
Abstract
Background:
Infection is one of the most common causes of death in hemodialysis patients. Catheter infections are among the most common infections in this patient group. Spondylodiscitis which has a high incidence in ESRD is more commonly encountered in patients with CVCs compared to AVF. In this study, we aimed to evaluate the frequency and risk factors of spondylodiscitis in catheter-related bloodstream infections in hemodialysis patients.
Methods:
In total, 1620 patients were screened and 42 male and 35 female patients with central catheter infection with a mean age of 65.8 ± 14.9 years were included in this study. Patients with metastatic infections secondary to CVC related bloodstream infections were determined. The diagnosis of spondylodiscitis was based on clinical information, computed tomography (CT) and magnetic resonance imaging (MRI), and vertebral cultures.
Results:
Metastatic infection due to catheter infection was observed in 15 patients (19.5%). In the regression analysis, CRP level and RRT time were found to be significantly correlated with the development of metastatic infection. Spondylodiscitis was the most common subtype of metastatic infections (8/15). The presence of lumbar hernia was associated with increased risk of metastatic spondylodiscitis in case of catheter infection in hemodialysis patients. The only factor associated with resistance to medical treatment was the time from admission to diagnosis.
Conclusion:
Patients with long RRT time and high blood CRP levels on admission should be closely monitored for metastatic infection in patients with CVC related bloodstream infections. Screening for spondylodiscitis with CT or MRI should be performed in patients with symptoms, since early diagnosis may prevent the development of possible neurological deficits and treatment resistance.
Introduction
Hemodialysis is the most frequently used renal replacement therapy (RRT) modality in end stage renal disease (ESRD). In Turkey there are 83,738 end stage renal disease patients and 61,341 (73.2%) of these patients are under hemodialysis treatment. 1 Central venous catheters (CVC) are the second most common vascular access after arteriovenous fistulas (AVF) with a prevalence of 22.33%. 1
The incidence of catheter related bloodstream infections varies among the studies but known as the most common complication of CVC’s and is associated with increased morbidity and mortality.2,3 CVC related bloodstream infections can be complicated with metastatic infections. Spondylodiscitis which has an increased incidence in ESRD is more commonly encountered in patients with CVCs compared to AVF. 4
Infectious spondylodiscitis has non-specific symptoms including back pain, fever, local tenderness and neurologic defects, and the incidence rate is 2.2/100,000 patient years. 5 Treatment of spondylodiscitis consists of intravenous antibiotics directed by the culture results or empirical antibiotics for severely ill patients that cover common pathogens like Staphylococcus aureus and Escherichia coli. Debridement and decompression of the spinal canal are required in cases of neurological dysfunction, instability, deformities sepsis, and unresponsiveness to antibiotics. 6 Delays in diagnosis can result in mortality and neurological complications. Spondylodiscitis in CKD is generally presented as case series in the literature. In our literature review we could not find any study that determines the risk factors for development of spondylodiscitis in catheter related bloodstream infections in hemodialysis patients.
In this study, we aimed to evaluate the frequency and risk factors of spondylodiscitis secondary to catheter related bloodstream infections in hemodialysis patients.
Methods
We retrospectively screened 1620 patients who had been hospitalized in nephrology clinic of Gazi University Hospital between August 2018 and March 2020. One hundred and thirty-five of these patients had arteriovenous fistula or arteriovenous graft and 270 patients had CVC’s. Seventy-seven patients with CVC related bloodstream infections were included in this study. The study was approved by Gazi University Ethics Committee and was performed in accordance with Declaration of Helsinki. Demographic and clinical data were collected including age, gender, etiology of kidney disease, catheter characteristics (insertion site, type and duration), microorganisms responsible from infections, clinical signs and symptoms of patients, diagnostic tests performed, treatment, and clinical course. The patients with metastatic infections secondary to CVC related bloodstream infections were determined. As a first step, patients with metastatic infections were compared to patients with non-metastatic catheter related bloodstream infections. At the second step, patients with spondylodiscitis secondary to catheter related bloodstream infections were determined and compared with non-spondylodiscitis group. The diagnosis of spondylodiscitis was based on clinical information, computed tomography (CT) and magnetic resonance imaging (MRI), and vertebral culture.
Statistical analyses were performed using the SPSS software version 25. The variables associated with metastatic catheter related infection development and spondylodiscitis development were investigated using Chi-square, Fisher exact, Student’s t and Mann-Whitney U tests, where appropriate. For the multivariate analysis, the possible factors identified with univariate analysis were further entered into the logistic regression analyses to determine independent predictors of patient outcome. Hosmer-Lemeshow goodness of fit statistics were used to model fit. A 5% type-1 error level was used to infer statistical significance.
