
Abstract
Background:
Vascular access via a single arterial catheter for targeted chemotherapy delivery has difficulties with concentration, dilution, drug retention, plasma binding, and lack of control of the tumour microcirculation. An implantable arterial access system to accommodate multi-catheter access was developed address these problems. The system was also adapted for isolated arterial-to-arterial extracorporeal suprasystolic perfusion for end stage peripheral vascular disease. The arterial-to-arterial logistics were compared with standard venovenous and arteriovenous fistulae access employed in haemodialysis.
Methods:
Targeted chemotherapy delivery was addressed in a pilot study of vascular liver isolation. Ten patients with secondary colorectal cancer, were treated with multiple infusions employing up to five individually steered catheters. The arterial-to-arterial extracorporeal access system was also used to treat end stage peripheral vascular disease in 20 patients where amputation was the only option. The trial was named Hypertensive Extracorporeal Limb Perfusion (HELP).
Results:
Multiple day only infusions produced a partial response or stable disease in six out of the ten patients in an ‘end stage’ setting. The mean survival was 11.2 months. Of the twenty patients facing amputation 40% had avoided amputation at follow-up 22 months and 20% had delay of 4 months.
Conclusion:
The access system allows repeatable steerable multi-catheter arterial access for chemotherapy delivery to address difficulties of concentration, dilution, plasma binding and microvascular control. The access system supports multiple repeatable suprasystolic extracorporeal arterial to arterial access. It is cardiac independent generating flows of greater than 1 L/min with zero flow in between treatments. The device logistics compares favourably with arteriovenous and venovenous access systems.
Keywords
Introduction
The concept of ‘living with cancer’ is a reflection of difficulties in providing curative treatment. Chemotherapy induced side effects demand drug concentration reduction and treatment time expansion to allow normal systems to adjust and recover. Intravenously infused chemotherapy may actually reach the tumour in less than 1% of volume whilst the remainder accumulates in normal tissues.1,2 Locoregional organ targeting is the logical treatment progression with measures to protect normal cells within the target organ itself. For example, in the liver 85%, of blood supply of the tumours is the hepatic arterial tree. 3 The normal arterial supplies 300 mL/min with a portal system 1200 mL/min. Single catheter hepatic artery infusions 4 achieve targeting, but immediate concentration dilution and systemic recirculation determine that almost all chemotherapy is directed to normal hepatic cells via the portal system. Control of the portal system would require a reusable multicatheter arterial access system to obstruct the coeliac axis, the superior mesenteric artery and the inferior mesenteric artery. The initial pilot study was to test the safety and efficiency of an implantable, occludable chemotherapy deliverable system capable of repeatedly accepting at least four fluoroscopically independently steerable catheters specifically to completely control and isolate the blood flow to the liver. Hence to create a model of remote repeatable vascular isolation to any organ.
In contrast to decreasing the blood flow to an organ a universal access system would be capable of providing increased blood flow at suprasystolic blood pressures. Hence there was a requirement of compatibility with extracorporeal pumping systems. The concept was best assessed in the field of peripheral vascular disease. End stage peripheral vascular disease is defined as persisting ischaemic symptoms and signs despite exhaustion of all possible measures. Amputation is the only option. Herewith limb salvage would require substantial increase in collateral flow in the immediate term to relieve symptoms and the stimulation of vascular neogenesis in the intermediate term. The three essential components are extracorporeal extraction from the normal arterial tree above the circulation obstruction, limb isolation to avoid haemodynamic mixing and creation of suprasystolic return flows. Following successful animal experiments, a prospective human study was undertaken; hypertensive extracorporeal limb perfusion (HELP).5,6 The aim of the study was to test the safety and efficacy of an implantable arterial access system in remotely controlling extracorporeal arterial to arterial suprasystolic blood flow.
Arterial-to-arterial extracorporeal loop access may also prove beneficial in the context of haemodialysis for end stage renal disease. The vascular access components of arterio arterial access were compared with arteriovenous fistulae and venovenous access.
