
Abstract
The objective of the study is to conduct a systematic review and methodological quality appraisal on studies reporting the development of health and wellbeing outcome measures for Māori (Indigenous people of New Zealand), identify common features and processes, and critically appraise the measures using the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN). Key databases were searched using key terms in May 2022 without date limiters. English or Māori language publications were included if they reported Māori health and wellbeing outcome measure development. Studies were then appraised using the COSMIN. Seven publications developed outcome measures and seven reported the validation of the measures. All studies were Inadequate when appraised using the COSMIN so measurement properties were not appraised. This study highlights the value of integrating Indigenous and western research methods to yield culturally relevant outcome measures, promoting equity in health and wellbeing assessment for Māori.
Introduction
Is achieving content validity the first step towards equity for Indigenous populations?
Increasing attention is being given to Indigenous and First Nations peoples’ experiences of health care, with specific references made to understanding people within their cultural context when measuring health outcomes. It is now recognised globally that assessing people devoid of their cultural identity leads to, at best, inaccurate understandings of the individual and community needs, and at worst, contributes to discrimination and perpetuates systematic disadvantage within the health care system (Gall et al., 2021). COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN), a standard for reporting psychological and or health outcome measures, makes specific reference to understanding culture as an essential part of content validity (Prinsen et al., 2018). However, it is not yet fully elucidated how researchers are to critically appraise the degree to which cultural knowledge has influenced the measurement of psychological factors. The present research will inform outcome measurement development in Indigenous populations through using measures developed in Aotearoa New Zealand with Māori (Indigenous people of New Zealand), as a case study for researchers developing and implementing measures that aim to meet the needs of Indigenous populations. We do this, first, by identifying the literature to identify health and wellbeing outcome measures developed for Māori; second, by describing the approach used to develop and test items; and, third, by appraising the publications using the COSMIN framework to understand what elements were included when developing measures for Indigenous populations. The authors wish to acknowledge that many Indigenous peoples prefer to be identified by the names of their specific nations or tribes, although these names can sometimes be sources of contention. From the literature reviewed in this study, in the Australian context the term First Nations is often used, and in the Aotearoa New Zealand context Māori is often used. Given this review is focused on the Aotearoa New Zealand context and First Nations is not in common use, we have elected to use the term Indigenous peoples when speaking broadly and Māori, specifically, for the Aotearoa New Zealand context.
Background
There is growing understanding among policy makers that to address the consistent pattern of inequitable health outcomes experienced by Indigenous populations (Anderson et al., 2016), dimensions of health and wellbeing specific to Indigenous people must be recognised, understood and applied within context. In turn, health care delivery and the evaluation of health and wellbeing must reflect outcomes valued by Indigenous populations (Gall et al., 2021; Ruru et al., 2017). Accurate outcome measurement is critical to evaluate progress towards equity for Indigenous populations, and to identify and remediate shortcomings to make appropriate decisions about health resources. Outcome measurement in the present research is defined as the systematic collection of health-related data that include quantifying the construct of interest, for example, measuring the degree to which a person experiences depression. Outcome measurement differs to a conceptual model, which describes how constructs may relate to each other and can be used as an assessment but does not quantify the construct (de Vet et al., 2011).
However, if measures of health and wellbeing used with Indigenous populations are underpinned by western philosophical constructs, holistic dimensions valued by Indigenous people may be overlooked and the validity of the outcome measure is attenuated (Gall et al., 2021).
Assessing consequential validity is crucial when evaluating outcome measurements in Indigenous populations. Consequential validity is the aspect of construct validity that “appraises the value implications of score interpretation as a basis for action as well as the actual and potential consequences of test use, especially regarding sources of invalidity related to issues of bias, fairness, and distributive justice” (Messick, 1995, p. 745). If psychological tests do not have content validity for the cultural context where they are applied, there is a greater risk of harm to Indigenous populations, particularly as psychological tests lend credibility to the interpretations made. The evolutionary biologist Gould (1981, 1996) was an early critic of psychometrics writing a scathing and erudite critique of biological determinism and the use of intelligence testing to justify racist immigration policies in the early 20th century and notions of racial superiority for the remainder of that century. Gould’s (1996) early identification of the implications of psychometrics is an example of consequential validity and is still relevant.
Content validity is arguably the most critical element influencing consequential validity, and in turn the construct validity of outcome measures as it impacts all other measurement properties. For example, internal consistency, structural validity, and interpretability are decreased by including irrelevant items (Kaplan & Saccuzzo, 2017). A concern when developing a new measure is that the measured construct may be incomplete or incorrect but still measured reliably and real change under- or overestimated due to irrelevant or missing dimensions. This is especially significant when using measures developed in western populations with Indigenous populations, as the latter often have health models that diverge from the concepts represented in the western outcome measures content. Furthermore, when content validity is low, the users may be irritated when items appear irrelevant or important questions are not asked, leading to biased or missing data from non-completion (Terwee et al., 2018). The results from the outcome measure can subsequently be used in decision-making, potentially leading to adverse effects for the individual or group of users. This in consequence can exacerbate existing health disparities by propagating inaccurate statements about treatment effects or inappropriately guiding health care decisions that are often funded and delivered by people outside of the cultural context.
COSMIN developed a methodology for evaluating the content validity of patient-reported outcome measures (PROMs) which includes evaluating the quality of the development studies and the steps taken to validate the measure (Terwee et al., 2018). The COSMIN standards identified three essential components for content validity: (a) relevance of the items to the construct and context within the population where it is intended to be used; (b) comprehensiveness, that no key aspect of the construct is missing; and (c) comprehensibility, that the users can understand the items as intended. When applying the COSMIN standards for Indigenous populations, items must represent and adequately cover the intended Indigenous model of health and be presented in a language that is congruent with the Indigenous population. This is crucial as some western models of health are individualistic and isolate physical and or mental health, and consequently outcome measures reflect these theoretical foundations. In contrast to this, culturally informed models of health such as the Māori models explored by Wilson et al. (2021) are collective, holistic and contextual which contrast western approaches that tend towards physical or mental health. Without accurately defining the dimensions of health for the cultural context, the measure will lack content validity.
