
Abstract
Sarcomatoid carcinoma is a rare type of gallbladder cancer with no specific clinical manifestation. The final diagnosis depends on pathological and immunohistochemical examination. Sarcomatoid carcinoma is characterized by early lymphatic metastasis, rapid progression, a high short-term recurrence rate, and a worse prognosis than adenocarcinoma. This report describes a 60-year-old woman with poorly differentiated adenocarcinoma of the gallbladder. She underwent treatment with chemotherapy and surgery. Palliative surgery was performed for treatment of tumor recurrence in April 2018. Postoperative pathology showed infiltration of poorly differentiated carcinomas, most of which were sarcomatoid. After four cycles of chemotherapy, the disease continued to progress. Anlotinib tablets were given from August 2018 to November 2018 but were then stopped because of gastrointestinal bleeding. The patient died in April 2019. This paper reports the whole process of diagnosis and treatment in this case of gallbladder sarcomatoid carcinoma, thus providing a reference for treatment.
Introduction
Sarcomatoid carcinoma is a malignant tumor that originates from omnipotent mesenchymal stem cells. Morphologically and immunohistochemically, sarcomatoid carcinoma shows epithelioid and mesenchymal components. Sarcomatoid tumors are rare and can occur in all parts of the body, but they mainly develop in the kidneys, lungs, prostate, and upper respiratory tract. Sarcomatoid carcinoma of the gallbladder is rarely observed. 1 Surgical treatment is the preferred approach for patients with early-stage sarcomatoid carcinoma, while radiotherapy, chemotherapy, and other treatments such as targeted therapy and immunotherapy may help to prolong the survival time in patients with advanced disease. Only a few reports of gallbladder sarcomatoid carcinoma have been published to date, and the clinical characteristics and treatment methods of gallbladder sarcomatoid carcinoma are still in the exploratory stage. In this report, the whole diagnostic and treatment process of a case of gallbladder sarcomatoid carcinoma is described to provide a reference for the diagnosis and treatment of gallbladder sarcomatoid carcinoma.
Case report
A 60-year-old woman with a 1-month history of mid-upper abdominal pain and abdominal distension was admitted to the Second Affiliated Hospital of the Medical College of Zhejiang University in May 2017. Physical examination revealed mid-upper abdominal tenderness. Abdominal enhanced computed tomography (CT) showed that the gallbladder wall was significantly thickened, and further examination was recommended to exclude the possibility of a malignant tumor (Figure 1).
Abdominal computed tomography scan on 29 May 2017 showed that the gallbladder wall was significantly thickened.
Laparoscopic exploration and omental biopsy were then performed. The volume of ascites in the abdominal cavity was about 1500 mL. Miliary gray-white nodules were found in the liver, omentum, abdominal wall, and pelvis. The nodules in the greater omentum were obtained for analysis, and the frozen sections were sent for pathological examination. The pathological findings revealed poorly differentiated adenocarcinoma. The diagnosis was established based on the presence of gallbladder cancer with abdominal metastasis combined with the patient’s medical history and auxiliary examination results. After the operation, the patient was treated with gemcitabine + oxaliplatin + tiggio capsules for two cycles and albumin-bound paclitaxel combined with oxaliplatin for four cycles with an unknown dosage, and the curative effect was judged as a partial response (PR). Radical cholecystectomy + intestinal adhesiolysis + laparoscopic exploration + omental excision were performed in November 2017. During the operation, gallbladder consolidation, invasion of the serosa, dense adhesion between the serosa and transverse colon, and hepatic surface adhesion were observed; no other obvious metastases were observed in the abdominal cavity. Postoperative pathologic examination revealed poorly differentiated adenocarcinoma with infiltration of cancer tissue at the incision margin.
In April 2018, whole-body positron emission tomography–CT showed postoperative changes of gallbladder cancer, low-density mass lesions with an abnormal increase in fluorodeoxyglucose metabolism in the operative area, and tumor recurrence involving the left lateral lobe of the liver and hepatic flexure of the colon. The slightly low-density shadow in the gallbladder fossa accompanied by increased fluorodeoxyglucose metabolism was considered to be possible tumor infiltration. The patient then underwent right hemicolectomy + special hepatectomy + complex intestinal adhesiolysis + jejunal nutritional fistula formation + duodenal bulb repair. Intraoperative examination revealed gallbladder cancer recurrence, invasion of the colonic flexure, and colonic obstruction. The postoperative pathology results showed infiltration of poorly differentiated cancer tissues, most of which were metastatic sarcomatoid carcinoma of the right colon (Figure 2). None of the nine intestinal wall lymph nodes were metastatic, and the hepatic margin, ileum, and colon margins appeared negative. Albumin-bound paclitaxel combined with oxaliplatin chemotherapy was given for four cycles from May 2018 with an unknown dose. CT examination after chemotherapy indicated tumor progression.

