
Abstract
Evidence of the costly effects of first-attempt peripheral intravenous catheter (PIVC) insertion failures continues to mount. This study was conducted to determine if a unique catheter design can improve operative error, promote PIVC first-stick success and reduce the costs of first-attempt failures. In Phase One of this comparative simulation use in vitro study, 16 nurses from acute care hospitals inserted four PIVC types into a training model, each type characterized by distinct timing of flashback occurrence and needle design. Each nurse performed three attempts per catheter type (12 total per inserter). Insertions were video-recorded and analyzed for the effect of the needle on a vessel during insertion, double punctures and catheter placement failure or success. In Phase Two, 100 nurses and 25 purchasing agents nationwide identified items used and associated costs for PIVC insertions. In Phase One, nurses using a grooved needle flashback with a thin-tipped needle were 20% more successful with catheter placement than those using a notched needle flashback and 22% more successful than those placing a capillary flashback design. Catheter placement success with a grooved needle flashback was 15% higher than with a capillary flashback and 13% higher than with a notched needle flashback. Double punctures were highest among nurses using a capillary flashback catheter, and catheter placement failure was highest among nurses using notched needle flashback. In Phase Two, nurses reported an average of 51% first-attempt success. The authors calculated the estimated annual cost of first-stick failure to be $US 35,919.15 per nurse, including labor and materials used in the second and third attempts. In this study, the authors found the insertion technique with grooved flashback needle design reduced operative error, double punctures and improved first-attempt success. This flashback needle design could significantly improve patient outcomes, speed time to treatment and reduce hospital costs.
Keywords
Introduction
Peripheral intravenous catheters (PIVCs) are the most frequently used invasive medical device in healthcare.1 –3 Each year, it is estimated that more than 350 million (M) PIVCs are purchased in the United States (USA) alone. 4 More than 90% of patients require some form of intravenous (IV) access during the hospital stay. 5 While PIVCs are critical to patient care, one published study reports that the average first-attempt success rate is approximately 76%. 6 Another study estimates that up to 2.35 insertions are required for each successfully placed PIVC, and first-stick success is as low as 44%.7,8 With 33M patients admitted to hospitals annually, almost 15M patients require multiple attempts. 9 Each additional attempt risks injury and contributes to rising healthcare costs. 10 Some researchers have focused on the PIVC procedure in clinical training and education to reduce risk and improve first-stick success.11,12 One change behavior study suggests clinicians seek solutions by adopting cutting-edge technologies to improve first-stick PIVC success rates using an evidence-based proactive (EBP) learning model initiative implementing near-infrared (NIR) technology. 13 In another study, first-stick success was improved through ultrasound-guided insertions. 7 Should assessment of the veins not allow access based on anatomy or palpation/visualization, ultrasound-guided PIVC placements on DIVA patients is an option. Clinicians comment on limited success with these technologies and describe training and access barriers. Achieving first-stick PIVC insertions remains challenging even with new technologies. 14 Functional barriers to accessing and using these technologies are related to various factors, including limited training opportunities.
Failed insertion attempts delay treatment initiation, contributing to negative patient outcomes and poor satisfaction while adding to healthcare costs.15 –18 Manufacturers continuously strive to produce improved product designs and processes to promote successful outcomes. Differing catheter and needle designs with cutting bevels and catheter flashback visualization technologies have been shown to improve first-stick success.19,20 Early recognition of vein entry was achieved through a notched needle and flashback design. Blood flashback appears when the needle enters the vein. PIVCs with a notched needle have a higher placement success rate compared to those without a notched needle flashback mechanism.19,20 Faster visualization of blood flashback reduces the likelihood of penetration of the posterior wall of the vein, thus reducing post-insertional complications.
Another needle flashback design utilizes a catheter capillary, with blood flashback appearing in the catheter after the catheter is advanced by threading it into the vein. 21 In one study, a capillary PIVC insertion was successful on the first attempt in 67% of the insertions, with an average of 1.57 puncture attempts. 22 The design provides confirmation of vein entry before the entire length of the catheter is fully threaded inside the vein. 21 Manufacturer device “Instructions for use” (IFU) recommend decreasing the insertion angle and advancing the PIVC when using both a notched or capillary flashback catheter.21,23 Following vein access and blood flashback, the catheter is fully advanced to ensure it is within the vessel. Successful access of the catheter into the vein is confirmed after blood flashback is achieved and the catheter is fully advanced.
A change to the insertion process and angle of insertion was not necessary for the third flashback type, a grooved flash device. 24 This flashback type is facilitated by a grooved needle, with flashback occurring along the catheter when inserted into the vein. One study using PIVCs equipped with grooved needle technology reported a significantly less insertional force and higher first-stick success rate for catheter placement compared to PIVCs without the grooved flash feature. 25
Device designs vary significantly based on the distinct attributes of flashback visualization timing. Given these differences, a lack of understanding of the use of each catheter can impact operative success rates. Earlier studies measured the effect of specific types of flashback technology and the impact of first-stick failure or success. 25 However, no studies to date have compared existing needle designs with newer flashback mechanisms in relation to first-stick success. In addition, earlier studies conducted with human subjects did not record visuals of real-time access and analyze the results of catheter insertion attempts.