The COSMIN standards for content validity (Terwee et al., 2018) were developed using a Delphi method; however, the degree to which Indigenous voices were included was not elucidated and could contribute to bias within the standards themselves. The first four rounds reported 93% of representatives were from western countries and the culture of the representatives was not reported (Terwee et al., 2018). Importantly, consensus was not reached in the Delphi study on the avoidance of cultural bias in item wording. However, reliance on validation studies to identify cultural biases is problematic as it does not compensate for shortcomings in the construct validity or reliability of the original measure (Caron, 1999). Despite potential cultural bias, the COSMIN criteria are a meaningful framework for evaluating content validity and may support Indigenous outcome measurement development. Studies using the COSMIN criteria are emerging (Jarden et al., 2023) but as yet have not explored how the COSMIN can be applied to Indigenous studies. Applying a western framework such as the COSMIN to Indigenous research requires a critical lens so as to not repeat western biases, rather to identify touchpoints with western approaches and to understand where the methods diverge and why.
This study seeks to identify commonalities in the methods used to develop culturally valid health measures used by Māori health researchers in Aotearoa New Zealand to develop outcome measures for Māori as a case study to inform international research. This means that for Māori health and wellbeing assessment, dimensions and constructs for psychological and health outcomes measures must arise from a Māori world and incorporate the cultural customs and knowledge of being Māori. The design of outcome measures developed with and for Māori has occurred within a particular contextual lens but there has not yet been a review to understand the approaches taken in population-specific measurement development. Examining methods of Indigenous outcome measurement development in Aotearoa New Zealand has international significance as the government has prioritised health care delivery for Māori to achieve equity (Minister of Health, 2023b). Māori represent 17% of the Aotearoa New Zealand population and still experience inequitable health outcomes compared with the majority Aotearoa New Zealand European population (Manatu Hauora: Ministry of Health, 2022). Despite bold attempts to progress health delivery such as through creating a Māori-specific health service with an emphasis on evaluating health outcomes (Minister of Health, 2023a), there is very little information available on how outcomes will be measured.
Objectives
Objectives were to review the approaches that have been taken to develop health and wellbeing outcome measures specifically for Māori, identify common features and processes used, and describe how measure development has aligned with COSMIN criteria through critical appraisal.
Research questions
(1) What are the health and wellbeing outcome measures that have been developed for use with Māori?
(2) What are the characteristics of the studies describing the development of health and wellbeing outcome measures?
(3) What methods have been undertaken to develop outcome measures for health and wellbeing in Māori?
Methodology
The study used a COSMIN review methodology and focused on psychometrics which are embedded in a post-positivist paradigm. Wilson et al. (2021) argue post-positivism contrasts with Indigenous worldviews and the relational orientation of Indigenous paradigms. However, the authors agreed that, first, outcome measurement is a necessary method of understanding health status and, second, outcome measurement forms part of health policy and is used for benchmarking, quality, and funding decisions. Therefore, we position our role as researchers to provide a critical lens to outcome measures and ensure that they provide the best possible and fairest information on those whom they are used with.
In this review, Kaupapa Māori (Māori research theory, practice or way of working) methodology with a whakawhiti kōrero (active discussion and negotiation) method of critical discussion was overseen by the two Māori authors (M.C. and M.R.), alongside a western approach of COSMIN systematic review. Research within Aotearoa New Zealand has two prominent streams of research, the western way of knowing and being, as outlined above, and a Māori way of knowing and being. Kaupapa Māori research is largely a collaborating philosophy and, according to Smith (1999), Kaupapa Māori research has three main elements: Māori participation, Māori partnership, and protection of Māori in development of research. Kaupapa Māori research was created out of a necessity to provide an accurate, ethically reflective representation of Māori in research (Ruru et al., 2017). Prior to Kaupapa Māori research, westernised research methods were the main modality used to embark on understanding causation of Māori challenges which some argue created physical, emotional, and cultural harm (Waiti, 2014). As such, using correct processes is central—the overall goal of Kaupapa Māori research is to uplift and provide a high quality of research that contributes to the positive development and wellbeing of Māori (Smith, 2012).
A systematic review of outcome measures was considered appropriate for identifying, appraising, and synthesising the information necessary to describe the methods used for developing measures with Māori. Review limitations include the potential to repeat biases against Indigenous populations due to the quality appraisal component being applied retrospectively to research that was undertaken before these frameworks were in common use. Furthermore, Māori researchers may have purposefully deviated from western approaches in outcome measure development due to the previous harm caused by the misapplication of positivist research methods. In light of this, we considered how the research could be undertaken with Māori at the centre, but still employ a framework that has international use and shares a common language in psychometric research (Martel et al., 2021).
Method
This systematic review and methodological quality appraisal of measures followed the COSMIN approach (Terwee et al., 2018) and was underpinned by mātauranga Māori (Māori knowledge). The review followed an a priori protocol which was pre-registered with PROSPERO (https://www.crd.york.ac.uk/PROSPERO/view/CRD42022328318). The team was composed of both Māori and non-Māori researchers and throughout the design and evaluation of research, discussion with Māori members of the team occurred.
Design
Context
Aotearoa New Zealand has a population of 5.338 million as of the 2023 Census: 68% European, 19.6% Māori, 17.3% Asian, and 8.9% Pacific (Stats NZ, 2024).