Representative hematoxylin and eosin staining of tumor tissue. (a) ×200. (b) ×400.
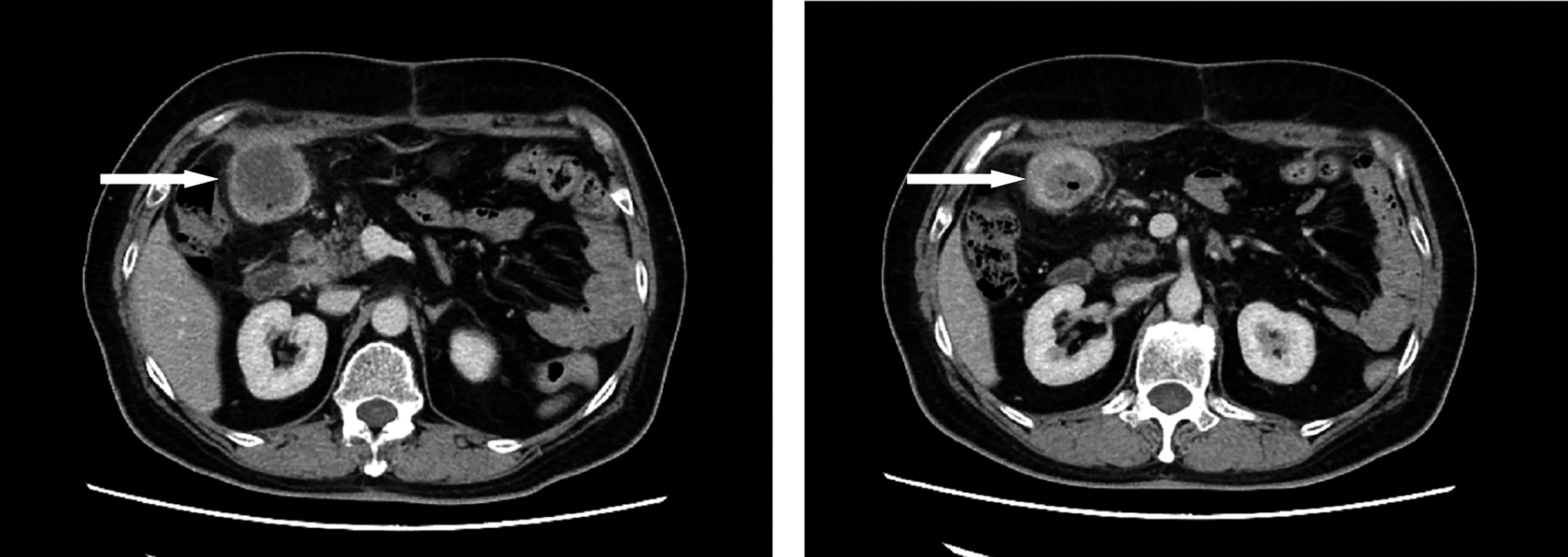
The patient then visited our hospital for treatment. Anlotinib tablets (12 mg orally every 24 hours, days 1–14, every 3 weeks) were given from August 2018. In September 2018, abdominal CT showed obvious lesion necrosis with cavity formation, and the curative effect was evaluated as PR. A comparison of the PR before and after treatment is shown in Figure 3. After two cycles, the anlotinib was reduced to 10 mg orally every 24 hours, days 1 to 14, every 3 weeks because of intolerable adverse effects including fatigue and hypertension. In November 2018, the patient stopped taking anlotinib because of gastrointestinal bleeding, and she died in April 2019.

(a) Abdominal computed tomography scan on 16 August 2018 showed abdominal metastases before treatment with anlotinib. (b) Abdominal computed tomography scan on 4 September 2018 showed necrosis of metastatic tumors in the abdomen accompanied by cavity formation after treatment with one cycle of anlotinib.