Design requirements for an implantable reusable multi catheter organisation device with arterial-to-arterial extracorporeal access
In order to control entire limb blood flow, the diameter components should be capable of flows greater than 1 L/min to overcome high peripheral resistance. Pressures up to 300 mmHg are necessary to continue for at least 24 h. To avoid cardiac work, extracorporeal blood extraction and pump return must be adjacent but separated sites on the arterial tree. Separation avoids the mixing of treated and untreated blood. There is zero resting blood flow between treatments. The concept of arterial-to-arterial loop compares with the arteriovenous loop concept requiring significant cardiac support.
For organ isolation for chemotherapy delivery, the requirement is a minimum acceptance of five removable individually steerable endoarterial catheters using balloons to control the inflow circulation both at an axial and collateral level. Pressure transduction capability is an essential component to verify vascular isolation. Optimally the device is available for immediate use as well as compatible with many anatomical implant sites.
Design inclusions to minimise complications
Transcutaneous devices have a propensity for infection. The infective process is often haematogenous in origin with deposition of organisms on the endoluminal surface of foreign material. Optimally there should be no long-term foreign body contact with the blood. The device should have a long subcutaneous tunnel protected by multiple infection rings to mitigate transcutaneous bacterial migration. In addition, the endoluminal occluder should be friction fit to remove any biofilm development during usage. Endoluminal biofilm development is also minimised by citrate installation of the dead space between the occluder and the shaft. After implantation negative pressure dressings may be used to create a seal between the silicone and the cutaneous tissues. Thrombosis prophylaxis consists of oral anticoagulation and the absence of a permanent endothelial foreign material profile.
Device description
The access system (AllVascular Pty Ltd, St Leonards, Australia) is shown in Figure 1. The surface of the chamfered occluder is flush with the anastomosis and is the only endoluminal component. It is changed every few days for access and treatment. The 2–3 mm anastomotic PTFE is distal to the occluder but is designed to have minimal surface area and to induce complete coverage with pseudo intima in the short term. These designs are in consideration of infective complications. In the non-treatment phase the device is completely occluded. During treatment the blood is returned to an adjacent arterial anatomical site so that the energy of flow is pump derived, that is, the heart is not included in the circulatory loop. To avoid mixing of inflow and outflow content the inflow catheter can be variably inserted proximally closer to the heart (Figure 1(b)). The device is available for immediate use and there is only a small segment of artery required for implantation allowing multiple placement options. The haemoreduction valve attachments (Figure 2) can accommodate up to five individually steered catheters with or without balloons. These are capable of carrying radioactive materials, cells or any chemotherapy to the target. The access system is a CE mark approved.
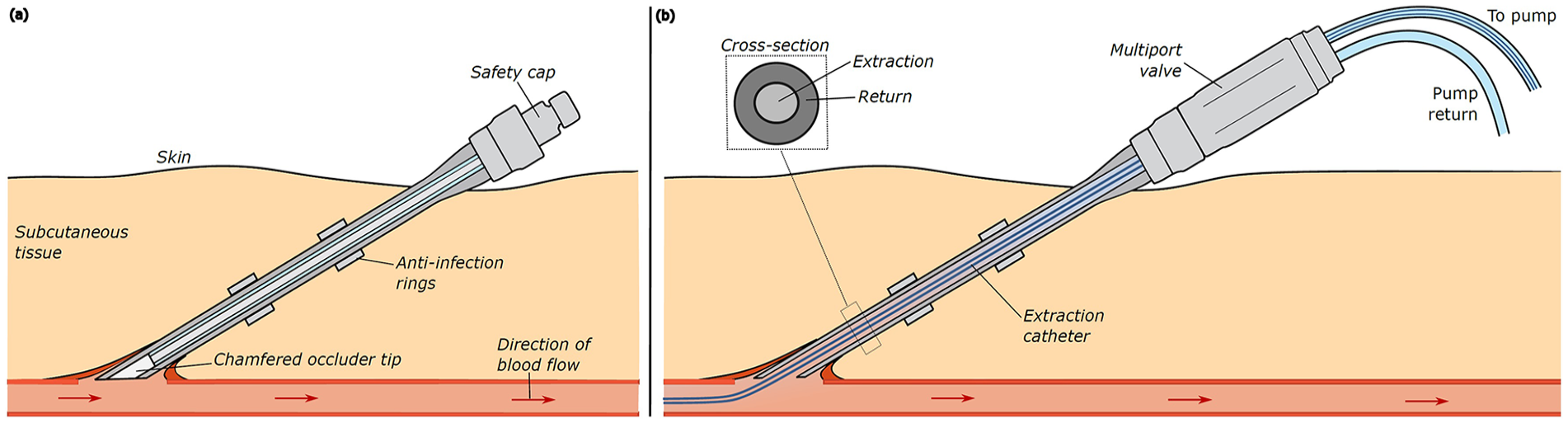
(a) The access system implanted with no flow and (b) connected to an extracorporeal pump.
