
Abstract
Background:
A major contributor to peripheral intravenous catheter (PIVC) failure may be related to PIVC movement within the vein which is associated with vein wall damage. The magnitude of PIVC movement against the vein wall has not previously been quantified. This study aimed to examine PIVC movement within the vein when minor forces were applied to the PIVC.
Methods:
This was a prospective, pilot trial including healthy volunteers in an outpatient research laboratory. The primary objective was to examine the in movement (millimeters) of the PIVC using ultrasound with external pull forces (4, 5, and 6 lbs; 1.8, 2.3, and 2.7 kg, respectively) applied to the PIVC in random order.
Results:
Participants (N = 11) were aged 40.36 ± 16.10 years with 54.55% being Male. Mean ± SD PIVC movement for 4, 5, and 6 lbs of force was 4.65 ± 1.88, 3.88 ± 2.28, and 5.25 ± 2.06 mm, respectively. There was substantial PIVC movement when a force was applied to the PIVC, but no statistically significant difference between 4, 5, and 6 lb forces (p > 0.05).
Conclusion:
When external pull forces were applied to the PIVC, substantial PIVC movement within the vein occurred in a healthy population. Strategies that reduce PIVC movement and/or remove or limit external pull forces from the PIVC are needed. Future studies on hospitalized patients are warranted to quantify vein wall injury and PIVC failure due to PIVC movement from various pull forces.
Keywords
Introduction
Placement of peripheral intravenous catheters (PIVC) is the most common invasive procedure in hospitals worldwide, with 60%–90% of patients receiving a PIVC when going to the hospital. This translates into over 235 million PIVCs placed in the United States and 2 billion globally each year. Despite the frequency of insertions and heavy reliance on these devices to deliver therapeutics, the rate of PIVC failures is alarmingly high. It ranges from 36% to 63% in randomized controlled trials, with an average failure rate of 46%. 1 PIVC failure often leads to PIVC restarts that require additional nursing time, medical supplies, and needlesticks for patients.2,3 In addition, the average hospital length of stay for acute care in the United States is 5.5 days, 4 and the average lifespan of a PIVC is between 1 and 4 days.5–7 As a result, many patients have multiple PIVCs during their hospital stay 5 leading to unnecessary procedures, cost, and poor patient satisfaction.8–10
Developing solutions to decrease the burden of poor PIVC outcomes requires understanding the mechanisms that lead to failure. There are multiple modes of PIVC failure including infiltration, phlebitis, occlusion, mechanical failure, dislodgment, and infection.1,10 While a minority of failure is related to improper flushing (i.e. occlusion) or kinking (i.e. mechanical failure) of the PIVC, a major contributor to the more frequently occurring complications may be related to the PIVC movement and injury to the vein wall. 11 Evidence illustrates that contact of the PIVC tip with the vein wall triggers an inflammatory reaction within and around the vein and PIVC, leading to complications and failure.12,13
It has been postulated that basic movements of the patient’s arm may trigger friction at the level of the PIVC within the vein and precipitate the progress to failure. 14 While these PIVC movements have been loosely described in the literature, the magnitude of the movement of the PIVC and the contact against the vein wall has not previously been qualified or quantified. Thus, this study aimed to examine the movement of a PIVC within the vein using dynamic ultrasound imaging when minor forces were applied.
Methods
Study design, participants, and setting
This was a prospective, pilot, blinded trial including healthy adult (⩾18 years of age) volunteers that was conducted in an outpatient lab. Participants were excluded if they were currently using steroids and/or anti-coagulation medications, had habitual intravenous drug use, or had an allergy to a skin adhesive. The study was approved by the Advarra Institutional Review Board as a nonsignificant risk device study. All participants provided written informed consent prior to enrollment.
Study objectives
The primary objective was to examine the movement (millimeters) of the PIVC with the application of external pull forces (4, 5, and 6 lbs; 1.8, 2.3, and 2.7 kg, respectively). The movement was calculated as the change in PIVC length within the vein from the neutral position (no force) to the secondary position with the force applied. Secondary objectives were to (1) explore predictors of PIVC movement related to patient characteristics and (2) to describe tip movement in relationship to the vein wall with a pull force of 4 lb and explore differences between tip movement and PIVC angle between patients who had vein wall contact versus those who did not.
