
Abstract
Aim:
In this study our aim was to elucidate whether advanced cancer patients benefit from antibiotic treatment in the last days of life in addition to reviewing the relevant costs and effects.
Materials And Methods:
We reviewed medical records from 100 end-stage cancer patients and their antibiotic use during the hospitalization in Imam Khomeini hospital. Patient’s medical records were analyzed retrospectively for cause and periodicity of infections, fever, increase in acute phase proteins, cultures, type and cost of antibiotic.
Results:
Microorganisms were found in only 29 patients (29%) and the most microorganism among the patients was E. coli (6%). About 78% of the patients had clinical symptoms. The highest dose of antibiotics was related to Ceftriaxone (40.2%) and in the second place was Metronidazole (34.7%) and the lowest dose was related to Levofloxacin, Gentamycin and Colistin (1.4%). Fifty-one patients (71%) did not have any side effects due to antibiotics. The most common side effect of antibiotics among patients was skin rash (12.5%). The average estimated cost for antibiotic use was 7 935 540 Rials (24.4 dollars).
Conclusion:
Prescription of antibiotics was not effective in symptom control in advanced cancer patients. The cost of using antibiotics during hospitalization is very high and also the risk of developing resistant pathogens during admission should be considered. Antibiotic side effects also occur in patients, causing more harm to the patient at the end of life. Therefore, the benefits of antibiotic advice in this time is less than its negative effects.
Introduction
Nowadays, given that medical interventions in terminal stage cancer patients have progressed, physical life can be prolonged to some degree from a few days to several weeks. 1 Two theoretical benefits motivate providers to prescribe antimicrobials to terminally ill patients; prolonging survival and relieving symptoms. However, there are limited data to provide evidence regarding these outcomes. 2 In a recent editorial, Furuno et al 3 argues that decisions on antibiotic use in hospice care should be made on a case-by-case basis and be consistent with the individuals’ goals of care.
When the decision to start treatment is made, it is helpful to be aware of pathogen and antibiotic susceptibility patterns to assist with antibiotic selection. 4 Rarely considered as increasing the burden of medications for the terminally ill patient, many physicians consider antimicrobials as a benign intervention even though it may result in adverse events [ie, adverse drug effects, Clostridium difficile infection (CDI), development and transmission of multidrug-resistant organisms (MDROs) in healthcare settings].5-7 In addition to medication burden, discomfort may result from evaluation procedures (eg, bladder catheterization, blood draws, imaging studies) and treatment (eg, intravenous lines, mechanical restraints) of suspected infections. 8
There are no written guidelines regarding the use of antibiotics in the dying cancer patient and to treat or not to treat these patients needs ethical considerations. The overall goal is to improve quality of life in patients facing the problems associated with life-threatening illness. Therefore, it is important that the side effects of any medical treatment do not outweigh possible beneficial effects. 9 Nosocomial infections result in morbidity, mortality and cost of care is greater than that would be expected from the patient’s underlying diseases alone. 10 Moreover, charges of the prolonged stay and resulting increased antibiotic use account for most of the costs related to nosocomial infection. 11 Studies in patients with terminal cancer have shown that with proper counseling, patients and families often are amenable to withholding or withdrawing antimicrobials when increasing signs and symptoms of death are present.12-15
One of the major challenges in treating patients with advanced cancer is the length of hospital care and treatment in the last days or weeks of life. These hospitalizations are usually accompanied by the administration of various antibiotics, many and often at exorbitant costs, which ultimately increase the cost of treatment and staff work, leading to an increase in various resistant and highly resistant microorganisms in different wards such as internal, infectious, and oncology ward. Eventually, these resistant microorganisms threaten the lives of many other patients and will incur staggering costs for the health care system. In this article, the question is to what extent conventional antibiotic therapy can increase life expectancy or improve the quality of life of advanced cancers patients that are in the end stages of life.
Materials and Methods
Between June 2018 and June 2019, 100 advanced cancer patients were included in this retrospective study in Imam Khomeini Hospital of Tehran- Iran and all participants provided verbal informed consent. Patients’ medical records such as laboratory results, treatments the patient has received for cancer, cause and periodicity of infections, fever, increase in acute phase proteins, cultures and type of antibiotic used through patient records are collected and were evaluated for the antibiotics received and their costs. All patients with advanced and end-stage cancer whose treatment had been discontinued or was progressing despite treatment, were included in this study and patients admitted for cancer treatment were excluded. General features of the patients were evaluated and the relation of antibiotic cost with these features was compared according to statistical methods mentioned below.
Statistical methods
For statistical analysis, SPSS software version 25 was used. Mann–Whitney U test was used for 2 group quantitative data comparison. Kruskal–Wallis test was used for 3 or more group and Bonferroni Dunn’s test was used for 2 groups comparison. Spearman’s correlation analysis was used for evaluation of correlation among variables.
