
Abstract
Chronic pain is one of the most common long-term conditions in Aotearoa (New Zealand), and there is a higher prevalence and greater impact of pain for Māori (Indigenous People of New Zealand). Māori tend to have a more holistic interpretation of pain compared with Western views; therefore, current assessments may not capture the full meaning and impact of pain for Māori. This study developed a holistic assessment tool for chronic pain in collaboration with Māori clinicians and Māori with chronic pain. The Pictorial Representation of Illness and Self Measure–Aotearoa (PRISM-A) is a verbal and visual assessment tool that is based on Te Ao Māori (Māori world), imbeds whakawhanaungatanga (relationship formation) between the patient and clinician, and incorporates Te Whare Tapa Whā, a Māori model of health. The tool is likely to provide a more meaningful assessment of pain and facilitate better outcomes for Māori with chronic pain.
Introduction
Chronic pain is one of the most prevalent health conditions in Aotearoa (New Zealand), impacting 21% of the adult population (Ministry of Health, 2023), and the estimated annual costs are greater than those for diabetes, dementia, or smoking (Moore & Davies, 2018). There are ethnocultural differences in pain prevalence and experience within Aotearoa, likely stemming from the ongoing impact of colonisation and inequalities in sociopolitical factors related to the determinants of health. Of significance, Māori (Indigenous People of New Zealand) experience a higher prevalence of chronic pain compared with non-Māori (Ministry of Health, 2023) and the impact of pain tends to be greater in Māori compared with people of British and/or European descent, particularly in measures of pain-related distress and disability (Lewis & Upsdell, 2018). People who identify as Asian and Pacific face a similarly high impact of pain (Lewis & Upsdell, 2018).
Pain management health services provide important mitigating effects on pain burden. In Aotearoa, management of chronic pain is rather fragmented. Patients may be managed solely by their general practitioner or seek or be referred to public or private chronic pain services, which offer various levels of multidisciplinary care. While multidisciplinary pain management programmes are the current recommended gold standard for management of long-term nonmalignant pain, there is evidence internationally to suggest these services are often not designed to meet the needs of non-Western populations (Brady et al., 2017). In support of this international evidence, there are inequities in outcomes from our chronic pain services in Aotearoa, with Māori, Asian, and Pacific people experiencing disproportional rates of poor outcomes following treatment (Lewis et al., 2021). Of note, across a national database, Māori experienced significantly worse outcomes compared with Pākehā (New Zealander of British or European descent) descent on almost all clinical measures at 3 months after treatment for chronic pain (Lewis et al., 2021). These data indicate a need for better understanding and management of pain for Māori as it is inadequately addressed by current services.
Research in Aotearoa and overseas has consistently identified that Western-based health care services, including those specific to pain management, often give rise to poor communication, poor responsiveness to spirituality and other cultural meaning-making, and lack validated assessment tools that are inclusive of additional cultures and health models (De Silva et al., 2019; Jimenez et al., 2011; Lin et al., 2018; Palmer et al., 2019; Yoshikawa et al., 2020). These issues contribute to reduced rapport with clinicians, which itself impedes health outcomes (Palmer et al., 2019). Specific to Aotearoa, a recent review identified a lack of culturally appropriate tools to capture interpretations and experiences of pain for Māori, and identified a need for such a tool so that clinicians can provide more appropriate care and management of pain for Māori (Hoeta et al., 2020).
The Pictorial Representation of Illness and Self Measure (PRISM) is a reliable, pictorial-based assessment tool that has been shown to provide a holistic assessment of suffering across several health conditions, including chronic pain (Brady et al., 2019), and in several non-Western cultures (Sensky & Büchi, 2016). The pictorial nature of the assessment and the narrative associated with it are designed to reduce communication barriers associated with questionnaire-based assessments (De Silva et al., 2019). In the original version of the tool, a white piece of paper is used to represent the patient’s life. A disc, termed the self-disc, is placed in the corner to represent the patient’s self. The patient is asked to place a second disc to represent where their condition sits in their life relative to their self, and to provide an explanation of that placement. The distance between the condition disc and the self-disc is a validated measure of suffering associated with that condition (Büchi et al., 2002; Büchi & Sensky, 1999). Additional resource discs can also be added, reflecting important aspects of the patient’s life that can be assessed and discussed, for example, work, family, or religion (Sensky & Büchi, 2016). Therefore, in addition to providing quantitative assessments of the patient’s life, the PRISM incorporates a narrative aspect that enables focused discussion around aspects of the patient’s life that are meaningful to them. There are many aspects of the tool that suggest it could provide a more holistic and meaningful assessment of pain for Māori than the currently used questionnaires.