Research shows first-stick PIVC failures contribute to the overall healthcare financial burden of $1.5 billion annually in the U.S., but the cost of first-stick failure alone was not measured.26 –28 This is the first study testing newer flashback technologies to measure and compare the performance in a vessel during insertion and the cost of first-stick failure.
This study was conducted to better understand the issues of PIVC catheter and needle designs for insertion success.
Methods
The aim of this research was to evaluate the performance of different needle bevel, flashback and catheter designs with simulated insertions of PIVCs performed by experienced nurses.
Study design
Phase One of this study was a simulation use test; each nurse inserted four types of catheters in vitro in a training model with first-stick success evaluated. Phase Two was a survey of nurses to identify items used when inserting PIVCs and with purchasing agents to identify the costs of these insertion-related items. Smartworks, a global market research and marketing company, and the Terumo Medical Corporation conducted internal ethics reviews of the study design. The study adhered to the Code of Professional Ethics and Practices set by the American Association for Public Opinion Research. The project was determined not to require Institutional Review Board (IRB) approval for unregulated research as defined by the Department of Health and Human Services (DHHS) regulations at 45 CFR 46. Research activities involving human subjects for behavior observation are exempt and meet the Federal Policy for the Protection of Human Subjects.
Phase one: A simulation study
A simulation use test was conducted with registered nurses and nurse practitioners from acute care hospitals in New York City in February 2024. The sample of respondents consisted of nurses who insert PIVCs with two or more years of experience. Subjects were selected from the following hospital areas: medical/surgical, intensive care unit, emergency, oncology, gastroenterology, palliative, preoperative, cardiology, endoscopy and post-anesthesia care. The study sponsor was not identified. Nurses reviewed blinded IFUs of four unidentified brands of catheters used in the simulation use test.
The PIVCs tested were selected as representative of predominant sizes and types of safety catheters and flashback mechanisms currently available in the United States today. 29 Each catheter was characterized by distinct timing of flashback occurrence. The Surflo ZERO, available only in Japan, was added as a comparative example of a PIVC that integrates a thin-tipped short bevel needle known to require less insertion force. 30 All catheters used in the study were polyurethane 22-gauge (G), 1-inch (in)/2.54 centimeters (cm) long. The needles were either lancet or backcut, and indicated for vascular access (Figure 1).
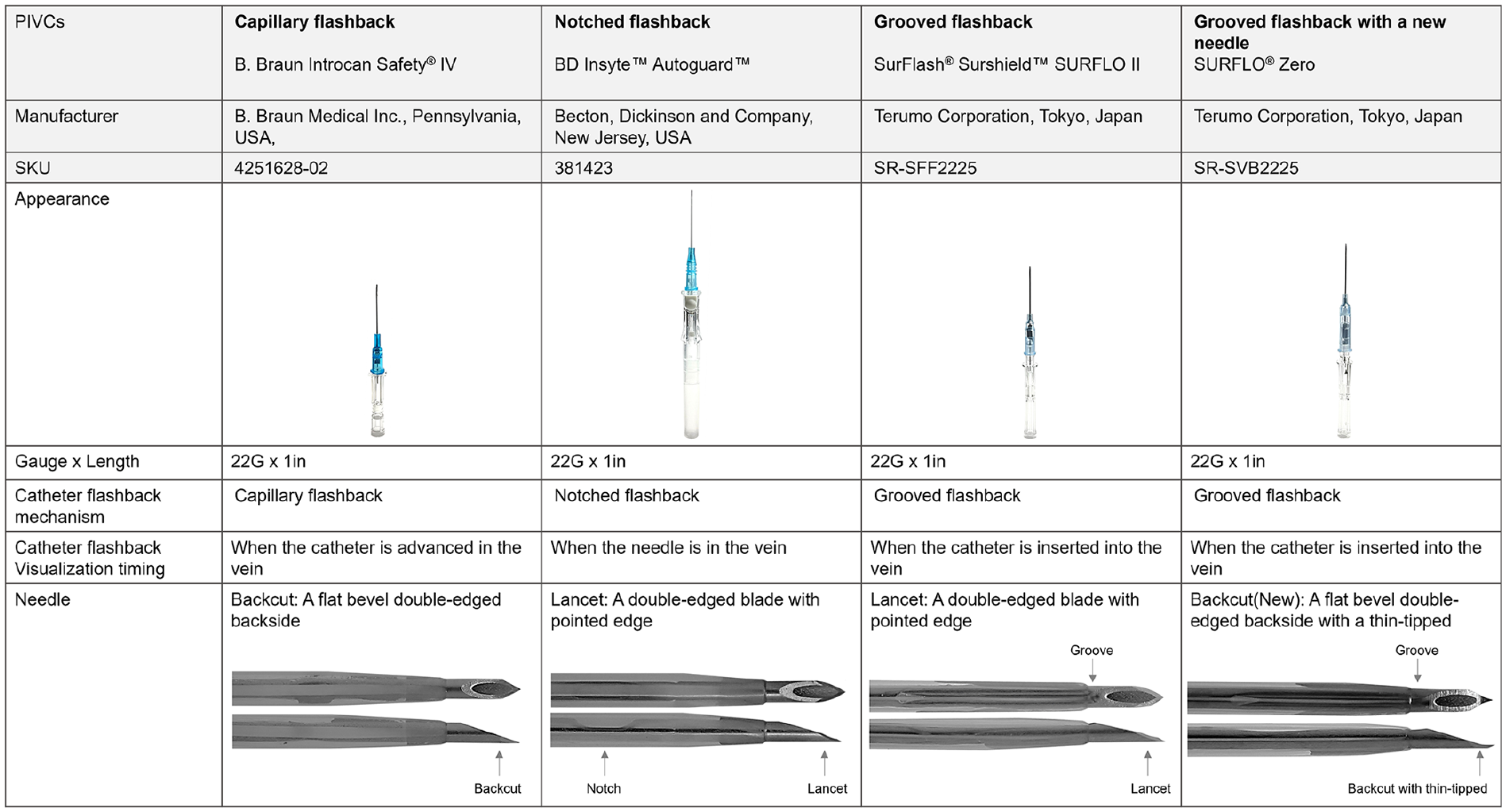
Comparing four types of PIVCs.
Nurses were asked to place each of the four PIVCs into an in vitro model, first in a tube for trial to familiarize themselves with each catheter, and then into a dedicated vessel training model (shown in Figure 2).
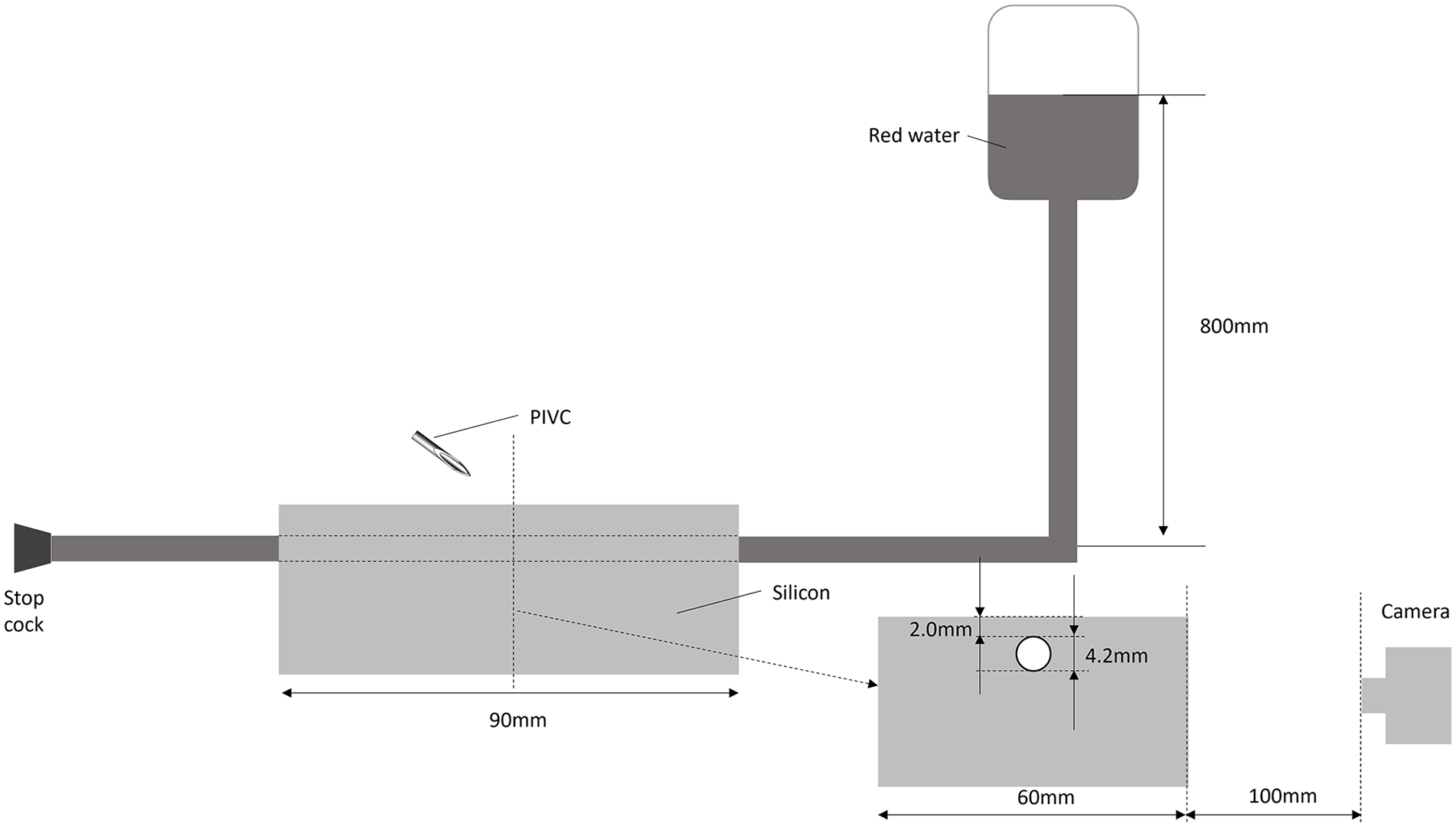
Experimental setup for observation of the insertion process.