Results
A total of 77 patients (42 males and 35 females) with CVC related bloodstream infections were included in the study. Mean age was 65.8 ± 14.9 years. Hypertension (80.5%), diabetes mellitus (51.9%), and coronary artery disease (37.7%) were the most common comorbidities. Eighty-seven percent of the patients had tunneled CVC as the vascular access and internal jugular vein was the most common site (89.6%) for catheter placement. Only four of the patients’ (5.2%) vascular access were femoral CVCs. Mean RRT time was 1042.9 ± 1602.9 days and mean CVC duration was 366.17 ± 567.66 days. Gram positive microorganisms were the most common group and coagulase negative staphylococcus (39%), and staphylococcus aureus (13%) were the most common infectious agents. All patients with catheter infections complicated by a metastatic infection underwent catheter exchange procedure and the new catheters were inserted to another site if possible.
Fifteen patients (19.5%) had a metastatic infection including eight spondylodiscitis (10%), two infective endocarditis (2.5%), two intraabdominal abscess (2.5%), one peripheral osteomyelitis (1.25%), one septic arthritis (1.25%), and one septic emboli (1.25%). Six (40%) of the patients were male. Mean age of the patients with metastatic infection was 66.3 ± 11.2 years. Demographic features and laboratory values of the CVC related bloodstream infected patients compared according to presence of metastatic infection is shown in Table 1. Fifteen patients with metastatic infection were compared with the catheter infection group without metastatic infection. Between two groups age (66.3 ± 11.2 vs 65.7 ± 15.7, p: 0.812) and gender (M/F: 36/26 vs 6/9, p: 0.254) were statistically similar. Twelve of 15 patients with metastatic infection (80.0%) and 55 of the 62 patients without metastatic infection (88.7%) had fever during the hospitalization. There was no difference in terms of fever between patients with and without metastatic infection (p = 0.399). We compared the interval between the start of the fever and the start of antibiotic therapy between patients with and without metastatic infection, and we observed that this interval was significantly longer in patients with metastatic infection compared to patients without metastatic infection (5 (1–30) days vs 2 (1–30) days, p = 0.03). Regarding comorbidities, no statistically significant difference was found in the two groups in terms of diabetes mellitus, coronary artery disease, heart failure, hypertension, or malignancy. There was no statistically significant difference with regard to CVC duration (362.9 ± 483.5 days vs 337.0 ± 589.6 days, p: 0.980) and presence of tunneled CVC (14/15, 93% vs 55/62, 88.7%, p = 0.822) but there was a significant difference in terms of the duration of RRT (1973.9 ± 2761.3 days vs 802.1 ± 1042.0 days, p: 0.011). When the groups were evaluated in terms of microorganisms, gram positives were observed most frequently in both groups (11/15 vs 41/62), while there was no statistically significant difference between the groups with and without metastatic infection in terms of the causative group and its type (p = 0.078, p = 0.448). Patients with lower hemoglobin levels and higher serum C reactive protein (CRP) values were more prone to metastatic infections (p = 0.019 for both parameters). In the regression analysis, CRP level (β = 0.234, p = 0.04) and RRT time (β = 0.269, p = 0.018) were found to be significantly correlated with the development of metastatic infection (Figure 1). The duration of antibiotic treatment was significantly longer in the patients with metastatic infection (28.3 ± 16.5 days vs 18.2 ± 8.5 days, p = 0.03).
Demographic features and laboratory values of the CVC related bloodstream infected patients compared according to presence of metastatic infection.
