
Abstract
Aim and objectives:
This study aimed to determine the impact of virtual reality glasses and ball squeezing methods on reducing pain and anxiety in adult patients undergoing short peripheral cannula placement.
Methods:
The pretest-posttest parallel group randomized controlled experimental study was conducted in a university hospital with 111 patients. Patients were randomly assigned to one of three groups: the VR group (n = 37), the ball squeezing group (n = 37), and the control group (n = 37). Descriptive information form, Numeric Rating Scale, Visual Analogue Scale for Anxiety, and State-Trait Anxiety Inventory-State were used for data collection.
Results:
There was no statistically significant difference between the groups in terms of sociodemographic characteristics (p > 0.05). The pain score of the patients in the control group was found to be statistically significantly higher than that of the patients in the virtual reality glasses and ball squeezing groups (p < 0.05). While the mean anxiety scores of the virtual reality glasses and ball squeezing groups significantly decreased after the intervention, they increased significantly in the control group (p < 0.05).
Conclusions:
The study found that virtual reality glasses and ball squeezing were effective distraction methods to reduce pain and anxiety in patients undergoing short peripheral cannula placement.
Introduction
Short peripheral cannula (SPC) placement is one of the most commonly used invasive procedures in healthcare. 1 Approximately two billion SPC placement are placed worldwide each year, 2 and 70%–80% of hospitalized patients undergo at least one SPC placement. 3 SPC placement, which provides rapid access to the bloodstream, is employed in a range of interventions, including intravenous fluid replacement, drug administration, transfusion of blood and blood products. 4 SPC placement, which is among the responsibilities of nurses, should be performed in a safe manner. 5 In order to maintain patient safety and determine the optimal cannula for a given patient, it is essential to consider a number of factors, including the patient’s condition, age, vascular characteristics, the region where the treatment is applied, and the purpose of the treatment.6,7
SPC placement is an intervention that causes pain, anxiety, and discomfort for patients.2,8 It is well established that pain and anxiety are conditions that affect each other, with the severity of one increasing the severity of the other. 9 It is possible that the pain experienced by the patient during SPC placement may increase their anxiety, which in turn may cause vasoconstriction. This may result in the vessels being more difficult to see and palpate, which may ultimately lead to the failure of the procedure.8,10 The use of appropriate techniques, calming the patient, informing the patient, and distracting the patient during the SPC placement plays an important role in reducing pain and anxiety. 11
Among non-pharmacological methods, distraction techniques are the most widely used. In this method, pain and fear levels are reduced by focusing on another stimulus. 12 There are numerous cognitive and behavioral distraction techniques that are actively used to reduce pain in acute and chronic pain. 13 Some of these techniques include distraction cards, blowing soap bubbles, virtual reality glasses, animated educational films, music therapy, therapeutic toys, play-doh, ball spin, flippits, computer games, discussing the patient’s area of interest, and squeeze balls. 14 Previous studies have demonstrated the efficacy of distraction techniques during SPC placement in reducing pain8,15 –18 and anxiety. 17
Virtual reality (VR) represents an innovative approach with proven positive effects in painful interventions. 19 Its effect in pediatric patients has been frequently examined and it has been reported to reduce pain and anxiety related to SPC placement in children. However, studies evaluating its effect in adults are quite limited. Basak et al. 16 has found that VR glasses have reduced pain in adult patients undergoing SPC placement. Nevertheless, further study results are necessary to substantiate the effectiveness of VR glasses. Additionally, although the impact of distraction methods employed during SPC placement on pain in adult individuals has been extensively investigated, there are limited studies that elucidate the combined effect of pain and anxiety. Based on these considerations, the objective of the study was to analyze the impact of VR glasses and ball squeezing methods on pain and anxiety in adults undergoing SPC placement. Study hypotheses included the following:
• The mean pain score of the intervention group that received ball squeezing intervention during SPC placement is different from the control group.
• The mean pain score of the intervention group that received VR intervention during SPC placement is different from the control group.
• The mean anxiety score of the intervention group that received ball squeezing intervention during SPC placement is different from the control group.
• The mean anxiety score of the intervention group that received VR intervention during SPC placement is different from the control group.
