
Abstract
Background:
Leukemia is a type of cancers that start in the bone marrow and produce a serious number of abnormal white blood cells. Bleeding and bruising problems, fatigue, fever, and an increased risk of infection are among symptoms of the disease. The main objective of this study is to identify the determinant of the progression rate of white blood cells among patients with chronic lymphocytic leukemia at Felege Hiwot Referral Hospital (FHRH), Bahir Dar, Ethiopia.
Methods:
A retrospective study design was conducted on 312 patients with chronic lymphocytic leukemia at FHRH, Bahir Dar, Ethiopia under treatment from 1 January 2017 to 31 December 2019. A linear mixed-effects model was considered for the progression of the white blood cell data.
Results:
The estimated coefficient of the fixed effect intercept was 84.68, indicating that the average white blood cell (WBC) count of the patients was 84.68 at baseline time by excluding all covariates in the model (P-value <.001). Male sex (β = 2.92, 95% confidence interval [CI] 0.58, 0.5.25), age (β = .17, 95% CI 0.08, 0.28), widowed/divorced marital status (β = 3.30, 95% CI 0.03, 6.57), medium chronic lymphocytic leukemia (CLL) stage (β = −4.34, 95% CI −6.57, −2.68), high CLL stage (β = −2.76, 95% CI −4.86, −0.67), hemoglobin (β = .15, 95% CI 0.07, 0.22), platelet (β = .09, 95% CI 0.02, 0.17), lymphocytes (β = .16, 95% CI 0.03, 0.29), red blood cell (RBC) (β = .17, 95% CI 0.09, 0.25), and follow-up time (β = .27, 95% CI 0.19, 0.36) were significantly associated with the average WBC count of chronic lymphocytic leukemia patients.
Conclusions:
The finding showed that age, sex, lymphocytic, stage of chronic lymphocytic leukemia, marital status, platelet, hemoglobin, RBC, and follow-up time were significantly associated with the average WBC count of chronic lymphocytic leukemia patients. Therefore, health care providers should give due attention and prioritize those identified factors and give frequent counseling about improving the health of chronic lymphocytic leukemia patients.
Background
Leukemia is a group of cancers that usually begin in the bone marrow and result in a large number of abnormal white blood cells. These white blood cells are not fully developed and are called blasts or leukemia cells. Symptoms may include bleeding and swelling problems, feeling tired, fever, and an increased risk of infections. The diagnosis of CLL can only be established if the total number of B lymphocytes is above 5 × 109/L. 1 Leukemia has 4 major types of categories, which are acute lymphocytic leukemia (ALL), acute myeloblastic leukemia (AML), chronic lymphocytic leukemia (CLL), and chronic myeloblastic leukemia (CML). Each main type of leukemia is named according to the type of cell that is affected (lymphoid cells or myeloid cells) and whether the disease begins with a mature or immature cell. Acute leukemia was rapidly growing and can overrun the body within a few weeks or months. In contrast, chronic leukemia is growing slowly and progressively worsening over the years. 2
Globally, CLL affected about 904 000 people in 2015 and resulted in 60 700 deaths. It is the most prevalent adult leukemia diagnosed in the western world, with an estimated 20 110 new cases in 2017 and accounting for 25% to 30% of all leukemia. 3 With an incidence of 4.1 per 10 000 persons per year the disease displays a high heterogeneity in its clinical course, patients presenting with an indolent form often do not require treatment, whereas others experience a very aggressive course, leading to death within a month. 4
In Africa, an estimated 119 386 people lived with chronic lymphocytic leukemia (CLL), a disease of the blood and marrow an estimated 15 720 people were expected to be diagnosed with CLL in 2014. 5 In Ethiopia, the magnitude of chronic lymphocytic leukemia did not be well studied, but according to the early study of leukemia in adult Ethiopian Shambo in the 1990s in Tikur Anbessa (black lion), a specialized hospital in Addis Ababa chronic lymphocytic leukemia (CLL) accounts 21.1% of each of other types of leukemia.6,7 Chronic lymphocytic leukemia is an increasingly common problem and is associated with high morbidity and mortality in Ethiopia. Patients who died from CLL increase from time to time. 8 However, there is a limited study to identify the determinants of chronic lymphocytic leukemia patients. The current CLL therapies are either symptomatic treatments like chemotherapy and immunotherapy that do not improve complete remission rates or effective treatments that target actual cancer but have excessive morbidity and toxicity rates. The etiology of CLL is unknown, no virus or oncogene is involved in its pathogenesis. Moreover, the optimal sequencing of drug combinations is unknown. 6 Relationships between various chemicals, drugs, other environmental agents, and the development of disease are much less well established for CLL than for other forms of leukemia. 9 However, there are few known risk factors for CLL include occupational causes by exposure to certain chemicals, radiation exposure, and tobacco users. 10 There is a scarcity of research conducted previously about the progression of WBC among chronic lymphocytic leukemia patients in the study area. Therefore, this study was aimed to investigate determinants of progression of WBC of chronic lymphocytic leukemia patients under treatment at Felege Hiwot Referral Hospital, northwest Ethiopia.