The goal of this study was to adapt the PRISM to provide an assessment of chronic pain that incorporates principles of Te Ao Māori (Māori world), or tikanga (Māori custom and protocols). A more culturally appropriate assessment is likely to provide a greater understanding of pain and its impact, be more engaging for patients, and provide a better guide for management, therefore improving outcomes and reducing the inequities that are present. By focusing on the development of a tool that prioritises Te Ao Māori, we envisage that the tool will also be more appropriate for the diverse cultures within Aotearoa New Zealand more broadly, and thus provide wider benefits.
Methods
The study was a Māori-centred project in that the participants involved were Māori but the research team was a collaboration of Māori (H.S., E.M., J.M.H., A.-L.H.) and non-Māori (G.N.L., N.L.T., N.S., G.T., D.J.B.) working together (Hudson et al., 2011). The research team included a mixture of clinical health care providers with experience in working with people with chronic pain and health researchers with expertise in pain and outcome measures. The team recognise the Tiriti o Waitangi (Treaty of Waitangi), Aotearoa’s founding document, principle of achieving health equity for Māori in Aotearoa (Tribunal, 2023) and the obligation of non-Māori to partner with Māori in conducting research that promotes better health outcomes for whānau Māori (Māori families). The lead author, who is Pākehā, grew up an area of high Māori population in south Auckland and spent many years at her institution promoting the engagement and involvement of Māori in research. Her earlier quantitative research documented some of the inequities experienced by Māori in relation to chronic pain and she has been involved in several projects investigating views of pain from different cultural perspectives. E.M. (Te Rarawa, a Māori tribe, Northland, North Island, New Zealand; Ngā Puhi, a Māori tribe, Northland, North Island, New Zealand) is a health psychologist who has a relationship with several team members through their research centred on Māori interpretations of pain and management. H.S. (Te Rarawa, Ngāti Tūwharetoa, a Māori tribe, central North Island, New Zealand) is a student counsellor who was connected to the project through his skills as a cultural advisor. A.L.-H. (Te Rarawa) is a health psychologist who works in the chronic pain field. She was a participant in the early part of the research and her meaningful contributions and ongoing interest in the project meant she became one of the study team. J.M.H. (Ngāti Maniapoto, a Māori tribe, Waikato-Waitomo, North Island, New Zealand; Ngāti Mahuta, a Māori tribe, Waikato, North Island, New Zealand) is a senior academic with a long history of research in Māori work experiences and Māori business. The remaining non-Māori members of the team are a mixture of clinicians, including health psychologists and a physiotherapist, and health researchers who have all been involved in previous projects related to cultural interpretations of pain and promoting more equitable outcomes from pain management.
The methodology was based on the principles of whakawhiti kōrero, which reflects discussion and negotiation. A series of wānanga (focus groups) and individual interviews were held with Māori clinicians and Māori with chronic pain to gauge their thoughts on the tool and its adaptation to reflect Te Ao Māori. This process ensured a strong Māori focus within the project.
Participants
Participants were recruited through existing personal networks and word-of-mouth. They were required to be Māori, aged >18 years, and either have experienced pain for >3 months or be a current or former health care provider. Participants were initially contacted by a member of the research team to discuss the project. If they expressed interest, they were contacted by phone by the lead investigator and were provided with further verbal and written information about the project.
The project was discussed with the Mātauranga Māori (Māori knowledge) Committee at the Auckland University of Technology, who provide a forum for researchers to discuss and receive feedback on their proposed projects in relation to Te Tiriti o Waitangi obligations. The project received ethical approval from the Auckland University of Technology Ethics Committee. All participants provided informed written consent prior to participation and were provided with an NZD $40 voucher as koha (gift).
Protocol
A flowchart of the study protocol is shown in Figure 1. Initially, one wānanga with three clinicians was held, followed by a wānanga with three people with chronic pain. Both wānanga served to present the tool as currently used and to discuss possible adaptations. Separate wānanga were used to reduce any potential power imbalances between the clinician and community participants. Discussion centred around (1) how to adapt the concepts and terminology of the standard PRISM assessment to reflect Māori concepts of health and well-being, (2) a possible protocol for completing the tool, and (3) physical aspects of the tool. Subsequent to these wānanga, individual interviews were held with three additional Māori clinicians to discuss the ideas raised at the wānanga and to further refine the tool. All wānanga and interviews were audio recorded and transcribed.
