
Abstract
A rapid systematized review of health care programmes for Indigenous peoples in Canada from January 1 2019 to March 9 2022 resulted in two programmes that were evaluated as safe by the Indigenous recipients of care. Thematic analysis identified four cultural safety domains that created a safe, high-quality, patient-centred approach to health programming for Indigenous peoples from the evaluated programmes, a scoping review and the grey literature: patient empowerment; patients are supported to draw strength from their Indigenous identity, culture and community; provide trauma-informed care; and Indigenous leadership, decision-making and health governance. We describe the cultural safety domains and how they were applied in the evaluated programmes. First Nations members of the Wâhkohtowin Research Group and Elders Mentoring Programme in Maskwacîs in the Treaty 6 region of Canada agreed in facilitated discussions that the domains were authentic from their perspective and applicable to perinatal programmes in their community.
Keywords
Introduction
Many countries promote cultural competence within the health care system to improve the provision of treatments and programmes for a diversity of patients. Culturally competent care providers appreciate the differences in languages, customs, belief systems and behaviours among cultures to deliver effective, quality care (Cross et al., 1989). However, culturally competent care alone is insufficient to reduce health inequities among ethnic, racialized, minority and Indigenous groups that result from unequal power relationships, the unfair distribution of the social determinants of health, marginalization, biases, unexamined privilege, colonialism and institutional racism. Consequently, several countries including Australia, Canada, New Zealand and the United States recognize the importance of cultural safety within health care as a strategy to provide equity-oriented health care that meets the needs, priorities, histories and contexts of patients and populations receiving care (Curtis et al., 2019; Ford-Gilboe et al., 2018). Cultural safety in health care first emerged in New Zealand in the 1980s among Māori (the Indigenous peoples of New Zealand) nurses in response to the poor health of Māori that could not be mitigated by cultural competency among care providers (Polaschek, 1998). Distinct from cultural competency with its focus on cultural awareness, cultural safety is the delivery of care that reduces the power differentials between the health care provider and the patient, requires the health care provider to work with patients in a way that is free from racism and discrimination, considers colonial policies and practices, and shows respect for culture, identity and rights, resulting in care that is client driven (Curtis et al., 2019; National Aboriginal Health Organization, 2009; Wylie & McConkey, 2019).
Indigenous peoples in economically wealthy countries such as Australia, Canada, New Zealand and the United States experience profound health inequities because of colonialism, racism and unfavourable social determinants of health, such as poverty (Anderson et al., 2016; Willows et al., 2022). Indigenous peoples in these countries have the need for high-quality health care, yet often interact with a health care system that is culturally unsafe for them, which furthers Indigenous people’s health inequities (Curtis et al., 2019; Yaphe et al., 2019). Given differences in health care systems and factors associated with health inequities, country-specific approaches to cultural safety may be required to address health inequities experienced by Indigenous peoples.
In Canada, Indigenous peoples is the collective name for the original peoples of North America and their descendants: First Nations, Inuit (Indigenous peoples of Arctic Canada) and Métis (one of three culturally distinct groups of Indigenous peoples in Canada, primarily of mixed First Nations and European ancestry). Indigenous peoples in Canada may lack trust in the publicly funded health care system given that Western medicine and knowledge systems are prioritized in the health care setting, and the anti-Indigenous racism that they may experience in the health care system (Allen et al., 2020). Anti-Indigenous racism is expressed at the interpersonal level through the stereotypes and prejudices held by health providers and their discriminatory behaviours towards Indigenous peoples, and at the systemic level through health care policies, practices and legislation that reinforce the constructed inferiority of Indigenous peoples (Wylie & McConkey, 2019). While cultural safety in health care is therefore deemed essential in Canada to reduce health inequities and improve health outcomes for patients from marginalized communities, including Indigenous patients (Erb & Loppie, 2023; Ford-Gilboe et al., 2018), there has been limited discussion of how to design and implement culturally safe health programmes for Indigenous peoples and there are few examples in the peer-reviewed literature of programmes in health care settings that have been evaluated for cultural safety by Indigenous patients or clients receiving care (Brooks-Cleator et al., 2018; Chakanyuka et al., 2022; Tremblay et al., 2023). The uncertainty about how cultural safety is achieved for Indigenous peoples who access care services has hindered the implementation of culturally safe programmes as well as the evaluation of programmes for cultural safety (Mackean et al., 2020). While one scoping review of the literature pertaining to culturally safe health programmes, initiatives, services or care was done to identify the key components of culturally safe health initiatives for the Indigenous population in Canada, it did not specifically include programmes that had undergone evaluation for cultural safety (Brooks-Cleator et al., 2018).