Materials and Methods
Description of the study area and design
This study was conducted at Felege Hiwot Referral Hospital, Bahir Dar, northwest Ethiopia. The area is located 563 km from Addis Ababa, the capital city of the country. This hospital also serves as a referral hospital for the people who are referred from different districts. 11 A retrospective study design was carried out to retrieve relevant information from the medical records of chronic lymphocytic leukemia patients to address the objective of the current investigation.
Source of population and data
The chronic lymphocytic leukemia patients were the source of the population for this study. The data was collected from the medical chart of chronic lymphocytic leukemia patients at the hospital under treatment from January 2017 to December 2019. The longitudinal were extracted from the patient’s chart which contains socio-demographic and clinical information of all chronic lymphocytic leukemia patients under follow-ups. Hence, the data for the current investigation was secondary.
Quality of data measurement
The data collection tool was pre-tested before the actual data collection to maintain data quality. Pre-testing is testing the validity, reliability, practicability and sensitivity of the tool before it is used for actual data collection. The completeness and consistency of questions related to secondary data were checked and pre-tested on 35 sample data and proper amendments were included after getting feedback from the pilot test. Data cleaning was performed daily and timely feedback was communicated to the data collectors.
Sample size
Patients who attended a minimum of 2 follow-up during the period 1 January 2017 to 31 December 2019 Bahir Dar, northwest Ethiopia was included in the study. Therefore, among the total of 1295 chronic lymphocytic leukemia patients registered from 1 January 2017 to 31 December 2019, only 312 chronic lymphocytic leukemia patients satisfy inclusion criteria and hence are included in this study. The longitudinal WBC count were measured every 4 months at 0 (baseline), 4, 8, 12, 16, 20, 24, 28, 32, and 36 month visits (so that
Variables in the Study
Response variables
The response variable was the longitudinal count of the progression of WBC among chronic lymphocytic leukemia patients. It is measured in WBC count ×
Independent variables
The independent variables in the current investigation were socio-demographic variables and clinical factors.
➢ Socio-demographic variables and their codes
● Sex (Female = 0 and Male = 1) ● Place of residence (Urban = 0 and Rural = 1) ● Age is a continuous variable measured in years. ● Educational level (0 = illiterate and 1 = literate) ● Marital status (0 = single, 1 = married, and 2 = widowed/divorced)
➢ Clinical variables
● Platelet is a continuous variable measured in platelet count × ● Hemoglobin is a continuous variable measured in ● Hematocrit is a continuous variable measured in percent. ● Lymphocyte is a continuous variable measured in number /µL. ● Red blood cell is a continuous variable measured in RBC count × ● Stage of CLL (0 = low, 1 = medium, and 2 = high) ● Presence of anemia (0 = no and 1 = yes)
Operational definition
For most cancers, staging is the process of finding out how far the cancer has spread. Stages are often useful because they can help guide treatment and determine a person’s outlook. Most types of cancer are staged based on the size of the tumor and how far the cancer has spread. Doctors separate the Rai stages into low, intermediate (medium), and high-risk groups when determining treatment options. 12
Data processing and analysis
In this study, R 4.0.3 version software was considered for data analysis. A statistical decision was made at 5% of level of significance.