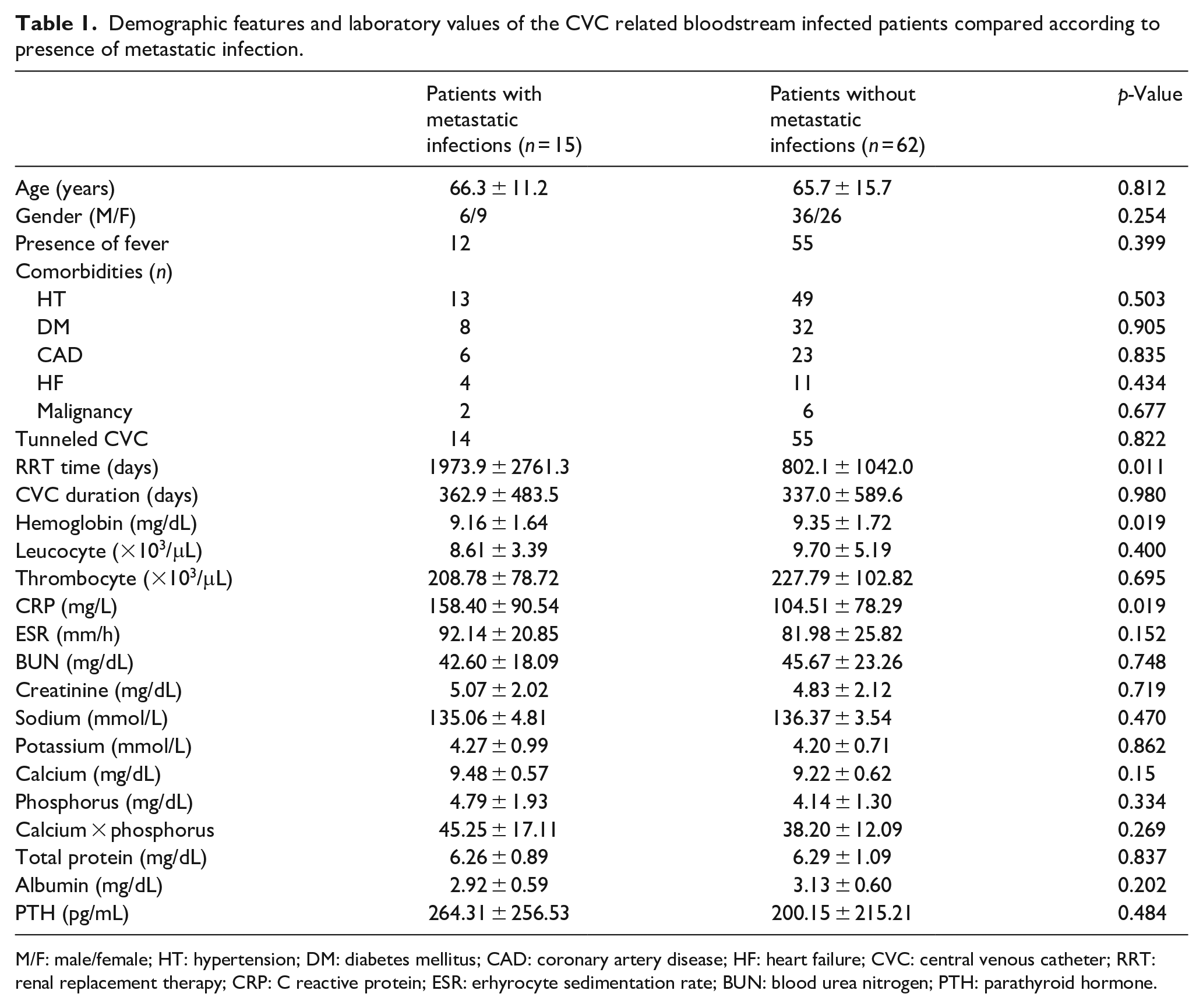
M/F: male/female; HT: hypertension; DM: diabetes mellitus; CAD: coronary artery disease; HF: heart failure; CVC: central venous catheter; RRT: renal replacement therapy; CRP: C reactive protein; ESR: erhyrocyte sedimentation rate; BUN: blood urea nitrogen; PTH: parathyroid hormone.
