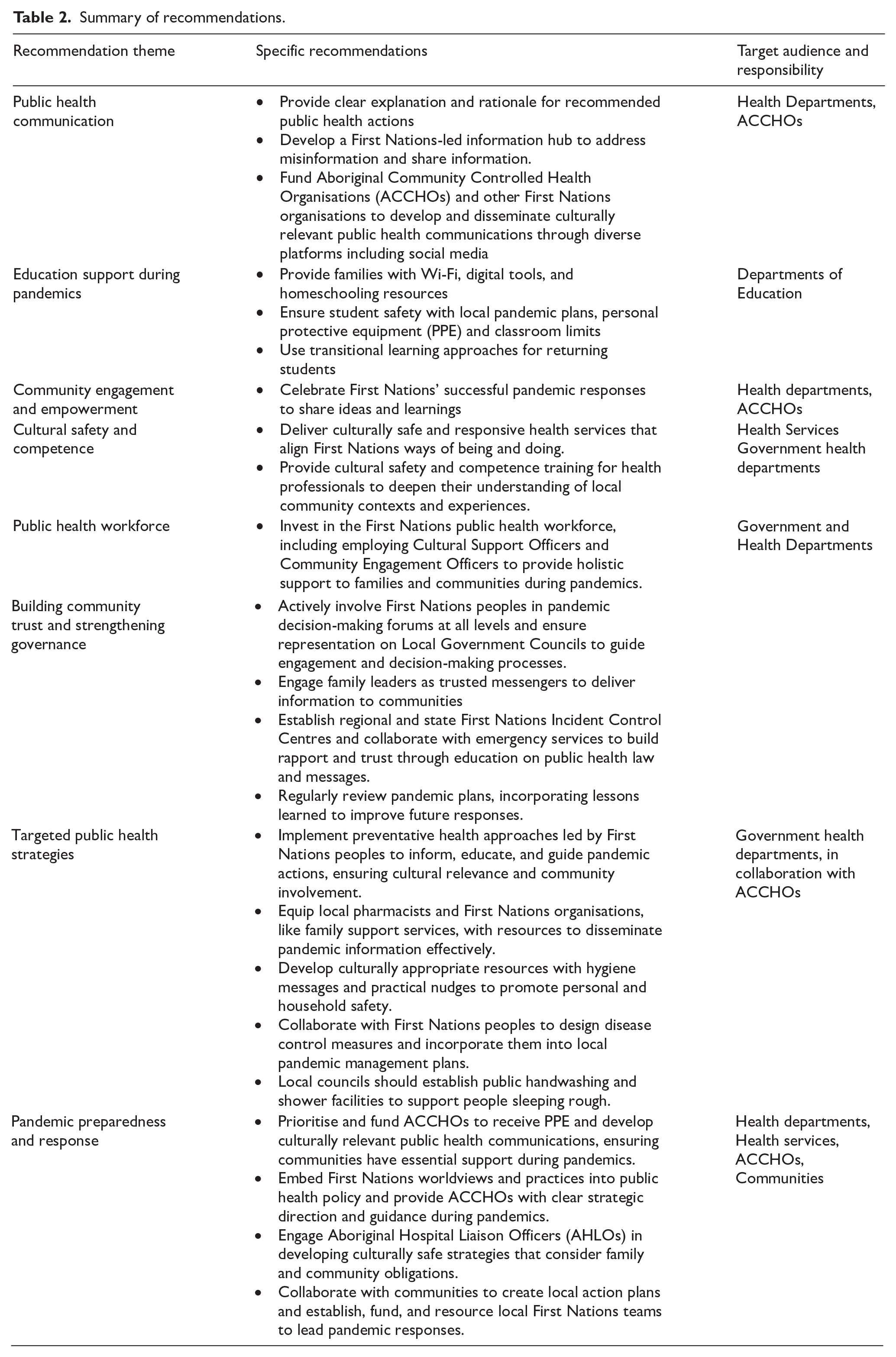
The combined panels’ strategies and recommendations reflect Indigenist, holistic and preventive perspectives focusing on community-controlled services, community development, and proactive approaches (Table 2). The findings are considered in three sections, with some overlap reflecting the holistic approach to the issues. Recommendations are synthesised from the three panels, highlighting shared priorities and panel specific perspectives.
Summary of recommendations.
Part A: COVID-19 actions to keep families and communities safe
The introduction to COVID-19 actions included a presentation on public health strategies to reduce COVID-19 transmission; physical distancing, wearing of face masks, enhanced hygiene and cleaning, limits on gatherings, protecting Elders, and community lockdowns. Discussions and deliberations centred on identifying important and achievable actions.