Statistical Models
Linear mixed-effect model
A linear mixed model is a parametric linear model for longitudinal or repeated measures data that quantifies the relationships between a continuous dependent variable and various predictor variables. It extends from the classical linear regression model that takes into account both fixed effect and random effect. The random effect contains subject-specific effects and the fixed effect contains the set of predictors that are fixed across the subjects or the same for all subjects. The fixed effect parameters describe the relationships of the predictors to the dependent variable for an entire population and random effects are specific to subjects within a population. Consequently, random effects are directly used in modeling the random variation in the dependent variable. 13 The random effects are not only determining the correlation structure between observations on the same subject but also taking into account heterogeneity among subjects, due to unobserved characteristics.
The general linear mixed-effects model defined as

Where,
✓
✓ β is a
✓
✓
✓
✓
The corresponding assumptions for model are
Results
The data consists of 312 patients who were chronic lymphocytic leukemia patients and treated under chronic lymphocytic leukemia follow-up between 1st January 2017 up to 31st December 2019 at FHRH, Bahir Dar, Ethiopia (Table 1).
Characteristics of categorical variables of chronic lymphocytic leukemia patients.

Assessment of normality assumption
We could observe that histogram of the original data seems to satisfy the assumption of normality. However, for the histogram of the log-transformed data, the assumption of normality was violated (Figure 1).
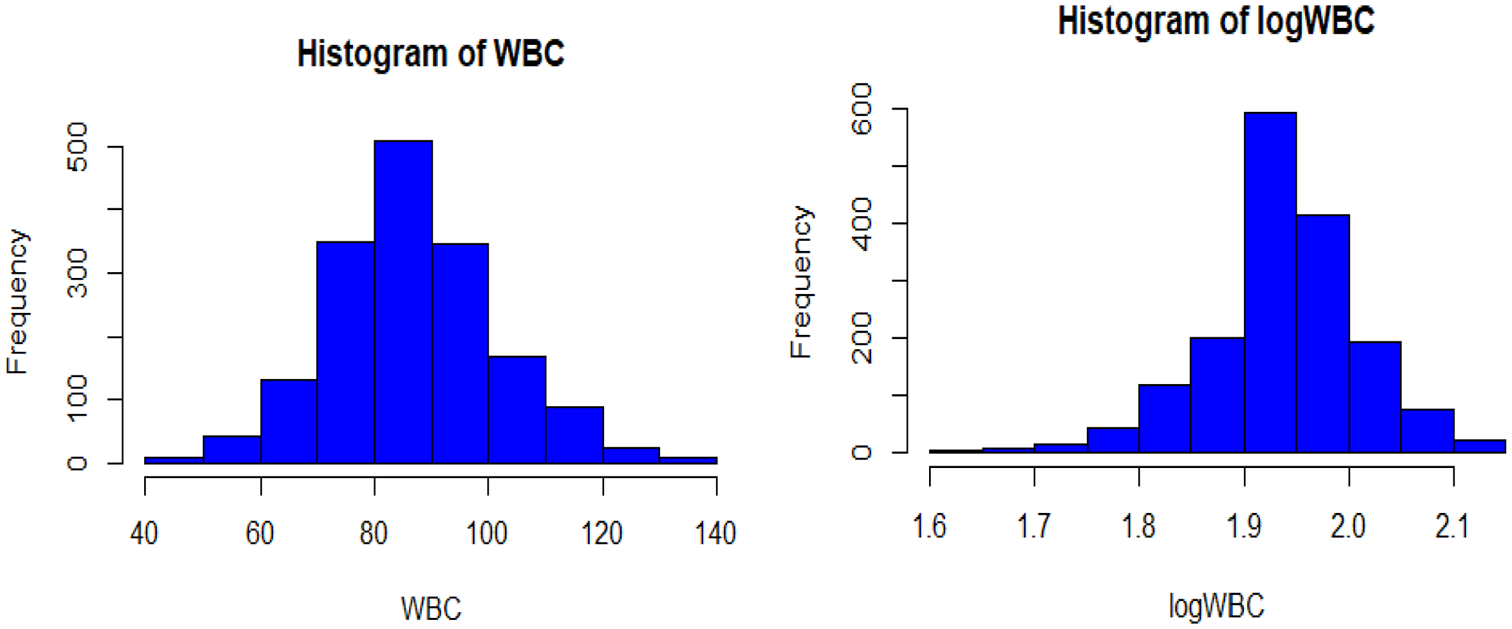
Histogram of actual WBC and log of WBC for CLL patients’ data.
The model with the smallest Akaike Information Criterion (AIC) and Bayesian Information Criterion (BIC) value of covariance structure. Therefore, an unstructured covariance structure was selected due to the smallest AIC and BIC compared to the remaining covariance structures (Table 2).