Methods
Study design and setting
This study employed a pretest-posttest, parallel group randomized controlled experimental design. The trial was registered in ClinicalTrials.gov. Reporting was according to the CONSORT extension for parallel-group randomized trials (Figure 1). It was conducted at the general surgery clinic of a university hospital between July 15, 2023 and August 04, 2023. Patients, who were newly admitted to the clinic and decided to undergo SPC placement were included in the study. Prior to SPC placement, patients were randomly assigned to one of the three groups: the VR group, the ball squeezing group, and the control group. The control group received standard procedures. The VR group commenced watching a nature video for a period of 3 min, which concluded following the procedure. VR glasses compatible with smart mobile phones were used to watch the distracting 3D video. VR glasses removed the person from the environment by watching and listening to the video and helped him focus his attention on the image or sound. With the headphone feature in the glasses, ambient sounds were blocked and the patient could listen to the content he watched. The mobile phone was placed in the front part of the VR glasses. The VR glasses worn on the head are personalized thanks to their adjustable bands. The ball squeezing group was instructed to squeeze the stress ball just before the SPC placement, which also concluded following the procedure.
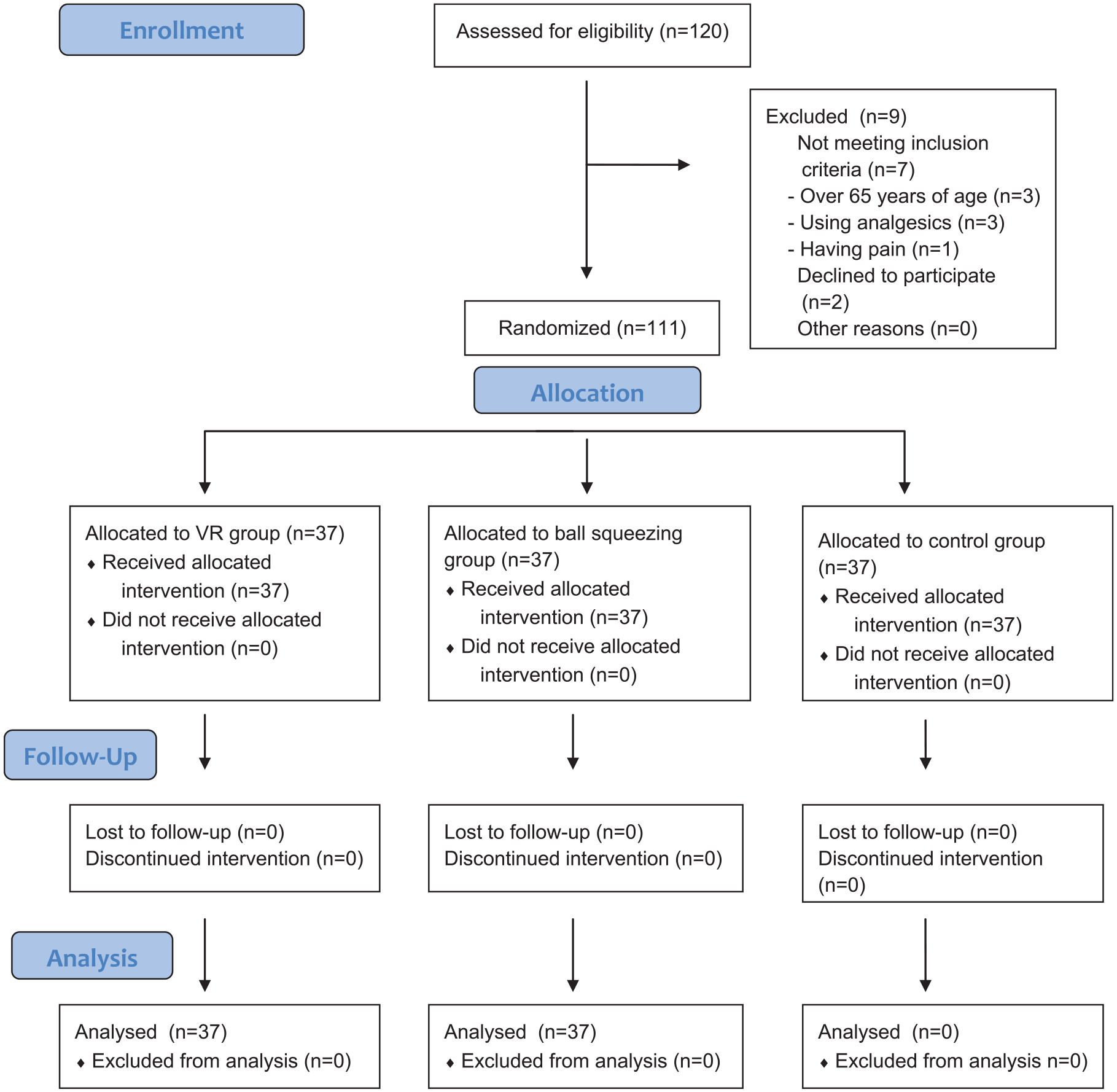
CONSORT flow diagram.
