
Abstract
Objective
To assess the 10-year risk of cardiovascular disease and potential impacting factors among patients undergoing hemodialysis in Yaoundé, Cameroon.
Design
A cross-sectional study in January 2016.
Setting
Patients were recruited at the dialysis unit of the Yaoundé University Teaching Hospital, Cameroon.
Participants
These were hemodialysis patients aged 20 years and above, dialyzing in the above unit since at least 3 months and volunteering to be enrolled in the study.
Main outcome measures
The risk of cardiovascular disease was assessed using the Framingham risk score.
Results
We included 44 patients. The risk of cardiovascular disease ranged from less than 1% to more than 30% with a median of 12.3% (interquartile range 4.9–24.4). Twenty hemodialysis patients (45.5%) had a low risk of cardiovascular disease (<10%), 10 (22.7%), a moderate risk (10–20%), and 14 (31.8%) presented a high risk of cardiovascular disease (>20%). In multivariable linear regression analysis, duration on dialysis (adjusted β = 0.11; p = 0.003), number of weekly sessions of physical activity (adjusted β = −1.35; p = 0.018), fasting serum glucose levels (adjusted β = 4.22; p = 0.022), serum triglycerides levels (adjusted β = 5.94; p = 0.033), and serum urea levels (adjusted β = −2.08; p = 0.039) were independently impacting our patients’ risk of cardiovascular disease.
Conclusion
Around 55% of our study population presented a moderate or high risk of cardiovascular disease. Duration on dialysis, number of physical activity sessions per week, fasting serum glucose, serum triglycerides, and serum urea levels may impact our hemodialysis patients’ risk of cardiovascular disease.
Background
The worldwide incidence of chronic kidney disease (CKD) has been sharply increasing over the recent decades. In developing countries where there is cohabitation of a double burden of infectious and non-communicable diseases [1], CKD constitutes a significantly more important challenge for health systems than elsewhere [2,3]. Morbidities and mortalities arising from CKD in these areas are enormous and related to limited access to treatment options [4].
Currently, renal replacement therapy (either maintenance hemodialysis (HD) or peritoneal dialysis) has been widely adopted as the mainstay of care for patients with end-stage CKD [5]. Dialysis prolongs survival, reduces morbidities, and improves patients’ quality of life. However, these patients are at an elevated risk of cardiovascular disease (CVD) [6–8]. Indeed, CVD is the leading cause of deaths in this category of patients; it accounts for almost 40–50% of all-cause mortality, a rate 10 to 30 fold higher than in the general population [9–11]. This risk is even greater for young dialysis patients [12].
Evidence has accumulated a number of risk factors for CVD in dialysis patients among which are older age, hypertension, diabetes mellitus (DM), vascular calcification, inflammation, increased visceral fat level, dyslipidemias, high serum uric acid levels, and lower calcium levels [6,13–17].
These risk factors may vary from one population to another; they should be identified and addressed in an attempt to mitigate the burden of CVD in dialysis patients. Some studies have evaluated the global risk of CVD in people living in sub-Saharan Africa (SSA) [18,19], but very few have been carried-out among patients on maintenance HD. This study was thus designed, willing to assess the risk of CVD among a group of patients undergoing maintenance HD in Cameroon (a SSA country) and to identify potential factors likely to impact this risk.
Methods
Ethical statement
Before starting this study, an ethical clearance was delivered by the Ethical Review Board of the Catholic University of Central Africa based in Yaoundé, Cameroon (Number 0132/2016), and an authorization was obtained from the administrative authorities of the Yaoundé University Teaching Hospital. All the procedures used in this study concurred with the current revision of the Helsinki Declaration. All aspects in relation with the study were fully presented and explained to each participant, and we enrolled only those who volunteered to participate; they signed the consent form in this respect. Refusal to be included did not expose the person to any management prejudice. Results of patients were sent to their physicians for better care. In addition, participants were educated and sensitized on the huge benefits of healthy diets and regular physical activity.
Study design, setting, and participants
In January 2016, we carried-out a cross-sectional study at the Yaoundé University Teaching Hospital, which is located in Yaoundé, the capital city of Cameroon. This is a tertiary reference hospital including a dialysis unit with nearly 70 patients being regularly dialyzed 2 to 3 times per week with each session lasting for 4 h.
Participants were end-stage CKD patients, aged 20 years and above, who have been dialyzing for at least 3 months in the unit, and who voluntarily accepted to be included in the study. Patients on transit in Yaoundé and coming to be dialyzed in the unit were not included in this study.
Data collection
A structured, auto-administered, and pre-tested questionnaire served for data collection, which comprised socio-demographic characteristics (age, sex, religion, marital status, level of education, ethnic origin, and profession), medical history (past medical events, family history of diabetes, hypertension, or other relevant disease), and lifestyle habits (physical exercise, smoking, consumption of alcohol, and consumption of fruits and vegetables). No amendments were brought to the questionnaire following pre-testing. Thereafter, we conducted a physical examination during which blood pressure (composite of systolic blood pressure (SBP) and diastolic blood pressure (DBP) in mmHg), body dry weight, and height (respectively to the nearest kilogram and centimeter) were measured. Body mass index (BMI) was then derived as weight (kg)/height2 (m2). Subsequently, we agreed on an appointment for blood collection.