Study procedures
Participant’s demographic information was collected in addition to smoking status, body mass index (BMI), comorbidities, previous significant weight loss ⩾50 pounds, and a skin turgor test was performed. 15 An ultrasound assessment was also performed to identify an appropriate vein to use for the study (M9 Ultrasound System, Mindray North America, Mahwah, NJ). Once an appropriate vein was identified, a 20 gauge 1.25″ (Introcan Safety® Straight IV Catheter, B. Braun Medical, Inc., Bethlehem, PA) PIVC was aseptically placed. A 7″ extension tubing was attached to the PIVC via a luer connection, and the extension tubing contained a sliding clamp and a needleless connector on the opposite end (TKO, Nexus Medical, LLC Lenexa, KS). A drop of cyanoacrylate glue (SecureportIV®, Adhezion Biomedical®, Wyomissing, PA) was placed at the PIVC insertion point. The PIVC was secured in place using a borderless 6 cm × 7 cm adhesive dressing (Tegaderm™ 1624W, 3M™, St. Paul, MN), with gum mastic (Mastisol®, Eloquest Healthcare®, Ferndale, MI) applied to the entire area underneath the dressing.
The participant’s arm was then placed in a test fixture and secured by Velcro straps. The test fixture was mounted with a sliding mechanism that allowed a pull force of 4, 5, or 6 lb to be applied at a 20-degree angle from the axis of the patient’s arm pulling in the distal direction. The sliding mechanism was fitted with a force gauge (Mxmoonfree ZMF-5N, China) (Figure 1).
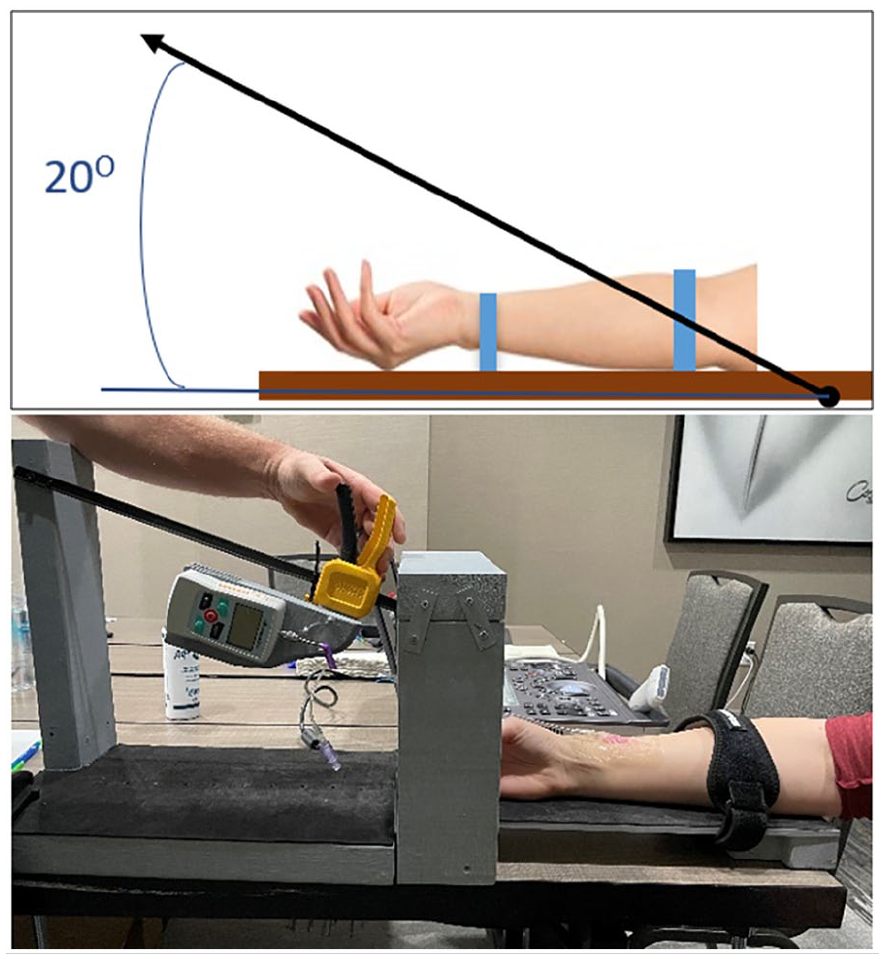
Graphic and actual representation of the test fixture with an arm in place. Top image: this graphic representation of the test figure demonstrates an arm secured to the fixture by two straps (blue lines). The black arrow represents the direction of the pulling force, where there is a 20° angle from the axis of the patients arm to the pull. Bottom image: Actual image of the device used in the study.
The 20-degree angle pull on the PIVC was selected based on the study team’s clinical experience and represents a clinically realistic situation regarding forces placed on PIVCs. A previous study which included the four market leading adhesives concluded that pull forces <4 lbs were associated with activities of daily living (e.g. bathing, eating, grooming) and pull forces ⩾4 lbs were likely harmful forces that could lead to PIVC failure. Authors from this study also concluded that PIVC securement dressings tend to completely dislodge due to a pull force as low as 6 lb, but more commonly at pull forces ⩾8 lb. 16 Based on this information, pull forces of 4, 5, and 6 lbs were selected for this study.