Results
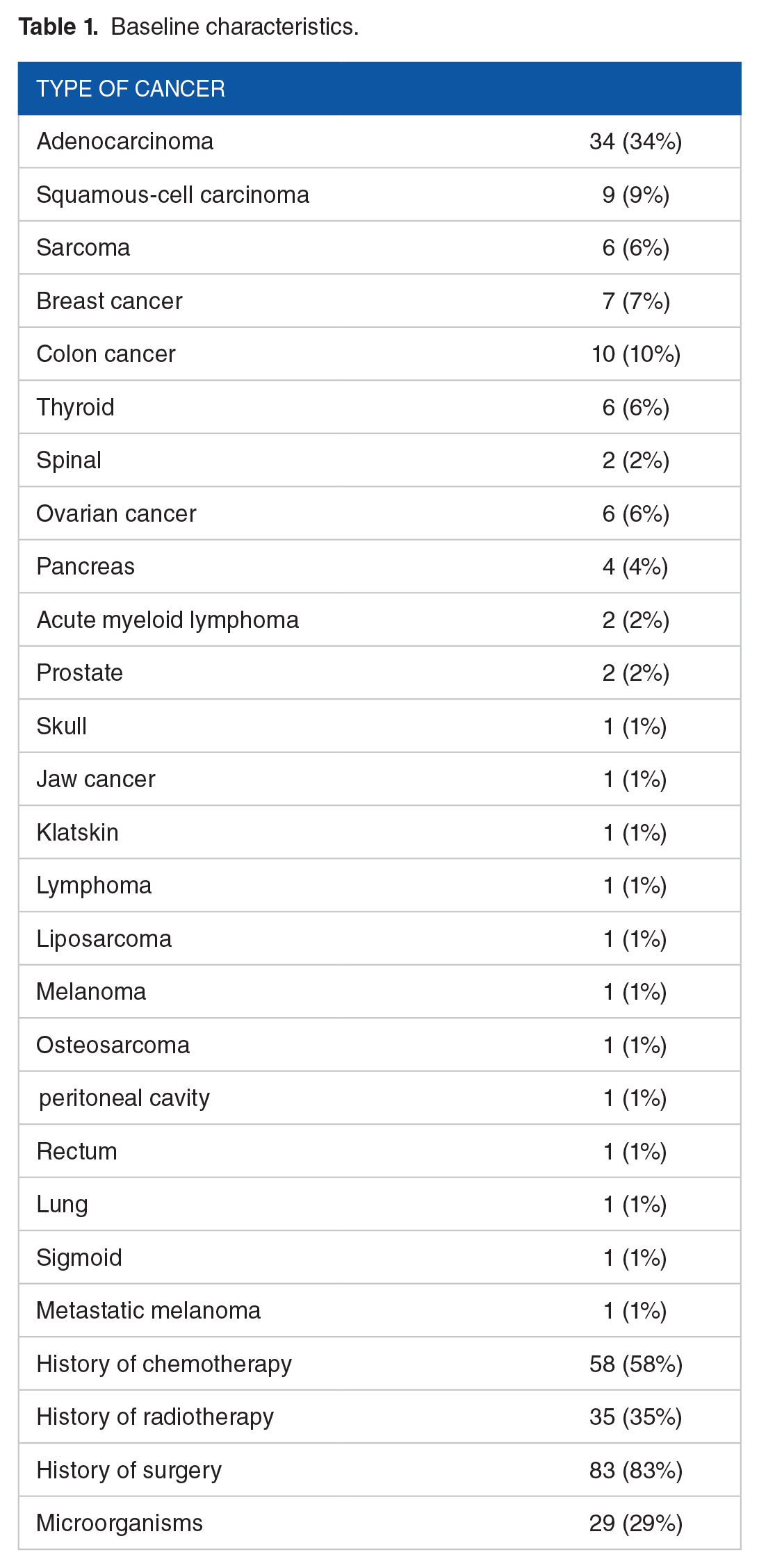
According to the inclusion criteria, 100 end stage cancer patients including 56 males and 44 females were enrolled with a mean age of 59.8 years. 34% of the studied patients had esophageal and gastric cancer which more than half of them (58%) had a history of chemotherapy. Thirty-five patients (35%) had received radiotherapy and 83 patients (83%) had a history of surgery.
Microorganisms were found in only 29 patients (29%) and the most microorganism among the patients was E.coli (6%) (Table 1).
Baseline characteristics.
