
Abstract
Introduction:
Central venous catheters are increasingly inserted using point-of-care ultrasound (POCUS) guidance. Following insertion, it is still common to request a confirmatory chest radiograph for subclavian and internal jugular lines, at least outside of the operating theater. This scoping review addresses: (i) the justification for routine post-insertion radiographs, (ii) whether it would better to use post-insertion POCUS instead, and (iii) the perceived barriers to change.
Methods:
We searched the electronic databases, Ovid MEDLINE (1946-) and Ovid EMBASE (1974-), using the MESH terms (“Echography” OR “Ultrasonography” OR “Ultrasound”) AND “Central Venous Catheter” up until February 2023. We also searched clinical practice guidelines, and targeted literature, including cited and citing articles. We included adults (⩾18 years) and English and French language publications. We included randomized control trials, prospective and retrospective cohort studies, systematic reviews, and surveys.
Results:
Four thousand seventy-one articles were screened, 117 full-text articles accessed, and 41 retained. Thirteen examined cardiac/vascular methods; 5 examined isolated contrast-enhanced ultrasonography; 7 examined isolated rapid atrial swirl sign; and 13 examined combined/integrated methods. In addition, three systematic reviews/meta-analyses and one survey addressed barriers to POCUS adoption.
Discussion:
We believe that the literature supports retiring the routine post-central line chest radiograph. This is not only because POCUS has made line insertion safer, but because POCUS performs at least as well, and is associated with less radiation, lower cost, time savings, and greater accuracy. There has been less written about perceived barriers to change, but the literature shows that these concerns- which include upfront costs, time-to-train, medicolegal concerns and habit- can be challenged and hence overcome.
Introduction
Annually, countless central venous catheters (CVCs) are inserted worldwide, and increasingly this is facilitated by point-of-care ultrasound (POCUS).1,2 While POCUS has changed how we insert CVCs, it has yet to have a similar impact on post insertion practise, namely, how we rule out complications and confirm line placement. It is still common to order a post-insertion chest radiograph (CXR) after internal jugular (IJ) or subclavian (SC) CVCs, at least in the Intensive Care Unit, and Emergency Department. 3 This scoping review examines (i) whether routine CXRs are still justified following thoracic CVCs, (ii) whether post-insertion confirmation could be improved using POCUS instead, and (iii) the perceived barriers to change.
The post CVC CXR is typically justified as a way to screen for complications and to confirm catheter tip placement. Alternatively, it may be little more than an unexamined habit or an anachronistic protocol. For example, even before the advent of POCUS, most practitioners were content to postpone CXRs after CVCs were inserted in operating suites (OSs), and when vasoactive infusions could not wait. This is because those CXRs rarely changed management and commonly caused delays. Importantly, the routine use of POCUS has made CVC line insertion safer still.1–6 However, many are still ordering CXRs after CVC insertion even though thoracic CVCs are even less likely to be associated with pneumothorax (PTX) (<0.5%), catheter misplacement (<2.0%), or the perceived need for post-insertion catheter adjustment (<0.5%). 4 Moreover, those CXRs can still miss a small or loculated pneumothorax (PTX), especially in supine patients. 5
When it comes to confirming CVC placement after insertion, and screening for complications, POCUS offers many putative advantages over CXR. These include lower cost, less delay, less radiation, no need to move patients, no need to break the sterile field, and greater accuracy.1–6 We therefore explore the evidence base surrounding POCUS confirmation after upper extremity CVC insertion6–21 because it is less well known than that supporting POCUS during insertion, and because it may be time to forego the post insertion CXR.1,2,4,22–28 There has also been comparatively little discussion regarding resistance to change and therefore this is reviewed too. Overall, we explore the benefits of foregoing the routine CXR, and switching to POCUS, a technology that is (quite literally) already at hand.
