
Abstract
The COVID-19 pandemic has disproportionately impacted Indigenous populations worldwide placing much importance on rapid and equitable vaccination. Nevertheless, many Indigenous communities have reported high vaccine hesitancy and low COVID-19 vaccine uptake. This may be attributed to various factors, including a lack of support for Indigenous leadership efforts to protect their communities and the pervasive infodemic targeting First Nations Peoples. In August 2022, we hosted an international symposium to bring together Indigenous and non-Indigenous community leaders, clinicians, and researchers to discuss pandemic experiences and lessons learnt. This commentary highlights examples of harnessing Indigenous leadership and self-governance to design and deliver tailored community-based and culturally appropriate COVID-19 vaccination programmes that improved vaccine uptake in Australia and Canada. These case studies demonstrate that Indigenous social-governance systems need to be valued, respected, and upheld if we are to make meaningful efforts to address health inequities among Indigenous communities during future pandemics.
Introduction
“Ask us, listen to us, share with us”
On March 11, 2020, the World Health Organization (WHO) declared a pandemic due to a novel coronavirus (severe acute respiratory syndrome coronavirus 2 [SARS-CoV-2]) (Ciotti et al., 2020). The virus spread globally and as of March 2024, the coronavirus disease (COVID-19) has caused almost 775 million cases and more than 7 million deaths (WHO, n.d.). Globally, Indigenous populations have been negatively impacted by the COVID-19 pandemic (Spence & Sekercioglu, 2023). This public health emergency has brought to the forefront the durable pattern of inequities between Indigenous and non-Indigenous populations across a wide range of social and health indicators spanning different geographical regions, which is a product of colonialism (Sekercioglu & Spence, 2023; Spence & Sekercioglu, 2023). The potential long-term, disproportionate, direct and indirect impacts of the COVID-19 pandemic on Indigenous Peoples across social, health, and economic factors have been highlighted, which may further exacerbate existing inequities (Mashford-Pringle et al., 2021; Pickering et al., 2023; Spence et al., 2023).
Aboriginal and Torres Strait Islanders, herein also respectively referred to as First Nations Peoples, represent 3.8% of the total Australian population (Australian Bureau of Statistics, 2022). In Canada, the Constitution recognises three groups of Indigenous peoples: First Nations, Inuit, and Metis that collectively represent 5.0% of the total population (Statistics Canada, 2022). The present-day realities of Indigenous Peoples in Canada and Australia reflect enduring colonial policies and practices that have negatively impacted Indigenous ways of living, being, and doing (Dudgeon et al., 2014; Hahmann & Kumar, 2022; Reading & Wien, 2009). The transgenerational effects of colonisation have contributed to the adverse conditions experienced in many Indigenous communities, for example, overcrowded impoverished housing, inequitable access to quality health care, food insecurity, and so forth, leading to poorer health and well-being outcomes among Indigenous Peoples in Australia and Canada compared to the non-Indigenous populations (Dudgeon et al., 2014; Hahmann & Kumar, 2022; Reading & Wien, 2009).
Pandemics can exacerbate pre-existing vulnerabilities in Indigenous communities and contribute to an increased risk of disease (Crooks et al., 2020; Power et al., 2020; Spence & White, 2013). During the 2009 H1N1 influenza pandemic, First Nations Peoples in Australia experienced relatively higher infection, hospitalisation, and death rates than their non-Indigenous counterparts (Flint et al., 2010; Goggin et al., 2011; Kelly et al., 2009; Rudge & Massey, 2010). Similarly, Canadian Indigenous Peoples were more likely to be admitted to an intensive care unit compared to non-Indigenous populations, with those residing in geographically remote communities experiencing further hardships (Boggild et al., 2011; Kermode-Scott, 2009).