The order of pull forces (4, 5, or 6 lb) applied to each participant’s arm was randomized. The ultrasound technician captured a baseline measurement of the length of PIVC in the vein by ultrasound in long axis orientation and angle of distal catheter tip against the proximate vein wall (Figure 2). A second investigator, the equipment technician, applied the pull force per the randomization scheme, monitored the force gauge to ensure the desired pull force. In parallel, the ultrasound technician, utilizing the ultrasound, brought the PIVC into view with the pull force applied to the line and recorded the length of the PIVC remaining in the vein capturing clips of the PIVC pre- and post-force application of the entire process of the external force application. All images captured by the ultrasound technician were later reviewed and interpreted by a blinded expert reviewer.
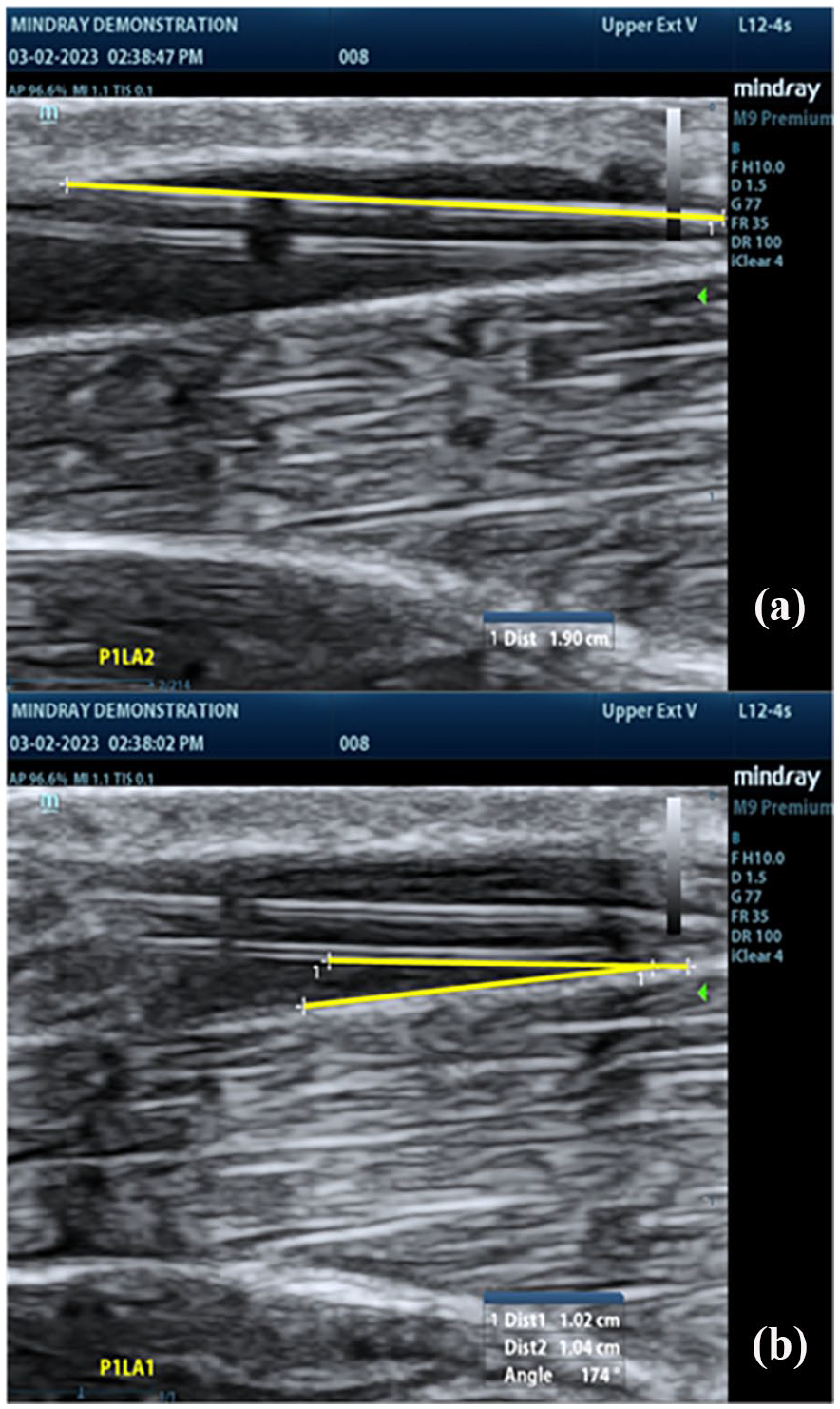
Example measurements for catheter length in vein and catheter angle. A peripheral intravenous catheter (PIVC) captured via ultrasound using a linear probe in the long-axis orientation: (a) yellow line representing the measurement of the length of the PIVC in the vein and (b) yellow lines representing the measurement of the angle of the PIVC in the vein.