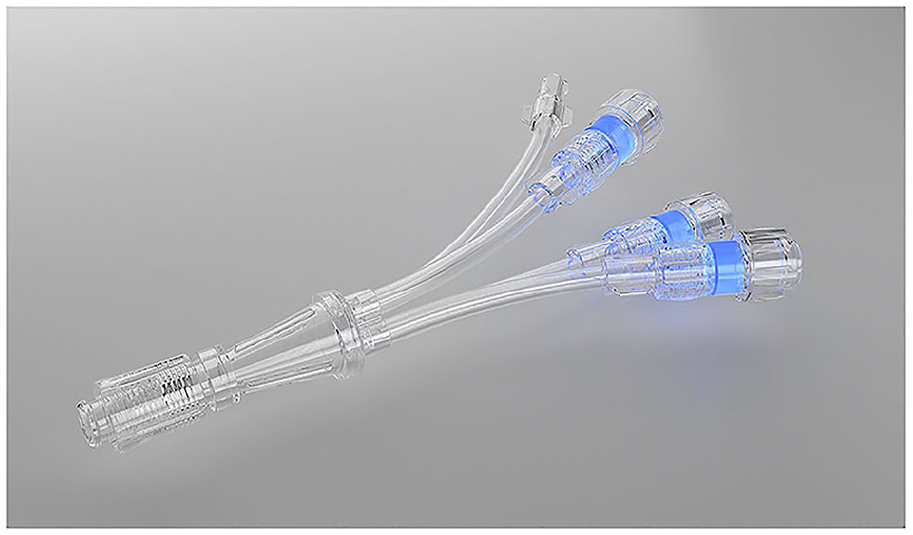
Demonstrates the multiport haemoreduction valves which can accommodate simultaneous multicatheter access.
Implantation method
Under general or local anaesthetic, a 7 cm incision is extended subcutaneously to expose the donor artery. After vessel control an arteriotomy 1.5 cm long is anastomosed to the access system. In smaller vessels a vein patch using autogenous materials, such as the saphenous vein, is essential. Foreign material should be avoided as both the patient groups, end stage peripheral vascular disease and advanced cancer are repeatedly plagued by bacteraemia. The anastomosis and the occluder function is tested for haemorrhage by release procedures. The lower limb arteries were used for regional hyperperfusion related to the site of ischaemia. As the system was immediately connected to an extracorporeal pump with pressures up to 300mmHg with anticoagulation, wound drainage was an important addition for regional chemotherapy. The upper limb vessels were implanted related to the ease of access to the abdominal arteries. As chemotherapy was often commenced at operation, anticoagulation was required and hence the need for wound drainage. Wound drains are removed within 24 h post-implantation while indwelling catheters are only used intraoperatively and removed after each regional chemotherapy procedure.
Explantation method
There is re-opening of the wound followed by vascular control via direct suture. The access system is divided and removed from the exit foramen, arterial closure is directly or with an autogenous patch from the saphenous vein. The wound is closed with drainage. There is no foreign material left in situ.
Method
Chemotherapy delivery trials
This was a registered, single-arm non-randomised pilot study (ACTRN12611001273976) approved by the institution’s Human Ethics Committee and conducted in accordance with the Declaration of Helsinki.7,8 Ten patients who met the specialised inclusion criteria were enrolled with histologically proven colorectal end stage adenocarcinoma with inoperable hepatic metastases. Essential clinical requirements were fitness for multiple anaesthetics, adequate hepatic reserve and approval by the multidisciplinary committee. Infusions of oxaliplatin were performed bi-weekly for 4 weeks using balloon catheters with segmental and total liver isolation for 25 min.