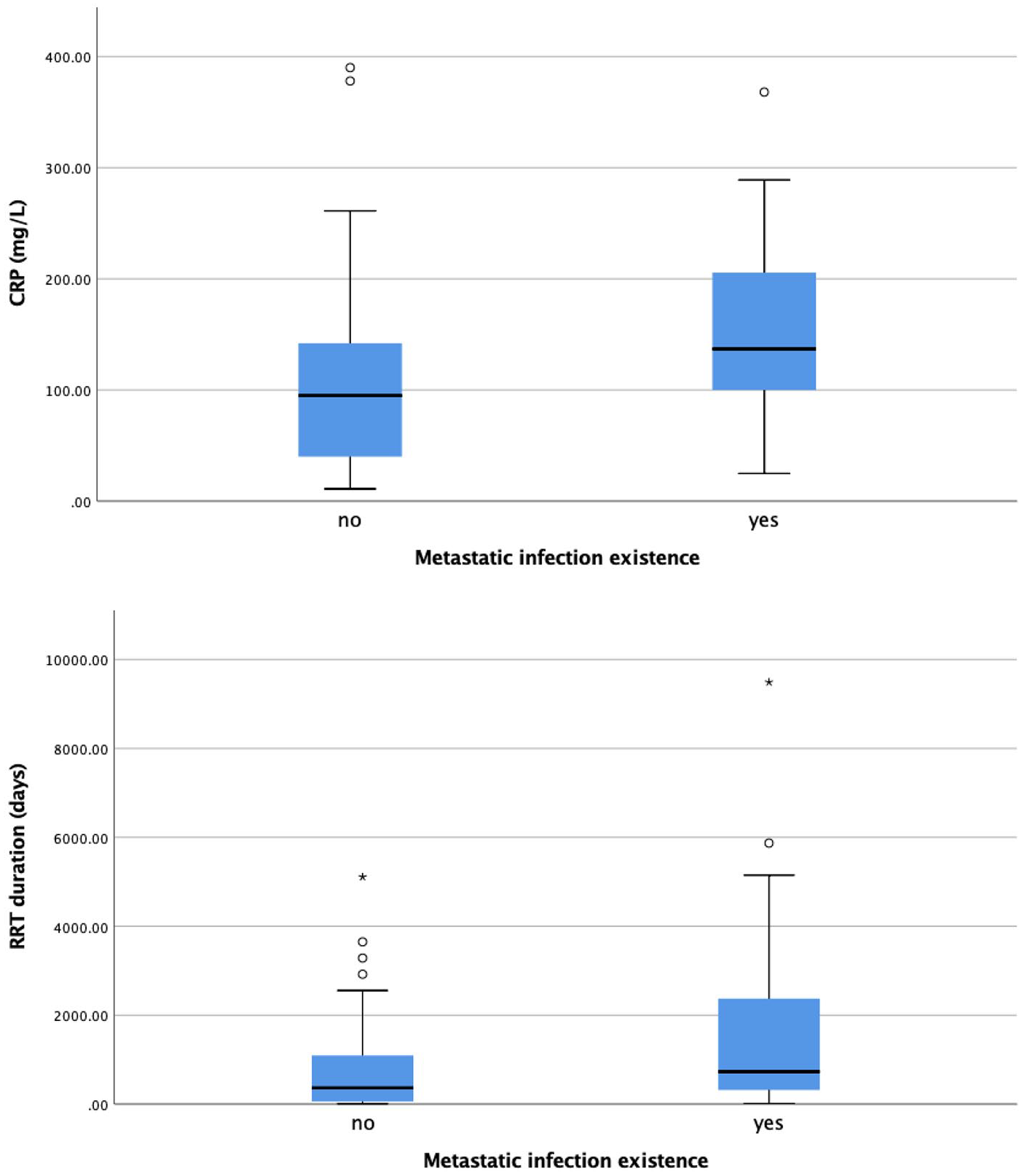
C-reactive protein (CRP) (mg/L) (β = 0.234, p = 0.04) and renal replacement therapy (RRT) duration (days) (β = 0.269, p =0.018) in patients with and without metastatic infections.
Spondylodiscitis was the most common subtype of metastatic infections (8/15, 53.3%). Biopsy and culture of the vertebrae could be performed in only two patients. The microorganisms that grew in the vertebral cultures were same with the microorganisms that were produced in the blood for both of these patients. All of the diagnoses of spondylodiscitis (including these two patients) were made by characteristics findings in the vertebral imaging which were edema of the vertebral body, irregularity of the vertebral margins, hypointense and indistinct bone marrow on T1-weighted images, and increased fluid expression of inflammatory exudate on T2 images for MRI. Two of the cases were diagnosed with CT while six cases were diagnosed with MRI. Spondylodiscitis of the patients was observed in different areas from the degenerative hernia sites detected before the diagnosis.