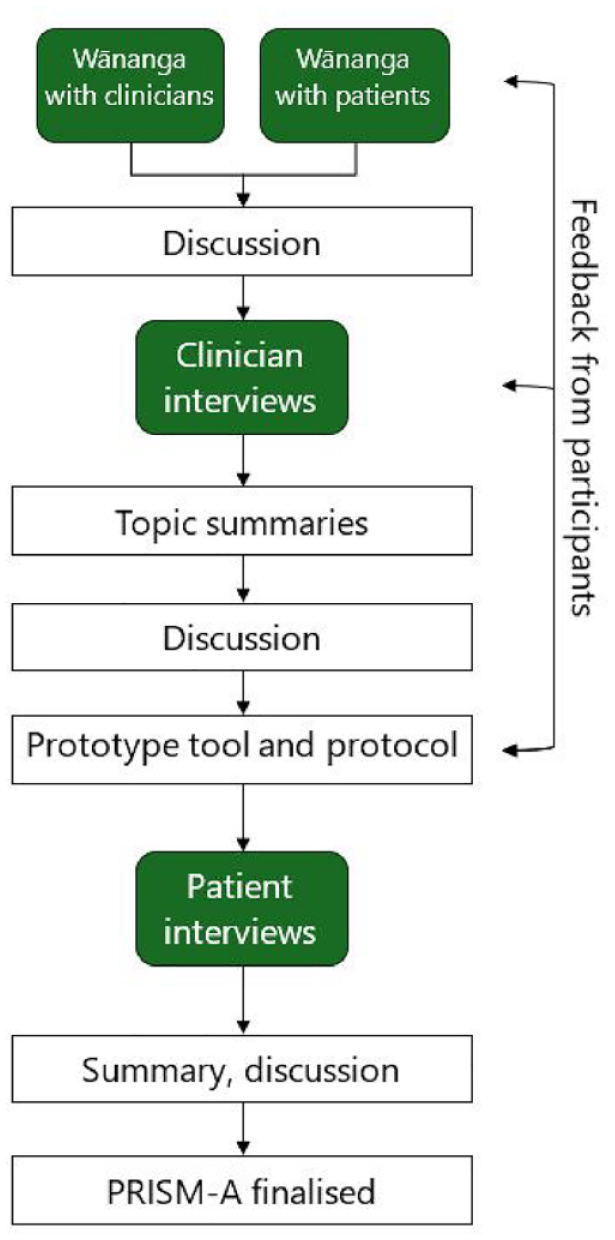
A flowchart of the study protocol.
The first author familiarised themselves with the data by listening to the audio recordings of the wānanga and clinician interviews at least twice and then extracted the main suggestions from each to summarise the data. Unlike themes in thematic analysis, topic summaries provide “an overview of what participants discussed in relation to a specific topic” (Braun & Clarke, 2022, p. 297). Topic summaries are an appropriate analytical output for user-informed enhancement of design (Dumas & Redish, 2000). Based on these topic summaries, a draft version of the tool and protocol for assessment was created and shared with the full research team for discussion. During this process, the lead author regularly checked with the two interviewers regarding her interpretation of the interviews, consulted with te reo Māori (Māori language) speakers in the team when kupu Māori (Māori words) were used, discussed design aspects of the tool and their meaning with Māori members of the team, and liaised with clinical members to ensure the tool remained relevant for practice. While the lead author had moderate experience in qualitative research, a senior researcher in the team was routinely consulted in relation to the data analysis procedures.
Following these discussions, a final prototype tool and protocol for assessment was developed. A video explaining the prototype and assessment process was created and a link to the video was emailed to the previous participants so they could provide any additional feedback and comments. Following integration of this feedback, individual interviews were held with three additional Māori with chronic pain, to get further insight and feedback from people who had no previous experience with the tool. During the interviews, the participants completed the assessment using a cognitive interviewing process with verbal cueing. This process involved the participants completing the assessment with an interviewer but with additional questions to probe the participant’s understanding of the task. The questioning for the actual assessment tool is aimed at increasing the participant’s sense of meaning by bringing into awareness deeper reasoning behind their choice of disc placement. The cognitive interviewing technique was adopted to check the interpretation, clarity, and suitability of the instructions and questions to elicit this reasoning. Recordings of these interviews were listened to by the first author and discussed with the team before the tool and assessment protocol were finalised.
After the initial wānanga, the ideas raised were discussed before progressing to the individual interviews with three further clinicians. Topic summaries were completed by the lead author using the wānanga and interview data and were discussed with the whole team prior to development of a prototype tool, which was sent to the previous participants for feedback. The prototype tool was used in three additional patient interviews. The lead author summarised these interviews, discussed with other team members, and then finalised the tool.
The methods centralised tikanga. Wānanga and interviews opened with karakia (prayer), whakawhanaungatanga (relationship formation), and then the whakapapa (genealogy or history) of the project was explained. Wānanga were run by one Pākehā and one Māori facilitator. Individual interviews with clinicians were conducted by a Pākehā researcher and participants were given the choice of whether they wanted a Māori facilitator present or not. Individual interviews with people with chronic pain were facilitated by one Māori and one Pākehā researcher. All wānanga and interviews were closed with kai (food) and karakia.
Results
In total, six Māori clinicians and five Māori who had experienced chronic pain participated. The clinicians were four health psychologists, one podiatrist, one nurse. One additional participant was a non-Māori who had chronic pain who attended and contributed to one of the wānanga as a support person. The final model of the tool, which we have named the Pictorial Representation of Illness and Self Measure–Aotearoa (PRISM-A), incorporates the basic principles of the original version but the physical and conceptual aspects have been substantially adapted to reflect Te Ao Māori. Here, we present the ideas and concepts raised by the participants in general about the tool as well as about specific elements. We also describe how these ideas and concepts were used to inform the development of the PRISM-A.