The HELP trial
This study evaluated 20 patients with critical limb ischaemia who were treated with HELP. 6 These patients had no other option but major amputation, as determined by at least two vascular surgeons. The arterial circulation to the ischaemic limb was isolated from the systemic circulation by the use of an endoluminal balloon catheter in seven patients and by an implantable, inflatable, occlusive cuff in 13. The limbs were hyperperfused through the peripheral access system with an extracorporeal pump, producing a minimally pulsatile waveform at 200% to 300% of the mean arterial pressure. This was performed repeatedly in sessions of 24 to 36 h, up to a maximum of 74 h. The primary end point was avoidance of major amputation
Results
Chemotherapy delivery trials
Pressure verified, multiple day-only hepatic vascular isolation infusions were achieved in nine of ten patients, with a single patient receiving multiple hepatic arterial infusions.7,8 Positron emission tomography-computed tomography (PET-CT) imaging confirmed partial response in three of ten patients and stable disease in three of ten patients. Systemic toxicity was minimal.
The HELP trial
Given adequate arterial access, 39 of 40 connections developed flows four to eight times those supplied to the limb by the normal cardiac output. 6 A progressive decrease was noted in peripheral resistance. All patients developed a pain-free, warm foot or hand while on the pump in the short-term. In the longer term at a mean of 22 months (range, 12–54 months), eight of 20 patients (40%) had avoided major amputation and four more had a delay in amputation of an average of 4 months.
In both of these studies repeated multi-catheter arterial access was achieved. Volume flows for arterial-to-arterial extra corporeal axis created unrestricted flow without apparent cardiac instability. There is zero flow in between treatments. Infection was 4% over all catheters. There was one minor thromboembolic event without residua, without interruption of therapy. There was no known incidence of mixing of inflow and outflow, that is, isolation complete. There was no haemolysis encountered. There was no vascular stealing encountered.
Discussion
The concept of arterial-to-arterial extracorporeal access compared with arteriovenous fistulae and venovenous access.
Cardiac work
The HELP trial verified that large volumes of blood could be repeatedly recycled extracorporeally to similar but physically separated adjoining arterial sites by the access system. Induction of increasing collateral flow did not induce general cardiovascular instability as the return volume was intraarterial (Figure 3). The concept of minimising cardiac work is particularly important in ischaemic limb patients who have a background of diabetes, smoking and general cardiovascular disease. The arterial-to-arterial cardiac sparing effect contrasts with arteriovenous systems used in haemodialysis. Autogenous fistulae require an additional cardiac work of 919 ± 300 mL/min 9 whilst graft fistulae 1270 ± 604 mL/min interdialysis. 10 Added to this there is 300–500 mL/min donated to the pump during dialysis. Included is the cardiac derived ultrafiltrate removal which may be 2 L over the 5-h dialysis period (7 mL/min). The high incidence of cardiac morbidity and mortality is understandable with AV fistulae. 11 As well as substantial cardiac workload, needle puncture diameters limit filtration volume. (15 gauge has an ID of 1.2 m, 14 Gauge and ID of 1.6 mL). The access system’s cross sectional areas are shown in Figure 1(b). Given the wall thickness of the extraction catheter is 1French, the flow, counter flow cross sectional diameters are optimal with a 9 French central catheter with the access system diameter being 5.1 mm. Assuming the flows are proportional to the fourth power of the radius (Poiseuille’s Law), flows of upward of 1 L are available as demonstrated in the HELP trial. The combination of minimal cardiac work, and unrestricted blood flow, haemodialysis time reduction is a distinct possibility.