Given the limited literature on programmes in Canada evaluated for cultural safety in health care settings, the first objective of this research was to do a rapid systematized review to identify health care programmes that had been evaluated as culturally safe for Indigenous patients or clients. The second objective was to identify and authenticate cultural safety domains for health programmes for Indigenous individuals in Canada from the evaluated programmes included in the systematized review, a scoping review of culturally safe health initiatives for Indigenous peoples in Canada (Brooks-Cleator et al., 2018) and the grey literature. Information from this research about cultural safety domains and evidence-based programmes would be beneficial for Indigenous peoples receiving care as well as in health care leadership, decision-making and governance. It was anticipated that the research would also contribute to the Cree (a culturally distinct group of Indigenous First Nations peoples some who live in the Treaty 6 region of Alberta, Canada) beneficiaries of this research. The Wâhkohtowin Research Group and the Maskwacîs Elders Mentoring Programme was established in response to perinatal health risks in Maskwacîs, Alberta, Canada. Using participatory evaluation, through facilitated discussions we determined if the identified cultural safety domains were considered authentic by members of the Wâhkohtowin Research Group and Maskwacîs Elders Mentoring Programme. Domains were considered authentic if members consensually agreed that the domains were convincing to them, and if they could perceive incorporating them into community health programmes (Johnson and Rasulova, 2017).
Methods
Self-location of the authors
Author self-location allows the reader to understand the lens from which research was conducted (Chakanyuka et al., 2022). The incentive for the research by the authors was our relationship with or interest in the Wâhkohtowin Research Group and Maskwacîs Elders Mentoring Programme. All authors were committed to improving prenatal health services in Maskwacîs through this research and had personal or professional interests in advancing the health of Indigenous peoples in Canada, including by ensuring cultural safety in health programmes. Author 1 is a community health activist through her work with communities and families, which includes working with Indigenous communities to support grant funding for mental wellness and addictions. Her interest in families and improving perinatal outcomes culminated in her doing this cultural safety research for her MSc project in Community Nutrition under the supervision of Author 7. In doing her research, she worked closely with Author 6 who is a Public Services Librarian at the University of Alberta who identifies as a Métis who is in the process of reconnecting with her Indigenous heritage and becoming decolonized. Author 6 has expertise in evidence syntheses, including reviews related to Indigenous peoples in Canada completed with Author 7 (Gillies et al., 2020). The authors had a collective interest in participatory health intervention development and evaluation. With backgrounds in public health nutrition, non-Indigenous Authors 1, 4, 5 and 7 at the University of Alberta are interested in preventing non-communicable diseases and promoting Indigenous maternal-child health and wellness through community action and by harnessing the immense cultural strength within communities to overcome adversity. Authors 4, 5 and 7 have had long-term community-based participatory research relationships with First Nations communities in the Treaty 6 region, including Maskwacîs. They prioritize respectful collaborative partnerships with these communities with the goal of diminishing the health disparities that disproportionately burden Indigenous populations in Canada. Author 5 participated in the Wâhkohtowin Research Group as a University of Alberta researcher while Ermineskin Cree Nation Authors 2 and 3 are Core Team members leading the Wâhkohtowin Research Group.
Community-based participatory research partnership
A community-based participatory research partnership was established in 2013 between Maskwacîs community members, including Elders, Maskwacîs Health Services and researchers at the University of Alberta. The partnership includes community programmes and managers within Maskwacîs, as well as clinical and health services within the area. One outcome of the partnership was the establishment of the Wâhkohtowin Research Group, in response to a community voiced desire to improve the health and wellbeing of families. It develops and evaluates strengths-based, community-led and culturally informed strategies in Maskwacîs aimed at supporting families during pre-conception, pregnancy, infancy and early childhood. Responding to concerns about perinatal health risks and adverse outcomes, a community-derived Elders Mentoring Programme was designed and implemented in 2016 to provide additional support for pregnant women and their partners beyond what is typically provided in mainstream prenatal health care services for pregnant women and their partners (Bruno et al., 2022; Oster et al., 2021). In January 2023, Elders and Wâhkohtowin Research Group members decided that the Elders Mentoring Programme needed to undergo a redevelopment to focus more specifically on culture, language and ceremony and to align more with community priorities that are being assessed through community engagement and research. The present research was done to contribute to the future redevelopment of the programme through an improved understanding of culturally safe health care programmes.
Objective 1: identify health care programmes in Canada that had been evaluated as culturally safe by Indigenous patients or clients
A rapid review is a form of evidence synthesis that provides timely information for decision-making compared with standard systematic reviews, through streamlining of methods (Garritty et al., 2021). A systematized review is an appropriate method for a rapid review. It includes elements of the systematic review process without meeting all standards for a systematic review, for example, quality appraisal. The methods for this systematized review were guided by Lefebvre et al. (2021) in consultation with a Public Services Librarian who is Author 6.
A preliminary search of the literature yielded few studies that had evaluated the impact of cultural safety of health care programmes for Indigenous peoples in Canada possibly because cultural safety is a newer concept than cultural competency to ensure patient care in Canada. To provide current information on cultural safety in the health care setting in a timely manner to benefit the Wâhkohtowin Research Group and the Elders Mentoring Programme, the literature search was restricted to January 1 2019 to March 9 2022. It included research that had evaluated cultural safety in health care programmes for Indigenous populations in Canada. The search was done on March 9, 2022, in MEDLINE (version 1946-present via Ovid) and CINAHL Plus with Full Text using Medical Subject Headings (MeSH) and keywords developed by the research team related to Indigenous peoples, health care settings, cultural safety and Canada. This comprehensive list of search terms was derived from a preliminary search of the peer-reviewed literature and from search terms previously developed by the Public Services Librarian and Author 7 (Gillies et al., 2020). Terms used to identify Canadian literature were selected based on all the provinces and territories, major cities and cities that have high Indigenous populations (Supplementary Material 1). Included articles were peer-reviewed, had an evaluation component to determine effectiveness, included Indigenous peoples in Canada, solely or in part and were published in English. Literature reviews and original research articles were eligible for inclusion.