Comparison of covariance structure for linear mixed-effects model.

The random intercept and slope model allows the intercept and coefficient to vary randomly among individuals. That means the individual WBC count of chronic lymphocytic patients varies from visit to visit randomly. Therefore, the random intercept and slope model is a more parsimonious model for the linear mixed-effects model based on its lower values of AIC and BIC (Table 3).
Selection of random effects to be included in the linear mixed-effects model.

Univariable analysis for linear mixed model
Univariable analysis was performed to see the effect of each covariate on the progression of white blood cells by using purposeful variable selection in linear mixed effect model analysis and to select variables to be included in the multivariable analysis. Based on univariable analysis except for residence, all predictors were candidate variables for multivariable analysis of linear mixed models at 25 % level of significance.
Multivariable analysis for linear mixed model
Multivariable analysis of the linear mixed model was done by using all significant covariates at univariable analysis. Table 4 displays the result of the final linear mixed model, the result showed that the predictor age, sex, marital status, hemoglobin, platelets, lymphocyte, stage of CLL, RBC, and follow-up time were significantly associated with the average WBC of chronic lymphocytes leukemia patients at a 5% level of significance. The variability between patients was 100.20
Result of the final linear mixed model for CLL patients.

Abbreviation: Ref, reference category.
Significance at 5% of level of significance.
Discussion
The main objective of this study was to identify factors that affect the progression of WBC among chronic lymphocytic leukemia patients at Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia. In this study, the linear mixed-effects model for longitudinal WBC count was used. The assumption of normality was checked using the histogram by comparing the plot of original and log-transformed data of chronic lymphocytic leukemia patients. All plots of the original data indicate that there is no deviation from the normality assumption and no need for transformation. The data were analyzed using the linear mixed-effects model by incorporating subject-specific variability. In this study, the unstructured covariance structure and random intercept and slope model had a smaller AIC and BIC compared to other models.
For a year’s increase in age, the average WBC count of the patients was significantly increased by .17 ×
The average WBC count of the respondents whose marital status was widowed/divorced chronic lymphocytic leukemia patients were significantly higher by 3.30 ×
The average WBC count of the medium stage of chronic lymphocytic leukemia patients was significantly lower by 4.34 ×
For a unit increase in hemoglobin, the average WBC count of the patients was significantly increased by .15 ×
For a unit increase in lymphocytes, the average WBC count of the patients was significantly increased by .16 ×
For a unit increase in RBC, the average WBC count of the patients was significantly increased by .17 ×
Conclusion
The main goal of the current study was to identify the determinants of the progression of WBC among chronic lymphocytic leukemia patients at FHRH, Bahir Dar, Ethiopia. The data were collected from 312 chronic lymphocytic leukemia patients of medical charts at the hospital under follow-up from 1 January 2017 to 31 December 2019. The linear mixed model analysis showed that the predictor sex, age, marital status, CLL stage, hemoglobin, platelets, lymphocytes, RBC, and follow-up time (visits) were significantly associated with the progression of WBC among chronic lymphocytic leukemia patients. Therefore, health care providers should give due attention and prioritize those identified factors and give frequent counseling about improving the health of chronic lymphocytic leukemia patients.
Footnotes
Acknowledgements
The authors would like to thank the Amhara Region Health Bureau, Bahir Dar referral hospital and staff members at Felege Hiwot Referral Hospital for supporting the study by granting them access to their medical records. They would also like to extend their gratitude to the Bahir Dar University the Department of Statistics for carrying out the research.
Declaration of Conflicting Interests:
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding:
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Contributions
GDA has led the overall activities of the research process such as drafted the proposal, did the analysis, wrote the results, and prepared the manuscript. MWM, AST, DBB, and MAK participated in editing, analysis, prepared and critically revised the manuscript for its scientific content. All authors read and approved the final manuscript.
Data Availability Statement
Data available on request.
Ethics Consideration
The authors got an ethical approval certificate from Bahir Dar University Ethical approval committee, Bahir Dar, Ethiopia with Ref≠ BDU/14/2020 to use the secondary data related to patients. The Ethical approval certificate obtained in this committee can be attached upon request. Since the data used in the current investigation was secondary, there was no verbal or written consent from the participants.