Positionality
Authors M.S., R.J., and R.S. are non-Maori and authors M.R. and M.C. are Māori. The authors are all users and or developers of health-related outcome measures and take the position that outcome measures are part of the health system and are in common use; therefore, our role as researchers is to improve their reliability and validity. While we accept that the misuse of outcome measures has caused harm to Indigenous populations, we believe that developing and appraising measures specifically for Māori is a step towards addressing health inequities.
COSMIN
The COSMIN initiative has developed comprehensive methodological guidance for systematic reviews of PROMs (Prinsen et al., 2018) to support selection of outcome measurement instruments in research and clinical practice. A COSMIN User manual provides information on conducting the 10 steps of a systematic review of PROMS, using the COSMIN Risk of Bias checklist, and making recommendations (Terwee et al., 2018). While this method is robust, the authors recognised that COSMIN is a western framework; therefore, Māori worldviews were integrated through the participation of Māori co-authors in the review. The COSMIN review has three parts: Part A, perform the literature search, Part B, evaluate the measurement properties, and Part C, select a PROM (Terwee et al., 2018). As the present research aims to identify measures and describe methods of development, Part C is not included in the present research. Part B in this study focuses on content validity from the COSMIN. Māori co-authors co-constructed the research questions and participated at each part.
COSMIN Part A, perform the literature search
We used the COSMIN systematic review methodology procedure to systematically search and select studies according to inclusion and exclusion criteria (Prinsen et al., 2018). A research librarian specialising in systematic reviews supported the development of search terms and variations, database selection, and developing and testing the search strategy. A citation chaining method was used alongside traditional database searches. The final search was conducted in May 2022 and was conducted in the following electronic databases: CINAHL (EBSCO), EMCARE, MEDLINE, PsycINFO, and SCOPUS.
Search terms
Search terms were developed, tested, and then translated across databases. Key search terms included variations of “Māori OR Māori” OR “te reo [the Māori language]” AND “outcome*” OR “psychometric*” OR “scale*” OR “measure*” OR “index” OR “indices” OR “assess*” AND “Reproducibility of results” OR “Psychometrics” OR “measurement properties” OR “Outcome Assessment” OR “Sensitivity” OR “Specificity” OR “content” OR “item” OR “validity” OR “Validation” OR “reproducibility” OR “repeatability” OR “precision” OR “variability” OR “consistency” OR “dependability” OR “stability” OR “agreement” OR “measurement error” OR “reliability.”
Record selection was based on relevance to the below inclusion criteria. Record screening and selection was undertaken by a minimum of two reviewers independently, and then consensus was gained through consultation among reviewers.
Review inclusion and exclusion criteria
Types of instruments
Instruments developed or validated for the measurement of Māori health and wellbeing as an outcome were eligible for inclusion. Health and wellbeing in the context of this study has taken an inclusive approach to include measures where their development was informed by a model of wellbeing. Therefore, the theoretical framework underpinning the measure is health-related but the measure itself may not overtly appear as health-related; for example, cultural identity is essential for good health when working in a Māori worldview, is embedded in Māori models of health, but in a western worldview does not necessarily fit a definition of health. The disparate theoretical views and definitions of both health and wellbeing led us to include instruments where domains from Māori health and wellbeing models and frameworks were evident (Wilson et al., 2021). Eligible data collection instruments included interviewer-administered, self-administered, or computer-administered. Examples included an online survey, a written questionnaire completed by an individual, or an individual’s responses to an interviewer administering the survey.
Studies were excluded if they were a translation of an existing non-Māori measure into Māori language. Measures of constructs without a health or wellbeing model underpinning them were excluded, for example, education. Studies and measures published in languages other than English or te reo Māori (the Māori Language) were excluded. Abstracts, books, and conference proceedings were excluded. Frameworks that did not have a measurement component were excluded.
Types of study design
All publications that developed outcome measures for use specifically with Māori were included, sourced from journal databases; web searches for grey literature, for example, government documents; or from searching reference lists of included studies. We also screened articles that authors had prior knowledge of that contained measure development. Articles eligible were published as full texts in English or te reo Māori. Studies were eligible if they reported the development of a psychometric measure or reported qualitative steps that later contributed to the development of a measure. Measures must be either (a) entirely new or (b) were an existing measure that was adapted specifically for Māori through including new items or removing items. Māori must be included on the authorship team alongside tauiwi (non-Māori), consulted in the article, or the authors must all be Māori. Excluded were studies that were not developing or adapting a measure specifically for Māori, or if the articles were not available as full texts or were published in an excluded language. Also excluded were articles where the authorship team were non-Māori and there was no evidence of Māori consultation or inclusion on the authorship team. This was determined through viewing author profiles and the research teams’ prior knowledge of authors, however no study was excluded on this basis.
Types of settings and participants
Studies need to include a representative sample of Māori of any age group and data collection must have occurred within Aotearoa New Zealand.
Data management
Endnote X9 was used to export references identified in execution of the search strategy. Next, references were imported to Covidence, Veritas Health Innovation Ltd for screening, removal of duplicates, appraisal against inclusion and exclusion criteria, and data extraction.
Selection process
Titles and abstracts were independently screened by reviewers (M.S., R.J., and M.C.). The full texts of potentially relevant studies were screened against the eligibility criteria by two independent reviewers (M.S. and R.J.). Conflicts were resolved through discussion and gaining consensus among the review team. Findings from the execution of the search and selection process are presented in a flowchart (Figure 1). A third reviewer (M.R.) who is Māori and has expertise in outcome measurement also completed the quality appraisal and provided guidance on the inclusion or exclusion of measures at this stage.
