
Abstract
Objective:
Few studies have been conducted on whether catheterisation via the lower limb pathway is suitable for intracavitary electrocardiogram (ECG) technology. This study explored the positioning of the epicutaneo–caval catheter (ECC) tip with intracavitary ECG via the lower limbs in newborns to determine its optimal placement and to improve the success rate of ECC placement using this method.
Methods:
Twenty-eight cases were selected for the observation group. The tip location with intracavitary ECG method was used to observe the changes in specific atrial depolarisation (P-wave) during the catheterisation process to determine whether the catheter tip was in the correct position. For comparative observation, chest X-rays and abdominal radiographs were taken within 24 h to determine sensitivity and specificity. The control group included 28 cases where the ECCs were inserted via the lower limbs, and chest X-rays and abdominal radiographs were taken within 24 h after the line was placed to confirm the correct positioning.
Results:
The success rate of the observation group was 91.30% (there were two cases of primary malposition), and the success rate of the control group was 78.57% (there were six cases of primary malposition). The success rate of the observation group was higher compared with the control group.
Conclusion:
The tip location with intracavitary ECG method improved the success rate of ECC placement via the lower limbs in neonates. This method can effectively prevent the occurrence of lower limb primary catheter malposition and has significant clinical application value.
Keywords
Introduction
The epicutaneo–caval catheter (ECC) has rapid and accurate characteristics and is useful for delivering parenteral nutrition to stable infants. 1 In adults, the sites for peripherally inserted central catheters (PICCs) include the median, cephalic, basilic and brachial veins. For neonates and children, other options include axillary and temporal veins, posterior auricular veins of the head and the great saphenous veins of the lower extremities. For newborns, the complication rate of upper and lower extremity veins is similar, but the tip position of the peripherally punctured central venous catheter in the upper limb is more prone to displacement.2,3
To reduce catheter dislocation and displacement, X-rays, ultrasounds and electrocardiograms (ECGs) are often used to locate the catheter. In the conventional X-ray film positioning method, the patient must be X-rayed in the radiology department or at the bedside after catheterisation, and if the catheter is displaced or the tip is not in the best position, adjustments are required. Due to health care providers’ lack of experience of using ultrasound, it is not widely used for detecting the catheter tip location in secondary hospitals in China.
In recent years, the effect of the tip location with intracavitary ECG method in ECC placement in newborns has gradually been confirmed. 4 However, research on the topic has primarily focussed on ECC placement via upper limb access. Few studies have investigated whether catheterisation through the lower limb pathway is suitable for intracavitary ECG technology, though some researchers indicated that catheterisation via this route has good safety and reliability. 5
To further explore the effectiveness and sensitivity of intracavitary ECG technology in the positioning of lower limb ECC tips in neonates, 28 cases of ECCs inserted via the lower limbs in the neonatal intensive care unit of our hospital were positioned by using an ECG lead. These cases were compared to a control group using chest and abdomen X-rays to determine the effect of intracavitary ECG technology in the neonatal lower limb ECC placement.
Method
Research participants
This retrospective study included 56 cases of ECC insertion via lower limb access between February 2017 and March 2019. Cases were divided into an observation group and a control group using the historical control grouping method, and the results of two different positioning methods were compared.
The inclusion criteria were: (1) an ECC was suitable for placement according to the patient’s condition; (2) all catheters were placed by lower extremity venipuncture; (3) the local skin of the catheter was normal; (4) the femoral vein was passed smoothly during catheterisation; (5) the body surface ECG showed a sinus rhythm with a heart rate of 100–180 beats per minute; (6) atrial depolarisation (a P-wave) was clearly visible; (7) the patient’s family members agreed to participate in the study.
The exclusion criteria were: (1) unstable vital signs; (2) infants younger than 2 days old; (3) uncompleted skin at the pre-puncture site; (4) the catheter failed to pass through the femoral vein; (5) the body surface ECG showed severe arrhythmia.
The observation group comprised 28 children with ECCs inserted via the lower limbs between January 2018 and March 2019. The intraluminal ECG positioning technique was used during the catheterisation process, and chest and abdomen orthoscopic radiographs were taken of the positioning after successful catheter placement.
The control group comprised 28 premature infants with ECCs inserted via the lower limbs between February 2017 and January 2018. After successful catheterisation, chest radiographs were used.
The children had no fever, bacteraemia or complicated congenital heart disease, and their immediate family members signed an informed consent form for their inclusion in the study.
Catheter preparation
An ECG monitor (COMEN C100) and an ECC catheter (Medcon 1.9 Fr) were used in this study.
Operation procedure
A comparison of ECG lead positioning sensitivity and specificity
The judgement standard of catheter positioning sensitivity was: sensitivity = the number of true positives/(the number of true positives + the number of false negatives) × 100%.
The judgement standard of specificity was: specificity = number of true negatives/(the number of true negatives + the number of false positives) × 100%.
The sensitivity was 96.30% and the specificity was 100%.
Statistical analysis
The data were analysed using the SPSS™ Statistics v18.0 software. A chi-squared (χ 2 ) test was used for comparing the data, which were expressed by n (%), and the difference was considered statistically significant (p < 0.05).