Overview of PRISM-A
At the initial wānanga and clinician interviews, participants highlighted the simplicity and flexibility of the tool. The visual nature and simplicity of the assessment meant it was perceived as being more appropriate across cultures and reduced the language burden of questionnaires: The simplicity of it means we can use it across many populations . . . . So, it’s transferable to everybody from different cultures. And I really love that, it’s what’s needed, it’s something universal and holistic. (female 1, health psychologist)
Simplicity also appealed to the patient participants. After receiving an explanation of how to place the pain disc, one commented, “That’s an easy way of doing it, yeah” (male, patient). Simplicity was therefore kept in mind when deciding on the specific components of the adapted tool. Flexibility and opportunity for choice within the assessment were also viewed positively. As one clinician said, “then it becomes a pūrākau, a story, a story of their telling” (female 2, health psychologist). Permitting patients the opportunity to define elements of the assessment themselves was also thought to open up conversations about their beliefs and what the patient sees as important. This kōrero (talk or conversation) was seen by clinician participants as important to facilitate whakawhanaungatanga between the patient and clinician: It’s a subjective thing and it covers quite a lot, each of those domains, but that’s a really good opportunity for further narrative and whakawhanaungatanga, I guess, and understanding each other and what it means for one another. (female 1, health psychologist) From my personal experience, it would almost be more powerful to kind of self-disclose what it means for the practitioner who is doing the assessment. You know, saying, “for me, tinana [physical well-being] means am I able to go and do my sports in the weekends, can I physically clean the house, go for my walks in nature.” I think that kind of self-disclosure and sharing of understandings can trigger, you know, the right ideas to make them think, what does it mean for me? (female 1, health psychologist)
Sharing from the clinician during the assessment was therefore seen as able to serve a dual purpose of facilitating relationship building with the patient and providing examples relevant to completion of the assessment. Therefore, the PRISM-A has been designed to be completed interactively with a clinician. As the patient and clinician go through each step of the assessment, the clinician provides an explanation of the concept and then shares some of themself by describing how they would complete that step relative to their own life.
Finally, there was some discussion around the physical presentation of the tool. While one of the wānanga raised the idea of an electronic version of the tool, most others found the visual and physical aspects of the discs and paper to be appealing. For example, one participant said, “I love it ‘cause it’s tactile too . . . you can touch it and move it around” (male, health psychologist), while another stated, “I think, personally, I think it’s far more powerful doing it with kind of physical . . . you know, people actually moving it and kind of discussing, you know, why they specifically place, placed it in certain places” (female 3, health psychologist). These views were also reflected by a patient, “This is really lovely to be able to see it, how I actually work and, you know, visual effect” (female 1, patient).
The perceived value of a tangible tool meant that the PRISM-A has been constructed as a paper version with physical discs.
Background page
It was strongly recommended by the participants that patients are invited to define what the piece of paper reflecting my life meant to them. There were various suggestions by clinician and patient participants for appropriate te reo Māori words for this. Thus, the piece of paper has been termed background page and has multiple additional title options, including Hauora (health), Te Taiao (world or environment), and Mauri (life principle or life force). In completing the assessment, patients are invited to describe what the background page represents for them and then choose one of the labels or create a label of their own.
Various options for colour and patterns on the background page were discussed. There was some concern that a pattern may influence where discs were placed. One clinician stated, “To me, white seems appropriate because it’s like a blank slate” (female 1, health psychologist) and white was not disliked by any of the participants, so the background page has been left as plain white. It was felt that a larger page would work better than an A4 (210 × 297 mm) size as the smaller size was reported as constraining, and so an A3 (297 × 420 mm) size page has been adopted.
Centre disc
While participants understood why the self-disc was in the corner of the background page in the original PRISM, they felt the centre was a better location to reflect what sat in the centre of life. As one clinician stated, “yeah ‘cause if you have a look at a marae [meeting place], it’s central to everything, it’s never at the back” (male, counsellor), and one clinician felt that a central location “provides more opportunity and space to visualise that you are at the centre of this” (female 1, health psychologist).
Therefore, the self-disc is now termed the centre disc that sits in the middle of the background page. Participants also unanimously agreed that patients should be able to define for themselves what the centre disc represents. An individualist view of self in the centre was described as Western and preference was given to incorporating a collectivist view: I think being Māori is quite, you know, maybe we don’t see ourselves as being kind of singular. We see ourselves as more, more than just ourselves and maybe carry, I guess, our whānau [family, families] and our, you know, ancestors with us. (female 3, health psychologist) We get a reality of, well, this isn’t just affecting a person, this is affecting a person who belongs to a marae. This is a person that is of this, this iwi [tribe]. This is a person who’s of that hapū [subtribe]. You know, those kind of things. (female 2, health psychologist)
And so then here, if this disc signifies your pain, where would you put it?