Indigenous populations have historically and continue to be excluded from pandemic planning processes, which have been dominated by Western knowledge, values, and command and control military models (Assembly of First Nations, 2020, 2021; Dynes, 1994; Miller & Durrheim, 2010). This can lead to mitigation measures that are countercultural and unfeasible to implement among Indigenous communities, given their realities (Charania & Tsuji, 2011a, 2011b; Crooks et al., 2020; Massey et al., 2011). Moreover, Indigenous communities have viewed and view government policies and communications suspiciously for its authoritarian approach that can undermine Indigenous self-determination and empowerment. For example, in Australia, top-down COVID-19 government policies perpetuated a paternalistic discourse that constructed pandemic related issues of Aboriginal and Torres Strait Islanders as a problem of vulnerability and mobility, thereby requiring a law and order response (Donohue & McDowall, 2021). In doing so, these policies overlooked interrelated determinants of disease risk among Aboriginal and Torres Strait Islander communities and disregarded their leadership actions to protect their communities (Donohue & McDowall, 2021).
Given how government policies and strategies can overlook the realities faced by Indigenous communities and their knowledge, cultural values, and processes, it is vital that they have ownership over planning efforts. In Aotearoa (New Zealand), local safety protocols were implemented that were based on Māori (Indigenous people of New Zealand) concepts like tapu (prohibited or restricted), noa (free from restriction), and rāhui (temporary restriction) (Severinsen et al., 2021). This involved iwi (extended kinship group or tribe in Māori society) setting up road checkpoints in rural regions and restricting access to natural areas, showcasing community-driven efforts to identify public health risks, particularly in communities vulnerable to COVID-19 due to isolation, chronic health issues and limited health care access (Severinsen et al., 2021). In Navajo (a Native American people of the Southwestern USA) Nation, older age, multigenerational housing, and lack of running water increased the impact of COVID-19; therefore, the Navajo Department of Health ordered all members of their jurisdiction over the age of 2 years old to wear masks in public and instituted isolation measures including weekend curfews (Power et al., 2020). These examples illustrate that despite facing various systemic challenges, Indigenous communities were independently harnessing Indigenous wisdom, principles, and innovative strategies to safeguard their populations.
Our previous research has shown the importance and value of respectful and meaningful engagement with Indigenous populations to develop tailored community-based and culturally appropriate pandemic plans and responses (Charania & Tsuji, 2012; Crooks et al., 2020; Crooks et al., 2022; Massey et al., 2011; Rudge & Massey, 2010). Indeed, the COVID-19 pandemic continues to bring greater attention to strengthening the capacity of Indigenous leadership and the critical nature of Indigenous-led and delivered responses. During the COVID-19 pandemic, there were instances of successfully implementing Indigenous-specific strategies to reduce the disease burden among Indigenous communities (Power et al., 2020). Proactive efforts were made early on during the COVID-19 pandemic to ensure there was Aboriginal and Torres Strait Islander leadership, voice, and representation in making decisions and recommendations to the highest levels of government, through the establishment of the national Aboriginal and Torres Strait Islander Advisory Group on COVID-19 (Crooks et al., 2020). A recent study further highlighted Indigenous nursing leadership that provided trusted, holistic, and culturally meaningful care during COVID-19, leading to calls to support the self-determination of Indigenous Peoples (Clark et al., 2021).
Rapidly vaccinating the global population has been an important pillar of the pandemic response to reduce transmission and severe outcomes, and prevent millions of deaths (Watson et al., 2022). To prevent COVID-19 outbreaks and minimise health inequities, it has been critical to achieve high vaccination rates in Indigenous communities. However, Indigenous populations generally have lower COVID-19 vaccination uptake and higher rates of vaccine hesitancy compared to non-Indigenous populations (MacDonald et al., 2021; Pickering et al., 2023). Despite some efforts to engage Indigenous communities during the COVID-19 vaccine rollout, vaccination booking systems and services were not appropriately tailored to address the communities’ needs (Kholina et al., 2022). These Western-dominated models of vaccine delivery dismissed the root causes of vaccine hesitancy among Indigenous communities, thereby increasing mistrust and vaccine reluctance (Kholina et al., 2022; Mosby & Swidrovich, 2021). For example, although Indigenous communities in Canada were prioritised for vaccine allocation, concerns about the new COVID-19 vaccines stemmed from past medical experimentation on Indigenous Peoples (Mosby & Swidrovich, 2021). That being said, some Indigenous communities have reported high vaccination rates, which were largely attributed to Indigenous autonomy and control of vaccine delivery programmes (Pickering et al., 2023).