Methods
This scoping review followed a comprehensive search of electronic databases including Ovid MEDLINE (1946-), Ovid EMBASE (1974-) using the MESH terms (“Echography” OR “Ultrasonography” OR “Ultrasound”) AND “Central Venous Catheter” and screened relevant articles, up until February 2023. We searched additional literature including clinical practice guidelines, and targeted literature, including cited and citing articles. We included adults (⩾18 years old) and limited to the English and French language. We included primary studies (RCTs, prospective and retrospective cohort studies), systematic reviews and surveys. We excluded case reports, case series, and articles that did not address ultrasound confirmation techniques, Lung-US, or US related to CVC insertion. We extracted data points onto Excel, grouped by type of technique: design, operators, technique, comparator, results, time to perform, feasibility, and reported barriers (Tables 1–3). All steps were performed in duplicate by two authors (JD, LM), with disagreements arbitrated by a third author (BB).
Primary studies regarding the use of ultrasound to screen for central venous line placement and complications.

CVC: Central Venous catheter; USG: Ultrasound-guided; LM: Landmark; SC: subcostal; US: ultrasound; ITT: Intention to treat; PP: per protocol; Sn: Sensitivity; Sp: Specificity; PPV: Positive predictive value; NPV: Negative predictive value; min: minutes; CXR: Chest X-Ray; IM: Internal Medicine; ICU: Intensive Care Unit; POCUS: Point of care ultrasound; TEE: trans-esophageal echocardiogram; SV: Subclavian