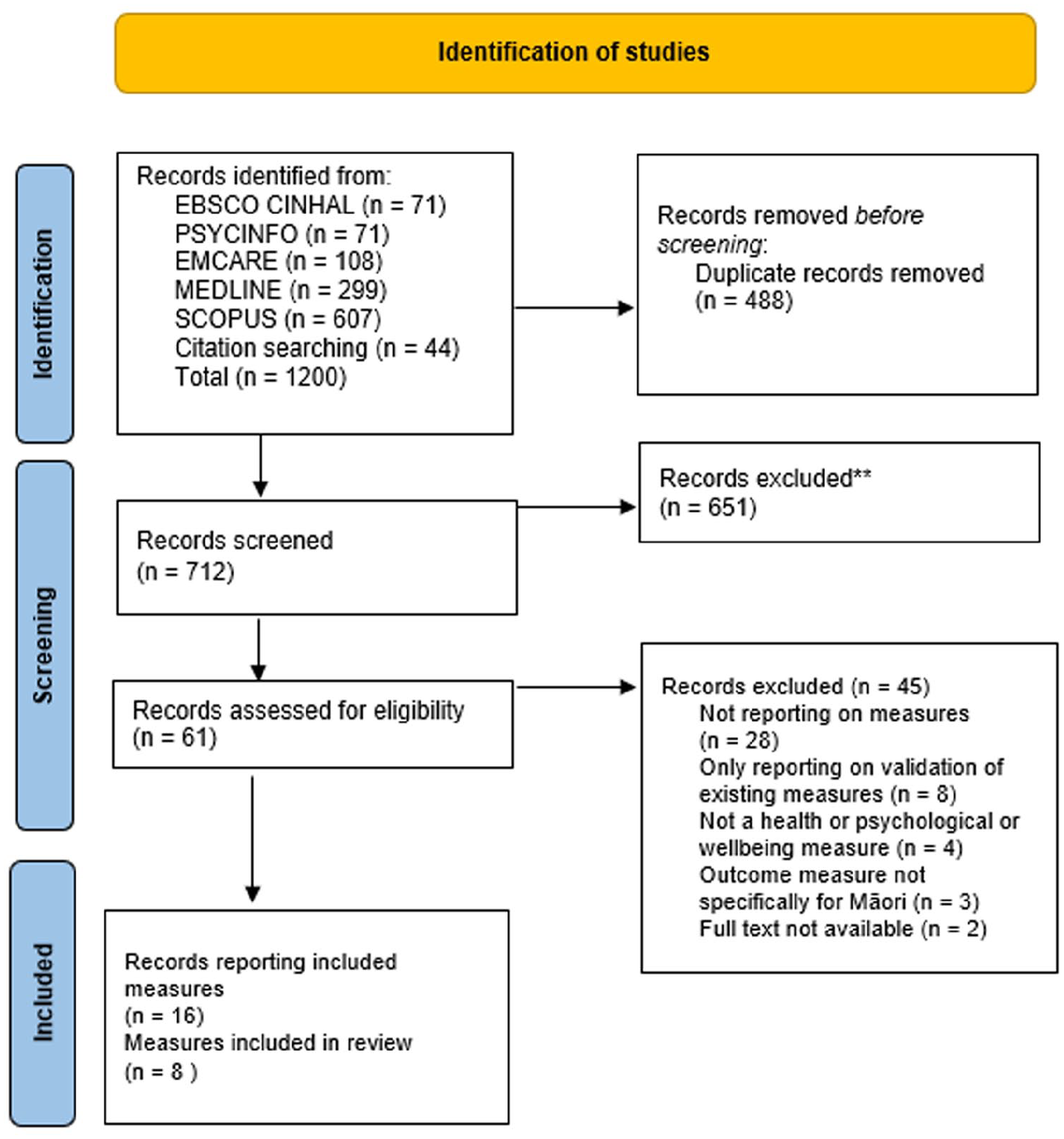
Flowchart of the search and screening process.
Data extraction
Relevant data were extracted in duplicate from the included publications and then consensus was established. When extracting data, if the article did not include relevant information, we recorded not reported.
COSMIN Part B, evaluate the measurement properties
The full COSMIN checklist (Terwee et al., 2018) progresses from content validity through to internal structure, reliability, measurement error, criterion validity, and hypotheses testing for construct validity and responsiveness. The evaluation of content validity has three steps: (a) evaluate the quality of the PROM development, (b) evaluate the quality of content validity studies on the PROM, and (c) evaluate the quality of the content validity of the PROM based on the quality and results of the previous studies along with scoring the PROM using the COSMIN criteria. Studies may be rated as very good, adequate, doubtful, or inadequate. The rating not explored was applied when any measurement properties not investigated for an instrument in any individual article. For a study to receive a very good rating, the study must be methodically sound with adequate sample size and appropriate methods. Given in the present research no studies progressed past part A of the COSMIN, methods pertaining to parts B and C of the COSMIN are not described here.
Data analysis process
The findings from the search are illustrated in a flowchart (Figure 1) and the characteristics of the included studies are presented in Supplementary Material 1. The COSMIN methodology for systematic reviews of PROMs (Prinsen et al., 2018) was followed along with the COSMIN Risk of Bias assessment. The COSMIN checklist progresses through numbered boxes, for example, box one refers to PROM development reviewers independently appraised studies against the COSMIN PROM development criteria. Reviewer consensus occurred through discussion.
Results
The study search took place in May 2022. Database searches yielded 1156 publications, and 44 additional publications were sourced from citation searching. A flow chart of the search and screening process is illustrated in Figure 1.
Of the publications identified from databases, 488 were duplicates, and the remaining 712 articles were title and abstract screened, from which 61 manuscripts were full-text screened. The majority of the 45 reports that were excluded were due to not reporting on measures (n = 28), eight were validating existing measures, and the remainder were not reporting on health or wellbeing measures (n = 4), were not for Māori (n = 3), or full texts were unavailable (n = 2). Sixteen publications reported eight measures of Māori health and wellbeing. Of these, one measure had two revisions, and one had one revision. No study was excluded due to the absence of Māori on the research team.