Results
Basic information
In the observation group, the gestational age of the newborns was from 28 ± 1 to 35 ± 1 weeks (220.82 ± 28.58 days), and there were 12 males and 16 females with a birth weight ranging from 720 to 2120 g (1456.43 ± 324.94 g). In the control group, the gestational age of the newborns was from 26 ± 1 to 33 ± 2 weeks (217.00 ± 24.78 days), and there were 15 males and 13 females with a birth weight ranging from 820 to 1650 g (1387.86 ± 269.98 g).
A comparison of the one-time catheter tip placement rate between the two groups
As shown in Table 1, in 28 patients in the observation group, the tip location with intracavitary ECG method was used to locate the position of the catheter tip. One-time placement without secondary adjustment was successful in 26 patients. Compared with the control group, the first-attempt success rate was improved.
Comparison of two groups of catheter tip in place rate at one time [n (%)].

A comparison of ECG lead positioning sensitivity and specificity
In the observation group, the specificity of the tip location with intracavitary ECG method in the atria was 96.3% with a sensitivity of 100.0%, as shown in Table 2. Characteristic changes in the P-waves and QRS complex amplitudes are shown in Figure 1.
Comparison of ECG monitor positioning.

Susceptibility = 96.30%, Specificity = 100%.

Characteristic changes in the P-waves and QRS complex amplitudes.
Dates related to the average duration of catheters and complications
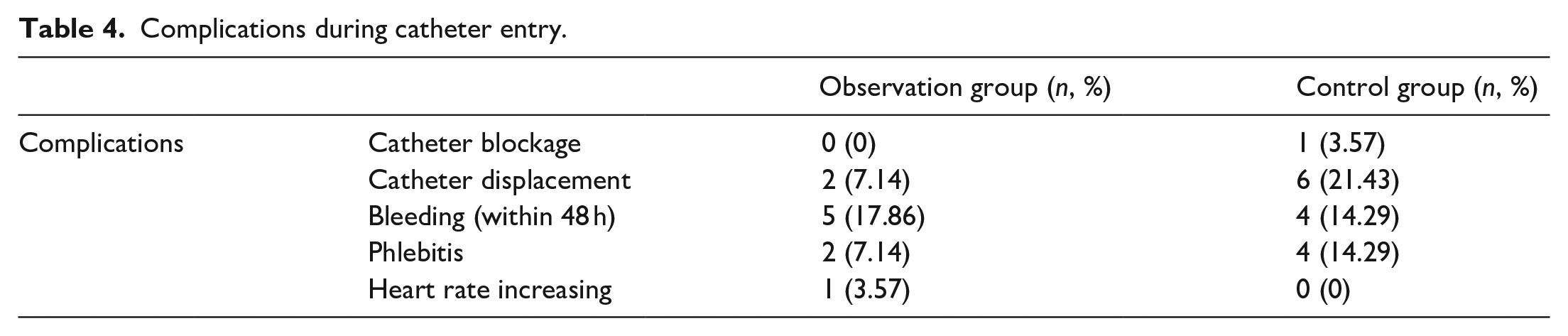
Catheters were used for 10–45 days with an average of 20 days. The indwelling time of the catheters in the observation group was 20.14 ± 8.10 days, and in the control group, it was 23.75 ± 11.10 days. No elective removal was performed in this study. See Table 3 for the reasons for catheter removal. In the observation group, there was still a small amount of bleeding on the second day of catheterisation in five cases; catheter displacement occurred in two cases, phlebitis occurred in two cases and an accelerated heart rate occurred in one case when the catheter entered the right atrium (see Table 4).
Reasons for catheter removal in the study.

Complications during catheter entry.
Discussion
ECCs are used in neonates to deliver parenteral nutrition or drugs not suitable for peripheral infusion.8–12 However, one difficulty faced in catheter placement is primary malposition. The location of the primary malpositioned catheter tip affects the indwelling time of ECCs, and it is more likely to cause fluid extravasation, phlebitis and other risks in newborns compared with adults. Because of the low weight, thin blood vessels and rapid growth of newborns, primary malposition of the catheter tip may cause more serious clinical problems.13–17 At present, X-rays of the ECC tip’s position are still commonly used in secondary hospitals in China to determine its position. However, the biggest limitation of X-rays is that the chest X-ray is not accurate. If the catheter tip was initially malpositioned and requires readjustment, an aseptic operation cannot be guaranteed, and there is a risk of catheter-related infection; if the adjustment fails, it will seriously affect the indwelling time of the catheter or even cause catheter failure.18–20 An ultrasound can provide real-time location, correct the dislocation in time and support continuous monitoring. Compared with X-rays, ECG is affordable, offers real-time positioning, and it is a simple operation. It also prevents exposure to excessive X-ray radiation.
ECG monitors are used to locate catheter tips and have been widely used in clinics in recent years. The principle is to convert the intra-atrial ECG to the body surface ECG through an intracardiac connection converter and directly observe changes in the cardiac P-wave electrophysiology under ECG monitoring.21–24 However, the study of the tip location with the intracavitary ECG method for lower extremity ECC placement is still in its infancy. The focus of this study was to explore the feasibility of this technology for use in lower extremity central venous catheterisation.