Based on this study, the highest dose of antibiotics was related to Ceftriaxone (40.2%) and in the second place was Metronidazole (34.7%) and the lowest dose was related to Levofloxacin, Gentamycin and Colistin (1.4%). For 72% of patients, antibiotics were started at the beginning of hospitalization and for some patients antibiotics were modified based on culture results. For initiate, selective antibiotics were usually Ceftriaxone with Metronidazole or Ciprofloxacin with Clindamycin. Due to the length of hospitalization of some patients or intubation for some of them, patients subsequently developed ventilator-associated lung infection (VAP); especially in the case of ICU patients who developed resistant pathogens and taking broad-spectrum antibiotics. According to the WHO standardization guide, the amount of antibiotic use, the standard amount of antibiotic consumption (Antimicrobial consumption Index) and the per capita consumption of antibiotics (Defined Daily Dose) were calculated for patients.
About 78% of the patients had clinical symptoms, of which 21 patients (21%) complained of weakness and lethargy. Seventy-two patients (72%) received antibiotics. Fifty-one patients (71%) did not have any side effects due to antibiotics. The most common side effect of antibiotics among patients was skin rash (12.5%) (Table 2).
Clinical symptoms and antibiotic side effects of patients.

The blood culture included the following: Wound cultures included 2 cases of multidrug-resistant Pseudomonas-aeruginosa (MDR) and 1 case of Carbapenem-resistant Klebsiella-pneumonia (KPC).
Positive trachea cultures included 6 cases of multidrug-resistant (MDR) Acinetobacter baumannii, 2 cases of Imipenem-resistant Acinetobacter baumannii, 1 Ampicillin-resistant Acinobacar bumani with intermediate sensitivity to Amikacin, 2 cases of Carbapenem-sensitive Klebsiella-pneumonia, and 1 case of Enterobacter susceptible to Imipenem and Amikacin.
Seven positive blood cultures included 2 cases of Imipenem-sensitive E-coli, Ampicillin-sulbactam, and Ceftriaxone resistant, 2 cases of linezolid-sensitive Enterococcus faecalis, 1 case of Enterobacteria sensitive to Imipenem and Amikacim, 1 case of methicillin-resistant coagulase-negative staphylococcus (MRSE), and 1 case of Cotrimoxazole and Ciprofloxacin sensitive Stenotrophomona Maltophilia.
Five positive urine cultures included 1 case of beta-lactamase-releasing E. coli (ESBL), 1 case of E. coli sensitive to Ciprofloxacin, Ampicillin sulbactam and Imipenem, 1 case of Enterococcus faecium sensitive to linezolid, and 2 cases of Imipenem sensitive Klebsiella-pneumonia.
In the case of liver mass culture, there was 1 case of Imipenem and Ampicillin-sulbactam sensitive E. coli. One case of Imipenem, Amikacin, and Ceftazidime sensitive E.coli was in the abdominal fluid culture (Table 3).
Characteristics of different types of microorganisms.

The average estimated cost for antibiotic use was 7 935 540 Rials (24.4 dollars) (Table 4). It should be noted that in 2018, the average price of the dollar was 40 422 Rials and in 2019, its average was 42 000 Rials, which has been considered to calculate the average of the 2, that is, 41 000 Rials.
Costs related to antibiotics used by patients studied.

Twenty-three patients were hospitalized for 10 days. The daily cost of a bed in the general ward is 1 465 000 Rials ($ 36). The daily cost of an ICU bed is 7 342 000 Rials ($ 179). The average cost of tests in the records of our patients is 4 000 000 Rials ($ 97). The cost of one cardiopulmonary resuscitation (CPR) was 1 160 000 Rials (28 dollars). Of course, the calculations of the above figures are related to the average prices in 2018-19.
Discussion
In recent years, due to the increasing resistance of microorganisms, the authorities have decided to systematize the prescription of antibiotics to slow down the process of antibiotic resistance and also reduce the unnecessary costs of antibiotic use. Rational management of antibiotic therapy (Antibiotic Steward ship) is on the agenda of medical centers around the world. This program was performed in general in all hospitalized patients. 16
In this article, we examined the possibility of implementing this program specifically in patients with advanced and incurable cancers and cancer patients who are candidate for palliative therapy in the end of life. In these studies, all patients died in the same hospital regardless of receiving or not receiving antibiotics. Different antibiotics were prescribed to the patients. We examined the antibiotic resistance and the presence of positive symptoms, cultures or experimental therapy (Empirical Therapy), the side effects and the cost of the antibiotics used.
In our study, the rate of antibiotic use was 72%. In previous studies, this rate was 47%, 49%, 84.4%.1,9,17 Some patients received antibiotics, for some of them antibiotics were not prescribed according to the doctor and for others, several different types of antibiotics were prescribed. The cultures sent were positive for the patients and the patients’ antibiotics were changed based on the antibiotic sensitivity (Antibiogram) but at the end of the therapeutic process, the treatment had no effect.