Characteristics of outcome measure development studies
The 16 publications reporting outcome measure development studies used both western and Māori approaches to develop and refine the outcome measures. The supplementary materials present a summary of the development studies describing the aims, population, participant characteristics, sample size, and funding sources.
Studies ranged in aim from exploratory work informing item development, to pilot testing and to validation of a measure. Most studies included only Māori participants, and two also included non-Māori participants. Eight studies reported funding. No study declared a conflict of interest.
Characteristics of measures developed
All measures (Table 1) were developed using constructs that related to models of health and wellbeing for Māori. Constructs predominantly were from a Māori worldview but some measures also included western concepts alongside Māori (Stewart & Gardner, 2015). Cultural identity and culturally specific constructs were commonly included and few measures included physical health. Māori concepts of wairua (spirituality) (Elder et al., 2017; Houkamau & Sibley, 2010; Lindsay et al., 2021, 2022; Palmer, 2004) and whānau (extended family) (Matika et al., 2020; Palmer, 2004; Tamati et al., 2021) as impacting on health were evident from the inclusion of these constructs in several measures. Methods used to develop items were predominantly literature review and expert opinion, drawing items from concepts known to the authors or from their previous studies. A study by Lindsay et al. (2022) was the only study to elicit constructs from participants for a scale and go on to develop a measure with this information. The studies which undertook a refinement of the developed measure with participant feedback did so in an unstructured and spontaneous way which did not meet the stringent COSMIN criteria. These methods included generally asking what they thought about the measure, for example, the Waka Huaka (Elder & Kersten, 2015), or by editing based on comments on the measures in the emails that accompanied returned surveys, for example, the MMM-ICE (Houkamau & Sibley, 2010).
Characteristics of measures and development phases.
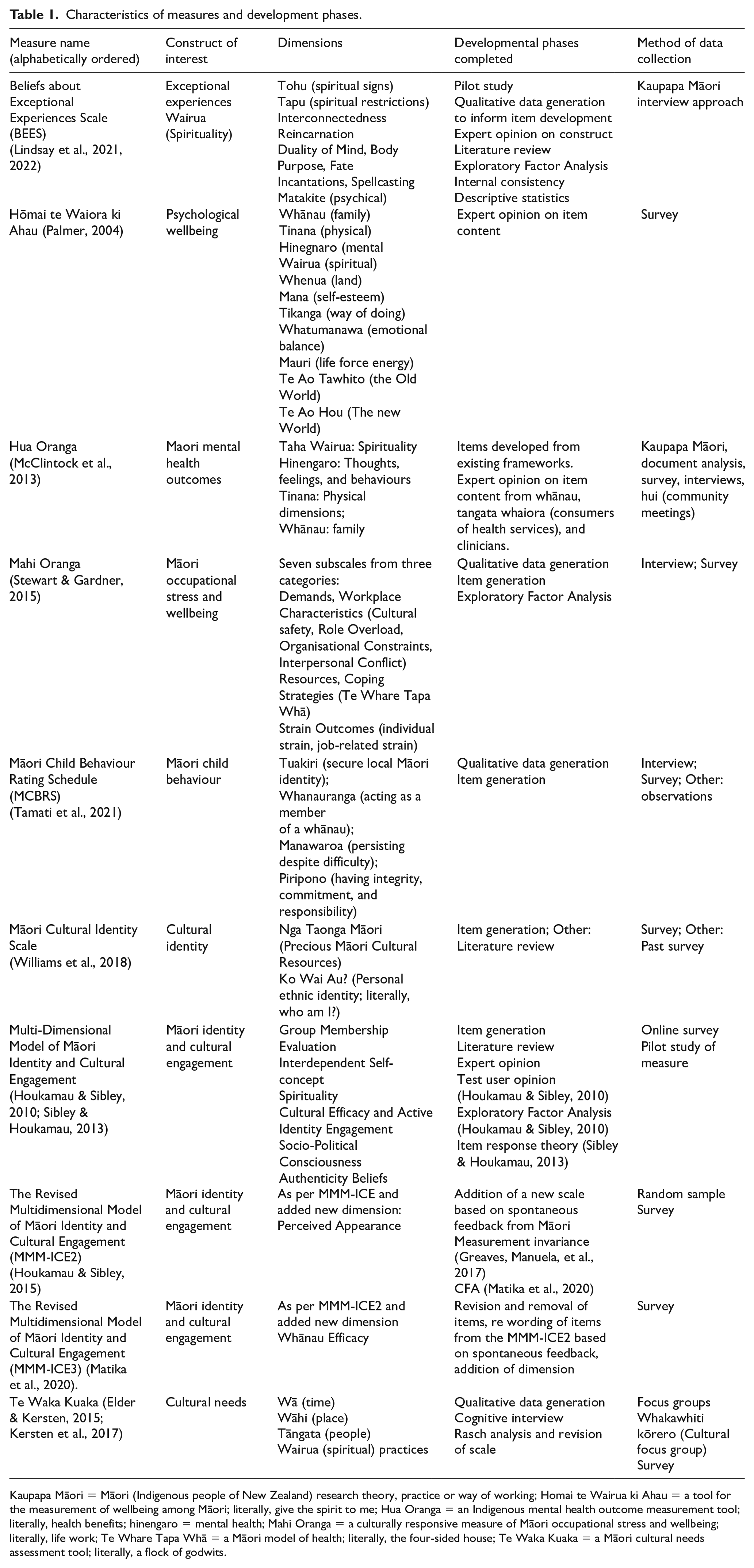
Kaupapa Māori = Māori (Indigenous people of New Zealand) research theory, practice or way of working; Homai te Wairua ki Ahau = a tool for the measurement of wellbeing among Māori; literally, give the spirit to me; Hua Oranga = an Indigenous mental health outcome measurement tool; literally, health benefits; hinengaro = mental health; Mahi Oranga = a culturally responsive measure of Māori occupational stress and wellbeing; literally, life work; Te Whare Tapa Whā = a Māori model of health; literally, the four-sided house; Te Waka Kuaka = a Māori cultural needs assessment tool; literally, a flock of godwits.