Discussion
Sarcomatoid carcinoma was first reported by Landsteiner in 1907. 2 It can occur in all parts of the body but mainly develops in the kidneys, lungs, prostate, and upper respiratory tract. 3 Sarcomatoid carcinoma of the gallbladder is rare. 1 The etiology of gallbladder sarcomatoid carcinoma is still unclear; studies have shown that it might be related to gallstones, 4 gallbladder polyps, and estrogen. 5 The age at onset of gallbladder sarcomatoid carcinoma reportedly ranges from 45 to 91 years, and it is more commonly seen in women. 6 The present case involved a 60-year-old woman, which is consistent with the literature. Sarcomatoid carcinoma is characterized by early lymphatic metastasis, rapid progression, a high short-term recurrence rate, and a worse prognosis than adenocarcinoma. 7
The clinical manifestations for this type of gallbladder cancer are nonspecific and mainly involve right upper abdominal pain and an abdominal mass. Some patients may have fever, jaundice, nausea, and vomiting. 8 Abdominal ultrasonography, CT, and magnetic resonance imaging are important imaging examinations in the diagnosis of gallbladder sarcomatoid carcinoma and can show the location, size, and characteristics of the tumor. However, because of the similar characteristics of gallbladder sarcomatoid carcinoma and adenocarcinoma, these cancers are difficult to distinguish by imaging examination. The final diagnosis depends on pathological and immunohistochemical examination. Histologically, sarcomatoid carcinoma of the gallbladder often exhibits two components: sarcomatoid carcinoma and epithelial carcinoma. 1 Sarcomatoid carcinoma is the main component of the tumor and is composed of shuttle cells or pleomorphic cells arranged in intricate or intertwined bundles. The cells have obvious atypia and many mitoses. Immunohistochemistry shows cytokeratin expression in the sarcomatoid carcinoma cells and epithelial membrane antigen and vimentin expression in some of the cells. Ki-67 is highly expressed. 7 In the present case, both the omental biopsy and the first postoperative pathologic examination showed poorly differentiated adenocarcinoma. The pathologists found that some of the poorly differentiated carcinoma had transformed into sarcomatoid carcinoma in the process of the pathological diagnosis after recurrence. The cells changed to a short fusiform morphology, the volume increased, the nucleus-to-cytoplasm ratio was high, and the heteromorphism increased. The reason for these changes may be that in the process of tumor recurrence, because of its heterogeneity, the cell phenotypes may be transformed. 9
Surgery is the preferred treatment option. 10 Radiotherapy, chemotherapy, and other treatments might also help to prolong the patient’s survival time. Because of the low incidence rate and lack of data analysis of sarcomatoid carcinoma, no standard radiotherapy or chemotherapy methods have yet been proposed. In the present case, the effect of chemotherapy for gallbladder sarcomatoid carcinoma was poor, and the effect of anlotinib was evaluated as PR. The findings of this case suggest that anlotinib has a certain therapeutic effect on gallbladder sarcomatoid carcinoma. The patient finally stopped taking anlotinib because of gastrointestinal bleeding; therefore, attention should be paid to the adverse effects of anlotinib.
Anlotinib is a new type of small molecule multi-targeted tyrosine kinase inhibitor developed independently in China. Unlike other tyrosine kinase inhibitors, it strongly inhibits many targets such as vascular endothelial growth factor receptor, platelet-derived growth factor receptor, fibroblast growth factor receptor, and c-Kit. 11 It has the effects of anti-angiogenesis and anti-tumor growth without inducing significant toxicity. 12 A series of clinical trials showed that anlotinib had survival benefits and good safety in the treatment of non-small cell lung cancer, medullary thyroid cancer, and soft tissue sarcoma after the failure of standardized therapy.13–15 In the present case, obvious tumor necrosis was observed after treatment with anlotinib. This provides an important reference for studying molecular-targeted therapies of gallbladder sarcomatoid carcinoma.
Conclusions
Sarcomatoid carcinoma of the gallbladder is rare and highly malignant. Extensive and careful pathological sampling and immunohistochemical examination are needed to establish the diagnosis. Surgery is the first-choice and main treatment method. Surgery combined with chemotherapy and target therapy may help to prolong the survival time. This report has described the whole process of diagnosis and treatment of a case of gallbladder sarcomatoid carcinoma, providing a reference for treatment.
Ethics
The study protocol was approved by the Ethics Committee of the Tongde Hospital of Zhejiang Province, Hangzhou, and the patient provided written informed consent.
Footnotes
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This study was supported by the Zhejiang Province Famous Traditional Chinese Medicine Experts Inheritance Studio Construction Project (GZS2017001), the Zhejiang Province Association of Traditional Chinese Medicine (2017ZB013, 2018ZA005), and the Science and Technology Department of Zhejiang Province (2018KY198).