vein; SVC: Superior vena cava; RIJ: Right Internal Jugular; RPA: right pulmonary artery; JV: Jugular vein; 4C: four chamber; ED: Emergency department; RASS: Right atrial swirl sign; PLAX: Parasternal long axis view; IJV: internal jugular vein; CLABSI: Central line bloodstream infection; CEUS: contrast-enhanced ultrasound; PI: primary investigator; BMI: body mass index; COPD: Chronic obstructive pulmonary disease; AUC: Area under curve; LR+: positive likelihood ratio; LR-: negative likelihood ratio; PTX: pneumothorax.
Systematic reviews regarding the use of ultrasound to screen for central venous line placement and complications.
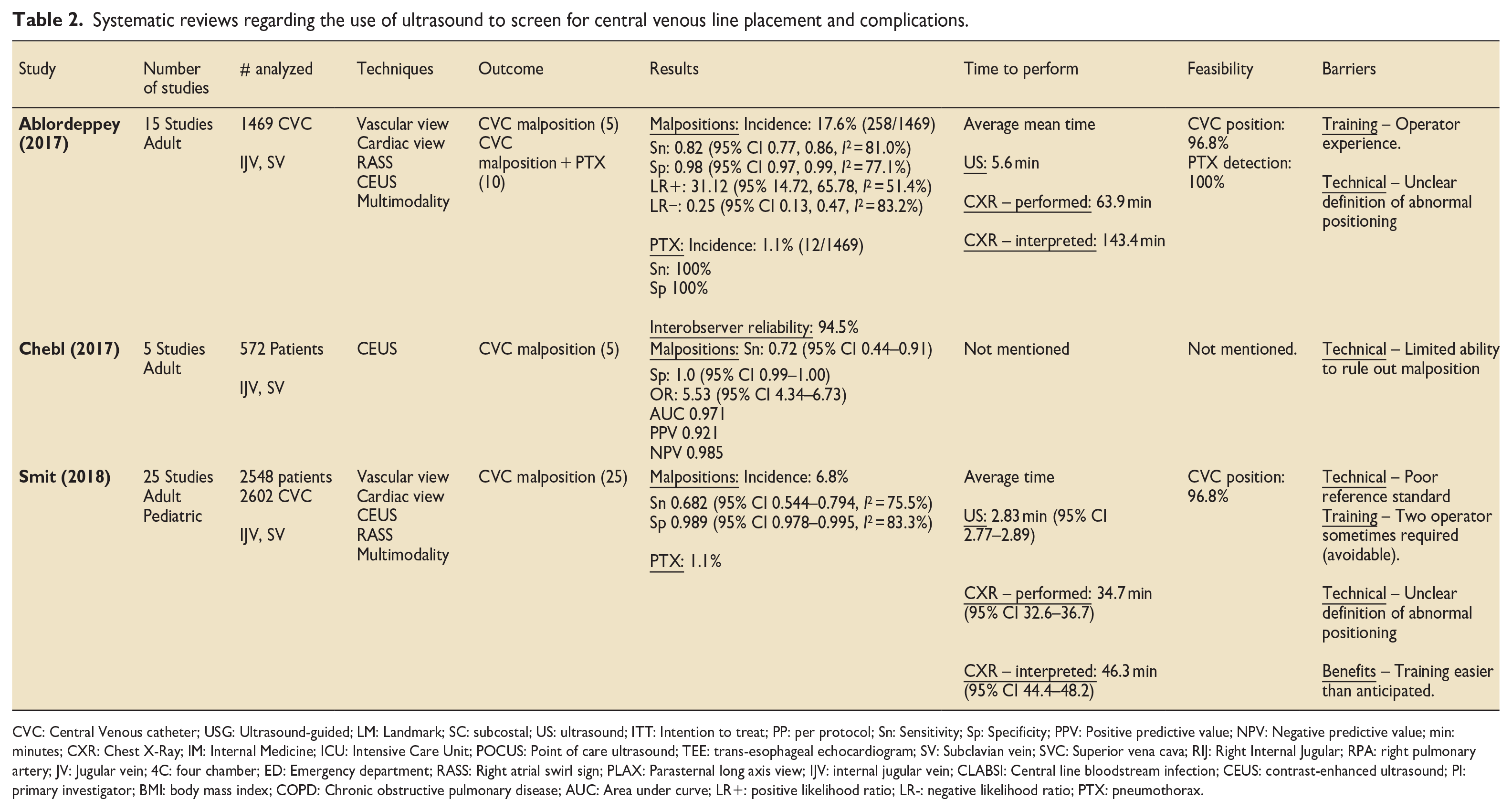
CVC: Central Venous catheter; USG: Ultrasound-guided; LM: Landmark; SC: subcostal; US: ultrasound; ITT: Intention to treat; PP: per protocol; Sn: Sensitivity; Sp: Specificity; PPV: Positive predictive value; NPV: Negative predictive value; min: minutes; CXR: Chest X-Ray; IM: Internal Medicine; ICU: Intensive Care Unit; POCUS: Point of care ultrasound; TEE: trans-esophageal echocardiogram; SV: Subclavian vein; SVC: Superior vena cava; RIJ: Right Internal Jugular; RPA: right pulmonary artery; JV: Jugular vein; 4C: four chamber; ED: Emergency department; RASS: Right atrial swirl sign; PLAX: Parasternal long axis view; IJV: internal jugular vein; CLABSI: Central line bloodstream infection; CEUS: contrast-enhanced ultrasound; PI: primary investigator; BMI: body mass index; COPD: Chronic obstructive pulmonary disease; AUC: Area under curve; LR+: positive likelihood ratio; LR-: negative likelihood ratio; PTX: pneumothorax.