Quality appraisal of measure development
The COSMIN standards (Terwee et al., 2018) can either give an overall rating for PROM development using the worst score counts method, or a rating for specific parts of the checklist. Instead of the worst score counts method, we chose to separately rate the concept elicitation, total PROM design, and the cognitive interview study. For box two as per the COSMIN recommendation, we report overall ratings per sub-study separately as not all studies have been completed for the measures reported here.
With the exception of the Beliefs About Exceptional Experiences Scale (BEES) (Lindsay et al., 2021), all measures were developed prior to the publication of COSMIN and consequently the criteria were applied retrospectively. No study referenced the COSMIN. The initial stages of the concept elicitation study quality (items 1−5) for the studies were rated very good (Table 2); the remaining two studies were inadequate as they did not clearly define the construct, for example, cultural identity in Williams et al. (2018), or did not involve the target population (Houkamau & Sibley, 2010). All studies except one included the intended test-users in the development phases. Studies that undertook a pilot study (n = 1) or cognitive interview (n = 1) were rated as inadequate or doubtful quality due to not detailing methods that would raise the rating, for example, Elder and Kersten (2015) reported a method called whitiwhiti kōrero (cultural interview similar to a cognitive interview), but the COSMIN score was inadequate as the study did not report systematically asking participants about the comprehensiveness or comprehensibility of the measure (see Terwee et al., 2018, p. 41). Although Elder reported adjusting the measure following the feedback from the study, the final measure did not repeat the cognitive interview phase as required in COSMIN. Studies that conducted a pilot did not include asking users about content (Table 2) and instead conducted exploratory factor analysis, descriptive statistics, and internal consistency (Lindsay et al., 2021; Stewart & Gardner, 2015).
Quality appraisal of the measures.
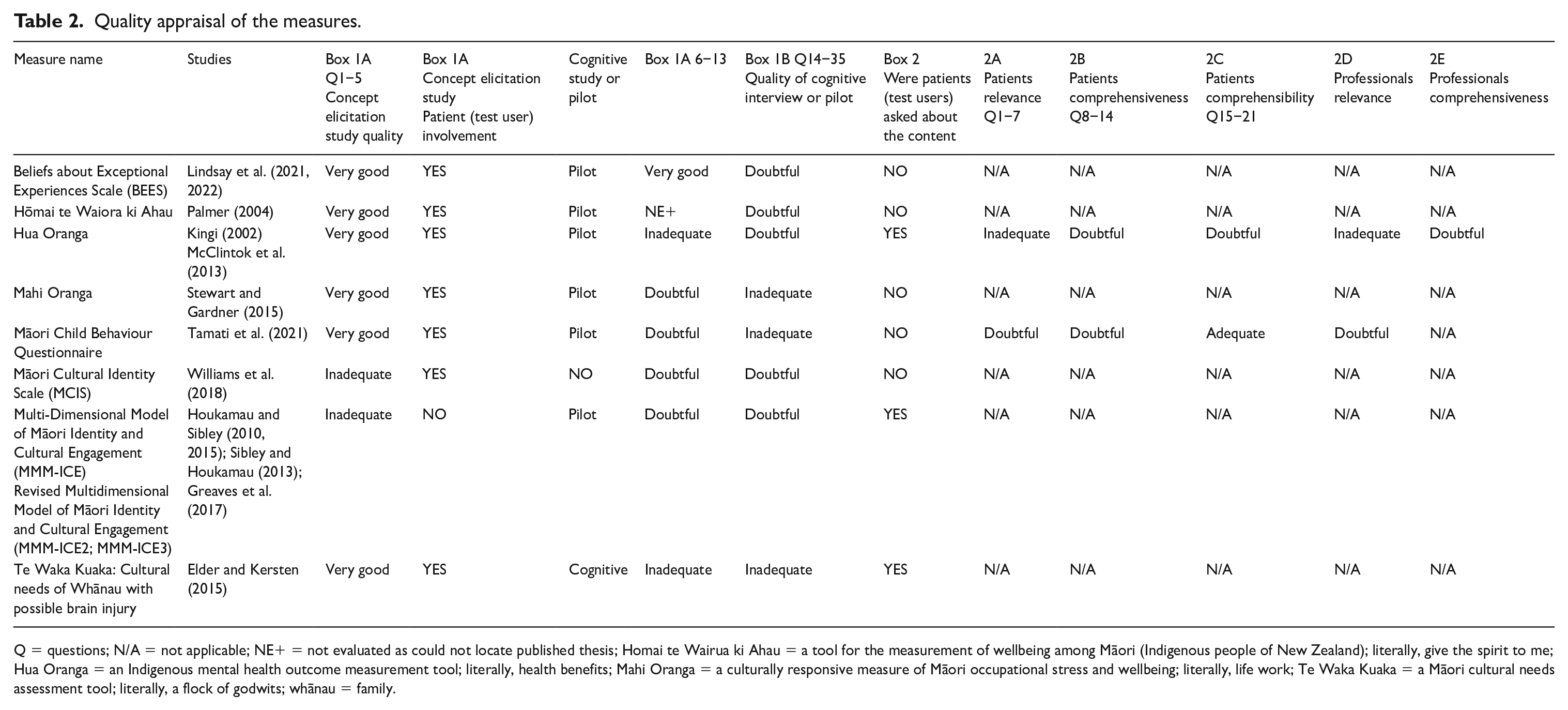
Q = questions; N/A = not applicable; NE+ = not evaluated as could not locate published thesis; Homai te Wairua ki Ahau = a tool for the measurement of wellbeing among Māori (Indigenous people of New Zealand); literally, give the spirit to me; Hua Oranga = an Indigenous mental health outcome measurement tool; literally, health benefits; Mahi Oranga = a culturally responsive measure of Māori occupational stress and wellbeing; literally, life work; Te Waka Kuaka = a Māori cultural needs assessment tool; literally, a flock of godwits; whānau = family.