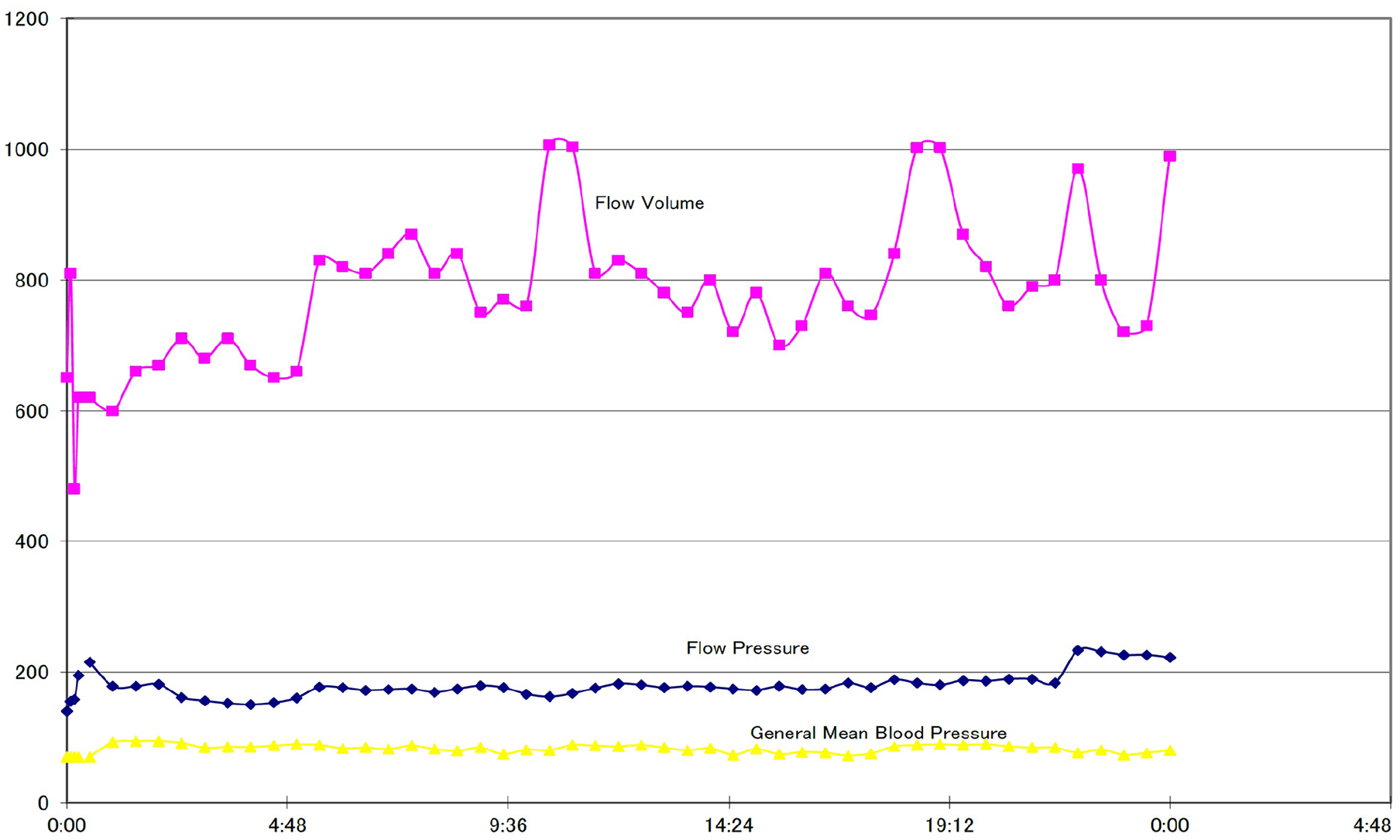
Shows the relationship between extracorporeal flow (mL/min), pump pressure (mmHg) and patient mean systemic pressure (mmHg). The graphs illustrate cardiovascular stability.