After the first pull force was released from the PIVC, the ultrasound technician “reset” the PIVC in the vein by applying light pressure from distal to proximal to the PIVC hub through the dressing. Then, a new baseline measurement was recorded for the length of PIVC in the vein. A resting period lasting a minimum of 1 min took place before another pull force was placed on the PIVC. This process was repeated for each of the randomized pull forces of 4, 5, and 6 lbs.
A fourth pull force of 4 lbs. was applied to the PIVC and the movement of the PIVC was video recorded via ultrasound. Next, the participant’s PIVC was removed with the assistance of an adhesive removal (Detachol®, Eloquest Healthcare®, Ferndale, MI) and a bandaged applied.
Data source/measurement
The data retrieval process involved direct collection from participants and digital review and interpretation by investigators of saved ultrasound images and videos of PIVCs. Researchers collected data on paper data collection forms regarding patient demographics, relevant clinical history variables, and preliminary ultrasound measurements. De-identified ultrasound clips were reviewed by a blinded reviewer, a board certified, fellowship trained expert in vascular ultrasound, to finalize all measurements and interpret videos describing the 4 lb force on the vein wall using a predetermined key (secondary objective). This reviewer had access to the preliminary ultrasound technician measurements with the accompanying ultrasound images. Both the ultrasound technician and the reviewer were blinded to pull force and participant level data.
Randomization and blinding
The order of the external pull forces applied (i.e. 4, 5, and 6 lb; 1.8, 2.3, and 2.7 kg) were randomized to minimize or prevent ordering effects. The randomization plan was developed using www.Randomization.com. The participant as well as the ultrasound technician capturing the ultrasound images and PIVC length measurements were blinded to the order of the forces being applied. The final image reviewer was also blinded to the forces. The participant was blinded to prevent reactivity bias due to anticipation of an increase or decrease in force being applied to the PIVC.
Statistical methods
Sample size recommendations for standalone benchmark studies established by Sauro 17 was used to determine an adequate sample size. For standalone benchmark studies, it is recommended that 10–15 patients are tested to achieve a margin of error of approximately 20% with 90% confidence for most metrics. Considering logistics and feasibility, the aim was to enroll 12 participants.
All data were checked for normality using the Shapiro-Wilk test as well as observed graphically using Q-Q plots and histograms. All data were normally distributed and therefore means and standard deviations (mean ± SD) summarized continuous data and frequencies, with percentages were used to describe categorical data. Primary measures of data dispersion including mean ± SD, minimum, maximum, range, and interquartile range were used to describe data dispersion of PIVC movement at 4, 5, and 6 lb (1.8, 2.3, and 2.7 kg, respectively) pull forces (primary objective).
The association between PIVC movement and participant characteristics including age, BMI, ethnicity, and smoking status was assessed. The secondary objective 1 was examined using a linear regression analysis and by comparing PIVC movement between the three pull forces (4, 5, and 6 lb) using repeated measures analysis of variance (ANOVA) for paired samples. Post-hoc analysis was performed with Bonferroni correction if a significant difference was found with the ANOVA test.
Frequencies and percentages were used to describe PIVC movement characteristics (secondary objective 2). These characteristics included: (1) movement without vein wall contact (Yes/No), (2) PIVC tip contacts vein wall transiently during movement, but not in final resting position (Yes/No), and (3) PIVC tip contacts vein wall with continued contact in resting position (Yes/No). PIVC movement and angle were compared between participants who had vein wall contact versus those who did not using an independent samples t-test. In addition, a logistic regression was used to adjust for PIVC angle when PIVC movement was compared and to adjust for PIVC depth when angle was compared. All analyses were performed using IBM Statistical Package for Social Sciences (Version 26.0). Alpha threshold was established at p < 0.05.
Results
Participants enrollment and data collection were completed in 1 day. Thirteen participants were enrolled, however, two were excluded and not included in the analysis. One participant had a PIVC kink under the skin after a pull and chose not to continue in the study, and another participant did not have an adequate vein to receive a PIVC. Included participants (N = 11) were aged 40.36 ± 16.10 years with the slight majority (54.55%) being Male. All participant characteristics are shown in Table 1. No PIVC in any participant dislodged.