Survey of practice norms and barriers to using pocus to confirm central line placement and complications. 3
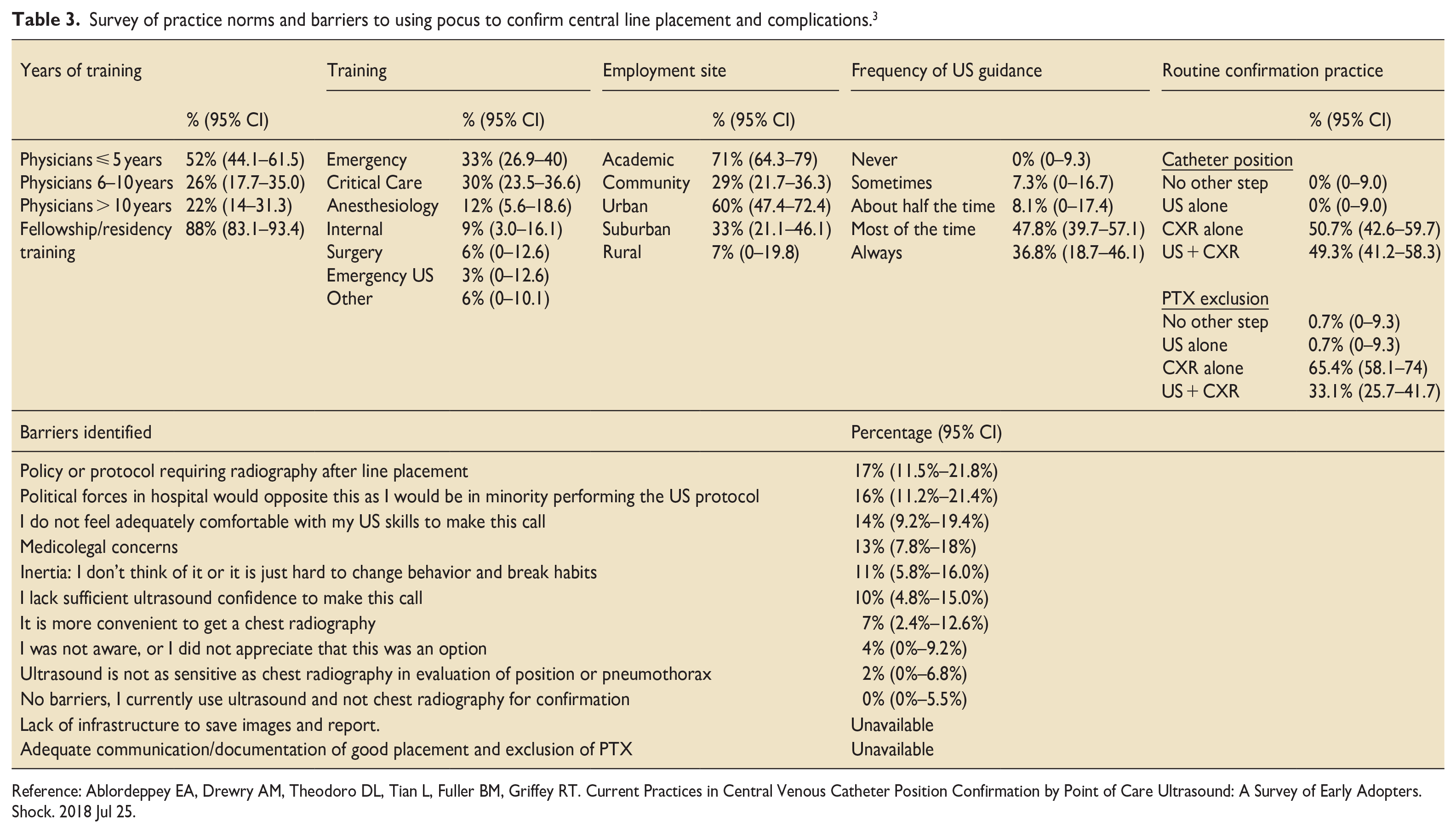
Reference: Ablordeppey EA, Drewry AM, Theodoro DL, Tian L, Fuller BM, Griffey RT. Current Practices in Central Venous Catheter Position Confirmation by Point of Care Ultrasound: A Survey of Early Adopters. Shock. 2018 Jul 25.
Results
General Search Results
Our search identified and screened 4071 articles, of which 117 full-text articles were accessed for eligibility (Figure 1).3,6–11,13,14,17–20,29–57 We retained 41 articles based on prespecified criteria for inclusion (Table 1). Regarding ultrasound guided placement and confirmation methods, 13 articles examined cardiac/vascular methods; 5 examined isolated contrast-enhanced ultrasonography (CEUS); 7 examined isolated rapid atrial swirl sign (RASS); and 13 examined combined/integrated methods (Table 1). We included three systematic reviews and meta-analyses (Table 2) and one survey (Table 3) in order to explore barriers to adoption (Table 3). Lastly, Table 4 outlines integrated lung/cardiac and vascular approaches.