Participants
The sample size was calculated with reference to the pain scores obtained from the study conducted by Basak et al. 16 The G*Power software was used to calculate the sample size. Minimum sample size was found to be 99 for a 95% confidence interval (1−α), 95% power (1−β), and f = 0.203 effect size. Given the possibility of withdrawals, the sample size was increased by 10%. The final sample size was 111 patients, with 37 patients in each group.
The study included voluntary patients between the ages of 18 and 65 years who were literate and capable of squeezing stress balls. Patients who used chronic analgesic drugs, had chronic or acute pain, underwent SPC placement in the last month, had any scar tissue or infection in the areas to be used for SPC placement, had any diseases that influenced the feeling of pain, or exhibited signs of discomfort during SPC placement were excluded from the study. If SPC placement was unsuccessful, the participant was removed from the study.
Randomization and blinding
Patients were block randomized into the VR, ball squeezing, and the control group by a statistician who was not involved in the research project, using a computer program (https://www.randomizer.org) to ensure confidentiality and prevent bias.
Outcome measures
The results were measured twice, initially at the pretest stage and subsequently at the posttest stage. Prior to the commencement of the study, the patients were required to provide informed consent. At the pretest stage, a descriptive information form, Visual Analogue Scale for Anxiety (VAS-A), and State-Trait Anxiety Inventory-State (STAI-S) were completed by the patients. At the posttest stage, the Numeric Rating Scale (NRS), VAS-A, and STAI-S were utilized. The intervention tools employed in the study were the VR glasses and a stress ball.
Descriptive information form
The researchers prepared the form in accordance with the existing literature, which included six questions on age, gender, educational level, body mass index (BMI), and the arm and the site that the SPC placement was performed.15,16
Numeric Rating Scale (NRS)
The NRS is a frequently employed instrument for the assessment of pain intensity. The individual is presented with the scale and asked to select the number that most accurately reflects their pain on a horizontal line, ranging from 0 (no pain) to 10 (the worst pain).
Visual Analogue Scale for Anxiety (VAS-A)
The VAS-A is a 100-mm horizontal line with numbers ranging from 0 (no anxiety) to 100 (the worst anxiety). Participants are asked to place a mark on the line corresponding to their level of anxiety. The distance from the lowest level to the patient’s mark is measured with a ruler, and the numerical value of the anxiety level in centimeters or millimeters is obtained. 20 Various studies have proven the reliability and validity of the VAS-A to measure the level of anxiety.
State-Trait Anxiety Inventory-State (STAI-S)
The STAI-S is a 20-item scale designed to ascertain the individual’s emotional state at a specific point in time and under specific circumstances. Each item is scored on a 4-point Likert scale, ranging from 1 (almost never) to 4 (almost always). The possible scores range from 20 to 80, with higher scores indicating a higher level of state anxiety.21,22
SPC placement procedure
Prior to the procedure, the patient’s hands were washed and gloves were worn. The patient was positioned in an appropriate manner. A suitable vessel was selected by palpation and inspection on the right or left arm. A tourniquet was tied approximately 10–15 cm above the site of vascular access. The area to be entered was wiped with 70% alcohol. The skin in the area where the vein was to be entered was stretched. The SPC was inserted approximately 1 cm below the area with a 30–45-degree angle and the angle was subsequently reduced to 15° following the insertion. The guide needle in the cannula was pulled back 1 cm, and the presence of blood in the plastic cannula was observed. When blood was detected, the guide needle was slowly withdrawn while the plastic cannula was advanced in the vein. Once the tourniquet had been removed, the guide needle was completely removed. Subsequently, the cannula was secured in place with a plaster.16,23 During the procedure, the palpation method was used to identify the vein. Imaging methods such as ultrasonography were not used.