Right beside it [centre disc].
Right beside it?
It does influence what I do. So that’s, yeah, so what I can do for my whānau. Yeah. It’s a big part of it. If I’m not well, then it will directly affect them, where we are and what we do. It affects them too.
The inclusion of multiple interpretations of the centre disc appeared to not only capture that the individual was not seen as most important, but that pain also impacted more than just the individual.
Participants also reported that pictures would be better than words to reflect these meanings on the centre disc. For example, one clinician said, “If it’s pictorial, yeah. A little marae on there, a little maunga [mountain] there, and a nice little, you know, wai [water]” (female, podiatrist). One clinician thought a picture or an icon would provide a better connection for the patient than a plain disc: Something might be nice just to connect with in there, rather than just a circle with a thing but something that, you know, if I’m gonna do a representation of me and my pain here I want something to connect me to that spot on the paper . . . . For me, if there was some kind of design or something here that wasn’t just a circle, I might connect better with that. (male, health psychologist)
The centre disc appeared to provide an opportunity for the patient to connect with the assessment and ground their world view in the centre of the tool. PRISM-A, therefore, has a selection of centre discs with icons representing both individualist and collectivist concepts, such as a person, whānau, waka (ancestral migration canoes), and marae that patients can select from and place in the middle of their background page (Figure 2). One clinician also suggested some patients may want to write their name on the centre disc to reflect that this captured their whānau and ancestors, “Your whānau give you your name, and then it’s connected that way” (female 3, health psychologist). To accommodate this option, a blank disc is also available that a person can add their own meaningful design or name to.
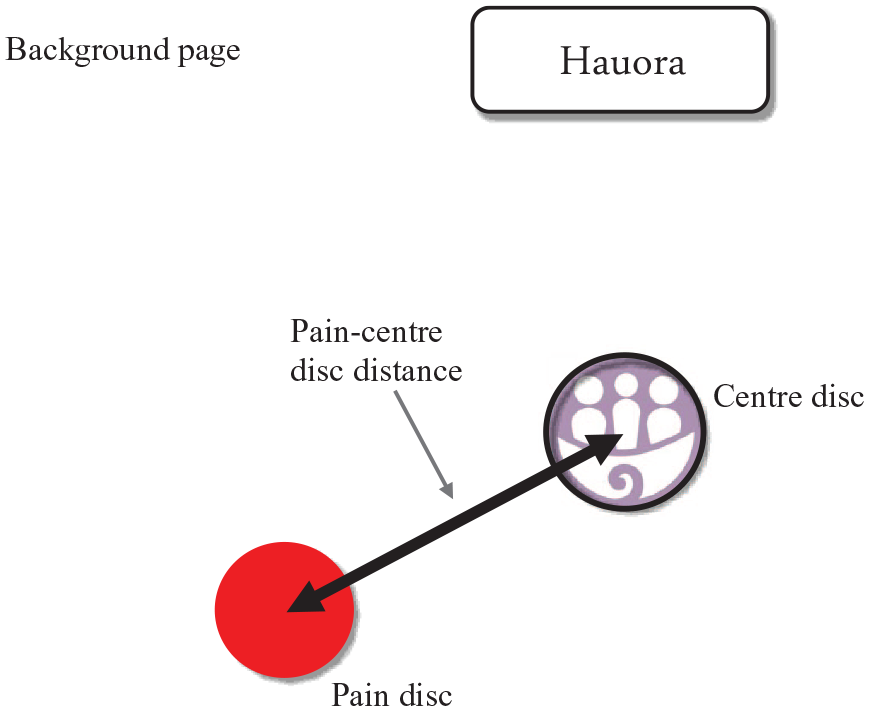
Pictorial Representation of Illness and Self Measure–Aotearoa (PRISM-A) tool showing the background page, label, example self-selected centre disc, and the pain disc.hauora = health.
Pain disc
There was agreement that mamae (pain) was an appropriate word for the pain disc. Similar to previous versions of PRISM, in PRISM-A, patients are asked to place the mamae or pain disc on the background page to reflect where pain sits in their life relative to the centre disc. This concept was viewed by participants as logical and more meaningful than using other numerical rating scales for pain: I think as a health psychologist you look at, at the, at the distance of it. I mean the darn thing might be right over there or it could be right on top of them, which kind of would indicate that that the pain is overwhelming them. (female 2, health psychologist) We’re not asking them to look at a very objective scale which is measuring subjective things. It is something that is actually, this is you, this is your life, where is the pain in your life and how is it impacting you? How is it impacting your identity? (female 1, health psychologist)
Does that sort of make sense to you that idea, that it would be right on top of you when it was at its worst?
It does, yeah, it does, yeah, yeah.