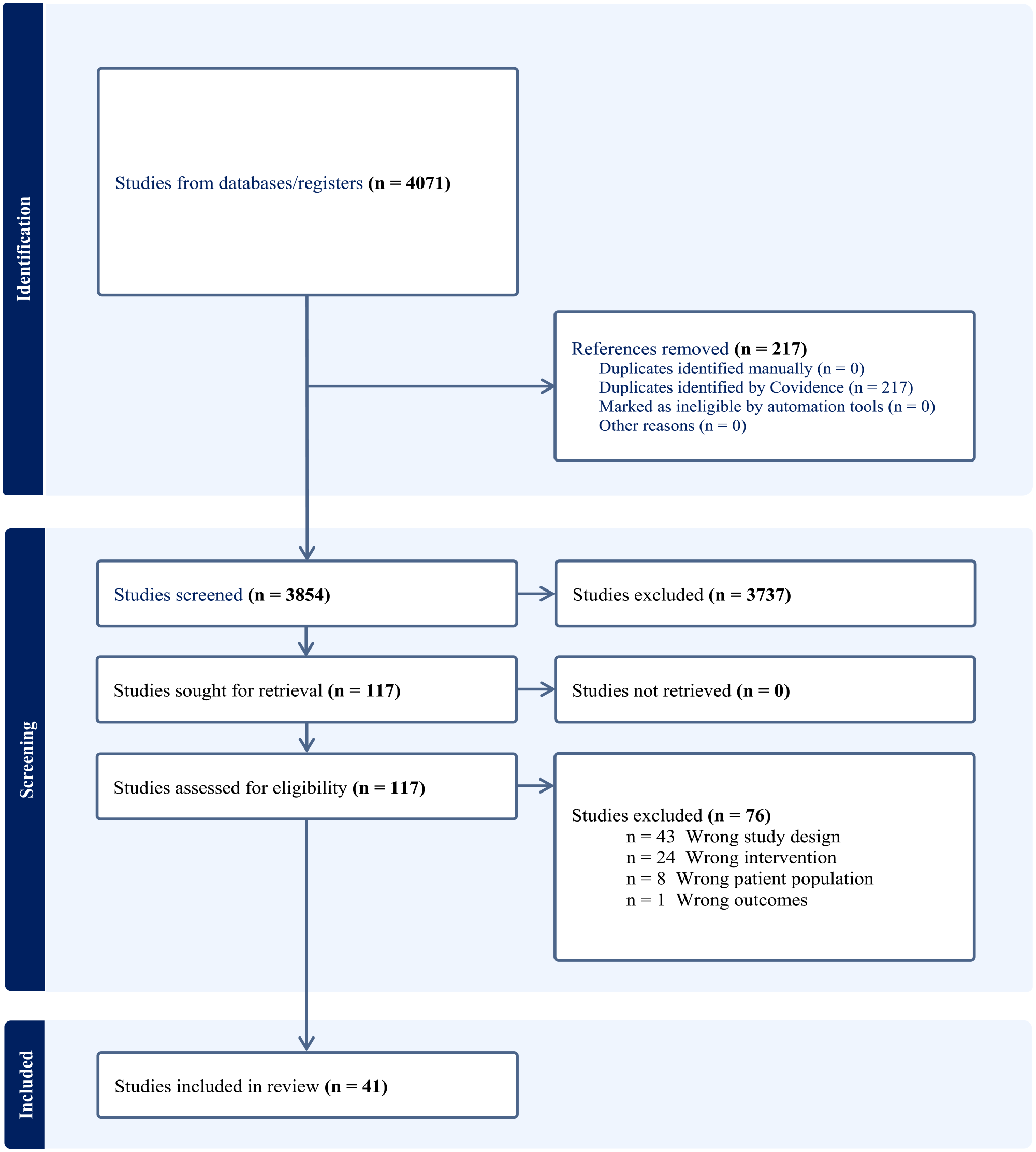
Search strategy regarding the use of ultrasound for central venous catheter placement and complications.