The inner diameter of the tube in the dedicated training model was 4.2 mm, simulating the diameter and depth of the cephalic vein in adults; the outer diameter was 4.8 mm (thickness 0.3mm), and the depth of the vessel was 2.0 mm from the surface. 31 The tube was covered with a transparent silicone gel, and the top surface, where the PIVC was inserted, was covered with a polyurethane gel that prevented participants from seeing the tube. The tube was filled with red water at a pressure of 80 mmHg to simulate blood pressure when a tourniquet was applied. 32
Insertions were video-recorded from the side located 100mm from the silicon base and later analyzed. Nurses inserted each of the four catheters, which was considered one cycle, into the experimental setup (Figure 2). Following the nurses' insertion of each of the four catheters (a “cycle”), responses were collected regarding if successful placement had occurred for each catheter in the cycle. Qualitative feedback was collected on the nurses’ responses.
Nurses continued placing the four catheter types for two more cycles for a total of 12 insertions. Nurses performed three insertions of each catheter type. At the end of each cycle, feedback was collected on responses to the successful placement of each of the four catheters.
Data analysis
Video recordings of each insertion for each cycle of the simulation use test were analyzed for first-stick PIVC insertion success. Insertion was defined as the process of needle insertion into the tube/vein. A double puncture was noted when the needle was inserted into the tube and penetrated the posterior wall of the tube during insertion. Catheter placement failure applied when the catheter’s final length and position were not within the tube. Catheter placement success was achieved when nurses inserted the needle into the training vessel model, and the full catheter length was placed into the tube/vein without penetration of the posterior wall. After each cycle, nurses were asked if each catheter in that cycle was successfully placed. Nurses were not provided with a definition of first-stick success or successful placement. Responses were analyzed and compared to their actual performance, as captured in the video recording.
Phase two: Online study of nurses and purchasing agents
The primary goal of Phase Two was to measure the cost of first-attempt failure. An online study measured nurses’ first, second and third-stick PIVC success rates and identified supply materials used when inserting PIVCs. To qualify, nurses were required to have at least 2 years of nursing experience that included the job functions of PIVC insertions. The supply evaluation included items in IV kits, whether unused kit items were discarded, items used but not included in the kit, the number of items used, and the time nurses report taking to insert each PIVC. Nurses were asked to define first-stick success and then asked to choose one from a number of definitions.
This Phase Two study was conducted in May 2024 with registered nurses and purchasing agents (or materials managers) in acute care hospitals throughout the United States. Purchasing agents were surveyed to identify the cost of each item nurses reported using when inserting IV catheters. The purchasing agents were also required to know the facility current price for supplies used by nurses for catheter insertion. The study facilitators were blinded to the participants for data collection in Phases One and Two.
Data analysis
Survey responses were processed and managed using two software programs, SPSS Statistics (IBM Corporation, Armonk, NY., Version 27) and WinCross Executive (Analytical Group, Inc., Scottsdale, AZ.).
Study results
Phase one: Simulation study
In a simulation use test of 16 registered nurses (RNs) from acute care hospitals in the USA, each nurse inserted four types of PIVCs into a training model three times (12 insertions each) for a total of 192 procedures. Nurses using a grooved needle flashback had fewer double punctures than those using a capillary or notched needle flashback, resulting in higher catheter placement success for the grooved needle (Figure 3(a) and (b)). The thin-tipped short bevel needle had no catheter placement failures and had the highest catheter placement success of any flashback mechanism.