Ethical considerations
Prior to the commencement of the study, permission was obtained from the Scientific Research Ethics Committee of the university (Date: 02.11.2022, Number: 2022/316) and the hospital. The trial was registered with the United States National Institutes of Health Clinical Trials Registry (NCT05769647). All participants were informed of the study’s purpose, the voluntary nature of their participation, their right to withdraw from the study at any time, and the confidentiality of their identity information. Written informed consent was obtained using an informed consent form prepared in accordance with the principles of the Declaration of Helsinki.
Data analysis
The data were analyzed using SPSS version 23.0. Quantitative data were presented as the mean, standard deviation, and median, while categorical data were presented as frequency. The chi-square, Kruskal-Wallis, analysis of variance (ANOVA), and independent sample t-test were used to compare the categorical variables. Post hoc analyses were conducted using the Tukey’s and Scheffe tests. The significance level was set at p < 0.05.
Results
Table 1 presented the sociodemographic characteristics of the participants in all the three groups. There was no statistically significant difference between the groups in terms of sociodemographic characteristics (p > 0.05).
Comparison of demographic characteristics of VR, ball squeezing, and control groups.
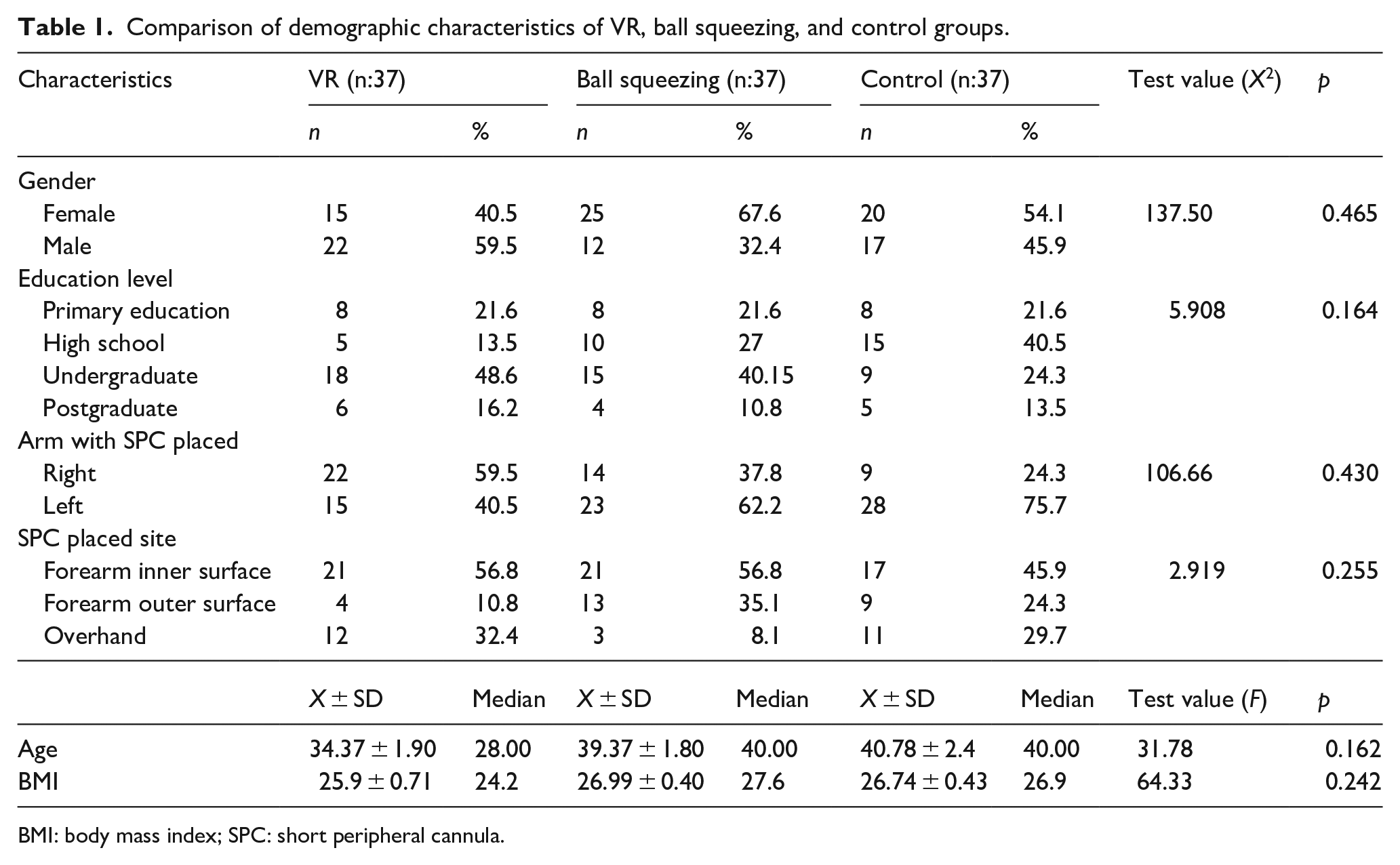
BMI: body mass index; SPC: short peripheral cannula.
Table 2 presented the mean scores obtained from the NRS. The mean pain scores of the VR, ball squeezing, and control groups were 1.94 ± 0.40, 0.85 ± 0.23, and 2.80 ± 0.360, respectively. The NRS scores of the control group were statistically significantly higher than those of the VR and ball squeezing groups (p < 0.05; Table 2).