Participants completing the assessment therefore seemed to view the visual nature of the disc and its placement on the background page as providing a simple yet holistic assessment of the impact of pain.
In the assessment, the distance between the pain and centre discs is measured and provides a quantitative value of pain suffering (Figure 2). Once the disc is positioned, patients are asked why they have placed it there to invite further, focussed discussion on the impact of pain. To provide greater understanding, it is also possible to ask questions such as “Where would you like the pain disc to be?” “Where is it on a good day, or a bad day?” and “What shifts the disc around?”. For one participant with chronic pain completing the assessment, the interviewer was able to use the disc to more fully understand what pain encompassed:
I just want to come back to something you just mentioned in passing before. You said, that’s not just pain. That’s pain, but it’s there’s more to it than just pain. Is that right?
Yeah.
So, what would, what else is encompassed in that, that red dot?
Well, it’s just, it is all pain, but it’s not just the physical pain. It’s how my journey from experiencing a lot of my domestic violence pain, and pain from that. Look, I had teeth knocked, cracked, and had to be taken out, and dealing with organisations like ACC [Accident Compensation Corporation; national no-fault insurance provider] who would not recognise it.
Okay.
So, you’re left with a lot of those things through not being addressed.
The inherent physical and narrative aspect of the tool therefore appears to be able to more fully explore the broad concept of pain and the associated emotional, mental, and spiritual narratives that contribute towards the pain experience.
Well-being discs
The resource discs from the original PRISM generated the most discussion and a wide range of ideas were presented as to how these could be incorporated in a simple but meaningful manner. The ability to select different resource discs was seen as a limitation by one clinician, who raised the question, “how do you compare if people are choosing different things?” (male, health psychologist). There was agreement among participants on the desire to incorporate Te Whare Tapa Whā, a Māori model of health (Durie, 1985), into this aspect of the assessment. Te Whare Tapa Whā incorporates four elements of health and well-being: taha whānau (social well-being), taha hinengaro (mental and emotional well-being), taha wairua (spiritual well-being), and taha tinana (physical well-being). As one clinician said, “I think what first comes into mind if, I definitely think the aspects of Te Whare Tapa Whā are definitely worth being included” (female 3, health psychologist). The four elements of the health model were viewed by clinician and patient participants as sources of support and key areas of well-being to be assessed. One patient participant stated, “So, Te Whare Tapa Whā is a great way to articulate it actually . . . . It’s what I draw on, on all of those to keep us well” (female 1, patient), while a clinician participant indicated similar thoughts:
What would be most meaningful for you to assess?
Connection and relationships is definitely one. To me personally, spirituality. My physical ableness, my physical functioning. Mental and emotional obviously. Also, your purpose, which can be interpreted so differently.
We therefore felt it critical that Te Whare Tapa Whā was overtly incorporated into the assessment. In PRISM-A, the resource discs were re-designed as well-being discs reflecting the four elements of Te Whare Tapa Whā. For each disc, the clinician first explains what the element means or encompasses (Table 1), or invites the patient to provide their own interpretation. The clinician then asks the patient what aspects of that element are important to them and provides an example from themselves. This concept of defining and sharing was captured in a conversation between the two interviewers during an assessment with a participant with chronic pain:
So, so tinana, what does tinana mean to you [interviewer 2]?
Well, it’s my physical well-being, the way I, like you, I have a young daughter. So, I need to be physically well enough to be able to engage with her just simply at a park. You know, which means I’ve got to be able to walk, run . . . chase her, play tag. You know, so my physical wellness requires me to do something in order to be able to engage in those activities. So, that’s how I see physical. It’s just allowing you to be able to do simple things well enough.
Yeah. And then, I suppose, for everyone it might be different if you think of the particular things. So, for you it’s about your daughter, being able to play at the playground. For me, so, like running is quite a big part of my life. I do quite a lot of running, so if I couldn’t do that, that would be a big problem for me. So, for me, when I think about tinana, you know, I do, I sort of think about my hobbies and recreation and trying to escape and running.
The four elements of Te Whare Tapa Whā (a Māori model of health) represented by the well-being discs, along with examples of what each can encompass.

Once the important aspects of that element are identified by the patient, they are then asked to position the relevant disc on the background page to reflect where those aspects sit in their life at the moment, relative to the centre disc (Figure 3). For these discs, positioning closer to the centre disc reflects a larger involvement in the person’s life in a positive manner, supporting their well-being. This method enabled us to incorporate the participants’ desire to make the tool personal to the patient, yet also provide a consistent measure that could be compared across people and over time.

Four well-being discs placed on the background page. For each disc, the distance to the centre disc is measured.
Similar to the pain disc, the distance from each of the well-being discs to the centre disc is measured and the patient is asked to explain why they positioned the disc in that location. Therefore, each of the four elements are assessed quantitatively, but the specific aspect of each element that is assessed is individualised to the patient to reflect what is meaningful to them. One of the clinician participants also brought in the aspect of balancing the four elements of well-being:
I’d be looking more at balance between them.