To reduce bias two reviewers, Authors 1 and 4, examined the abstracts independently. If an abstract did not clearly describe the contents of an article, the full text was obtained, to determine if it was eligible. After abstracts were reviewed and confirmed to be appropriate, a full-text review was conducted to determine appropriateness for inclusion. Results were compared between the two reviewers and any disagreements were discussed. Discrepancies that could not be resolved were reviewed by third team member, Author 5 or 7, to make the final decision. Progress was tracked by each reviewer using an Excel spreadsheet and Covidence, which is a screening and data extraction tool used in creating systematic reviews. A data charting form was used to systematically capture relevant information from each study, including study design, number of participants, type of health care programme, how the programme was evaluated for cultural safety, individuals who evaluated the programme, such as Indigenous patients or health care providers and programme characteristics that contributed to cultural safety.
Objective 2: identify and authenticate cultural safety domains for health programmes
One source of cultural safety domains were the articles included in the systematized rapid review. Author 1 deeply engaged with the articles that met the inclusion criteria for the systematized review through multiple readings of each article, accompanied by note taking of programme attributes that could be considered distinct cultural safety domains. Author 4 confirmed that the domains identified by the first reviewer were congruent with the cultural safety domains that had been identified. A second source of cultural safety domains was a scoping review of culturally safe health initiatives for Indigenous peoples in Canada (Brooks-Cleator et al., 2018). Additional domains were sought May 1, 2022, by hand-searching in the Google search engine to find grey literature by Canadian health authorities or health care agencies about the delivery of culturally safe care in health care settings. Search terms included were “cultural safety,” “health care,” “Canada,” and “Indigenous people.” The intention of the search was to identify a few salient sources that could provide qualitative descriptions of cultural safety domains and describe how the domains could be used in practice. The first five pages were reviewed considering the ranking algorithms used by the Google search engine.
Thematic analysis was used to identify a set of domains from the systematized review, the scoping review and the grey literature sources that would help to create a safe, high-quality, patient-centred approach to health programming for Indigenous peoples in health care settings. A subset of elements for each domain was created. We did not focus on cultural safety domains or health care programmes related to the development or transformation of professional roles as a strategy for achieving cultural safety in health organizations; cultural safety training for health professionals; Indigenous health curriculum for medical students or nurses; or the enhancement of organizational capacity to deliver culturally safe health care. Programmes and cultural safety domains for these purposes have been described (Tremblay et al., 2023; Ward et al., 2021).
Members of the Elders Mentoring Programme and the Wâhkohtowin Research Group who advised this research, including Maskwacîs Authors 2 and 3, reviewed the cultural safety domains for authenticity. Through facilitated discussions, they were presented with each cultural safety domain to evaluate whether it was convincing to them from their perspective. To help ensure that the research was action-oriented members considered each domain in relation to prenatal programmes in Maskwacîs, the evolving Elders Mentoring Programme, as well as additional strategies supported by the Wâhkohtowin Research Group. A consensually agreed upon domain therefore could ideally be acted upon in health programming, empowering community members to improve their situation (Johnson & Rasulova, 2017). These facilitated discussions occurred at two monthly Community Advisory Committee meetings for the Elders Mentoring Programme that includes Elders facilitating the Programme, university researchers and community members. Everyone at the meetings had the opportunity to share their thoughts. Notes were taken of these meetings and were summarized using a team-based approach. Notes were internal to the Community Advisory Committee therefore, quotes from Elders were not available.
Ethical considerations
The literature reviews used publicly accessible documents as evidence, as such, institutional ethics approval was not required. The Âcimostakewin (sharing stories): Innovative Collaborations to Improve Health of Pregnant First Nations Women study was approved for the University of Alberta (Alberta Health Services, n.d.). The Wâhkohtowin Research Group has a research agreement, which envelopes the current study, outlining the purpose, approach, roles and responsibilities, methods, dissemination, ethical issues and data ownership, including the principles of Ownership, Control, Access and Possession® (OCAP) (First Nations Information Governance Centre, 2014). Community approval was received for discussions of the literature reviews and cultural safety domains from Elders, Knowledge Keepers and community members as part of the Wâhkohtowin Research Group. Elders were approached in one-on-one meetings to discuss the intent of the research using community-appropriate protocol. Elders provided verbal approval to participate.