The panels identified several issues that made it difficult for communities to understand and follow public health actions. Barriers to understanding public health actions included limited English, and literacy which meant many people did not fully understand what they were being asked to do.
Challenges with hotel isolation emerged as the government provided hotel accommodation for COVID-19 cases and contacts to suppress transmission. Participants shared experiences of supporting First Nations people who were required to isolate away from their families, often where English was not their first language, and lacked understanding of hotel-isolation process:
There were assumptions in the hotel that Aboriginal people would know how to look after themselves in isolation. People didn’t understand the language, they didn’t understand the reasoning, all they knew they come out of community to go to the doctors . . . and should have gone home the next day. . . . Some people came out with one piece of clothing, because the remote communities weren’t armed with enough information about what to tell their people. (participant 1, female)
Confusion about public health messages arose as communities were confused about the reasons for compliance with certain public health actions due to inadequate explanations of reasons from authorities.
Access to hygiene supplies and facilities like running water and soap were limited particularly for many remote First Nations communities, creating barriers to adhere with public health advice.
Challenges with physical distancing and limits on gatherings was difficult for some communities to understand and implement, with some using role-playing to demonstrate what physical distancing meant.
Systemic failures including lack of coordinated leadership and involvement in the pandemic, with one participant stating; “all the systems are against [First Nations people] . . . [because] there was no direction from the top” (participant 1, female). The extra challenges and burdens of cultural obligations during the pandemic was left for First Nations people to manage, with no additional resources and support. The pandemic response “brought about a bit of systemic racism too” (participant 4, female) and “because it’s such a racist place, how do we get our [non-Indigenous] community to help us with our mob?” (participant 3, female).