Comparison of pain score averages of groups.

p < 0.05, VR: Virtual reality, BS: Ball squeezing
Table 3 presented the pretest and posttest scores obtained from the VAS-A. The mean pretest and posttest VAS-A scores obtained by the VR group decreased from 89.54 ± 7.19 to 66.60 ± 19.24. The mean pretest and posttest VAS-A scores obtained by the ball squeezing group were 68.45 ± 11.47 and 55.50 ± 10.36, respectively. In contrast, the mean pretest and posttest VAS-A scores of the control group increased from 84.34 ± 16.28 to 94.67 ± 13.32, respectively. Although there was a statistically significant decrease between the pretest and posttest VAS-A scores of the VR and the ball squeezing groups, we found a statistically significant increase between the pretest and posttest VAS-A scores of the control group (p < 0.05).
Comparison of anxiety score averages of groups.
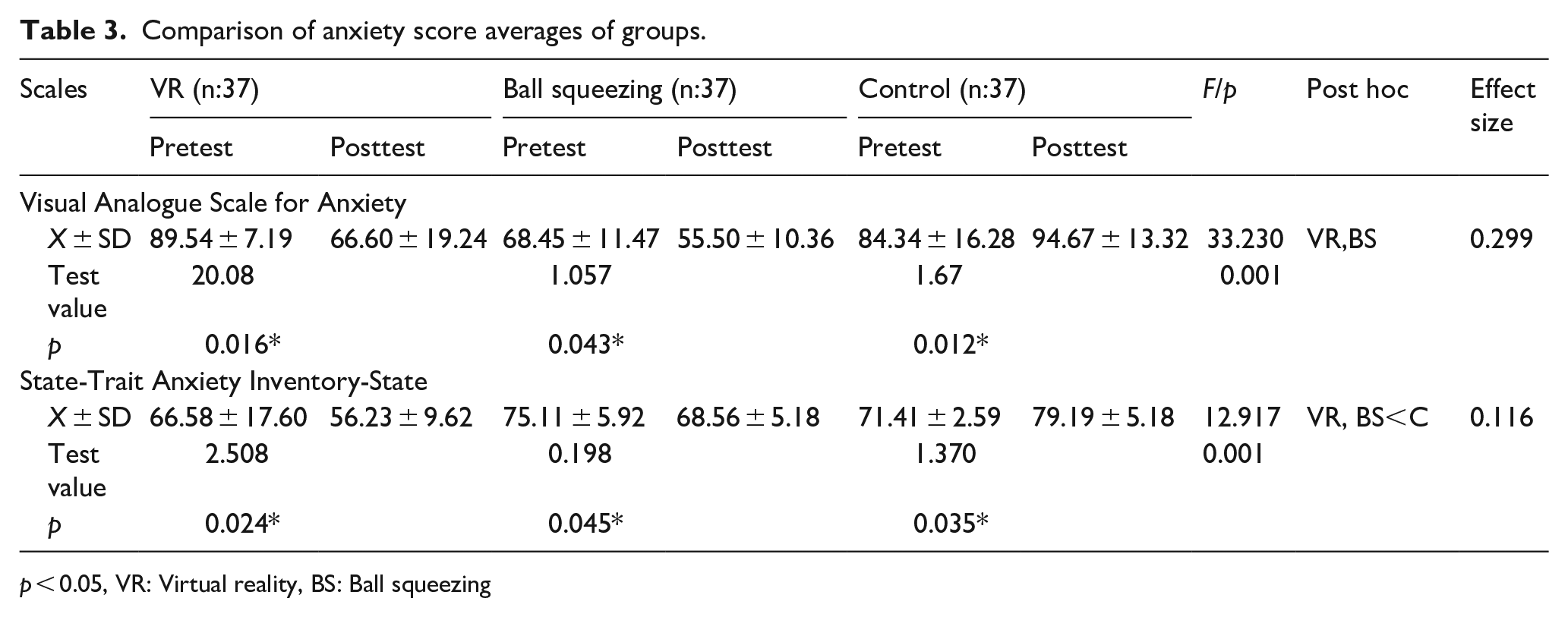
p < 0.05, VR: Virtual reality, BS: Ball squeezing
Table 3 also presented the scores obtained from the STAI-S. The mean pretest and posttest STAI-S scores for the VR group were 66.58 ± 17.60 and 56.23 ± 9.62, respectively. The same scores for the ball squeezing group were 75.11 ± 5.92 and 68.56 ± 5.18, respectively. Finally, the mean pretest and posttest STAI-S scores of the control group were 75.11 ± 5.92 and 68.56 ± 5.18, respectively. Although the posttest STAI-S scores of the VR and ball squeezing groups were statistically significantly lower than their pretest scores, we found that the posttest STAI-S scores of the control group were statistically significantly higher than their pretest scores (p < 0.05).
Discussion