Among the 28 newborns included, characteristic changes in the P-waves and QRS complex amplitudes of 26 cases were observed. If the P-wave had a negative wave, a negative–positive two-way wave, or a high–sharp positive wave fall, it indicated that the catheter tip position had reached the atrium and/or was near the sinus node. 25 According to the anatomy of neonates, the catheter may have entered the right atrium, indicating that the catheter was too deep. Therefore, in this study, when characteristic changes in P-waves and QRS complex amplitudes were observed, the catheter was withdrawn until the P-wave amplitude became normal. A chest X-ray was taken to check that the catheter tip was above the diaphragm and had not entered the right atrium.
Observation of the one-time success rate for catheter placement in the two groups showed that in the observation group, 26 catheters were in place, and the one-time in-place rate was 92.56% (26/28). The catheter was not in place in two cases; in one case, it entered the right atrium, and in the other, it was withdrawn too far below the diaphragm. In the control group, 22 catheters were in place, and the one-time in-place rate was 78.57% (22/28). There were six cases of primary catheter malposition; in two cases it was inserted too deep into the right atrium, in one case it was inserted into the right renal vein, in one case it was folded in the inferior vena cava, in one case it was too shallow to enter above the diaphragm and in one case it was inserted into the inferior vena cava branch. In three cases, it could not be adjusted to the ideal position.
In summary, a comparison of the one-time success rate between the two groups revealed the observation group had a higher success rate than the control group, indicating that the catheter tip with intracavitary ECG method has important clinical significance for preventing primary catheter malposition. This study confirmed that this technique was also suitable for the positioning of central venous catheters inserted in the veins of the lower extremities. No elective removal was performed in this study. Some patients could have benefitted from the use of a different device, such as a tunnelled centrally inserted central catheter (CICC) or femorally inserted central catheter (FICC).
This study revealed the intraluminal ECG positioning technique to have a sensitivity of 100% and a specificity of 96.30% for ECC placement via the lower limbs. These results show that, provided the catheter reaches the vicinity of the sinus node, the P-wave must demonstrate characteristic changes; however, one case did not produce such changes. According to the observation of chest and abdominal radiographs, although the tip of the catheter was above the diaphragm in this case, it did not reach the level of the right atrium. This was related to the fact that the operator stopped delivering the line without eliciting the characteristic P-wave changes. This study suggests that when the clinical operator inserts the ECC via the lower limbs, the catheter should be inserted to a sufficient depth to observe characteristic changes in the P-wave before withdrawing the catheter and until the P-wave shape becomes normal. In one case of primary catheter malposition, the intraluminal ECG showed a P-wave with a high tip, but there was too little catheter retraction; the P-wave’s shape did not return to the original surface ECG state, and the chest and abdomen radiographs showed the catheter’s position was too deep. Comparing the changes in the P-wave’s shape before and after catheterisation can effectively prevent the occurrence of excessive catheter depth.
This study included some limitations. First, the number of cases included was small, which may have caused result bias. Second, without the prior intervention of researchers, blinding and randomisation, the results may have been subjected to bias. Third, our hospital lacked ultrasonic positioning instruments and inspection technology; therefore, the X-ray positioning commonly used in the hospital was applied, which was not the gold standard. Fourth, skin disinfection with povidone–iodine in pre-term infants, the use of heparin caps and securement with elastic bandages is inappropriate; using tissue adhesives and a transparent and semipermeable membrane for catheter stabilisation should be implemented since these are now considered the standard of care for stabilisation.
Conclusions
In summary, compared with traditional chest radiographs and body surface measurement methods, the positioning of the catheter tip with the intracavitary ECG method in placing ECCs in newborns via the lower limbs offers some advantages. These are the high success rate for one-time catheterisation, prompt adjustment of abnormal positioning during catheterisation and the timely guidance of the operator in reinserting the catheter if the adjustment fails, thereby effectively preventing the occurrence of line insertion failure and reducing radiation exposure to the newborn. This technology is easy to operate and affordable. It can be popularised and applied in placing ECCs via the lower limbs of newborns. In addition, this study observed changes not only in the P-waves but also in QRS complexes in the intraluminal ECG; however, no statistical analysis of this was performed. The sample size of this study was small and, inevitably, incurred biased results. Accordingly, the sample size should be increased in future research.
Footnotes
Author’ contributions
Conception and design: ZS, YX. Administrative support: ZS. Provision of study materials or patients: YM, XX. Collection and assembly of data: YM, XX. Data analysis and interpretation: ZS, YX. Manuscript writing: All authors. Final approval of manuscript: All authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: 2015 Hebei Province Medical Science Research Guidance Project: Clinical study of positioning the tip position of PICC catheter in newborns by intracavitary electrocardiogram.
Ethical approval
This study was conducted in accordance with the Declaration of Helsinki and approved by the Medical Research Ethics Committee of Shijiazhuang People’s Hospital [2020] No. 105. All the immediate family members agreed to sign an informed consent form.