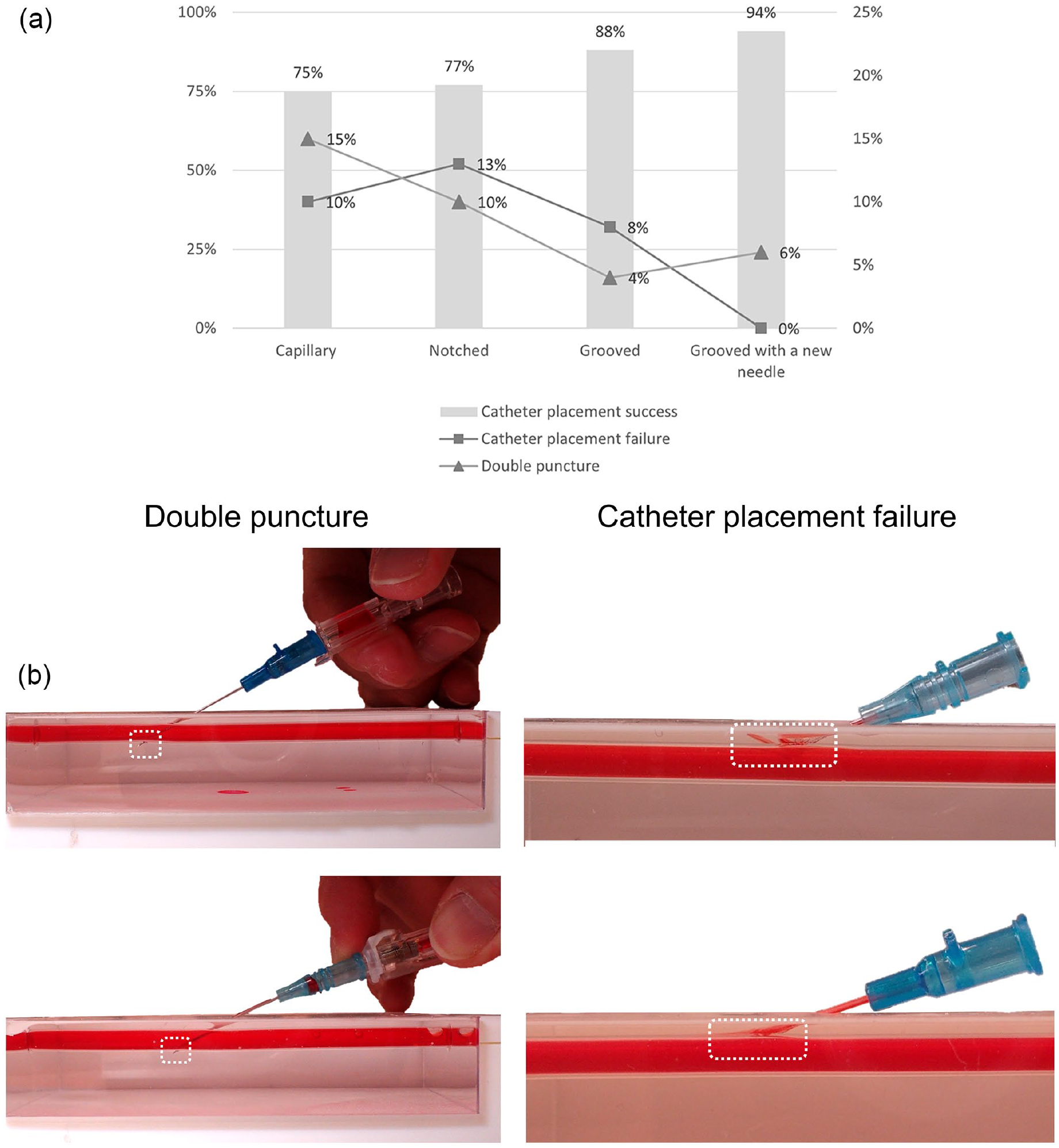
(a) A simulation use test results comparing four catheters and (b)Representative example of double puncture and catheter placement failure from simulation test. Background images of tables, camera, laptop, etc. (backgrounds) were removed to focus on catheter insertions.
Figure 3(a) and (b) show double punctures were highest among nurses using a capillary flashback catheter, and catheter placement failure was highest using the notched needle flashback catheter. Nurses using the grooved needle flashback with a thin-tipped bevel needle were 20% more successful with catheter placement than when using a notched needle flashback, and 22% more successful compared to a capillary flashback. Catheter placement success with a grooved needle flashback was 15% higher than with a capillary flashback and 13% higher than when using a notched needle flashback.
A high percentage of nurses reported successful placement of the PIVCs when the analysis demonstrated failure. The misconception rate was 82% for double puncture of the vein and 60% misconception rate for successful catheter placement (Table 1).
Perception and reality.


Shading in the tables indicates nurses’ perceptions that did not match reality. Unknown means no answer.