Participant characteristics.
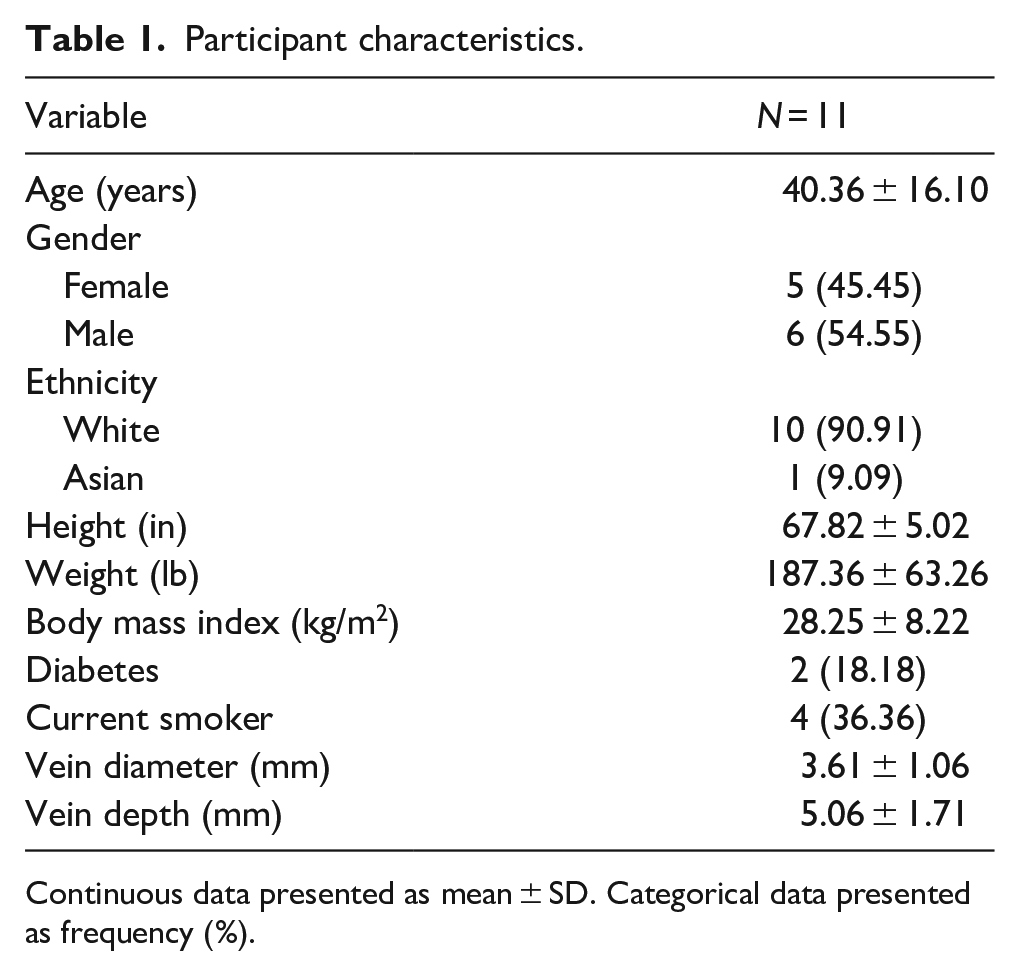
Continuous data presented as mean ± SD. Categorical data presented as frequency (%).
Shapiro-Wilk tests indicated that data did not significantly deviate from a normal distribution for 4 lb (p = 0.074), 5 lb (p = 0.183), or 6 lb (p = 0.378) pull forces. In addition, Q-Q plots and histograms for each of the forces indicated normal distribution of data. The primary measures of dispersion for PIVC movement due to external forces placed on the PIVC (primary objective) are shown in Table 2. PIVC movement was greatest after 6 lb, followed by 4 lb, and 5 lb pull forces. The dispersion of data was greatest for 5 lb pull forces.
Catheter length movement with 4, 5, and 6 lb pull forces applied to the PIVC.