Here, despite receiving various antibiotics, the recovery process in patients was not clearly seen, whereas other studies have demonstrated recovery process. In one of them, out of 79 patients who received antibiotics, in 37% the treatment resulted in evident symptom relief and among these 50% had a positive bacterial culture, 43% had a negative culture and in 7% no culture was taken. 9 As another example, in a previous study outcome of antibiotic use revealed 42 patients (17.3%) with symptoms improved 71 patients (29.2%) with stationary symptoms and 130 patients (53.5%) revealed symptom deterioration. 17 In another study by Oh et al, out of 119 patients who received antibiotics, 48% had fever control, of which 15% had a recovery process, and 66% of patients did not improve their recovery despite fever control or lack of fever control. Eventually all the patients died. 1
According to the contents of the file, the cost of antibiotics used was 7 935 540 Rials (187.60 dollars). In another study conducted in 2016 in Turkey, this was 2009.72 TL (122.54 dollars). 10 As an instance, in a study by Ham et al 18 the antibiotic related cost was 20.16 euro (21.60 dollars) per patient and 947.52 euro (1015.14 dollars) in whole group. In addition to the cost of antibiotics, the current costs of hospitalization, including the daily cost of the intensive care unit (ICU), the average cost of tests per patient, the cost of specialized counseling and cardiopulmonary resuscitation (CPR) was also extracted from the patients’ files. Each of the patients underwent cardiopulmonary resuscitation at least once during hospitalization. The average number of hospitalization days for patients in the normal ward was 9 days and in the intensive care unit was 7 days.
Rash and urticaria, itching, diarrhea, nausea, and vomiting were side effects of antibiotics founded in this study, which the most common was skin rash. As demonstrated in the same studies, the major aspect of antibiotic disadvantages and side effects is cell resistance and obstruction of reproductive which is divided into 5 categories: the modification or destruction of antibiotics by enzymes; reduction in the intake of antibiotics into bacteria; increase of antibiotics from bacteria active outward excretion; changes in the target or the creation of new targets and overexpression of drug targets.19-22
E. coli was the most microorganism among our study patients and other related studies.23-25 As well as in some other articles, it was coagulase-negative staphylococci (CNS) and Corynebacterium spp. 26
It seems that advanced cancer and failure of the main organs (ie, heart, kidney, liver, and lung) and complications of the organ failures are the cause of patient’s death. Antibiotic therapy not only cures the patient but also increase the risk of resistant pathogens occurrence, 27 causes complications such as rash, itching, diarrhea, etc. and hurts the patient in the end of life. Moreover, due to the patient’s hospitalization days and the use of various antibiotics, it creates an unnecessary financial burden on the health system.
Limitations
The present study had some limitations; this study was a single center research with small sample size, so the results could not be generalized to other patients. Also, there was no data regards to inflammatory laboratory results to antibiotic use (for follow up the patients response).
Conclusion
We tried to evaluate the effect of different antibiotics as a treatment outcome of advanced cancer patients. The results showed that regardless of not prescribing antibiotics or the type of antibiotics prescribed, it was not effective in control of symptoms in advanced cancer patients. The cost of antibiotics uses during hospitalization is very high and also the risk of developing resistant hospital strains during admission should be considered. Antibiotic side effects also occur in patients, causing more harm to the patients at the end of life. It seems that those who are in charge of prescribing antibiotics in advanced cancer patients should design a written program about the rational prescription of antibiotics, especially broad-spectrum antibiotics.
It is recommended that to do future researches in multicenter setting, so the results and conclusions would be more reliable. Also, all advanced cancer patients be visited by the palliative care team so that in addition to determining the prognosis and treatment goals by focusing on the wishes of patients and their families, they benefit from optimal control of distressing symptoms until the last moment of life and avoid unnecessary diagnostic and therapeutic interventions as much as possible.
Footnotes
Acknowledgements
The authors would like to thank the Clinical Research Development Unit (CRDU) of Baharloo Hospital and palliative care and cancer unit of Imam Khomeini Hospital for their support, cooperation and assistance throughout the period of study.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration Of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions
Mamak Tahmasebi, Hadiseh Hosamirudsari and Mohammadreza Salehidesigned the study. Masoud Parash and Mamak Tamasebi, Mahsa Abbaszadeh managed the patients. analysis, Shirin Familrashtian help in writing and submission of manuscript. Hadiseh Hosamirudsari and Mamak Tahmasebi analyzed, discussed and wrote the manuscript. Hadiseh Hosamirudsari reviewed and submited the manuscript.