Lack of support for Aboriginal Community Controlled Health Organisations (ACCHOs) left many under-resourced, which participants noted led to decreased services to local communities.
Following the evidence and discussions, the panels were asked to make decisions and recommendations to guide future pandemic responses.
Decision 1, which involved ranking actions from most important to least important, highlighted that all three panels ranked information, education and health promotion as the most important action to reduce COVID-19 transmission in First Nations communities (Table 3). The panels agreed that equipping individuals with knowledge about reasons for public health actions was essential to build trust and reduce confusion. This reflected the need for transparent communication with communities to address the change in public health information and could alleviate fear and concerns. While protecting Elders, physical distancing and community lockdowns were also important, their rankings varied based on local experiences and needs. There were other shared priorities, with some variations in the rankings:
COVID-19 actions from most important to least important.
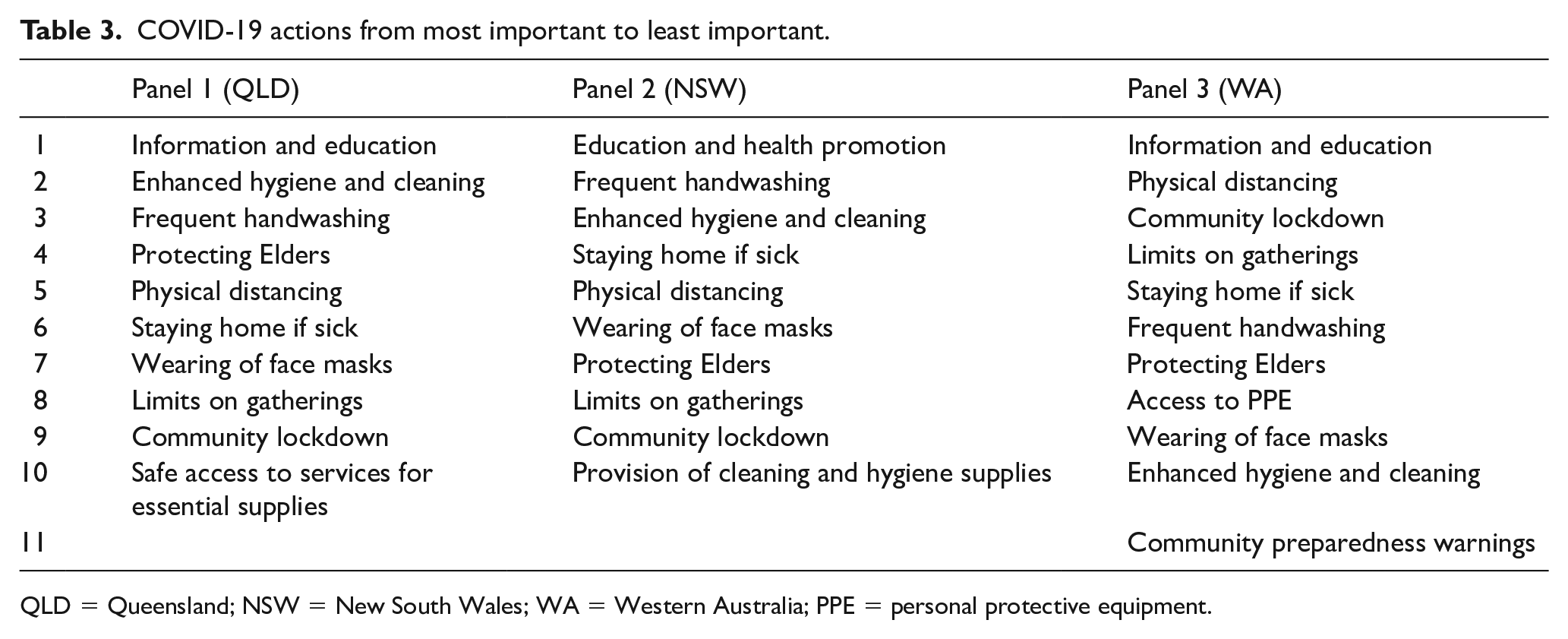
QLD = Queensland; NSW = New South Wales; WA = Western Australia; PPE = personal protective equipment.
Enhanced hygiene and cleaning, which included provision of hygiene resources and improving public facilities
Frequent handwashing, emphasising the importance of access to water and soap, especially in remote communities.
Decision 2 involved ranking the most achievable actions. Similarly, the panels ranked information, education and health promotion as the most achievable action. The justification aligned with the rationale for Decision 1; practical and actionable strategies, empowering First Nations families with the knowledge needed to stay safe, and on the importance of provision of reliable and relatable and easy to understand information (Table 4).
COVID-19 actions from most achievable to least achievable.
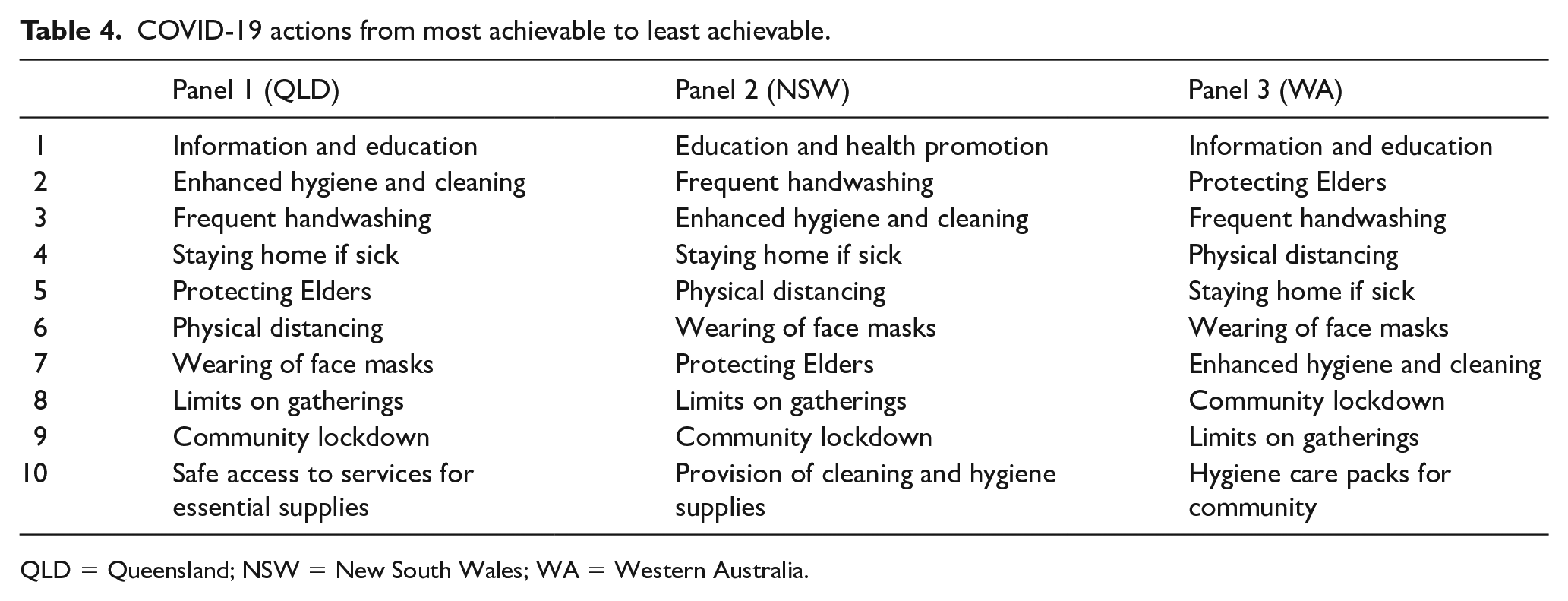
QLD = Queensland; NSW = New South Wales; WA = Western Australia.