This study analyzed the efficacy of the VR glasses and ball squeezing distraction methods on pain and anxiety levels of adult patients undergoing SPC placement. The study found that the pain levels of the intervention groups that received VR and ball squeezing interventions during the SPC placement were statistically significantly lower than the control group. The efficacy of the techniques employed to alleviate discomfort associated with SPC placement in adults has been evaluated in a limited number of studies. Basak et al. 16 demonstrated that the pain levels of patients, who received optical illusion images and VR glasses as distraction methods during SPC placement, were significantly lower than those of the control group. Yılmaz Koçak and Kaya 24 found that the distraction methods of couching and VR were effective in pain management and increasing the level of patient satisfaction. Similarly, Alan and Khorshid 8 reported that the valsalva maneuver can be utilized as a non-pharmacological method to reduce pain during SPC placement. Balanyuk et al. 15 had also underlined the importance of distraction methods during SPC placement in reducing pain compared to local analgesics. In a separate study, Yılmaz and Güneş 18 demonstrated that squeezing a stress ball was an efficacious method for alleviating discomfort during SPC placement. Additionally, Basak et al. 2 reported that rose oil aromatherapy and hand-holding interventions were found to be effective in reducing pain during SPC placement.
A review of the literature reveals a considerable number of studies that have examined the effect of distraction methods on pain in children. These studies have demonstrated the efficacy of VR glasses19,25,26 and other distraction methods, including cartoon watching, 27 computer games, 28 kaleidoscopes, 29 blowing soap bubbles, and ball squeezing 30 in reducing pain levels during SPC placement.