Integrated approaches regarding the use of ultrasound to screen for central venous line placement and complications.
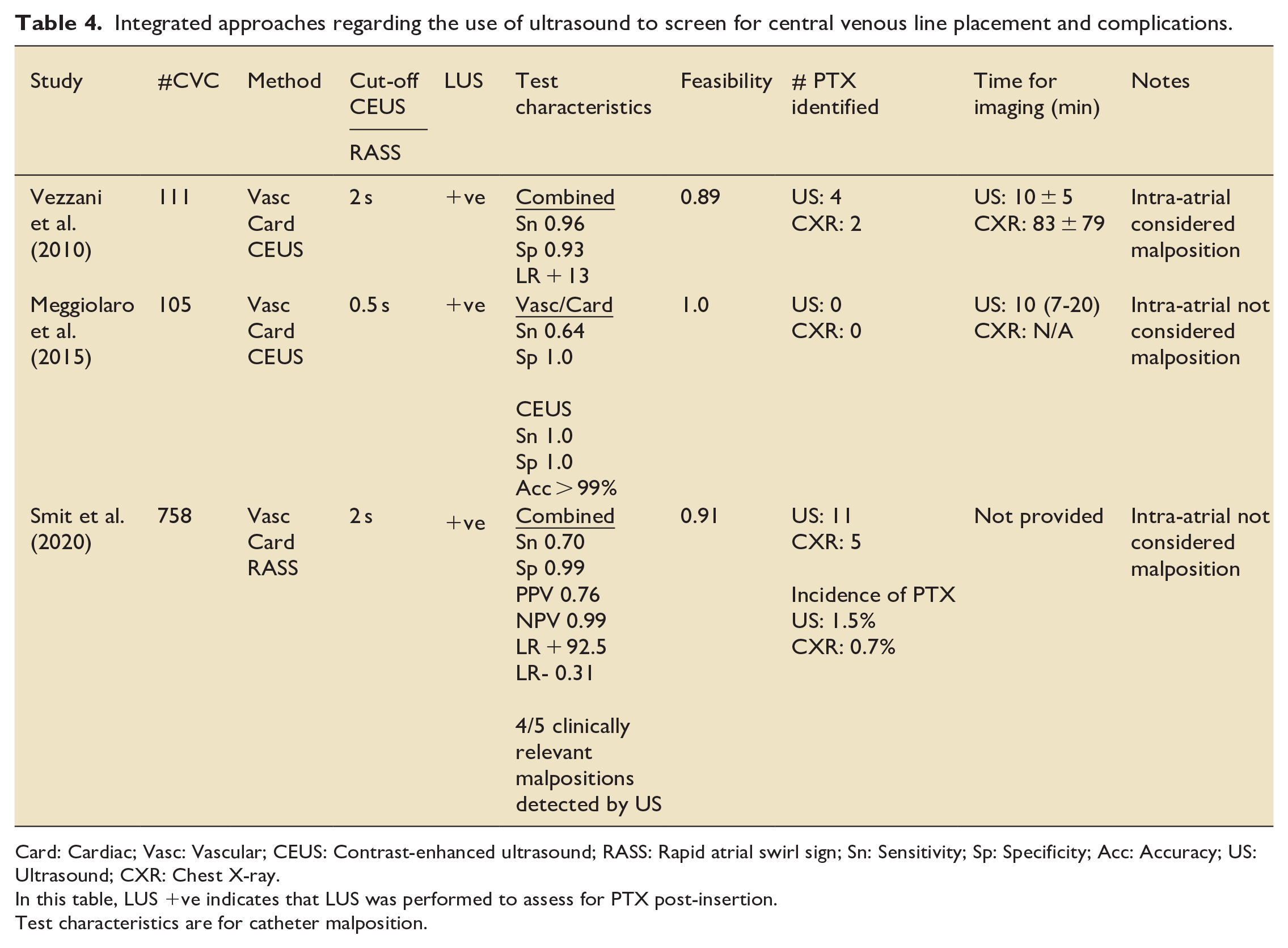
Card: Cardiac; Vasc: Vascular; CEUS: Contrast-enhanced ultrasound; RASS: Rapid atrial swirl sign; Sn: Sensitivity; Sp: Specificity; Acc: Accuracy; US: Ultrasound; CXR: Chest X-ray.