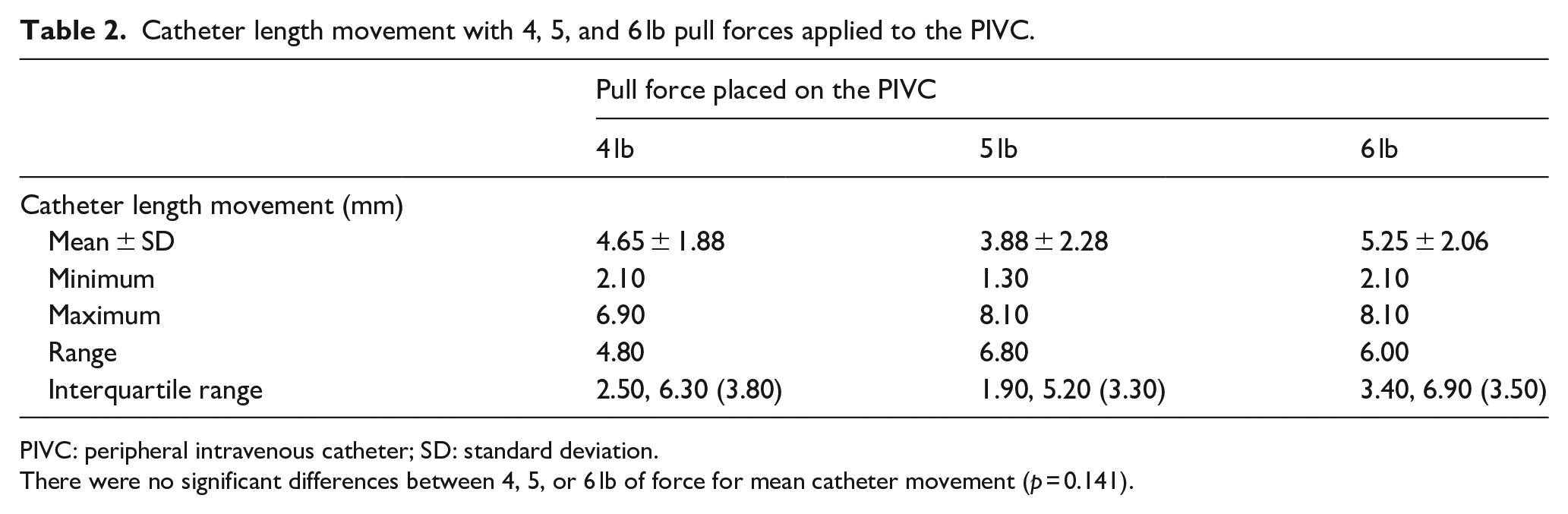
PIVC: peripheral intravenous catheter; SD: standard deviation.
There were no significant differences between 4, 5, or 6 lb of force for mean catheter movement (p = 0.141).
Exploratory analysis examining a priori potential predictors of PIVC movement at each force (secondary objective) did not find any significant associations (Table 3). There were also no statistically significant differences (F(2, 20) = 2.164, p = 0.141)) between each of the three forces for average PIVC movement (secondary objective). The PIVC tip contacted the vein wall and remained in contact with the vein wall in six participants (54.6%), while the PIVC tip moved without vein wall contact in the remaining five participants (45.5%). Participants with vein wall contact had significantly more PIVC movement compared to patients without vein wall contact (p = 0.040), which was no longer significant when adjusting for PIVC angle (p = 0.071; Supplemental Table). However, PIVC angle was not a significant covariate in the model. There were no significant differences (p > 0.05) between patients with versus without vein wall contact for PIVC angle with and without adjusting for vein depth (Supplemental Table).
Potential predictors of catheter movement (mm) at 4, 5, and 6 lb of pull force.
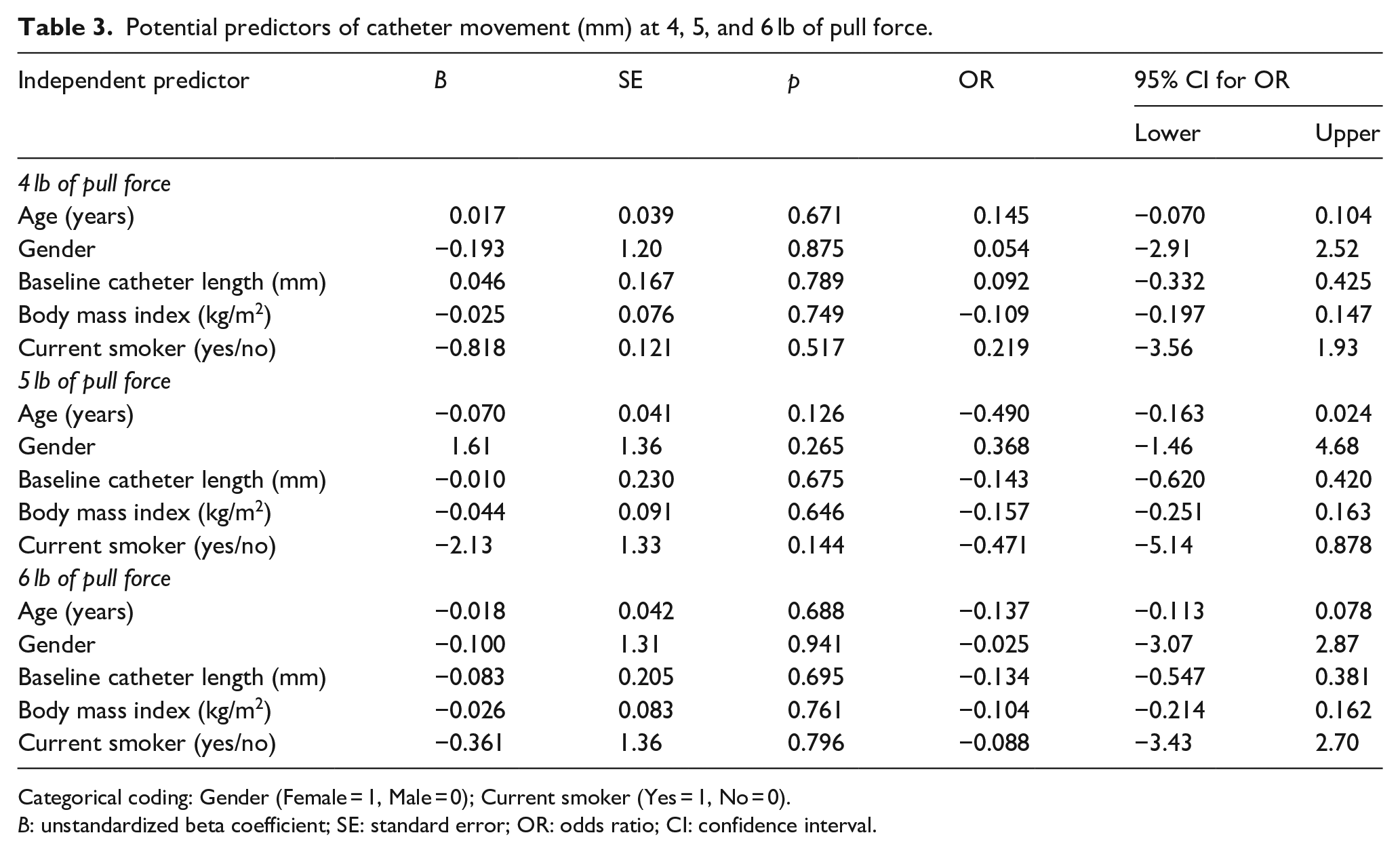
Categorical coding: Gender (Female = 1, Male = 0); Current smoker (Yes = 1, No = 0).
B: unstandardized beta coefficient; SE: standard error; OR: odds ratio; CI: confidence interval.
Limitations