Results
Evaluated programmes for Indigenous peoples in health care settings in Canada
Figure 1 is the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flow diagram for reporting systematic reviews (Page et al., 2021). Two articles met the inclusion criteria (Churchill et al., 2020; Firestone et al., 2019). Both were qualitative evaluations of programmes run in the city of Toronto in the province of Ontario, Canada. One study was a process evaluation of the Niiwin Wendaanimak Four Winds Wellness Programme (Niiwin Wendaanimak programme) (Firestone et al., 2019). The programme took place in a community health centre in Toronto’s west end. The objectives of the programme were to improve primary and harm reduction services for Indigenous populations, to identify and develop pathways to care for Indigenous adults and youth, particularly those who are homeless, living in poverty and at-risk of homelessness and to provide Indigenous culturally specific healing and psychosocial support. A qualitative process evaluation was carried out to (1) assess the collaborative service delivery model; (2) identify service gaps and issues for homeless and at-risk Indigenous populations; and (3) develop recommendations for how non-Indigenous organizations can provide culturally responsive services for Indigenous populations. Clients of the programme had often experienced multiple sources of trauma including colonization and its impacts. Other sources of trauma were coping with the grief and loss of peers and family and the high turnover of staff at health and social service organizations. Qualitative data were obtained from focus groups with community members who accessed the Niiwin Wendaanimak programme and from key informant interviews with staff and peers. Interview guides included questions on defining cultural safety and understandings of cultural safety. A thematic analysis of the interview data was guided by an advisory council, which included Indigenous Elders and Indigenous service users.
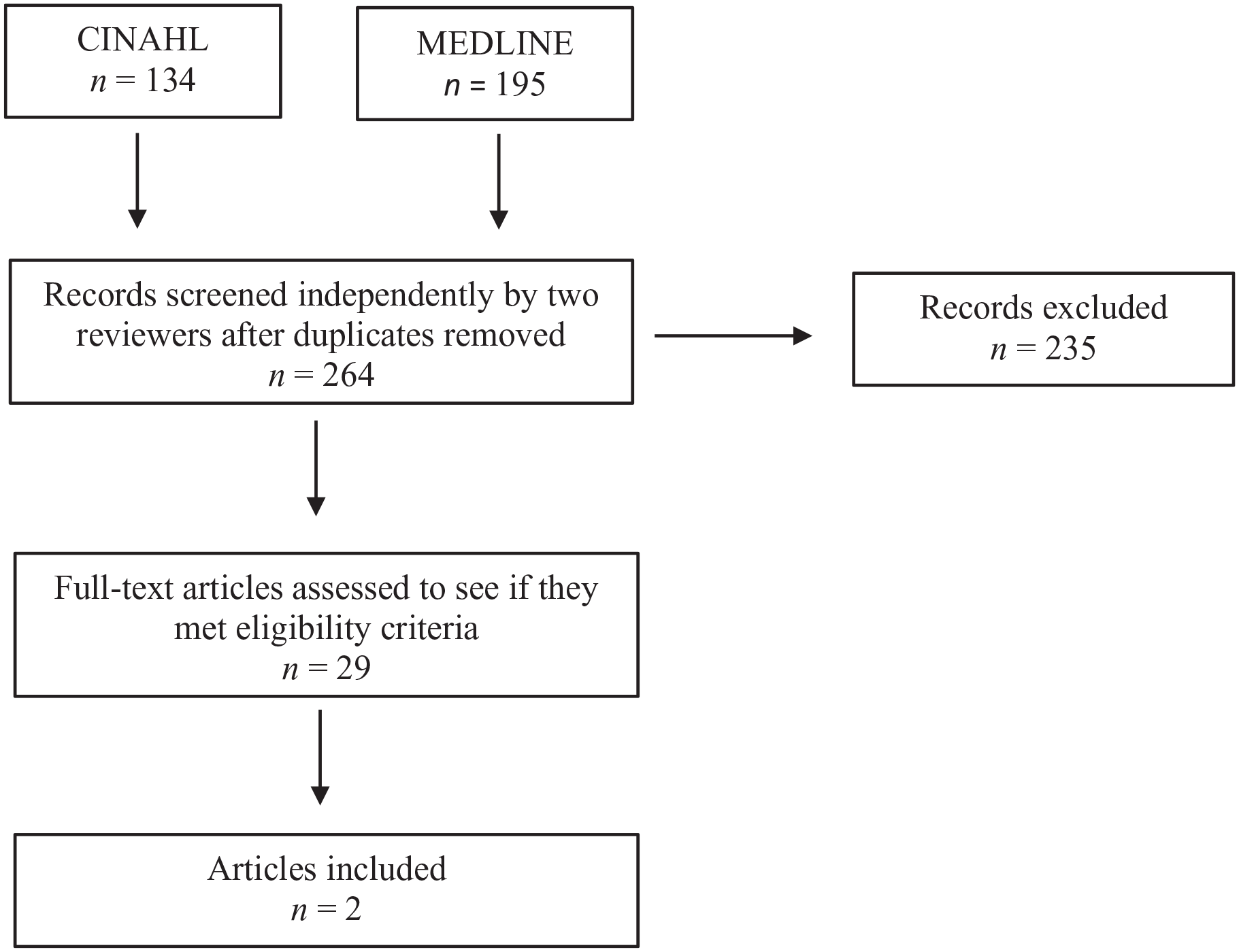
PRISMA flow diagram.