The quality of the outcome measure design and item development phase (Box 1A, 6−13) were mainly inadequate or doubtful, with two studies rated very good. Lower rated studies often had insufficient descriptions of their interview guides, coding, data analysis, training of the interviewers, and did not report who undertook the analysis and the methods. In some studies experts were asked for their opinions on test content and wording in the initial development stage, but this was inadequately described to evaluate and did not map onto items of the COSMIN, which is why some studies were rated very good but did not progress within the box. Elder and Kersten’s (2015) was the only measure that progressed to box 2 of the COSMIN which appraises the quality of content validity studies; however, it was not clear whether users were asked the necessary questions to ascertain the comprehensiveness and comprehensibility of the PROM.
Evidence synthesis
No high-quality evidence was available for the measures included in the study, and thus using the COSMIN it was not possible to establish which measure had the best content validity.
Expert review
To align with a mātauranga Māori approach, we undertook an expert review of the measures to establish the strengths of the measure development process. (Stewart & Gardner, 2015) study was identified as having a sound approach to development as it was rooted in theory, employed qualitative item generation with the target population, used mixed qualitative and quantitative approaches, and the entire Māori sample was taken from a range of organisations and professions.
Discussion
This research sought to review previous approaches to develop health and wellbeing outcome measures for Māori, identify common features and processes used, and describe how measure development has aligned with COSMIN criteria through critical appraisal. Of the published health outcome measures, few had subsequent validation studies. The domains measured included domains such as cultural identity (Houkamau & Sibley, 2010), cultural needs (Elder & Kersten, 2015), spirituality (Lindsay et al., 2021), child behaviour (Tamati et al., 2021), and healthy workplaces (Stewart & Gardner, 2015). The measures highlight the importance of the Indigenous cultural practices and beliefs as forming part of the measure of health. Several studies were excluded that provided assessment frameworks but were not measures as they did not quantify the dimensions. For example, the Meihana Model was described as a clinical assessment framework (Pitama et al., 2007) which uses the qualitative domains of tinana (physical wellbeing), hinengaro (consciousness and awareness), iwi katoa (wider support), wairua (spiritual wellbeing), and taiao (environmental wellbeing).
Outcome measures are in common use within psychology in Aotearoa New Zealand, yet this study found only a small number have been developed with Māori participants for Māori. The COSMIN is a relatively new framework for developing and evaluating measures and as such was applied retrospectively for all but one of the measures identified. The measures identified were all in the early stages of development, with one (Houkamau & Sibley, 2010) that had progressed past the initial development and piloting of items to multiple scale revisions, but these studies did not meet the quality standards of COSMIN. Few measures had been cited in further research, suggesting an ongoing preference for western measures or unpublished measures, or qualitative methods in health research with Māori.
Drawing together the western psychometric and Kaupapa Māori worldviews of research was fundamental to this study. As such, we considered “touchpoints” in developing this review (Haar et al., 2019). The concept of touchpoints is used to understand Kaupapa Māori (Māori cultural values) that relate to similar but not necessarily identical western concepts while remaining true to Māori values. We acknowledge that direct translations between western and Indigenous perspectives are not always possible (Haar et al., 2019; Ruwhiu & Elkin, 2016), but may provide different ways of seeing the world. Cognitive interviewing can be aligned with Indigenous methodologies, for example, whitiwhiti kōrero (Elder & Kersten, 2015), yarning (Byrne et al., 2021), and talanoa (Vaioleti, 2013). The whitiwhiti kōrero method was used in the Te Waka Huaka (Elder et al., 2017) measure development whereby community members were invited to give feedback using hui (community meetings) where kōrero (discussion) takes place, and pūrākau (reflection upon on experiences) which are incorporated to explore understanding. In these methods, the researcher must be able to work within the cultural context and understand the interactions, and the non-interactions or spaces of silence, as well as the hierarchical dynamic of the room and the spiritual context of the discussion. These methods are often undervalued when assessed against the western criterion of validity. In our study, the quality rating given for this method was lower due to the non-directed way of gathering information. However, further refinement of the reporting of methods would enable the COSMIN criteria to be met while holding true to Māori principles.
Kaupapa Māori is a unique methodology and is Indigenous led and as such does not currently fall into the traditional content validity methods. However, we feel it offers an opportunity to strengthen traditional western psychometric approaches, as power differentials between the researcher and phenomenon being researched may be addressed through the processes within the methodology, and there is likely to be greater depth. Furthermore, Kaupapa Māori offers a spiritual “bookending” of the research process which for Māori enables more comfort in sharing phenomena related to health, as spirituality and physical health are intertwined. Research developing outcome measures using Kaupapa Māori approaches are emerging (Elder & Kersten, 2015; Lindsay et al., 2021; Menzies et al., 2022).
Achieving content validity may be the first step towards equity for Indigenous populations
The measures identified in the study were predominantly based around cultural identity and experiences and while had a health lens, these could not presently be used as stand-alone measures for health outcomes. We do not yet have a sufficiently validated measure that relates to a health phenomenon that uses a Māori lens; instead, we are left with using western measures and supplementing them with cultural identity tools. This practice when health practitioners are burdened with administration may mean that cultural measures are overlooked, and furthermore, may not have meaningful outcomes for Māori. Measures should be purposeful and have clinical utility for the practitioner, but have meaningful content for the test user. When considering holistic Māori views of health where spirituality, physical, mental, and family health are equal, health outcome measurement should cover all of these domains. While there have been health outcome measures developed for Māori, these have not been specifically mentioned in the Ministry of Health documentation as a means to evaluate if health equity has been reached. Furthermore, we have made little progress from Palmer’s (2005) assertion that wellbeing measures were “not responsive to the needs of Māori, are not based on Māori concepts or constructs” (Palmer, 2005, p. 87).