Phase Two: Online study of nurses and purchasing agents
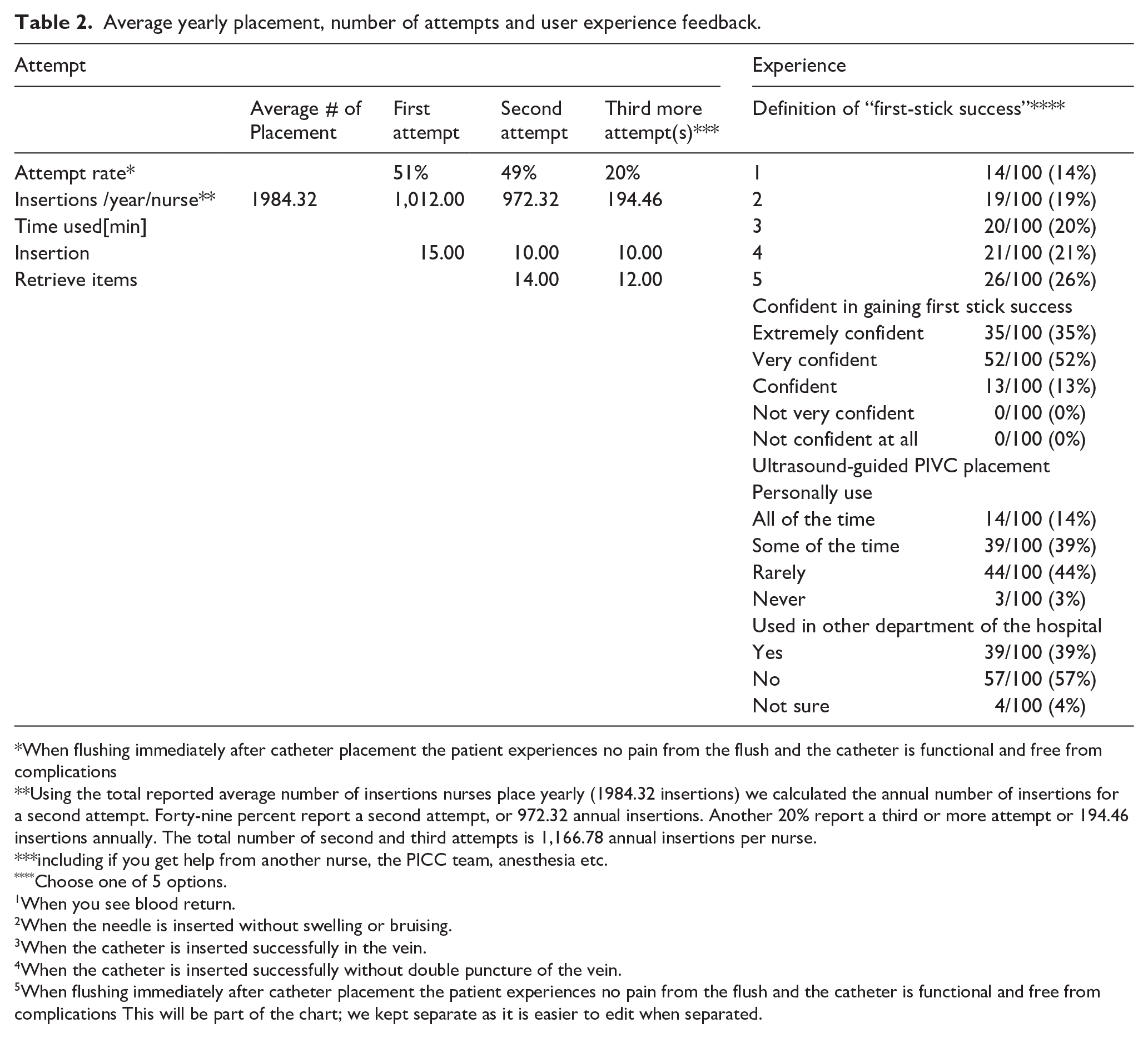
The authors calculated four categories of cost: PIVCs, IV start kits, items not in the IV kit and RN labor. On average, the nurses place 165.36 PIVC catheters a month, or 1984.32 PIVCs annually. The average annual number of second and third insertion attempts combined is 1,166.78. One hundred percent of nurses reported confidence in first insertion success at each facility using the current model of PIVC, notched or capillary; more than a third were extremely confident, and more than half reported very confident (Table 2).
Average yearly placement, number of attempts and user experience feedback.
When flushing immediately after catheter placement the patient experiences no pain from the flush and the catheter is functional and free from complications
Using the total reported average number of insertions nurses place yearly (1984.32 insertions) we calculated the annual number of insertions for a second attempt. Forty-nine percent report a second attempt, or 972.32 annual insertions. Another 20% report a third or more attempt or 194.46 insertions annually. The total number of second and third attempts is 1,166.78 annual insertions per nurse.
including if you get help from another nurse, the PICC team, anesthesia etc.
Choose one of 5 options.
When you see blood return.
When the needle is inserted without swelling or bruising.
When the catheter is inserted successfully in the vein.
When the catheter is inserted successfully without double puncture of the vein.
When flushing immediately after catheter placement the patient experiences no pain from the flush and the catheter is functional and free from complications This will be part of the chart; we kept separate as it is easier to edit when separated.
All nurses reported using a PIVC and an IV start kit on the first PIVC placement attempt; 72% reported using another PIVC on the second attempt, and 90% reported using an additional kit. The increased annual cost calculated for the 2nd and 3rd attempts per nurse per year was $US 35,919.15 (Table 3).