In August 2022, we hosted an international symposium to bring together Indigenous and non-Indigenous community leaders, practitioners, and researchers from Canada, Australia, and Aotearoa to discuss pandemic experiences and collective ways forward in a safe sharing space. This commentary highlights examples of COVID-19 vaccination programmes in Australia and Canada that harnessed models of Indigenous leadership and self-governance. Authors of this commentary identify as Indigenous people: Katrina Clark, Kristy Brooks, Gisele Kataquapit, Celine Sutherland, and Nicholas Spence; and as non-Indigenous people: Bavatharane Jeyanathan, Fatima Ahmed, Leonard Tsuji, Robert Moriarity, Fatih Sekercioglu, Eric Liberda, and Nadia Charania. Five case studies were chosen as the Indigenous authors were either aware or directly involved in designing and implementing strategies to improve COVID-19 vaccine access and uptake in their communities and could speak to the details of how Indigenous leadership made each strategy successful. As opposed to the dominant deficit approach that often characterises structurally marginalised communities, we collaboratively wrote this commentary using a strengths-based approach. In the context of Indigenous research, there is a growing recognition and adoption of strengths-based approaches, which emphasise values and practices centred on Indigenous self-determination and challenge deeply ingrained assumptions regarding deficits (Bryant et al., 2021). The paradigm shift highlights the transformative power of strengths-based approaches as they facilitate a deeper appreciation of Indigenous strengths and resilience, and empowers Indigenous voices and agency (Bryant et al., 2021). In the conclusion, we discuss the patterned elements of success within these Indigenous communities that contributed to improving COVID-19 vaccine uptake. Importantly, we frame this discussion within the tenants of the United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) that affirm Indigenous sovereignty.
Case studies
Kimberley region (Western Australia, Australia)
The Kimberley region is the northern remote region of Western Australia, which is home to the Ngarinyin Aboriginal Australian people that represents approximately 60 clans who belong to four larger nations. In February 2020, the Kimberley Aboriginal Medical Service (KAMS) of Western Australia developed a collaborative partnership model that included key public health, clinical health services, and community with Aboriginal and Torres Strait Islander representation embedded in the central pandemic management teams across the Kimberley. KAMS implemented several planning and decision-making groups to assist in a timely and effective COVID-19 response for Aboriginal and Torres Strait Islander residents. KAMS set up three integral response groups: (a) the leadership group, who made decisions about the COVID-19 response and provided oversight; (b) the clinical response group, who provided advice on the clinical response; and (c) the communications group, who developed and distributed approved communication materials. Each group reported to the KAMS COVID-19 Command Centre that made high-level strategic decisions, and reported further through to the KAMS and the Kimberley Renal Services Boards, which held ultimate responsibility and accountability for all organisational matters. This Board of Directors is comprised of highly respected and experienced Aboriginal health leaders from their Member Services, which was vital to facilitate a coordinated and timely pandemic response. KAMS was funded by the Australian Government, and Aboriginal staff members were part of working groups and expert panels throughout the pandemic response, including the Commonwealth COVID-19 Indigenous Advisory Group, the Commonwealth COVID-19 Point-of-Care Testing Advisory Group, the Western Australia COVID-19 Aboriginal Advisory Group, COVID-19 clinical evidence care panels, Kimberly Regional Emergency Operations Committee, and the Kimberly Operational Area Support Group.