Okay, so that they’re sort of evenly distributed?
Yeah, well, well if this one’s closer, it means I’m gonna wo-, if I’m taking a strength-based approach, this is what I’m looking at working with in order to bring it in to me, closer.
The idea of balancing and bringing in the well-being discs closer to the centre disc enables targeted discussion around what can be done to achieve this:
You got anything in particular that might help you in that regard, to get it closer to self?
I know with hinengaro, it’s more my own thinking, so like, even though the worries about “am I actually capable of doing this?” are legitimate because everyone does, but it’s still not putting itself down on yourself. So, using things like the CBT [cognitive behavioural therapy] and all that, you know, and it’s just kind of being, you know, that kind of like checking in on yourself and making sure that you’re good and stuff like that.
Having the four discs visible together around the centre-disc also enabled patients to articulate how these different aspects of their well-being interact and overlap with each other, enabling a more holistic view. One participant with chronic pain completing the assessment described the four elements as, “they’re all working together” (female 1, patient), while another discussed with the interviewer how the different aspects of well-being interacted:
I reckon so because as I’m getting more in touch with Te Ao Māori and stuff like maramataka [Māori lunar calendar] or doing things in the way that we would have done them ages ago, I feel like this is getting better.
Okay, so your hinengaro, I’m just going to, I’m saying it so that the recording knows what we’re talking about. So, so, when the wairua or the whānau things are going well, as you explore that more, it’s improving the hinengaro?
Yeah.
Or bringing that in closer.
And then the same with having a whānau that’s supportive, and then the wairua improving, which improves hinengaro. I think the tinana in terms of, like, well-being, that kind of stuff would probably start to come through.
Seeing the four components together on the background page appeared to enable the clinician and patient to see the patient as a whole more easily, rather than as separate components assessed by separate assessments.
Discussion
One of the ways that health outcomes for Māori in Aotearoa are impeded is the general lack of culturally appropriate approaches across a multitude of health professions to diagnose and treat chronic pain (Devan et al., 2021). These include the lack of diagnostic assessment tools that specifically address aspects of well-being that are important for Māori (Hoeta et al., 2020). The PRISM-A has been adapted from a standard measure to incorporate key principles of Te Ao Māori to make it a culturally appropriate assessment of chronic pain, including whanaungatanga (relationship), collectivism, and holistic views of health and well-being (Wilson et al., 2021). Participants in this study viewed the visual and physical nature of the tool, the opportunity for flexibility, choice, and control, and the incorporation of Te Whare Tapa Whā as important attributes. These aspects have been woven into the tool in a way that enables chronic pain to be assessed more fully, facilitates whakawhanaungatanga, and overtly directs clinicians to areas of management that are meaningful for the patient. Indeed, many of the principles that have been incorporated in the assessment are similar to those integral to Hua Oranga, a measure of mental health outcome for Māori (Durie & Kingi, 1997), Te Waka Kuaka, a cultural needs assessment tool for Māori with traumatic brain injury (Elder & Kersten, 2015), and Mahi Oranga, a measure of occupational health for Māori (Stewart & Gardner, 2015).
For a tool to be accepted in mainstream clinical practice, it needs to provide a valid and reliable assessment that can be meaningfully compared within and across patients. The five quantitative measures attained from the PRISM-A, representing inter-disc measures for mamae, taha tinana, taha wairua, taha hinengaro, and taha whānau, enable such standardised measures to be obtained, although a full validation study across multiple cultures would be needed to fully confirm its measurement properties. The condition and self-disc separation measure in the standard PRISM has been validated as a measure of suffering in many cultures, including Japanese (Tomioka et al., 2021), South American (Krikorian et al., 2013; Lima-Verde et al., 2013), Southeast Asian (Brady et al., 2019), Middle Eastern (Brady et al., 2019), and European (Gardner-Nix & Kassardjian, 2009; Klis et al., 2008; Mühleisen et al., 2009). The resources discs used in previous versions have been used in various ways to probe broader, individualised aspects of a patient’s life. The PRISM-A affords a benefit in that it utilises four standardised well-being discs to enable consistency of assessment across patients, yet patients can individually define the important aspects of each element for themselves, ensuring the assessment remains relevant to the patient. The positioning of the four well-being discs around the centre-disc enabled the interrelationship and balance of these elements to be seen and discussed, rather than assessed separately (Durie, 2004). Therefore, similar to frameworks such as the Meihana Model (Pitama et al., 2014), the assessment enables clinicians to get a better understanding of the patient and their mamae within the broader context of the patient’s life. In addition, the ability of the centre-disc to reflect collectivist views and the incorporation of relational and spiritual aspects of well-being within the assessment mean the tool is more likely to resonate with other cultures that reside in Aotearoa that also have holistic models of health and interpretations of pain (Lewis et al., 2023; Upsdell et al., in press).