Specific priorities identified by the panels included:
Frequent handwashing and enhanced hygiene: Panel 1 (QLD) and 3 (WA) ranked frequent handwashing among the top three achievable actions.
Protecting Elders: Panel 3 (WA) emphasised cultural obligations and duty, and highlighted local measures like support with smartphones, limiting visitors and taking them out bush to shield them from disease.
Based on the discussions and decisions, the panels made the following recommendations to strengthen pandemic responses for First Nations communities:
Public health communication should include clear explanations and rationale behind recommended actions, focusing the how and why to promote greater understanding.
Embed First Nations worldviews and practices into public health policy.
Implement preventive models for pandemic preparedness and response, adapting past and current health programmes designed to educate communities about the nature of pandemics, how viruses spread and mitigation measures.
Provide hygiene care packs to communities that have limited support.
Local councils provide public handwashing and shower facilities for people sleeping rough.
Establish collective advocacy mechanisms disseminated through reliable community organisations.
Decision 3 focused on identifying actions that would make COVID-19 prevention more achievable for First Nations communities.
The panels recommended that health departments and services:
Invest in First Nations public health workforce to facilitate community engagement and liaison between health departments during a pandemic.
Support ACCHOs to implement pandemic programmes effectively.
Develop public health policies, strategies and flexible services to local First Nations contexts and cultural knowledge and practices.
Employ Aboriginal Cultural Support Officers to provide holistic support during isolation.
Include Aboriginal Hospital Liaison Officers in the development of accommodation strategies for First Nations people during pandemics that considers cultural and family obligations.
For ACCHOs the recommended actions included:
Lead the care component for First Nations people in pandemic responses, and construct and distribute messages with a focus on developing information for young people.
Provide free pandemic hygiene resources and support for transport and accommodation.
Develop pandemic workforce plans to address staffing issues.
For families and communities panels suggested:
Develop community action plans to determine local priorities, protocols and procedures.
Family leaders and champions to share public health messages.
While they play a role, the panels did not want to put blame, shame or responsibility on families. They stressed that access to information is a basic human right, and health departments and ACCHOs are ultimately responsible to ensure families are provided with accurate, timely and culturally appropriate information.
Part B: COVID-19 and education settings
The panels examined the impact of COVID-19 transmission in schools and heard evidence on strategies to support First Nations students and families. Although evidence indicated children were not superspreaders, participants were fearful and concerned the virus could spread fast, emphasising the need to keep children safe. Deliberations included discussions on safety, learning impacts, and culturally appropriate solutions to maintain education and learning during the pandemic.
Panels identified several key issues including the impact of school closures, systemic exclusions and widespread misinformation. Impact of school closures was a concern for participants, highlighting significant setbacks for First Nations students. Barriers included limited literacy and numeracy challenges for parents, carers and grandparents as well as a lack competence or confidence to facilitate homeschooling. Other challenges included limited Wi-Fi access or educational equipment like laptops, and crowded housing made having a designated homeschooling space difficult. In addition, having multiple children in the household at different school levels became difficult for parents, carers, grandparents to co-ordinate. Similarly, participants recognised the added burden and extra challenges on single parent families to balancing homeschooling, household and work.
Systemic racism, exclusion and distrust were highlighted by participants, noting that First Nations peoples are often excluded from educational decision-making processes, with institutional racism and paternalistic attitudes persisting. Many First Nations parents deeply distrust the education system, particularly regarding the efficiency of COVID-19 messages, leaving many families too scared to send children to school out of fear of getting COVID-19.
Misinformation in the community meant public health messages were not clear, and community were unsure of who and what to trust.
Vaccination concerns were raised by one panel questioned whether First Nations people, including young people, would be prioritised in the vaccination rollout.
Following the evidence and discussions, the panel put forward decisions and recommendations regarding school closures during a pandemic.
Decision 1 focused on whether schools should close prior to a case or following a case. Two panels recommended schools remain open until there has been a confirmed case, while, one panel voted schools close prior to a case. For communities under travel restrictions or lockdown, it was suggested that schools or child care centres should remain operational.