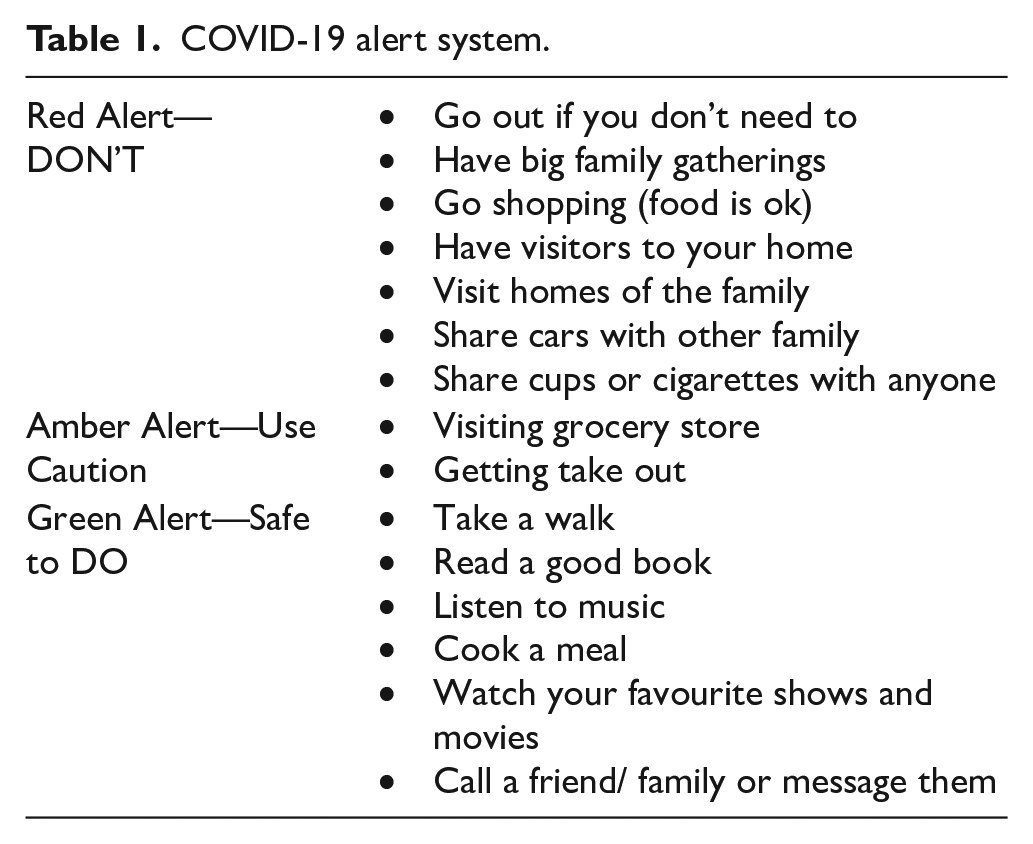
Leadership within Aboriginal health means working as a team and involving people with all experiences, including the community. For instance, during the COVID-19 pandemic, community members suggested that the communications should be modelled off the cyclone red, amber, and green warning system as they were already familiar with this system, being an area prone to cyclones. This decision helped speed up communications and made sure that the community understood the gravity of the COVID-19 situation and the appropriate procedures to take by adapting the colour-coded system for cyclone warnings. This three-stage COVID-19 alert system specified a list of actions and decisions to protect the community (Table 1). Moreover, it was crucial to include First Nations-focused efforts and effectively engage the community to increase COVID-19 vaccine uptake, which included understanding community needs, working in partnership with communities, using targeted messaging that was informed by the community, and addressing the systemic traumas experienced by First Nations People seeking medical care.
COVID-19 alert system.
Maningrida (Northern Territory, Australia)
Maningrida, also known as Manayingkarírra and Manawukan, is a community in Northern Territory home to more than 2,300 people with 77% identifying as Aboriginal. Maningrida’s COVID-19 talk straight vaccination strategy made national headlines after a record high number of community members got vaccinated (National Aboriginal Community Controlled Health Organisation [NACCHO], 2021). Between July and September 2021, three vaccination drives successfully administered 2,843 vaccine doses, representing over 70% of eligible community members aged 16 years and older, and almost 45% of community members were fully vaccinated (NACCHO, 2021). The community-led campaign was delivered by Mala’la Health Service, Aboriginal Health Workers, Traditional Owners, community leaders and multiple other agencies to build the community’s confidence in COVID-19 vaccines (NACCHO, 2021). They worked collaboratively to develop strategies that were based on Indigenous values, focusing on the importance of protecting their family, culture, and songlines—Aboriginal navigational tracks, as mainstream campaigns were seen as confusing and ineffective (NACCHO, 2021). The strategy involved local information road shows and campaign videos in dispelling COVID-19 vaccination myths (NACCHO, 2021). Tailored and clear messages in local languages were shared via social media, public town hall meetings, local businesses and organisations, and door-to-door to reach community members and address their concerns (NACCHO, 2021). Videos were broadcasted in multiple languages online and on large screens throughout the community, and Elders also supported sharing the message with community members (NACCHO, 2021). In Aboriginal communities, Elders hold a significant and respected role as those who have demonstrated wisdom, knowledge, and experience in their community. Elders play a critical role in preserving and passing down the cultural, social, and spiritual traditions to younger generations and as such, can support public health messages to protect their community.