The visual and physical nature of the tool and the inherent interaction with the clinician were seen as beneficial components. There are intrinsic language and comprehension barriers with written questionnaires, particularly when used across cultures (Beaton et al., 2000; De Silva et al., 2019), and Māori have a traditional preference for oral rather than written communication (Bishop, 1995; Hikuroa, 2017). The notion of sharing is also valued by Māori in forming relationships (Bishop, 1995); therefore, the requirement of the clinician to provide examples from their own life during the assessment is likely to facilitate the formation of a relationship with the patient. The therapeutic alliance is critical in health care and therapeutic outcomes (Kelley et al., 2014). Culturally driven differences in world view, values, and behaviour can be a barrier to clinicians forming meaningful relationships with Māori, which in turn adversely impacts health care delivery for Māori (Palmer et al., 2019), including pain management specifically (Dixon et al., 2021; McGavock, 2011). Thus, it is hoped that the interactive nature of the tool may mitigate some of these issues by strengthening rapport between the clinician and patient through relating and sharing. The incorporation of sharing resonates with the Hui Process (Lacey et al., 2011), a framework developed for clinicians to establish and build relationships with Māori that is guided by Te Ao Māori principles. The reciprocity of personal narrative reflects value in a mutual understanding of one another and provides an opportunity to reduce the usual hierarchical nature of Western clinical settings. Interestingly, some participants expressed potential for patients to complete the PRISM-A at home on their own or with whānau for their own self-monitoring. Completing the tool with whānau would enable patients to express and communicate to whānau the perceived impact of pain on their individual and collective well-being. This may facilitate a deeper understanding of pain for whānau, allowing those experiencing chronic pain to strengthen the support, connection to community, and feeling of belonging while navigating pain. Therefore, ongoing clinician involvement may not be needed and the PRISM-A may be able to be used to promote self-management.
The project had several strengths. The research team were a partnership of Māori and non-Māori clinicians and health researchers with experience in chronic pain. We incorporated recommendations regarding the development of Indigenous assessment tools (Deloitte, 2022), including consultation with both users of the tool as clinicians and those with lived experience of chronic pain, incorporating language and pictures as recommended by the participants, and the tool is underpinned by a Māori model of health. There were also some limitations. There was a relatively small sample size, although those involved provided meaningful contributions. The lead author is Pākehā. While she has experience teaching equity in health research and was a member of the institution’s Mātauranga Māori Committee for 11 years, a concerted effort was made to promote the voices of participants and Māori co-authors in developing the tool.
In conclusion, the PRISM-A was developed through a collaboration of researchers working with Māori clinicians and Māori with chronic pain. It was designed in a strength-based manner, incorporating aspects of Te Ao Māori that make it a holistic assessment that more fully captures the meaning and impact of pain for Māori. The inherent discussion around multiple aspects of well-being can also direct clinicians to important aspects of a patient’s life that could form the basis of a management plan. Further testing of the tool is needed to determine its validity as an outcome measure for chronic pain across the multiple cultures in Aotearoa.
Footnotes
Acknowledgements
We acknowledge the time, personal stories, and knowledge given to our project by the participants.
Authors’ note
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: Faculty of Health and Environmental Science, Auckland University of Technology.
Glossary
Aotearoa New Zealand
hapū subtribe
hauora health
Hua Oranga a measure of mental health outcome for Māori
iwi tribe
kai food
karakia prayer
koha gift
kōrero talk or conversation
kupu word
Mahi Oranga a measure of occupational health for Māori
mamae pain
Māori Indigenous People of New Zealand
marae meeting place
maramataka Māori lunar calendar
Mātauranga Māori Māori knowledge
maunga mountain
mauri life principle or life force
Ngā Puhi a Māori tribe, Northland, North Island, New Zealand
Ngāti Mahuta a Māori tribe, Waikato, North Island, New Zealand
Ngāti Maniapoto a Māori tribe, Waikato-Waitomo, North Island, New Zealand
Ngāti Tūwharetoa a Māori tribe, central North Island, New Zealand
Pākehā New Zealander of British or European descent
pūrākau a story
taha hinengaro; hinengaro mental and emotional well-being
taha tinana; tinana physical well-being
taha wairua; wairua spiritual well-being
taha whānau social well-being
te taiao world or environment
Te Ao Māori Māori world
te reo Māori Māori language
Te Rarawa a Māori tribe, Northland, North Island, New Zealand
Te Tiriti o Waitangi Treaty of Waitangi
Te Waka Kuaka a cultural needs assessment tool for Māori with traumatic brain injury
Te Whare Tapa Whā a Māori model of health
tikanga custom or protocols
wai water
waka ancestral migration canoes
wānanga focus groups or history
whakapapa genealogy
whakawhanaungatanga relationship formation
whakawhiti kōrero discussion and negotiation
whānau family, families
whanaungatanga relationship