Decision 2 addressed the implications of school closures. The panels expressed concerns that students would fall behind academically and children were already disadvantaged, as its impractical to deliver 6 hrs of homeschooling a day. The panels highlighted the potential stress and mental health load among students and not being able to spend time with their peers. Participants also noted the fear of the unknown of the virus and the broader pandemic response and whether children could cope with homeschooling.
The panels recommended ways to address these issues:
Provide families with Wi-Fi access, educational tools and resources during pandemics.
Schools should ○ distribute hard-copy curriculum packs. ○ include in the curriculum home-based learning, such as cooking, cleaning, shopping, and caring for others, alongside infectious diseases, incorporating cultural learning on Country. ○ explore remote or mobile classrooms to ensure continuity of learning. ○ engage First Nations Education Officers and Student Learning Support Officers for holistic student well-being care and learning support.
As part of the decision on school closures, the panels also considered who should make decisions. The panels recommended parents being active and equal participants in education decision-making processes. The Department of Education should develop engagement strategies to ensure appropriate representation of First Nations peoples. Also, public health should work with schools and engage ACCHOs to form decisions together. One panel recommended that ultimately state and regional Departments of Health should make decisions about school closures.
The panels also considered what would make families feel safe to send children back to school. There were similarities across panel discussions about what would make families feel safe to send children back to school including no community transmission, schools having pandemic plans in place, if the messages came from the Department of Health, and if children were tested prior to opening schools.
Based on these discussions, the panels recommended implementing a one-stop-information-hub coordinated by First Nations people. They also suggested that schools activate pandemic action and safety plans, provide Personal Protective Equipment (PPE), implement temperature testing and limit classroom numbers to ensure safe physical distancing.
The panels also considered whether there should be a blanket exemption for First Nations students from attending school during a pandemic. A blanket exemption refers to a policy enabling First Nations students to be exempt from attending school during a pandemic, giving families choice to keep children at home without facing penalties. There were different views on whether the Department of Education should have a blanket exemption for First Nations students and families during a pandemic.
For exemption: Two panels supported a blanket exemption. However, one panel set a condition that the blanket exemption be activated when there is community transmission.
Against exemption: Panel 3 (WA) opposed a blanket exemption because of the historical connotations and could be perceived as segregating and discriminatory. However, they noted that parents should have freedom of choice to keep children home, without judgement and penalties from the Department of Education. Caregivers who choose to keep children at home should be offered homeschooling resources. They also stated the word exemption relates to past exclusionary policies and practices, suggesting transitional be used instead. Transitional learning is a more strengths-based way of working with people through different phases under extraordinary circumstances, “we will work with you on the transition when you come back to school” (participant 7, male).
The panels made the following recommendations to ensure First Nations students and families are supported during a pandemic:
Implement conditional blanket exemptions during pandemics, activated when there is local community transmission, providing families the option to keep children home.
Provide families with homeschooling resources who choose to keep children at home, ensuring there are no penalties or judgement.
Use transitional learning and apply strengths-based approaches to support children returning to school.
The panels were asked whether there should there be a different return to school policy for First Nations students During a pandemic, but views were divided:
For different policy: Panel 1 (QLD) and 2 (NSW) supported a different return to school policy, because of the educational gap between First Nations and non-First Nations students. Consideration was given to burden of disease among First Nations peoples and the risk of children infecting other household members, especially Elders. Panel 1 (QLD) suggested a staggered approach where First Nations students return 1-2 weeks earlier than others, to ensure students are not left behind, particularly those who might not have had access to homeschooling. They suggested individual student assessments be conducted to determine the level of need and focus on key learning areas. Against different policy: Panel 3 (WA) reached consensus opposing a different return to school policy as it could cause division, children may face discrimination, and different policies could be seen as stereotyping or disadvantaging First Nations children.
Recommendations: consider staggered return approach and conduct individual assessments to identify learning needs. Ensure school policies are equitable and do not create division.
Part C: COVID-19 risk communication strategies & governance
The panels examined evidence for effective pandemic risk communication and governance. Deliberations focused on the importance of trust, openness and localised and community-driven public health strategies.
The panels identified several key issues regarding risk communication and governance during a pandemic, which impacted trust and engagement of First Nations communities.
One-size-fits-all approaches to pandemic communication, public health response and management and disease control measures do not work. Applying whole of population strategies to responses are ineffective and often fails to reflect First Nations lived experiences.
Issues with public health communication arose from false messaging, disinformation and misinformation, which fragmented communities, causing fear, confusion and distrust, and placed mistrust in the messengers.