Patients with spondylodiscitis were compared with the CVC bloodstream infection group that did not develop spondylodiscitis. Demographic features and laboratory values of the two groups are presented in Table 2. There were no statistically significant differences between the two groups in terms of comorbid diseases, age, and gender. However, 5 of 8 patients with spondylodiscitis and 5 of 69 patients without spondylodiscitis previously had lumbar hernia (p = 0.001). When the causative microorganism was evaluated, there was a statistically significant difference in favor of gram positives (6/8, 75% vs 46/65, 70%, p = 0.047). Three of the patients with spondylodiscitis were infected with staph epidermidis, two with staphylococcus aereus, two with multiple organisms, and one with candida albicans. The most common complaint of patients with spondylodiscitis was low back pain, while two patients was admitted with motor deficiency (25%). The time from admission to diagnosis of spondylodiscitis was 4.25 ± 4.31 days. All cases of spondylodiscitis were in the lumbar area (three patients L1-2, two patients L2-3, two patients L4-5, and one patient L5-S1). The duration of antibiotic treatment was significantly longer in the patients with spondylodiscitis (32.5 ± 16.37 days vs 18.72 ± 9.53 days, p = 0.003). Surgery was deemed to be indicated in two patients (25%). Recurrence was observed in two of the patients (25%). The only factor associated with resistance to medical treatment was the time from admission to diagnosis (7.25 ± 4.34 days vs 1.25 ± 0.5 days, p = 0.018).
Demographic features and laboratory values of the CVC related bloodstream infected patients compared according to presence of spondylodiscitis.
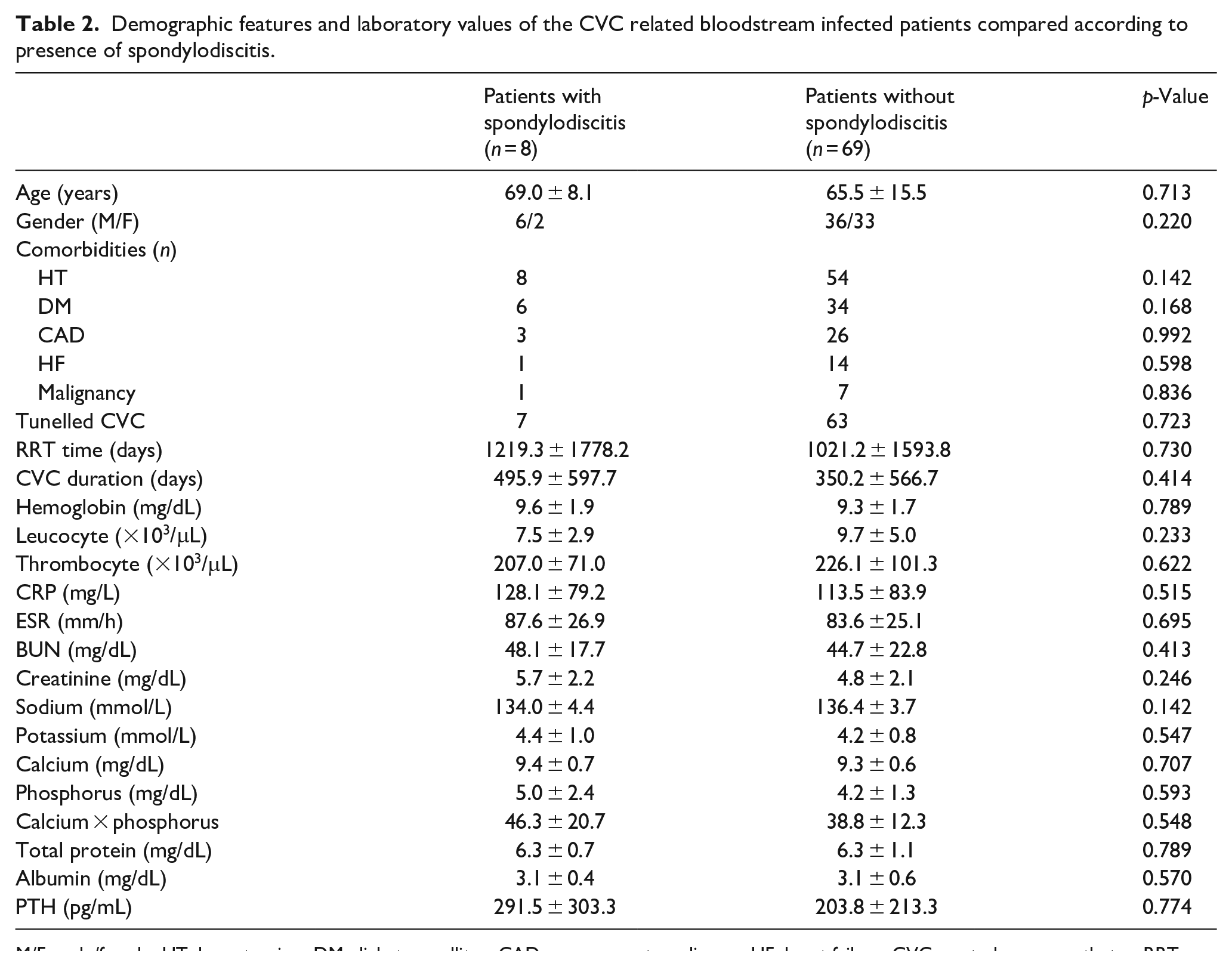
M/F: male/female; HT: hypertension; DM: diabetes mellitus; CAD: coronary artery disease; HF: heart failure; CVC: central venous catheter; RRT: renal replacement therapy; CRP: C reactive protein; ESR: erhyrocyte sedimentation rate; BUN: blood urea nitrogen; PTH: parathyroid hormone.