The other study was a qualitative evaluation of an Indigenous-focused midwifery practice, the Seventh Generation Midwives Toronto (SGMT) (Churchill et al., 2020). SGMT welcomes both Indigenous and non-Indigenous clients and has Indigenous and non-Indigenous midwives on staff. It trains student-midwives with priority placements for Indigenous students; includes Indigenous teachings, practices and protocols in the care of Indigenous clients; and supports families to reflect on the importance of culture and tradition. The study thematically analysed qualitative interviews with Indigenous and non-Indigenous clients participating in SGMT to explore how they conceptualized cultural safety and experiences of culturally safe care. Cultural safety was explained to participants as “what makes you feel comfortable, respected and able to be yourself.”
Cultural safety domains that create a safe, high-quality, patient-centred approach to health programming for Indigenous peoples in health care settings in Canada
Cultural safety domains were identified from the evaluated programmes from the systematized review (Churchill et al., 2020; Firestone et al., 2019), the scoping review by Brooks-Cleator et al. (2018) and four grey literature sources: two documents from Northern Health, which is a regional health authority of the province of British Columbia with a focus on Indigenous peoples’ health providing health care and support services to residents of the Northern regions of the province (Northern Health, 2015, 2017); one document from Wabano Indigenous Centre for Excellence in Health care Services in the Province of Ontario (Wabano Centre for Aboriginal Health, 2014); and, one document from HealthCareCan, an organization delivering products and services in support of health system innovation and transformation to health care organizations and hospitals across Canada (Richardson & Murphy, 2018). One Northern Health document described a thematic analysis of Indigenous patient journeys with the health system as detailed by Aboriginal Health Improvement Committees across the Northern part of the British Columbia. It identified strengths and opportunities for health system improvements from the patient’s point of view (Northern Health, 2015). The other Northern Health document described cultural safety domains for Indigenous peoples in health care settings (Northern Health, 2017). The Wabano Indigenous Centre for Excellence in Health care Services document summarized (a) the findings from focus groups with service providers and Indigenous community members in Ottawa, Ontario, about cultural safety and (b) a literature review of cultural safety resources (Wabano Centre for Aboriginal Health, 2014). The HealthCareCan document summarized cultural safety information from a literature review, interviews with key stakeholders and case studies of several health care organizations, under the advice and guidance of an Indigenous peoples’ Health Steering Committee (Richardson & Murphy, 2018).
The four cultural safety domains derived from these sources were patient empowerment; patients are supported to draw strength from their Indigenous identity, culture and community; health care workers provide trauma-informed care; and Indigenous leadership, decision-making and health governance. Members of the Wâhkohtowin Research Group, including Elders, endorsed the domains and elements as authentic from a Maskwacîs perspective. There were no opposing views expressed by the Elders during the discussions of cultural safety domains. Elders felt that some of the domains were already present in the Elders Mentoring Programme, including care delivery and resources that incorporate Indigenous culture; the presence of Indigenous staff and health care providers; and physical environments that incorporate Indigenous culture. They considered that other domains could easily be incorporated into the Programme as it evolves, including shared decision-making between the patient and the practitioner; clear, culturally appropriate and respectful communication directed at the individual receiving care; health care workers provide trauma-informed care; and Indigenous leadership, decision-making and health governance. Below are descriptions of each cultural safety domain as conceptualized from the sources and how the domains were applied in the two evaluated culturally safe programmes.
Cultural safety domain: patient empowerment
The patient empowerment domain acknowledges power dynamics, transfers power to the patient, examines the distribution of power, empowers the patient and has the patient assess their own experiences of safety.
Redistribution of power from health care practitioners to the patient through patient evaluation
Patients have power when they have the sole capacity to decide whether their interactions with a care provider or with the health care system are culturally safe, based on their own conceptualizations of cultural safety. They must be offered opportunities to acknowledge whether an interaction, programme or intervention is safe or not, in a way that feels comfortable to them (Brooks-Cleator et al., 2018; Wabano Centre for Aboriginal Health, 2014). Organizations or programmes can implement formal policies and procedures for both employees and patients to report culturally unsafe experiences and practices, to track breaches in cultural safety that could help to limit or eradicate future incidents and to track progress in achieving cultural safety (Northern Health, 2017; Richardson & Murphy, 2018). Both the Niiwin Wendaanimak programme and SGMT asked clients if the programmes were culturally safe as part of programme evaluation; however, neither programme discussed if client evaluation of cultural safety was an inherent part of the programme.
Shared decision-making between the patient and the practitioner
The recipients of care, either Indigenous patients or clients of a health care service or programme, must get the support they need to have personal agency for their health care by being included in decision-making and feeling free to ask questions. Health services and care should be client-driven, where patients share in decision-making with practitioners. Patients should feel free to voice their perspectives, ask questions and be respected by the care professional for their beliefs, behaviours and values (Brooks-Cleator et al., 2018). Health services need to facilitate the involvement of the patient, the patient’s family and others (for example, community Elders, Indigenous cultural navigators and interpreters) as needed in care-team meetings, so that the patient can make informed decisions about their care (Richardson & Murphy, 2018). Practitioners should ask patients if they feel comfortable in their understanding of the situation, or what would make their understanding easier (Wabano Centre for Aboriginal Health, 2014).