Hunter New England Region (Northern New South Wales, Australia)
Hunter New England (HNE) is a large geographical area in New South Wales, Australia, with approximately 72,000 Aboriginal and Torres Strait Islander residents. In March 2020, the local Public Health Incident Command System embedded an Aboriginal governance model to provide cultural oversight and insight into the local COVID-19 incident command system (Crooks et al., 2023). The model ensured the local pandemic response was culturally informed and inclusive of Aboriginal people’s voices and perspectives. The Aboriginal governance model enabled the establishment of the Public Health Aboriginal Team (PHAT) for COVID-19 that provided strategic and operational leadership, advice, and guidance for the local pandemic response. The PHAT coordinated three strategic and multiagency governance groups: (a) the HNE Aboriginal Governance Group on COVID-19; (b) the HNE Aboriginal Data Governance Group; and (c) the HNE Aboriginal Vaccination Steering Committee. These governance groups fostered and promoted transparent, two-way communication to support effective engagement (Crooks et al., 2023). As Indigenous data sovereignty is paramount, the Aboriginal Data Governance Group provided cultural oversight to ensure COVID-19 data were reported and interpreted through a cultural lens (Crooks et al., 2023). Importantly, an accountability framework was implemented so that response teams ensured that everyone had the opportunity to receive culturally appropriate support (Crooks et al., 2023). This involved the PHAT staff providing holistic care and follow-up telephone support to the case and their contacts and family members, including education, referral to testing and vaccine clinics, provision of personal and household items, and referral to local support services.
The PHAT, in partnership with the HNE Immunisation Team, activated the HNE Aboriginal Vaccination Steering Committee in October 2021 with the support of the local executive for emergency management, the Health Services Functional Area Coordinator, to respond to low initial COVID-19 vaccine uptake and the coverage gap between Aboriginal and non-Indigenous residents, and enable the development and implementation of locally informed and determined COVID-19 vaccination strategies. Situational reports were provided by PHAT to inform consensual decision-making by the Committee. The Committee consisted of Aboriginal and Torres Strait Islander health leaders, practitioners, and clinicians, as well as non-Aboriginal emergency management and immunisation leaders and clinicians. In the 5 weeks following the establishment of the Committee, 29,751 vaccinations were administered. This was achieved by working in partnership with key internal and external stakeholders including HNE Local Health District, Aboriginal Community-Controlled Health Organisations, the Australian Royal Flying Doctor Services, Universities, and the Primary Health Network to offer a variety of accessible options ranging from large pop-up walk in clinics, after hours and weekend clinics, to more personal at home visits. The Team also offered transport, developed culturally appropriate and targeted information and messaging, and engaged local public health experts to have conversations with community members who were undecided to have the COVID-19 vaccine. Rather than expecting community members to register online to have the vaccine to then book in to receive it, the Team removed the barriers and challenges that Aboriginal and Torres Strait Islander often face when accessing health care, by taking the vaccine to the communities through localised and tailored vaccination strategies. This governance approach to a pandemic response had not previously existed in New South Wales and provided a model for embedding culturally and community-responsive insights to improve outcomes for Aboriginal and Torres Strait Islanders.