Burden on First Nations health organisations included the extra challenges First Nations health organisations and employees faced during the pandemic. Many were overburdened and required adequate resourcing to meet additional service and programme delivery needs. In addition, First Nations health staff were utilised but expected to perform their primary role as well as fulfilling pandemic responsibilities.
Mistrust of government was exacerbated during with the pandemic, highlighting long-standing distrust between First Nations peoples and government health authorities and law enforcement.
As part of the deliberations on risk communication and governance, the panel made important decisions and several recommendations on how governments can share information rapidly with First Nations communities.
Decision 1 asked the panels to consider how authorities should share information with First Nations communities. The panels highlighted the importance of sharing information with First Nations communities as widely and rapidly as possible, emphasising building relationships and trust as essential in engaging communities. First Nations Health Workers were seen as integral in breaking down complex information, and debunking myths and misinformation. The Panels noted that First Nations peoples should construct and share information through local networks as well as First Nations media outlets, television, newspapers, radio, brochures and posters. Information could also be shared with education settings, pharmacies and medical practices, digital message boards, and letterbox drop-offs. Panels highlighted children as key deliverers of health information for families, with schools playing a pivotal role in delivering COVID-19 education programmes on public health actions.
All panels agreed the need for proactive and ongoing community engagement by government and health authorities. Panel 3 (WA) highlighted that local engagement and partnership agreements between ACCHOs and state health departments could improve policy and practice by embedding cultural inclusion in decision-making.
Following the discussions and decisions, the panels made some recommendations, grouped into key focus areas, including communication strategies, engagement and capacity-building.
For communication strategies, the panels recommended the following:
ACCHOs, and other First Nations organisations are funded and supported to develop and deliver localised and practical health communications in First Nations languages, including strategies for reaching people sleeping rough and those without digital access.
Ensure regular updates on trusted First Nations social media platforms and distribute through schools, pharmacies and family support services to promote reach and community engagement.
The panels made key recommendations regarding community engagement and capacity-building:
Establish and fund local First Nations pandemic response teams to support self-determination, empowerment, and leadership, and participation in strategic decision-making forums
Equip pharmacy staff with pandemic knowledge, and utilise family support services, early childhood education to distribute health information and resources.
Celebrate and share success stories of First Nations COVID-19 responses to promote knowledge exchange and pandemic learnings.
The panels also highlighted the importance of education and training to strengthen pandemic preparedness and response, and recommended:
Develop culturally appropriate resources to promote personal and household hygiene.
Train health professionals in cultural safety and local community contexts to enhance understanding
When asked about how government authorities could build community trust through communication, the panels stressed the need for inclusivity, through two-way learning and co-design of services and programmes. Inclusivity involves active listening and enabling First Nations peoples to determine the supports required to address local priorities. Trust, they noted, is built when people see their solutions and recommendations translated into tangible and practical policy actions.
The panel put forward a few recommendations for building trust with First Nations communities:
Ensure public health communication is informed, developed and disseminated by First Nations peoples, with consideration of remote, rural and urban communities.
Government authorities should be open, honest and transparent with the public about the evolving nature of the pandemic including the ongoing response options for First Nations communities.
Government authorities should appropriately engage with First Nations communities to ensure public health law supports First Nations cultural ways of doing and being.
Increase funding to build the First Nations workforce by employing community engagement roles to support health messaging, housing, food, transport, and socioemotional well-being, through a one-stop-shop approach.
Actively include First Nations peoples at all levels of pandemic responses, where there is inter-sectorial collaboration between local, regional, state, and national agencies.
The panels identified trusted and respected sources for pandemic information at different levels. At the local level, trusted sources and family champions play an important role in sharing crucial pandemic information to families and households. First Nations Health Workers working within government health departments and ACCHOs were recognised as being an important link to disseminate information. Also, local First Nations organisations including ACCHOs, local Aboriginal Land Councils, First Nations education workers and local disaster and emergency management groups, were seen as trusted sources in providing reliable information.
At the state level, panels stated many trusted government departments including Department of Communities and Justice, Department of Aboriginal Affairs, Primary Health Network, State ACCHO bodies, State Health Departments and State Emergency Services.
At the national level organisations such as the Department of Health, including First Nations Health Directorates, National Aboriginal Community Controlled Health Organisation (NACCHO) and HealthInfoNet online resource were entities seen as providing accurate, timely and trusted information.
At the international level, the World Health Organization was recognised to be a credible source of pandemic related information and guidance, particularly regarding its role during COVID-19.