Strengths and limitations
The subjective nature of health and the broad definitions and models of health and wellbeing meant the inclusion criteria of wellbeing measures at times were difficult to apply. To overcome this, we used the review of Māori models of health by Wilson et al. (2021) to identify constructs that from a Māori lens were health-related, such as cultural identity. The systematic approach drawing from the COSMIN methodology and Kaupapa Māori together provided a culturally sound means of progressing outcome measures research for Indigenous populations. The authentic partnership and diversity of the authorship team in terms of both culture and methodological knowledge strengthened the review. The authentic inclusion of Indigenous partners when developing measures is essential yet the degree of partnership is not always overtly identifiable when reviewing published papers.
The selected databases and search terms potentially limit the identification of relevant studies; however, to reduce this likelihood, we consulted with a librarian, undertook forward and backwards citation searching, and used authors’ knowledge of Māori researchers working in outcome measurement to identify publications that may have been overlooked. For example the Nohi (an online health assessment platform) wellness tool (Pursuit Limited, 2024) which was published on the internet and used in the Aotearoa New Zealand community but the psychometric development was unpublished and thus was not eligible for inclusion. Furthermore, we found frameworks that described phenomenon but did not quantify outcomes, and thus were outside of the scope of the study, such as, the Meihana Model (Pitama et al., 2007). The nature of a time-limited review is that there are potentially updates that occur over time that were not captured here. We were dependent on measures to have been reported to the public domain and searchable online.
Future research
Most of the measures in this study were developed prior to when the COSMIN methodology was published, however, the methodology provided a framework to consider the touchpoints with western measure development. The COSMIN methodology provided little information on the specific considerations with Indigenous or culturally specific measures. The touchpoints in this study provide an entry point into discussion with Māori outcome measure developers to identify common factors and necessary processes when developing outcome measures for use with Māori. Expert review to contextualise the use of COSMIN methodologies for Indigenous populations may strengthen newly developed outcome measures for Indigenous people. We recommend authors describe the ways in which Indigenous partners are included to help determine the level of cultural responsivity of the measure.
Conclusion
This study highlights the benefit of drawing together Māori and western research methods. While western approaches have a strong psychometric history rooted in post-positivism, there is a tendency to overlook contextual factors and the culture of the researcher in shaping the outcome measure. Kaupapa Māori, in contrast, pays attention to contextual and researcher factors with a qualitative lens. Kaupapa Māori psychometrics enables the strengths of both Kaupapa Māori and western psychometrics to be leveraged to develop culturally appropriate outcome measures. In turn, health and wellbeing−related outcome measures can be responsive to the needs of Māori and enable the measurement of health and wellbeing objectives important to Māori. Accurate and culturally responsive outcome measurement is an essential step on the journey towards equity. The methodology underpinning the development and refinement of outcome measures for Indigenous populations must reflect the value systems such as collectivist knowledge systems. For this to occur, the measures must be developed from the ground up with Indigenous knowledge and participation at the centre.
Supplemental Material
sj-docx-1-aln-10.1177_11771801251334176 – Supplemental material for Decolonising outcome measurement: a systematic review of health and wellbeing measures for Māori
Supplemental material, sj-docx-1-aln-10.1177_11771801251334176 for Decolonising outcome measurement: a systematic review of health and wellbeing measures for Māori by Margaret Sandham, Maree Roche, Melissa Carey, Richard J Siegert and Rebecca J Jarden in AlterNative: An International Journal of Indigenous Peoples
Footnotes
Acknowledgements
The authors acknowledge the contributions of Dr. Louise Cowpertwait (CEO, MindMatters) in data collection and preparation, and Mr. Andrew South (Research Librarian, Auckland University of Technology) in developing and testing the search strategy.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors received no financial support for the research, authorship, and publication of this article.
Supplemental material
Supplemental material for this article is available online.
Glossary
hinengaro mental health
kaupapa Māori Māori research theory, practice, or way of working
kōrero discussions
Ko wai au? personal ethnic identity; literally, who am I?
Homai te Wairua ki Ahau a tool for the measurement of wellbeing among Māori; literally, give the spirit to me
Hua Oranga an Indigenous mental health outcome measurement tool; literally, health benefits
hui community meetings
Mahi Oranga a culturally responsive measure of Māori occupational stress and wellbeing; literally, life work
mana self esteem
manawaroa persisting despite difficulty
Māori Indigenous people of New Zealand
matakite psychical
mauri life force energy
ngā taonga Māori precious Māori cultural resources
Nohi an online health assessment platform
piripono having integrity, commitment, and responsibility
pūrākau reflection upon on experiences
taha wairua spirituality
tāngata people
tangata whaiora consumers of health services
tapu spiritual restrictions
te ao hou the new world
te ao tawhito the old world
te reo; te reo Māori the Māori language
Te Waka Kuaka a Māori cultural needs assessment tool; literally, a flock of godwits
Te Whare Tapa Whā a Māori model of health; literally, the four-sided house
tikanga way of doing
tinana physical, physical dimension, physical wellbeing
tohu spiritual signs
tuakiri secure local Māori identity
wā time
wāhi place
wairua spirituality; spiritual; spiritual wellbeing
whakawhiti kōrero active discussion and negotiation; cultural interview similar to a cognitive interview
whānau extended family; family
whanauranga acting as a member of a family
whatumanawa emotional balance
whenua land
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.