Haemodynamics
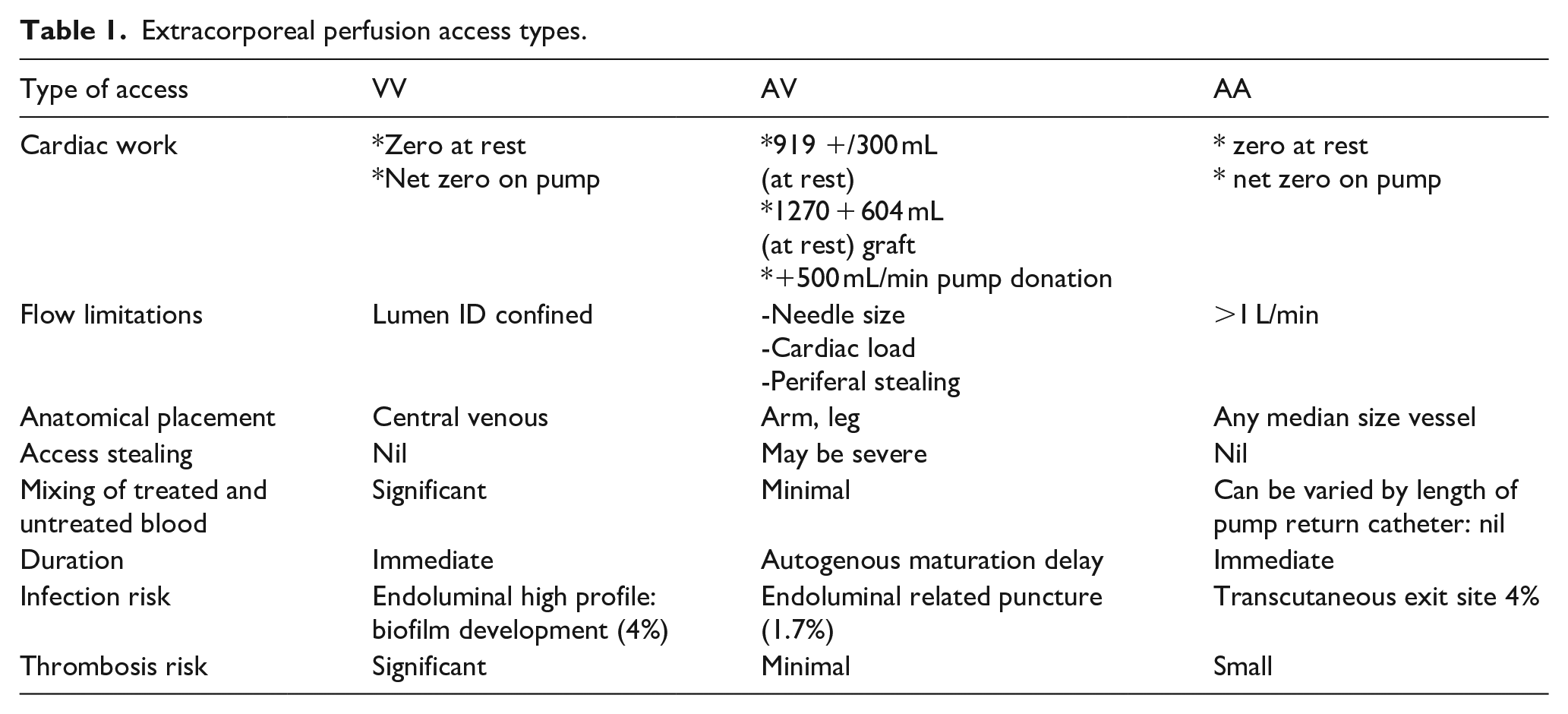
Arterial large bore access does not require needle punctures which are associated with high sheer forces which predispose to haemolysis. 10 There is no distal stealing which may be a consequence of arteriovenous fistulae. To avoid mixing of treated and untreated blood, the inflow and outflow orifices can be varied according to changing the length of the central endoluminal catheter (Figure 1(b)). In many ways the arterial-to-arterial access is similar to venovenous filtration in haemodialysis. 12 There is zero flow in between treatments, access is immediate, and it has a similar diameter to the access system. However, it does have some negative features, specifically a large endoluminal profile which predisposes the device to haematogenous derived infection, the mixing of filtered and unfiltered blood, flow limitations, and placement limitation to the central venous compartment. A summary of extracorporeal access types, that is, veno venous (VV), arteriovenous (AV) and arterial-to-arterial (AA) are compared in Table 1.
Extracorporeal perfusion access types.