Shared decision-making was a major aspect of the Niiwin Wendaanimak programme and SGMT. A client-centred approach was used in both programmes whereby patients felt respected and supported in their life and health choices, health practitioners supported patients in their health decisions without judgement or coercion and the practitioner advocated on the patient’s behalf. In the SGMT, health practitioners involved family members, established trust with patients and ensured that patients did not feel rushed and that they received individualized support. Practitioners gave enough information to patients so that they could make informed decisions, which were then honoured. Clients felt safe when they knew what to expect physiologically and what options were available.
Clear, culturally appropriate and respectful communication directed at the individual receiving care: patients must be able to make informed decisions about their health care based on access to information that is communicated in their own language and in a non-intimidating way that they can understand. Clear, culturally appropriate and respectful communication directed at the individual receiving care can be done using patient navigators, by providing services in Indigenous languages, having translators and using plain language in written and oral communication so that technical language and medical terms are replaced with clear, simple and easily understood terms (Richardson & Murphy, 2018; Wabano Centre for Aboriginal Health, 2014). In the SGMT. the practitioner used accessible language and inclusive language, such as pronouns for the LGBTQ population, to communicate information so that the patient could make an informed health decision. The Niiwin Wendaanimak programme used non-stigmatizing language to support their patients.
Cultural safety domain: patients are supported to draw strength from their Indigenous identity, culture and community
In this domain care delivery and physical environments must both reflect and respect local Indigenous communities and cultural values. Therefore, to provide culturally safe care, organizations implementing health initiatives must alter standards to support Indigenous cultural values and norms.
Care delivery and resources incorporate Indigenous culture
Care delivery and resources that incorporate Indigenous culture provide patients with welcoming, inclusive environments where Indigenous culture is celebrated, respected, acknowledged and accommodated. Patients must be supported if they request traditional Indigenous healing practices and ceremony. For example, smudge by burning traditional medicinal plants and spiritual expression, if they desire them. Greeting clients in their Indigenous language is one way to incorporate Indigenous culture (Wabano Centre for Aboriginal Health, 2014) as is serving Indigenous food (Richardson & Murphy, 2018). Care providers must acknowledge the client’s Indigenous identity and positionality, such as traditional, transitional, colonized or bicultural, without judgement (Wabano Centre for Aboriginal Health, 2014). To make this possible, care providers must honour and respect traditional approaches to health and healing and be willing to work with traditional knowledge keepers, empower Indigenous experts and support traditional medicine and healing. Ideally, Indigenous practitioners, Elders or cultural helpers would be present to support patients (Richardson & Murphy, 2018; Wabano Centre for Aboriginal Health, 2014).
There were examples of this element in the Niiwin Wendaanimak programme and the SGMT. Both programmes included and valued Indigenous practices such as ceremony, included Elders in programming and offered Indigenous healing methods. There were opportunities for patients to practice and celebrate their culture and to feel connected and supported in their culture and community. Having access to cultural and spiritual supports such as Indigenous knowledge, teachings and ceremony from Indigenous community members and Elders made the programmes feel culturally safe to patients. In the SGMT, a core value of the clinic was to support cultural expression and respect Indigenous patients. Clients had access to Indigenous knowledge, protocols, teachings, ceremonies and medicines. Practitioners treated cultural practices as normal and patients therefore felt safe to celebrate them. The Niiwin Wendaanimak programme held community events at clinics and had Indigenous-only time and places to share, pray or sing.
Presence of Indigenous staff and health care providers
Health care organizations and programmes should recruit, retain and mentor Indigenous staff, for example, receptionists and health care providers, for example, nurses, physicians, registered dietitians and occupational therapists, at all levels of the organization. The health care environment needs to be optimized to ensure that Indigenous staff can thrive (Richardson & Murphy, 2018). Having Indigenous staff and health care providers made both the Niiwin Wendaanimak programme and SGMT culturally safe. Thematic analysis of qualitative interviews related to SGMT indicated that having Indigenous midwives as part of the SGMT made their clients feel connected to their community. It was comforting for clients to have a shared history with their practitioner. Indigenous midwives therefore had a robust and positive impact on the health and wellbeing of programme clients.
Physical environments incorporate Indigenous culture
Culturally safe health care systems ensure that physical environments reflect local Indigenous communities and cultures (Northern Health, 2017; Wabano Centre for Aboriginal Health, 2014). The buildings and spaces in and around the health care setting should be designed to promote patient connectedness with their Indigenous culture and acknowledge Indigenous strengths and capabilities. Examples of this element are dedicated spaces that can be used for ceremonial purposes, medicine gardens, the use of traditional scents such as cedar, the integration of Indigenous architecture, signs and posters written in Indigenous languages and displays that include Indigenous art or symbols, such as the medicine wheel (Richardson & Murphy, 2018; Wabano Centre for Aboriginal Health, 2014). Both the Niiwin Wendaanimak programme and SGMT had dedicated spaces for Indigenous activities. The Niiwin Wendaanimak programme had Indigenous artwork in the clinic.