Panels provided guidance on ensuring public health decisions support First Nations cultural ways of doing and being. Key strategies include the following:
Community-informed public health approaches: engage with local communities in culturally safe environments to develop disease control measures informed by First Nations communities and include strategies into local pandemic plans.
Strengthen public health governance: by establishing regional and state First Nations Incident Control Centres to manage responses. As well as regularly reviewing emergency management plans to address resilience, recovery, partnerships and community engagement, and capacity-building, and lessons learnt, and including First Nations peoples on Local Government Councils to guide pandemic engagement processes and decision-making.
Build trust with communities by collaborating with emergency services to educate communities on public health law and messages, promoting rapport and trust.
Culturally considered approaches by developing culturally safe public health restrictions that respect First Nations kinship systems, particularly for Sorry Business and funerals.
Empower local communities by supporting and implementing community action plans that reflect First Nations protocols and practices.
Participant reflections
Participants valued the community panel process as a good way of sharing and learning about others’ COVID-19 experiences. Some participants felt “it’s like I got a voice, that’s what it feels like” (participant 3, female) and that “if it happens again [a pandemic] we will know how to move forward better and be more prepared . . . [and] no one ever comes back and asks us how could we do it better” (participant 5, female). In addition, one participant said, “we’re making decisions on contributing towards policy development based on evidence, practical evidence in the community, not evidence on paper where decisions are made inside a board meeting, within four walls” (participant 6, male).
Expert presentations were pivotal in shifting participants understanding of COVID-19 actions, with one stating; “we’re finding out more information . . . and my mind is a little different thinking of some of the little things [the expert] said” (participant 3, female).
Discussion
Our findings show that community panels can be a culturally safe approach to engage First Nations peoples in considering difficult public health decisions during pandemics, highlighting key issues for governments, the health sector, and communities.
Public health strategies during a pandemic
One-size-fits-all-approaches to pandemics do not work (Massey et al., 2009). Participants in our study told us that equipping First Nations peoples with reliable, timely and accurate information is the most important and achievable action to reduce the spread of infectious diseases among First Nations communities. It is also imperative that First Nations peoples are well-informed about the reasons behind public health actions and directives, which can help facilitate trust with government and health authorities. The foundation of the strategies must be based on First Nations governance in public health and embracing First Nations ways. Community and ACCHOs access to essential PPE was also noted as being important. Lack of appropriate funding, lack of First Nations health workforce, and lack of supplies to support First Nations communities in a pandemic have been previously described by other First Nations peoples in Australia and globally (Charania & Tsuji, 2011; McCalman et al., 2021; NACCHO, 2020). These strategies must now be considered and included in pandemic plans to guide public health practitioners in how to safeguard First Nations peoples from infectious disease emergencies.
Public health communications
Panels emphasised that pandemic information must be communicated in a way that is meaningful, accessible, easy-to-understand and considers the diversity of First Nations peoples and culture. Participants identified that local networks and trusted community leaders are critical in ensuring the dissemination of health messages. Tailoring information cannot be a quick factsheet fix and by adding the Aboriginal and Torres Strait Islander flags will not make it culturally appropriate. Countering misinformation through the development of localised messages (Massey et al., 2011) that come from local leaders (Kerrigan et al., 2023) and First Nations health organisations work better (Finlay & Wenitong, 2020).
Health services and supporting First Nations health
The panels identified the need for more structures that support and enable First Nations communities towards self-determination and empowerment, through adequate resourcing for ACCHOs and the building the First Nations public health workforce (NACCHO, 2020). First Nations health workers play an important role in the communities where they live and work, highlighting the special role that local and connected leaders in developing and disseminating pandemic programmes and information to communities.
Inclusive public health pandemic policy and decision-making
The strength of First Nations culture is connection to people, community and Country, with children at the heart of cultural continuity and Elders as crucial knowledge holders. These sociocultural realities can make public health actions like physical distancing hard for many people. Pandemic measures of physical distancing and home isolation need to be reviewed and revised. First Nations families and communities should be supported to be together during a pandemic by making public health measures more appropriate and reflective of the lives of First Nations peoples. However, health authorities must work with First Nations peoples on how this could be done in a safe way. Our findings align with other studies conducted with First Nations peoples following the 2009 H1N1 pandemic (Charania & Tsuji, 2011; Massey et al., 2011), and during COVID-19 (McCalman et al., 2021; NACCHO, 2020), which points to the need to redesign pandemic policy to factor in more acceptable strategies that support First Nations social realities. The COVID-19 pandemic impacted on the education system, and the learning and well-being of students. It is well reported that a significant education gap exists between First Nations and non-First Nations students, particularly where communities experience many layers of disadvantage (Dabrowski et al., 2020). Participants in our study told us that homeschooling was very hard for students and parents, carers, grandparents for many reasons which are supported in other studies (Dabrowski et al., 2020; McCalman et al., 2023). If schools are impacted and closed during major infectious disease emergencies more support is required to ensure those students at risk of disengagement, are offered and provided with additional assistance.