Fort Albany First Nation (Ontario, Canada)
Fort Albany First Nation is a remote and isolated fly-in only Cree (a North American Indigenous people) community located in the western James Bay area of Ontario, Canada, home to approximately 900 people. Being a community that is only accessible by air year-round and seasonally by water or winter-ice road, these are some of unique considerations to address when responding to a pandemic. Building upon experiences from the H1N1-pandemic (Charania & Tsuji, 2011a) and pandemic plan (Charania & Tsuji, 2012), the community took a collaborative approach that brought together local leaders representing the health centre, hospital, police services, education, grocery store, emergency medical services, clergy, power and water treatment plants, social services, and Band Council—Fort Albany First Nation’s elected form of government. Based on previous experience with the H1N1-pandemic, the initial goal was to stop the virus from entering the community. Therefore, the Health Director of Peetabeck Health Services began taking precautions, such as monitoring cases of respiratory illnesses in the community, in late December 2019, when there was first news of a virus circulating in Wuhan, China (Wu et al., 2020). After a pandemic was declared, mitigation measures later also included mandatory isolation for any health centre staff who were travelling for 10 days. Eventually, once testing was available, all travellers arriving in the community were swabbed to identify potential cases and allow for contact tracing.
Working in collaboration with Ornge and Weeneebayko General Hospital, the community’s COVID-19 vaccination programme achieved high uptake, with approximately 97% of the eligible adult residents receiving their first and second doses. Many factors, such as having accessible and culturally appropriate resources available in both English and Cree, contributed to the vaccine programme’s success. Accessibility was an especially important factor when caring for and vaccinating Elders in the community, who faced barriers such as language—only speaking Cree—and transportation, with some being unable to leave their homes due to illness or their vulnerability. To address this, free transportation options were available for the vaccine clinics, with some accommodations being made to vaccinate Elders in their homes. In addition, interpreters, who helped screen and guide residents through the consent process, were also available at the vaccine clinics. As the community is remote and does not have cell service, social media platforms, for example Facebook, were often used to share information on vaccines and booster clinics and information about COVID-19. Respected and trusted members of the community, such as the Chief, Health Director, and Community Nurse, livestreamed information sessions in both English and Cree to provide information about the vaccines, boosters, clinic information, and general updates about the pandemic. They also shared their own vaccine experiences, through the livestream or in-person, which also helped build confidence in the vaccines and boosters among community members. Having community members leading and at the forefront of the vaccine roll-out programme helped garner trust and inform community members, which ultimately led to high vaccine uptake rates. Having community members design and deliver the COVID-19 vaccination programme ensured that community-specific challenges were addressed, and using strengths-based approaches, vaccination programmes were easily accessible.
Operation remote immunity (northern Ontario, Canada)
When COVID-19 was initially detected, several remote and northern Indigenous communities in Canada—many already lacking adequate health infrastructure, personnel, and resources—raced to develop plans before the region headed into another health care crisis (Fiddler, 2021). In February 2021, largely credited to Nishnawbe Aski Nation — a tribal council comprised of 49 northern Ontarian First Nations — leaders organised teams of doctors, nurses, government officials, Canadian Armed Forces members, and Canadian rangers to coordinate and deliver COVID-19 vaccines to 31 fly-in communities and Moosonee (Government of Ontario, 2021). Supported by Ornge hospital, an existing air ambulance and critical care transport service with regulatory and oversight by the Ontario Ministry of Health, this three-phased effort was called Operation Remote Immunity (ORI) (Government of Ontario, 2021; Ornge, 2021, 2022).