Infection
Infection is a major consideration in the design and development of transcutaneous access devices. The Alan Brown arteriovenous transcutaneous shunt 13 was used for many years with quite high infection rates of 8.6% at 6 weeks somewhat related to the use of two transcutaneous tubes rather than one. An overall infection rate at 1 year was 20%. However, some 16% of these were related to secondary infections due to residual foreign body in situ following removal of the device for thrombosis. It is mandatory that all foreign bodies should be removed if a transcutaneous system is explanted. Similarly, Thomas shunts had a median shunt survival of 28 months with 24% failure rate. 14 The more modern large bore transcutaneous haemodialysis catheters such as the VectorFlow catheter (14.5 French) is used for venovenous filtration. This has a 90-day infection rate of 4%. 12 Graft fistulae have a much lower infection rate at 1.7% related to repeated needle puncture and combined with high endoluminal blood interface. 15 The majority of infections are blood derived from the development of a bacterial endoluminal biofilm. 16 For the transcutaneous devices, exit site and tunnel infection was 20% of the total. 17 Given these considerations the access system was designed to have a zero or minimal long term blood effacement with a long velore protected subcutaneous tunnel with extreme flexibility of the silicone tube within the tunnel. Other features were repeated instillation citrate and antibiotic in the dead space between the occluder and the inner tube interface. Mechanical removal of fibrin and biofilm by the friction fit occluder before activation of the device completes the prophylactic approach. Thrombosis was rare with the access system.
Chemotherapy delivery
The aim of any delivery system for chemotherapy is to create maximal targeted concentration without side effects. The elements determining efficiency are relative target size, drug retention, tumour vascular membrane permeability, drug neutralisation by plasma binding, lymphatic exposure and tumour microenvironment control. The relative concentration advantage over systemic delivery depends upon the mass ratio of the target to the total body mass, that is, liver 50:1, pancreas 2000:1, prostrate 2500:1. 18 The concept of retention – avoiding removal of chemotherapy from the target depends upon the rate of vascular washout into the venous system. This can be minimised by obstructing the axial and collateral inflows and/or increasing venous pressure. This mechanism of vascular isolation also avoids recirculation with the development of early side effects. Removal of red cells and plasma from the tumour allows remote control of the tumour microenvironment. Oncotic pressure control underscores the concept of Enhanced Permeability and Retention EPR 19 : hypoosmolality induces intravascular to extravascular fluid flux creating interstitial oedema. Lymphatics remove the drug containing fluid to the lymph nodes which are often the site of initial tumour metastases; indirect lymphatic targeting.18,19 Plasma washout also improves the pharmacological activity of protein bound drugs. Lipid soluble drugs may be bound 98% when systemically delivered. Delivered in a plasma free tumour environment they are only neutralised when entering the general circulation again minimising side effects. 19 Vascular isolation also allows other components of microenvironment control, temperature, PO2, PCO2, vaso-active drugs and adjunctive materials such as embolic or radioactive particles. Multiple catheter access also allows primary and secondary tumours to be treated simultaneously with or without the same drug. In the liver trial the access system illustrated the capability to induce a successful outcome.7,8 The multicatheter repeatable superselection components have been underscored by the improvements in two-point discrimination of radiation fluoroscopy, microcatheter development and the skills of the interventional radiologist (Figure 4).

Fluoroscopic intraoperative image of remote control of hepatic circulation. The five balloons are occluding the left and right hepatic entries, coeliac axis, superior mesenteric axis and inferior mesenteric axis.
Conclusion
These two pilot studies were developed to provide a basis for sample size clinical selection criteria to produce adequately powered statistical outcome. While clinical interpretations are limited due to ongoing clinical trials, the current experience to date is suggestive of the potential applications of the access system. It allowed repeated targeted chemotherapy delivery with locoregional drug retention, enhanced tumour vascular permeability, removal of plasma binding and remote microvascular control. Side effects were minimal. The access system design also allows repeated connection to an extracorporeal pump via arterial-to-arterial loop to deliver high volumes through vascular collaterals which avoided limb amputations. The haemodynamics of AA vascular access potentially compares favourably with both VV and AV systems.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Prof Rodney J Lane is a director of Allvascular Pty Ltd. Sarah Keogh and Nyan Khin are employees of AllVascular Pty Ltd.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NSW Health Medical Devices Funds