Materials used during 2nd/3rd attempt and the average cost.

Material costs:
The cost of PIVCs and kits for a second attempt was calculated by multiplying the number of insertions placed annually per nurse by the percentage of nurses who said they used a PIVC or kit on a second attempt. That number was multiplied by the average cost of the PIVC or kit as reported by purchasing agents. To calculate the percentage of each item not in a kit, the percentage of nurses who said they use each on a typical insertion and the percentage reporting that item not in their kit was calculated. Each item not in the kit was factored in based on the percentage who used that item. Each item was recalculated for the percentage of each item used by nurses on a second attempt but included in a kit.
The number of insertions were calculated using this percentage for each item not in a kit, multiplied by the average cost of that item to determine the cost per nurse for using items not in the kit. The cost of needleless caps/connectors, clean non-sterile gloves, and sterile catheter dressings are all reported to be in a kit in higher percentages than nurses used. Therefore, the cost of these items was not included separately, but included in the cost of the kit. The authors applied the same percentages used from the second attempt for each item to calculate costs for the third attempt.
Labor costs related to PIVC insertions are based on the national average hourly salary rate for RNs, $46.16. 33 The number of insertions and the average time used for both insertion and retrieval of items for insertions for second and third attempts was used for the final calculation.
Discussion
This is the first study to measure and compare catheter device flashback technologies (each with different flashback visualization timing), the effect on a vessel during simulated insertion and the cost of first-stick failure. It is also the first to evaluate nurses’ perception of PIVC placement success against actual performance and measure nurses’ definition of first-stick success. The study compared different flashback technologies and identified improved incidence of first-stick success and reduced operative error during insertion with the grooved needle flashback catheters. This in vitro study did not measure improvement in patient outcomes; however, first-stick success would impact the speed of the treatment delivery, mitigate trauma to patients and reduce hospital insertion costs.
The research question “Does the needle bevel and catheter design affect the successful insertion of peripheral intravenous catheters?” was effectively studied, with results indicating that the needle bevel and flashback mechanism do play a role in successful insertions. The grooved needle flashback resulted in higher catheter placement success by the nurses compared to either the capillary flashback or the notched needle flashback. The shape of the grooved needle tip also contributed to the success of the catheter placement by the nurses. As shown in Figure 3(a), insertions with capillary and notched needle flashback catheters had more double punctures and catheter placement failures than PIVCs with the grooved needle flashback. The inserters failed to reach the first-stick success goals reported in prior research with notched catheters, and non-notch catheter success was even lower. 19 Despite the nurses in our study having many years of experience inserting PIVCs with notched needle and capillary flashback technologies and no experience using grooved needle flashback, using grooved needle technology resulted in fewer double punctures and catheter failures. Grooved technology enabled nurses to overcome operative failure and issues related to quality education and achieve improved first-stick success.
The PIVC instructions for Use (IFUs) may play a role in these findings. IFUs for the notched needle and the catheter capillary flashback PIVCs instruct users to decrease the insertion angle and advance the catheter/needle assembly slightly to ensure the catheter is in the vessel. “Slightly” is a relative term. In our simulation, some participants may have pushed the needle and catheter forward more than necessary after vein entry, resulting in a posterior double-wall puncture. As shown in Figure 3(b), some other participants inserted the needle into the shallow upper layer of the vessel and failed to enter the vein. The catheter was not inside the vessel and was pushed out when the catheter was threaded due to the penetration force and/or hand movement during catheter advancement. This root cause was demonstrated in an earlier study. 25
The IFU for a grooved needle flashback instructs users to advance the catheter into the vein only after observing blood flashback in both the flashback chamber and the catheter itself. This double confirmation ensures full entry into the vein. Users are not instructed to “slightly advance the assembly after confirming flashback” because the grooved flash mechanism tells participants exactly when to stop needle advancement and when to advance only the catheter, which is expected to reduce double puncture.
In the Phase One simulation, researchers observed zero catheter placement failure when nurses used the PIVC with a thin-tipped short bevel needle. Earlier research indicates the thin-tipped short bevel needle showed significantly lower catheter insertion resistance than conventional lancet needles, allowing smooth insertion into the vessel. 34 The shorter thin bevel is thought to be a contributing factor in reducing catheter placement failure occurring when the catheter fails to fully penetrate the vein wall or results in an inadequate amount of the catheter within the vein and is later pushed out of the blood vessel due to vascular resistance.