Cultural safety domain: health care workers provide trauma-informed care
Trauma can have long-lasting negative impacts on physical and mental health and result in the development of health-risk behaviours. Trauma includes exposure to abuse, neglect, systemic discrimination, violence, poverty and other adverse event or circumstance that are experienced by an individual as physically or emotionally harmful or life-threatening (Menschner & Maul, 2016). As such, care provider, organization, and health care system must be sensitive to how an Indigenous person’s lived experiences, and the historical and contemporary impacts of colonization, can influence health behaviours and health status of Indigenous peoples, so that a patient is not retraumatized within the health care setting (Brooks-Cleator et al., 2018; Richardson & Murphy, 2018). Care providers must learn about the role of history in shaping health (Northern Health, 2017) and listen to and seek to understand the client’s lived experiences (Richardson & Murphy, 2018). They must consider Indigenous peoples’ reactions, such as treatment refusal and possible fear and mistrust of the health care system, to be the result of previous experience, rather than just as bad behaviour or non-compliance, to create an environment where authentic questions are asked, non-judgmentally (Richardson & Murphy, 2018; Wabano Centre for Aboriginal Health, 2014). Health care organizations must make reconciliation and Indigenous peoples’ health equity part of the organization’s strategic plan, develop policies that include the social determinants of health and take appropriate disciplinary actions in cases of racism. Processes to report racism must be user friendly and accessible to patients and posters and other visual reminders about zero tolerance for racism and for reporting racism must be apparent in the health care setting (Richardson & Murphy, 2018).
Clients of the Niiwin Wendaanimak programme related their sense of safety in the programme to the non-judgemental staff who were trained in trauma-informed approaches. A harm reduction policy ensured that clients could use the programme in whatever way they would like, without force, interference, or judgement. Practitioners fully supported the patient in their health decisions. They accepted patients for who they were, treated them with respect, and met the needs of patients no matter what shape they were in. Similarly, clients of SGMT emphasized the importance of feeling respected and supported in their choices, without judgement.
Cultural safety domain: Indigenous leadership, decision-making and health governance
Culturally safe care requires health care programmes and services to partner with Indigenous organizations and communities to ensure that they have a role in health care leadership and control over decision-making, service delivery and governance. Health care organizations must commit to building trusting relationships with Indigenous partners, establish Indigenous peoples’ health committees and connect staff and programmes with Indigenous community partners (Richardson & Murphy, 2018). The Niiwin Wendaanimak programme was run by Indigenous leaders. Indigenous peoples were included in the development and governing of the programme. Programme participants expressed the importance of having a programme specifically made for Indigenous peoples, which was run and governed by Indigenous peoples.
Discussion
We identified four cultural safety domains that create a safe, high-quality, patient-centred approach to health programming for Indigenous peoples in health care settings in Canada; conceptualized how the domains could be applied in practice; and, described how the domains were incorporated into two programmes in the health care setting in Canada that had been evaluated as safe by the Indigenous recipients of care. Cree First Nations members of the Wâhkohtowin Research Group and Elders Mentoring Programme perceived the domains to be authentic from a Maskwacîs Cree perspective. The information about cultural safety domains and their application in practice could be used to support the development, implementation and evaluation of culturally safe programmes for Indigenous peoples in health care settings throughout Canada.
This research adds to knowledge about cultural safety domains for programmes for Indigenous peoples in health care settings in Canada. While a scoping review had described domains of culturally safe care in Canada (Brooks-Cleator et al., 2018), we additionally described how the domains that made a programme culturally safe were applied in practice in evaluated programmes. Key aspects of cultural safety that we identified are that programme evaluation by Indigenous clients is essential; care should be trauma-informed; recruitment and retention of Indigenous staff should be a strategic initiative of health care organizations; and, that staff must acknowledge and respect clients’ diverse Indigenous identities.
Outcomes of a culturally safe care environment include the Indigenous patient feeling comfortable, respected and safe in their cultural identity and having a sense of connection with traditional ways of knowing (Churchill et al., 2020; First Nation Health Authority of British Columbia, 2016). Inclusive language is important as it positively includes and reflects the diversity of clients in health care in an accurate and respectful way. Practitioners are encouraged to acknowledge their privilege and recognize power differences between themselves and Indigenous patients (Brooks-Cleator et al., 2018; Mackean et al., 2020). As noted by Chakanyuka et al. (2022) while the issue of addressing power imbalances is critical to culturally safe care, few interventions describe how to redistribute power between health care practitioners and individuals receiving care.