The government has a historical patriarchal dominated system that lacks consideration for people’s culture and cultural diversity (Moreton-Robinson, 2009). Systemic exclusion of First Nations peoples in health policy decision-making processes was discussed in all three panels. The COVID-19 response and policies perpetuated paternalistic discourse where First Nations peoples had to be controlled to protect them (Donohue & McDowall, 2021). Home isolation and lockdown restrictions triggered traumatic experiences of past and current government legislation that intentionally excluded and marginalised First Nations peoples (McCalman et al., 2021). There were examples of First Nations communities being negatively treated and labelled by law enforcement because of public health law and restrictions (Donohue & McDowall, 2021), if public health actions reflected and respected First Nations peoples and culture, this would have increased trust. Government and health authorities can no longer keep doing the same thing and expecting different outcomes. Too often, infectious disease responses focus on doing the best for the most, while forgetting the rest, but we have highlighted different approaches are needed to enable equity and ensure those community members who are impacted the most, receive the most support.
Implications for public health policy and practice
Our findings suggest that engaging with First Nations people first before making any policy decisions about pandemic directives and actions is vital, and local partnership approaches and initiatives should be minimum standard practice (Wilson-Matenga et al., 2021). Using community panels as a way of engaging with First Nations peoples can inform the development of appropriate, acceptable, and achievable public health measures for First Nations communities. Studies have highlighted deliberative approaches, like community panels, empower communities to have a voice and a say, and ensures policies reflect community needs and values (Street et al., 2014). However, there is limited research that explicitly centre First Nations worldviews and practices, particularly relating to pandemic preparedness and response.
If First Nations people are mentioned in local, state, and national plans and policies, we are considered important; however, this is rarely translated into practice. Government and health authorities must do better to listen to First Nations people, provide a space to enable First Nations people to determine and drive local pandemic responses, and their solutions are translated from policy into actual practice.
The study has several strengths and limitations. First, this research was First Nations-informed and led, and participants were all First Nations peoples. This study was conducted with three First Nations communities, which cannot be expected to fully capture the perspectives or the experiences of other First Nations communities in Australia. This work was conducted in the first year of the COVID-19 pandemic, therefore some of the panel’s recommendations may need to be reviewed and updated to align with the evolving nature of the disease and response. Although face-to-face would have been preferrable, the panels were delivered virtually because of travel restrictions at the time of the research. The online approach may have limited participant engagement; however, we tried to minimise the risk through the engagement with local First Nations Health Workers at each of the study sites, who were known and trusted within their local communities.
Conclusion
This research emphasises the importance of engaging First Nations peoples in the development of public health strategies during a pandemic and that community panels is a suitable methodology. Through deeper understanding of contextual challenges and issues, government and health authorities can develop more effective, inclusive, and equitable responses to infectious disease emergencies that are more meaningful and reflective of First Nations people’s lives. The initial success of the First Nations COVID-19 response was attributed to being informed, led, coordinated, and delivered with a robust and strategic cultural lens provided by First Nations people, for First Nations people. The low COVID-19 case numbers and deaths in First Nations peoples in the initial phases of the pandemic, demonstrate the readiness and quick action of communities to ensure families and communities are safe from COVID-19. The success of this needs to be celebrated locally, at the state level and national level and recognised on a global scale. The insights, decisions and recommendations from these community panels are not limited to the COVD-19 pandemic but provide important and valuable ways government and health authorities can improve First Nations health outcomes for future pandemics.
Footnotes
Acknowledgements
We acknowledge the Custodians of the lands and seas on which we live and work as the First Nations Peoples of Australia. The First Nations authors acknowledge our ancestors and First Nations peoples who paved the way and give us the strength to enable us to work in this space. We also acknowledge the Custodians of the unceded lands of which the study took place, and acknowledge the strengths, contributions, wisdoms and stories of all First Nations peoples involved in this work.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This project was funded by the Australian Partnership for Preparedness Research on Infectious Disease Emergencies is a Centre of Research Excellence funded by the Australian Government National Health and Medical Research Council (NHMRC) GNT1116530.