The study had limitations to consider. While the sample size may have been adequate to establish benchmarking information, it was not powered for any of the secondary study objectives. Results from the analysis of secondary objectives may be used as pilot data for future studies with larger samples aiming to further examine the relationship between external forces, PIVC movement, and PIVC failure. In addition, the angle of the pull force was standardized to 20° from the arm in the distal direction. Pull forces on a PIVC in a clinical setting can occur from any angle and direction and therefore our findings may not be generalizable to all cases. The use of cyanoacrylate at the PIVC insertion site with the combination of gum mastic on the dressing was used to limit any migration of the PIVC at the skin level and prevent failure of the dressing with the external pull forces. These additional PIVC securements are well beyond what is commonly seen in clinical practice. Therefore, the PIVC movement recorded is likely an underestimation of what actually occurs at the bedside. Finally, as participants were healthy volunteers, the precise clinical consequences of this movement were not elucidated. Future studies should be conducted in the hospital setting with real patients rather than healthy volunteers.
Discussion
This study demonstrated that external pull forces on a PIVC of 4, 5, or 6 lbs (1.8, 2.3, and 2.7 kg, respectively) can cause substantial movement of the PIVC within the vein, ranging from 1.3 to 8.1 mm. PIVC movement was greatest after 6 lb, followed by 4 lb, and 5 lb pull forces, however there were no statistical differences in length of movement among the three applied forces. At a pull force of 4 lbs, video ultrasound showed that 54.6% of the PIVC made contact with the vein wall and remained in contact with the vein wall after the pull force was released. There was also a potential association between vein wall contact and greater PIVC movement.