Trauma-informed care has not often been discussed in the cultural safety literature. Trauma-informed care requires the care provider to realize the impact of trauma on health and wellbeing, to recognize the signs and symptoms of trauma in individual clients, to integrate knowledge about trauma into policies, procedures and practices; and to prevent patient re-traumatization (i.e., avoid creating an environment that inadvertently reminds patients of traumatic experiences and causes them to experience emotional and biological stress) (Menschner & Maul, 2016). Trauma-informed care shifts the focus from “What’s wrong with you?” to “What happened to you?” It includes training staff in trauma-specific treatment approaches, patient empowerment where patient strengths are recognized and built on, patient choice in treatment options, collaboration among health care staff, patients and their families in organizational and treatment planning and trustworthiness where decision are made with transparency and with the goal of building and maintaining trust (Menschner & Maul, 2016).
In Canada, to provide effective health care services with a healing orientation for Indigenous patients, it is important that providers of care acknowledge interpersonal and structural violence, as well as the ongoing impact of colonization, racism and intergenerational trauma as Indigenous determinants of health along with other social, economic and political factors that impact care for Indigenous populations. Violence-informed care goes beyond trauma-informed care to acknowledge and respond to the multiple layers of trauma and violence experienced by Indigenous peoples and the intersection of colonization and racism across time and place (Cullen et al., 2022).
Application of the finding to the Wâhkohtowin Research Group and the Maskwacîs Elders Mentoring Programme
Ongoing conversations between the Elders and members of the Wâhkohtowin Research Group continue, with the aim of incorporating these domains into the evolving Programme. For instance, pilot activities are being planned based on the ideas of both Elders and Indigenous women from the community in an effort towards shared decision-making. Creating safe spaces in the Programme to support Indigenous women, such as through crafting, beading and sewing sessions, are being planned to allow women and Elders to communicate in an environment of ease and grounded in cultural activities that necessitate respect. Elders facilitating the Programme are receiving ongoing training in trauma-informed care. Finally, the Wâhkohtowin Research Group is amending their research agreement to move even more towards community empowered leadership, governance and control over the research and its related programmes. For example, all generated research data will be stored on secure servers within the community, and all programme activity funding will be held and controlled within the community.
Strengths and limitations
A strength of this research is that it included Indigenous community members involved in community health and wellbeing programmes in the authentication of cultural safety domains, including how the domains could be applied to local health care programmes (Johnson & Rasulova, 2017). The systematized review had several strengths. It had many elements of a systematic review. A librarian-guided comprehensive search strategy was followed. Researchers with long-term research relationships with Indigenous communities or who had completed systematic reviews related to Indigenous topics developed an exhaustive list of search terms. Bias in study selection, final screening and analysis were reduced through having two reviewers. The results of the rapid review have limited generalizability given that the review did not include articles published prior to 2019, it focused on Canadian content and only two programmes were included in the review. The focus on Canadian content also likely limited the descriptions of strategies and actions to support cultural safety in health care delivery. A shortcoming of the research for the development and evaluation of culturally safe programmes for Indigenous patients and clients is that domains concerned with cultural safety education and training for health care practitioners or the requirement for health organizations to mandate cultural safety and practice as a requirement for ongoing accreditation and certification at both the organizational and practitioner levels were not included.
Conclusion
Evaluation of interventions to bring cultural safety into health care practice for Indigenous peoples has only recently been reported. More evaluation of cultural safety in programmes in health care settings in Canada is required. Evaluating culturally safe care in a health care setting means giving patients or programme clients opportunities to acknowledge whether an interaction, programme or intervention is safe by having them complete formal evaluations of their care. Programme evaluation by Indigenous clients who are the recipient of care is the only way to truly define if a health programme or service is culturally safe. Client evaluation of programmes and services shifts the power from the health-care providers to patients to assess their own experiences and provides an authentic understanding of culturally safe care.
Supplemental Material
sj-docx-1-aln-10.1177_11771801251334791 – Supplemental material for A rapid systematized review of evaluated health care programmes for Indigenous peoples in Canada with First Nations authentication of cultural safety domains
Supplemental material, sj-docx-1-aln-10.1177_11771801251334791 for A rapid systematized review of evaluated health care programmes for Indigenous peoples in Canada with First Nations authentication of cultural safety domains by Ryanna Coones Long, Luwana Listener, Denise Young, Maria F Torres-Ruiz, Richard T Oster, Jessica Thorlakson and Noreen Willows in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors acknowledge the contribution of everyone who has been involved in the Elders Mentoring Programme over the years. They acknowledge the contribution of the Maskwacîs Health Services staff, and in particular Director Randy Littlechild for his guidance and support. Finally, the authors express their gratitude to the communities of Maskwacîs for their warm hospitality and support.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship and publication of this article: Alberta Health & Wellness Vulnerable Women Programme (grant no. 009472) Maternal, Newborn, Child & Youth Strategic Clinical Network of Alberta Health Services—Health Outcomes Improvement Fund 2.0.
Supplemental material
Supplemental material for this article is available online.
Glossary
Cree a culturally distinct group of Indigenous First Nations peoples, some who live in the Treaty 6 region of Alberta, Canada
Inuit Indigenous peoples of Arctic Canada
Māori the Indigenous peoples of New Zealand
Métis one of three culturally distinct groups of Indigenous peoples in Canada, primarily of mixed First Nations and European ancestry
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.