The results of this study indicate that patients, who received VR and ball squeezing interventions, exhibited lower levels of anxiety than those in the control group. To date, a limited number of studies have analyzed the impact of distraction methods on the anxiety levels of adult patients during SPC placement. Fusco et al. 17 analyzed the effect of three types of communication, including hypnotic communication and negative and neutral connotations, on pain, comfort, and anxiety in patients undergoing SPC placement and found that hypnotic communication was an effective intervention to reduce pain and anxiety. Additionally, VR glasses have been demonstrated to be an effective distraction method in other interventions. For instance, Sikka et al. 31 demonstrated that the use of VR glasses was an effective method to reduce anxiety and pain in patients admitted to the emergency department. Similarly, Glennon et al. 32 reported that the use of VR glasses was an effective distraction method to reduce pain and anxiety in patients undergoing a bone marrow aspiration and biopsy. Other studies have also demonstrated the effectiveness of squeezing a ball in reducing anxiety levels. For instance, the study by Hudson et al. 33 on the effects of simple distraction interventions on pain and anxiety experienced during conscious surgery demonstrated that intraoperative anxiety ratings were significantly lower when participants interacted with nurses, used stress balls, or watched a DVD during surgery compared to treatment as usual.
Studies on children have demonstrated the effectiveness of VR glasses and ball squeezing in reducing pain and anxiety. Gold et al. 19 reported that VR glasses were an effective distraction method to reduce anxiety during SPC placement. Girgin and Göl 34 found that balloon inflation, ball squeezing, and couching were effective in reducing anxiety during venipuncture. Similarly, Oluç and Sarialioğlu 35 demonstrated that therapeutic play with a hand puppet was an effective method for reducing the level of pain and fear associated with the blood collection process.
As can be seen, the effectiveness of distraction methods in reducing pain and anxiety due to SPC placement has been demonstrated in the relevant literature. However, in addition to distracting methods, procedure success and procedure duration are very important in reducing pain and anxiety. Because these are directly related to the degree of tissue trauma. For this reason, bedside ultrasonography and near infrared light devices have begun to be used in recent years. 36 Not using these methods in this study may have affected the severity of pain and anxiety by increasing tissue trauma. It is recommended that this situation be taken into account in future studies.
Limitations
The study is limited in two ways. First, the study was conducted on young adults, so the findings may not be generalized to children and elderly individuals. Secondly, not using vein imaging methods such as ultrasonography during the procedure may have increased procedure time and tissue trauma.
Conclusions
This study found that the use of VR glasses and ball squeezing during SPC placement were effective distraction methods to reduce pain and anxiety in adult patients. Based on these findings, we recommend VR glasses and ball squeezing, especially in patients who experience fear during SPC placement. Thus, disruptions in the patient’s treatment process are prevented. In addition, low-cost VR can be used in healthcare institutions that cannot access technology due to insufficient healthcare resources, especially in special patient groups such as cancer and pediatrics, although not for all patients. Funding for this can be obtained from international organizations that provide financial support.
Further experimental studies comparing these methods with different non-pharmacological methods can be conducted. In particular, the results of studies examining the effect of distraction methods used during SPC placement on anxiety are needed. Additionally, similar studies can be performed using vein imaging methods such as ultrasonography. Finally, training sessions that increase the nurses’ awareness of distraction methods may be organized.
Footnotes
Acknowledgements
The authors sincerely thank all the patients who participated in this study and Necmettin Erbakan University Scientific Research Projects Coordinatorship.
Author contributions
Mihriban Rişvan: Conceptualization, Formal analysis, Methodology, Writing—original draft, Writing—review & editing. Serpil Su: Conceptualization, Formal analysis, Methodology, Project administration, Writing—original draft, Writing—review & editing.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Necmettin Erbakan University Scientific Research Projects Coordinatorship with grant number 22139001.
Ethical approval
Ethical approval was obtained from the Health Sciences Scientific Research Ethics Committee of the Necmettin Erbakan University (Date: 02.11.2022, Number: 2022/316). Institutional permission was obtained from the Necmettin Erbakan University Faculty of Medicine Hospital.
Informed consent
Written informed consent was obtained using a voluntary informed consent form prepared in accordance with the principles of the Declaration of Helsinki.
Consent to publish
Participants signed informed consent regarding publishing their data.
Clinical trials registration
ClinicalTrials. gov (identifier: NCT05769647).