Previous literature has described PIVC movement as unavoidable and a common occurrence due to patient activities of daily living and other traumatic forces. 13 However, to the best of our knowledge, this is the first study that empirically assessed the impact of specific forces on PIVC movement. Previous studies have indicated that pull forces above 4 lb are disruptive to the PIVC and dressing, potentially creating the need for a PIVC.2,16 In this study, a 4 lb pull force resulted in an average PIVC movement of 4.65 mm, a 5 lb pull force averaged 3.88 mm of movement, and a 6 lb pull force averaged 5.25 mm of movement. An unexpected finding was that the average movement of the PIVC on the 5 lb pull force was less than the 4 lb pull force. It was hypothesized that the distance a PIVC moved in the vein would increase based on the amount of external pull force that was placed on the line. A potential explanation of this unexpected finding may be due to the 5 lb pull force having the largest amount of data dispersion of the three applied forces. Perhaps a larger sample could have increased the precision of data for this particular force.
There are important clinical implications of this study. The movement of a PIVC in the vein can contribute to multiple mechanical complications: infiltration, mechanical phlebitis, occlusion, and dislodgement.17,19 Not only did this study quantify considerable PIVC movement with the application of defined forces, but it also illustrated that contact of the PIVC tip with the vein wall was frequent with movement and often persisted in the resting state. Evidence highlights that mechanical trauma to the vein wall is a core factor in propagating complications.18,19 On a subcutaneous level, laboratory models demonstrate that endovascular changes may begin immediately after PIVC insertion and progress significantly during the lifespan of a PIVC given this additional trauma to the vein wall secondary to PIVC movement.20,21 It is notable that inflammatory findings are a near ubiquitous in the PIVCs that fail. In fact, in one study, PIVCs failed in 85% of cases when these inflammatory findings were present on ultrasound, highlighting the critical importance of inflammation in the lifecycle of a failed PIVC. 20 Thus, reducing inflammation by restricting PIVC movement is critical to solving this problem.
In the hospital setting, patient movement is to be expected and external forces on the PIVC causing vein wall friction are likely to occur commonly. In one randomized controlled trial, forces greater than 4 lbs occurred 16.7% of the time. Notably, in the same trial, intentional reduction in PIVC movement resulted in decreased complications. Specifically, the use of a breakaway device in the PIVC that separates at 4 lbs of force showed reductions of 39% for infiltration, 58% for phlebitis, and 50% for dislodgement. 2 The idea behind the breakaway devices is to release the damaging force rather than hanging onto it. Thus, while complete prevention of movement is an impractical solution, technologies that can warn patients and staff about excessive stress or remove excessive stress on the PIVC may help mitigate complications. Other strategies aimed at reducing friction at the PIVC tip-vein wall junction such as improved stabilization/securement devices, improved PIVC composition, and longer PIVCs with a less acute angle against the vein wall may also be beneficial and require further inquiry.
Conclusions
This study demonstrated that external pull forces of 4, 5, and 6 lbs on a PIVC cause substantial movement of the PIVC within the vein in a healthy human population. As PIVC movement is strongly linked to complications and failure, it is prudent to seek strategies that reduce PIVC movement and the ensuing injury to the vein wall. Future studies on hospitalized patients with multi-directional pull forces are warranted to reveal the precise impact of the damage pull forces have on PIVC failure.
Supplemental Material
sj-docx-1-jva-10.1177_11297298231222052 – Supplemental material for Evaluating the impact of external forces on peripheral intravenous catheter movement using ultrasound: A randomized pilot study
Supplemental material, sj-docx-1-jva-10.1177_11297298231222052 for Evaluating the impact of external forces on peripheral intravenous catheter movement using ultrasound: A randomized pilot study by Amit Bahl, Vance Clement, Emily DiLoreto, Nicholas Mielke, Alexandria Carr, Gregory Panza and S. Matthew Gibson in The Journal of Vascular Access
Footnotes
Acknowledgements
The authors would like to thank Hailey Dirrigl, BSBME, MSBME for the design, and manufacturing of the fixture used to deliver and measure the force applied on the PIVC in this study.
Author contributions
AB, SG, and VC designed the study, had full access to the data, and take responsibility for the integrity and accuracy of the data analysis. GP contributed to data and statistical analysis. All authors contributed to the writing and editing of the manuscript. All authors contributed to data acquisition, analysis and interpretation, and all reviewed and approved the final version of the manuscript. The corresponding author attests that all listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Data sharing statement
The data that support the findings of this study are available via a data access agreement. Please contact the corresponding author (AB) for this request.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: AB has research grant support from B. Braun Medical, Becton-Dickinson, Teleflex, Adhezion, Medline Industries, Moderna, and Access Vascular. AB is a paid consultant for B. Braun Medical, Teleflex, Lineus Medical, and Interrad Medical. SG is a paid consultant for Lineus Medical, Nexus Medical, PICC Excellence, Beaumont Hospital, and Fujifilm Sonosite. VC and AC are employees of Lineus Medical. All other authors have nothing to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Lineus Medical.
Ethical approval
This study was approved by the Advarra Institutional Review Board.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.