In this table, LUS +ve indicates that LUS was performed to assess for PTX post-insertion.
Test characteristics are for catheter malposition.
Comparing CXR and POCUS after thoracic CVC insertion
Our literature review highlights three main metrics when comparing CXR and POCUS: (i) cost (ii) accuracy, and (iii) detection of the CVC tip. Regarding costs, Chang et al. 58 estimated savings from foregoing CXR to be $34.58 per patient, or $39,559.52 in total, after a retrospective study of 572 internal jugular CVCs. For this expenditure only two PTXs were identified by CXR. Chiu et al. reported similarly impressive savings ($105,000–$183,000) in a retrospective study of 6875 CVC insertions. That expenditure diagnosed 23 PTX and 131 catheter misplacements, of which over 80% (107/131) were not repositioned. Similarly, Hirshberg et al. 59 performed a retrospective analysis of 1483 supradiaphragmatic CVC and found an attributable annual CXR cost of $54,494. Our review confirms that the major concerns after CVC insertion are PTX, hemothorax, tamponade, and venous thrombosis. Regarding the detection of all four of these complications, US is more accurate than CXR.60–63
Confirmation of the CVC tip by POCUS
Regarding detection of the CVC tip, POCUS also performs at least as well as CXR. For example, if we follow the recommendation that the tip should be between the lower third of the superior vena cava and the upper right atrium,64,65 then CXR studies4,24,28 identified 2% as misplaced, whereas US studies identified over 10%.14,56 The important distinction between US and CXR however, is that US generally only permits indirect tip detection, unless that is, the wire or catheter is advanced deep into the super vena cava and/or right atrium, or is in a wayward structure. Bedel et al., 8 who insisted upon intra-cardiac detection of the US guidewire prior to vessel dilatation, reported a Sn of 96%, Sp of 83%, PPV of 98%, and NPV of 55% for misplacement.
POCUS achieves indirect detection by insonating the IJ and SC vein, the heart and/or by incorporating rapid injection of saline or an opacifying agent.8–11 Zanobetti et al. 21 demonstrated that when POCUS is used to examine these major veins and atria post CVC insertion, it has a high sensitivity (Sn) and specificity (Sp) (94% and 89%, respectively), and 82% concordance with CXR. Similarly, Matsushima and Frankel 12 reported a high accuracy (90%), positive predictive value (PPV) (91%) and negative predictive value (NPV) (83%) for detecting CVC misplacement with US.
As outlined, POCUS can indirectly detect the catheter tip using echogenic turbulence or following contrast injection. Rapid instillation of non-agitated saline can produce RASS on echocardiography, a finding exploited by Weekes et al.18,19 In one prospective convenience sample of ICU and ED patients, Weekes et al. reported a Sn, Sp, PPV, and NPV of 75%, 100%, 100%, and 99.2% when using RASS to identify the catheter tip. Although non-agitated saline minimizes the risk of air embolism; it also reduces echogenicity, and therefore potential accuracy.18,19,41
CEUS makes use of agitated saline or a lipid contrast agent. In one prospective observational study of using agitated saline, Cortellaro et al. 9 reported a Sn, Sp, PPV and NPV of 33%, 98%, 67% and 94% respectively. Baviskar et al. 7 found a SP (100%) and Sn (100%) in 25 non-consecutive patients. Although these results are promising, CEUS risks air embolism with inadvertent arterial placement or if there is a patent inter-atrial shunt. This is less likely when low volumes (<1 ml) of agitated saline are used. 66 Another downside is that two practitioners are needed while maintaining the sterile field: one to obtain images and one to inject.