While collaboration and communication fostered across multiple agencies with a focus on community engagement played a significant role in the success of ORI, it was ultimately the leadership of First Nation communities that drove the initiative forward. This leadership was crucial in ensuring that ORI was accessible, culturally appropriate, and effective. Part of the challenge was ensuring communities had access to the necessary resources and information to make informed decisions about getting vaccinated (Chidley-Hill, 2021). Months before vaccine approval, local leadership collectively built trust and vaccine confidence through public health campaigns on local radio stations and social media in local dialects, community visits by Elders and distribution of translated pamphlets and materials, discussing vaccine safety and efficacy and encouraging informed consent (Chidley-Hill, 2021; Ornge, 2021; Temerty Faculty of Medicine University of Toronto, 2021). In instances in which vaccine hesitancy was observed, First Nation Chiefs were often the first to address concerns and provide reassurance by receiving vaccines themselves, thereby promoting confidence in vaccine safety (Chidley-Hill, 2021b). Community leadership also played a crucial role in identifying and addressing challenges unique to each community, including coordinating transportation for Elders and those with mobility issues and, setting up vaccination sites that were accessible convenient, and ensuring that the most at-risk community members were protected (Burton et al., 2023; Northern Policy Institute, 2021). This led to an increase in vaccine uptake and a successful vaccination campaign, with over 42,000 doses administered by the end of ORI’s final phase in February 2022 (Government of Ontario, 2021; Ivers et al., 2022). The success of ORI serves as a model for future health care initiatives, emphasising the need to prioritise and integrate Indigenous leadership at all levels of planning. In the end, the success of ORI is an indication of what can be achieved to address diverse community needs and the potential to do things differently with greater emphasis on Indigenous autonomy and ownership.
Conclusion
These case studies celebrate a range of Indigenous-led approaches for COVID-19 pandemic responses and vaccination programmes in both Australia and Canada. Collectively, these case studies underscore the need for community-led, culturally responsive, and Indigenous-focused strategies in navigating the complexities of the COVID-19 pandemic. They demonstrate that when Indigenous communities are empowered to take ownership of their health care initiatives, they can effectively address diverse challenges and achieve meaningful outcomes, emphasising the need for greater Indigenous autonomy and ownership in future health care endeavours. While each region faced distinct challenges and circumstances, at the heart of these case studies are common threads of exerting Indigenous self-determination, empowerment, and leadership as key drivers of success. These programmes demonstrate that when Indigenous community health and planning is in Indigenous hands, strategies are culturally appropriate, reflect Indigenous cultural values of respect, particularly of Elders, and more relevant and accessible for Indigenous Peoples and their communities. Moreover, other supportive mechanisms include collaborative partnership models that bring together multiple agencies with representation of Indigenous voices for shared decision-making and the provision of funding and resources necessary to support Indigenous-led initiatives.
We note some limitations regarding the presented case studies. For instance, we acknowledge that other factors beyond Indigenous models of leadership contributed to high COVID-19 vaccine uptake in some communities. Moreover, we recognise that there is much diversity within the Indigenous populations, and we have not included case studies from all contexts, such as those living off reserve.
Indigenous models of leadership and self-governance must be respected and prioritised during pandemic responses to support collaborative, strengths-based, community-based, and community-led initiatives. These lessons should be incorporated for current and future pandemics and vaccine rollouts to support equitable outcomes for Indigenous communities. This cross-national work highlights how sharing information across countries is useful to identify common elements of strength despite differences between countries.
Supplemental Material
sj-docx-1-aln-10.1177_11771801241235418 – Supplemental material for Highlighting models of Indigenous leadership and self-governance for COVID-19 vaccination programmes
Supplemental material, sj-docx-1-aln-10.1177_11771801241235418 for Highlighting models of Indigenous leadership and self-governance for COVID-19 vaccination programmes by Katrina Clark, Kristy Crooks, Bavatharane Jeyanathan, Fatima Ahmed, Gisele Kataquapit, Celine Sutherland, Leonard J.S. Tsuji, Robert J. Moriarity, Nicholas D. Spence, Fatih Sekercioglu, Eric N. Liberda and Nadia A. Charania in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors acknowledge the community members who have supported these efforts and for sharing their experiences and knowledge. The authors also thank all the front-line and essential workers who played a vital role in keeping our communities safe and for their service. Finally, thank you to all the attendees of the symposium for their valuable insights and contributions.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Canadian Institutes of Health Research (grant no. FRN179413).
Glossary
Aotearoa New Zealand
Cree a North American Indigenous people
Inuit an Indigenous people of Canada
iwi extended kinship group or tribe in Māori society
Māori Indigenous people of New Zealand
Métis an Indigenous people of Canada
Navajo a Native American people of the Southwestern USA
Ngarinyin Aboriginal Australian people of the Kimberly region of Western Australia
noa free from restriction
rāhui temporary restriction
tapu prohibited or restricted
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.