Although it is impossible to visualize inside the vessel to detect failures during patient insertions, improving insertion failure rates through education on PIVC use is possible. IFU ambiguity and the complexity of the process may be barriers to learning the optimal technique. The needle flashback mechanism such as the grooved flashback may overcome issues contributing to failure and help to establish quality education that promotes greater success. This suggests that clarifying the IFU and using grooved flashback technology can help inserters overcome barriers to learning and improve catheter placement success.34 -36
An analysis of cost associated with second and third-stick attempts was performed to demonstrate the potential impact of the insertion improvement. Nurses were asked to indicate specific items used and purchasing agents were asked about the cost of each item. This secondary outcome of supply costs for each insertion attempt revealed the high cost of first-attempt failures per nurse based on the number of insertions placed annually, and additional materials used when a first attempt fails. Based on these data, the calculated total cost of first-stick failure was $US 35,919.15 per nurse per year. This study demonstrated first-stick catheter placement success with the grooved needle flashback was 15% higher than with a capillary flashback and 13% higher than when using a notched needle flashback. Applying this 15% improvement with grooved technology represents a significant potential savings of $US 5,387.87 per nurse annually.
Based on the economic analysis in this study using grooved technology, a 300-bed hospital with 180 nurses (3 shifts) could save an estimated $US 969,817.28 annually. These calculations do not include such additional costs as ultrasound-guided insertions (ultrasound device, gel, training, etc.), or multiples of items used by nurses during one insertion, nor do the calculations include post insertion complications (occurring in 36% of PIVC insertions). 35 Complications including phlebitis, occlusion, infiltration/extravasation, catheter-related bloodstream infections, prolonged hospitalizations (two additional days at a cost of more than $US 3,000 per patient) 36 all contribute to patient discomfort, dissatisfaction and delayed treatment.
It is interesting to note that in this simulation study, nurses experienced an 82% “misconception rate” for double punctures and 60% for catheter placement success (Table 1), leading to erroneous conclusions by the nurses reporting successful insertions despite actual failure. While there is limited evidence comparing nurse confidence versus actual performance success, it is vital for nurses to recognize insertion errors prior to initiation of infusions because failure can lead to serious problems such as infiltration, extravasation, and pain if failure is overlooked. Nurses’ misplaced confidence level in attaining first-stick success, misconception rates, unclear definition of first-stick success, and lack of access to education about newer technologies may all contribute to first-stick failures.
The successful insertion of PIVCs is facilitated by multiple factors. The design of the needle and catheter impacts insertion success, as demonstrated in this study. Grooved flashback technology reduces operative error, improves first-stick success, reduces healthcare costs, and contributes to improved patient satisfaction and outcomes. Familiarity with the recommended insertion procedure as indicated in the device IFUs, the ability to confirm entry into a vessel with flashback and the appropriate timing needed for advancement of the catheter all play a role in first-stick success. Within acute care hospitals, each failed attempt results in a cost to the patient in terms of pain, vein depletion, and rarely recognized mounting costs for each hospital. Close consideration of the type of device used for PIVC insertions could result in significant achievable savings.
Limitations
This multi-modal study has some limitations, and the results should be interpreted cautiously. The first phase in vitro investigation was necessary to facilitate real-time video of simulated vein entry that informed the performance success or failure of the nurses. The findings of the study could be strengthened with larger participant sample sizes. Phase One of the study was a convenience sample representing possible selection bias. Observational studies may have associated risk from the Hawthorne effect when individuals improve or modify behavior based on observation. While this investigation was a manufacturer-sponsored independently conducted multi-phasic study, it was the first study to compare performance of different PIVC needles and newer flashback designs, identifying benefits associated with device insertion success. Future larger-scale research studies are needed to strengthen and confirm these findings.
Conclusion
In clinical practice, the PIVC placement procedure has been attributed to the operator's experience and sensory perception. Different needle designs and catheter flashback mechanisms affect PIVC blood flashback during insertion and contribute to first-attempt success or misperception of success. In this study, nurses were able to successfully confirm vein entry with a double blood flashback in both the flashback chamber and the grooved flashback needle design. Overall, the nurses achieved 94% first-stick success with the grooved flashback technology integrating a thin-tipped backcut flat bevel needle and zero percent failure. This study found the insertion technique with the grooved blood flashback needle design significantly improved first-attempt success and had a high potential to positively affect hospital economics.
Supplemental Material
sj-pdf-1-jva-10.1177_11297298241313414 – Supplemental material for Comparative study of peripheral intravenous catheter insertions with capillary, notched, and a grooved needle flashback design
Supplemental material, sj-pdf-1-jva-10.1177_11297298241313414 for Comparative study of peripheral intravenous catheter insertions with capillary, notched, and a grooved needle flashback design by Nancy Moureau and Lois Kaufman in The Journal of Vascular Access
Footnotes
Acknowledgements
Special thanks to Catherine Adams for editorial assistance.
Author contributions
All authors contributed to the study design, data analysis, manuscript drafting, revision and approval of the final version for publication. Terumo Medical Corporation had no role in interpreting the findings or in the preparation of the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: NM is the owner and CEO of PICC Excellence, Inc. providing research consultation for the Terumo Medical Corporation. LK, PhD, President of smartworks discloses funding support from Terumo Medical Corporation.
Nancy Moureau, RN, PhD, CRNI®, CPUI, VA-BC, and Lois Kaufman, PhD
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research and manuscript support was funded by Terumo Medical Corporation.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.