Integrated POCUS for CVC placement: The future?
Our review serves as a reminder that “a full confirmatory US” has five distinct steps: (1) Identify and cannulate the correct vessel in real-time, (2) visualize the wire in the correct place, (3) visualize the catheter, (4) rapidly instill non-agitated saline or agitated-saline with 0.5 ml air to opacify the endovascular cavity and infer the location of the catheter tip, and (5) use lung-US to exclude PTX.7,9,11,14,16–19,41 Practitioners may be reassured by combining confirmatory techniques; however, we only found three studies that included bilateral 2D vascular and cardiac imaging, plus agitated saline or CEUS, plus lung ultrasound (Table 4).14,17,55
Discussion
Our review confirms that not only is there widespread literature support for POCUS during IJ and SC CVCs insertion,22,67 there is also widespread literature support for using POCUS after CVC insertion; even if the latter is not as widely known or followed.30,35,54 Overall, when used to confirm CVC placement and rule out peri-insertion complications, POCUS has superior Sn compared to CXR, and comparable Sn to computed tomography.6,7,9,11,13,14,16–19,21,41 When POCUS, rather than CXR, is used, it also means less radiation and shorter delays.4,5,9–11,17,20,25–27 POCUS added only 30 s to 10 min, whereas CXR added 20–83 min.9,12,17–19 While there was no evidence that POCUS resulted in better clinical outcomes when compared to CXR, there were no reported downsides, and numerous putative benefits. In short, the routine post-CVC CXR increasingly looks like an anachronism left over from pre-POCUS days.
When comparing POCUS and CXR, POCUS was also superior in terms of cost, accuracy and ability to detect the CVC tip.4,58,59 Moreover, three systematic reviews and a survey (Tables 2 and 3) have confirmed that there is robust support for US over CXRs.30,35,54 Regardless, before adopting POCUS we need to identify and overcome potential barriers. These include patients with obesity, pulmonary disease, pacemakers, and chest wall abnormalities8,13,33,34,36,48,55; though not cervical collars or open abdomens. 13 Notably, these same issues affect CXRs too. We also need skilled US operators and interpreters, though, again, this applies to CXRs too. Fortunately, for POCUS operators, less than 10 h of training usually delivers basic proficiency,12,13,21 and the need to practise on patients can be avoided by using mannequins and simulation. 68 In return for the upfront time investment the “payoff” is a significantly shorter time to confirmation with US: 5–11 min for cardiac/vascular studies.12,13,21 Integrated approaches demonstrated a wider time interval of 1–20 min.14,17,19 These longer intervals, while uncommon, could frustrate time pressured practitioners. Nonetheless, CEUS only added 30–60 s. 9 This compared to 65–75 min for CXR.12–14,17,21,55
The remaining barriers center on medicolegal concerns, and change inertia. These should not be ignored, but can be challenged by our cumulative literature review. Firstly, in terms of safety, CVC insertion represented only 1.7% of 6449 claims over 30 years from the 2004 American Society of Anesthesiologists Closed Claims database. 69 This low number was despite CVCs being one of the most common procedures, and came from a time before US made CVC insertion safer still. Others may assume that they have to do an XR to ensure that a SC CVC tip has not ended up in the ipsilateral IJ, or because patients are often intubated at the same time anyway (hence a single CXR can confirm both endotracheal tube placement and CVC placement). Again, though, this can all be done with POCUS by quickly insonating both the airway (via the front of the neck) and the veins (via the side of the neck). Finally, if practitioners and administrators still wish, or need, to have a radiologist’s review, then this can be done as easily with US images. This is because US images can now be easily stored and viewed remotely; just like the CXRs of old. In short, we humbly submit that the routine post CVC CXR is more ritual than rational.
Footnotes
Authors’ note
The authors have composed, revised and approved this manuscript
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
The work is original, and not under consideration elsewhere.