Discussion
Metastatic complications due to CVC related bloodstream infections can be as frequent as 7% according to literature. 7 Older age is a risk factor for these conditions and most common site of infections are listed as infective endocarditis, osteomyelitis, spinal epidural abscess, and septic arthritis. 8 In our study, the frequency of metastatic complications was 20.8%. This high frequency can be a result of increased life span and awareness of these conditions in the hemodialysis population. Mean age was higher in patients with metastatic complications. Although this difference did not reach statistical significance, it should be taken into account. Another important point is the RRT time which was statistically longer in the patients with metastatic complications. This difference can be a result of altered innate and adaptive immunity of the patients with ESRD and its connection to residual renal function. 9
Infectious spondylodiscitis is a rare condition but patients under hemodialysis treatment and elderly patients are expected to have a higher incidence of spondylodiscitis.10 –16 Spondylodiscitis in ESRD is mostly presented as case series in the literature. In a systematic review of 30 studies by Madhavan et al. there were 212 patients on maintenance hemodialysis with a mean age of 61.9 ± 13.0 years and a slight male dominance. However, this study’s population was consisting of patients with different vascular access types, even though the CVC related bacteremia was listed as the most common etiology in spondylodiscitis. 17 Our study is the first study that compares spondylodiscitis in isolated CVC related bloodstream infections to the best of our knowledge. We observed 8 spondylodiscitis cases among 77 patients with catheter related bloodstream infections in hemodialysis patients (10.4%). Spondylodiscitis was the most common site of metastatic infections in our population. Low back pain was most common symptom, lumbar area was the most common site of spondylodiscitis and gram positive microorganisms were the most common agents compatible with the literature.12 –15
The recognition of the spondylodiscitis in hemodialysis patients is complicated because of two reasons. The fist reason is that symptoms can be confused with destructive spondyloarthropathy of renal disease. 18 Most common symptom of the spondylodiscitis is back pain and destructive spondyloarthropathy can cause similar back pain in this population. This causes a delay in the diagnosis and results in high morbidity and mortality. Second reason is the nephrogenic systemic fibrosis risk in MRI. MRI with gadolinium is the gold standard non-invasive procedure to diagnose the infectious spondylodiscitis. Despite that group II gadolinium-based contrast agents are much safer compared to group I agents 19 there is still a great reluctance in performing MRI even with these safer agents in daily clinical practice for patients with impaired renal function and this limited use of MRI because of nephrogenic systemic fibrosis risk of gadolinium delays the diagnosis. 20 It’s known that CT scans require about 6 weeks for diagnosis of the lesion; thus, MRI is more diagnostic at an earlier time period and MRI without gadolinum cannot differentiate between infectious and non-infectious spondylodiscitis. 21
In our study, lumbar hernia was the only associated condition with spondylodiscitis and relapse rate was 25%. In a study of 18 maintenance hemodialysis patients with spondylodiscitis, baseline degenerative spinal disease was reported as 61.1% and relapse rate was 33.3%. 22 These numbers are higher compared to general population and compatible with our study. The only factor associated with unresponsiveness to medical therapy was time from admission. This can be due to late diagnosis which can result more neurologic deficits.
In conclusion patients with advanced age, long RRT time and high blood CRP levels on admission should be closely monitored for metastatic infection in the cases of CVC related bloodstream infection. Evaluation for spondylodiscitis with CT or MRI should be performed in patients who are on maintenance hemodialysis treatment and who describe new-onset back pain, change in back pain, or focal neurological deficits with active CVC related bloodstream infections. Symptom follow-up should be done carefully, as early diagnosis may prevent the development of possible deficits and unresponsiveness to medical treatment. Because of increased relapse rate ESRD patients with spondylodiscitis must be closely followed up.
Footnotes
Acknowledgements
This study was approved by Ethics Committee of Gazi University and was performed according to Declaration of Helsinki.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.