Blood collection and biochemical assays
Blood was aseptically collected after a 12-h overnight fasting and before dialysis, then put on ice and immediately transported to the biochemistry laboratory where plasma or serum specimens were separated by centrifugation at 3000 rpm within 5 min for analyses without delay. Biochemical assays included fasting plasma glucose (FPG), total cholesterol (TC), triglycerides (TG), high-density lipoproteins cholesterol (HDL-C), urea, and creatinine. Low-density lipoproteins cholesterol (LDL-C) was calculated using Friedwald’s formula [20]. The GFR was determined using the MDRD formula, which takes into account the age (years), sex (male/female), weight (kg), creatinemia (µmol/l), and ethnicity (African origin or not) [21]. We used an electronic calculator for this process, on this webpage: “http://publication.radioanatomie.com/002_manipulateurs/calcul-de-la-clairance-de-la-creatinine.php.”
Calculation and stratification of the cardiovascular risk (CVR)
We used the Framingham risk score (FRS) to assess the 10-year risk of cardiovascular events. It was electronically derived on this web page “https://www.cvdriskchecksecure.com/FraminghamRiskScore.aspx,” based on the following parameters: age (years), sex (male/female), diabetes (yes/no), smoking (yes/no), BP lowering medications (yes/no), SBP (mmHg), TC (mmol/l), and HDL-C (mmol/l). The FRS is a predictor of the 10-year risk of developing a coronary event (composite of myocardial infarction and coronary death), and is considered a standard and generally acceptable approach to risk prediction [22]. Participants were subsequently grouped into three classes, given they presented a low risk (score < 10%), a moderate risk (score 10–20%), or a high risk of CVD (score > 20%) [23].
Statistical analyses
Data were coded, entered, and analyzed using SPSS version 20.0 (IBM SPSS Inc., Chicago, Illinois, USA). Results are presented as frequency (percentage) for qualitative variables, and median (interquartile range (IQR)) for quantitative ones. Qualitative variable comparisons used the Chi-square test or Fisher exact test, and that of quantitative variables, the Mann–Whitney U test. The Spearman correlation test served to search for any relation between the CVR and other parameters, completed by univariable and multivariable linear regression analyses. We introduced in the multivariable model all variables with a p value <0.25 in univariable analyses, and used a backward selection process. Results were considered statistically significant if p < 0.05.
Results
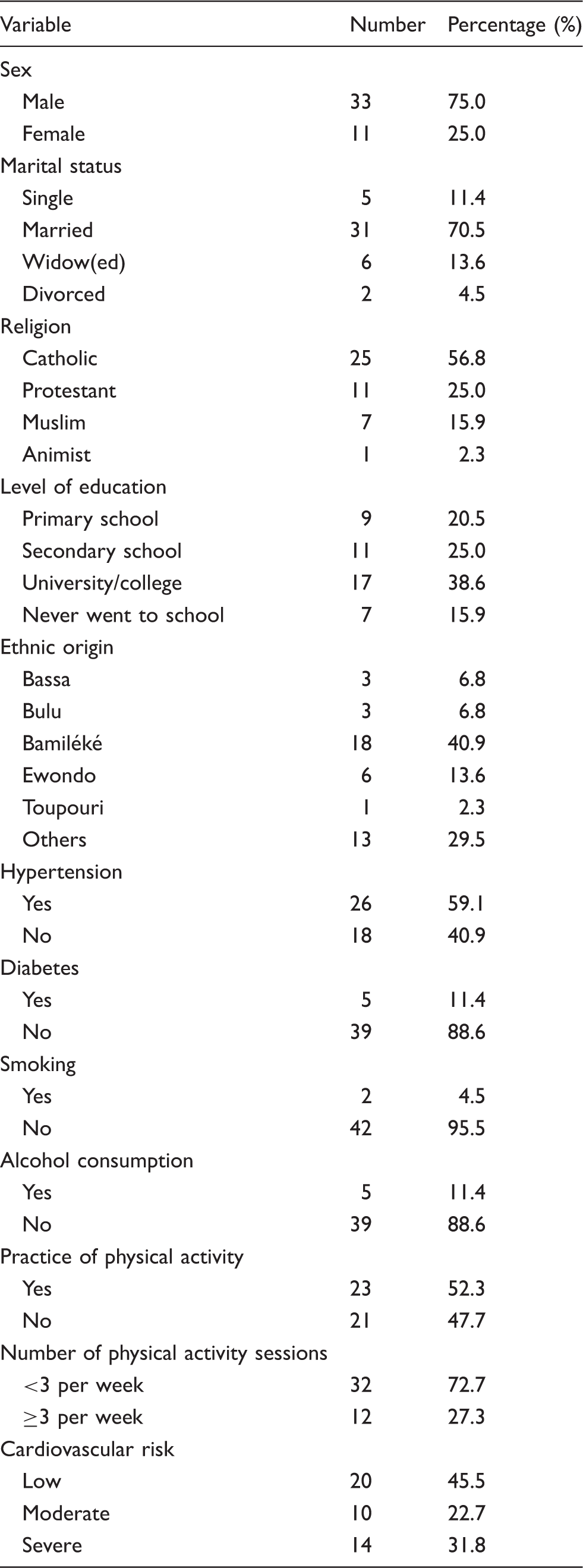
Characteristics of the study population.
Results of anthropometric and biochemical variables.

IQR: interquartile range; HDL: high-density lipoproteins; LDL: low-density lipoproteins; Max: maximum; Min: minimum.
We found 26 hypertensive patients (59.1%), 5 with DM (11.4%), and only two current smokers (4.5%). Twenty-three patients (52.3%) were practicing a regular physical activity, with only 12 (52.2%) having at least three sessions per week (Table 1). The number of sessions ranged from 0 to 7 with a median of 0.5 (0–3) sessions per week (Table 2). Median values of BMI, SBP, DBP, FPG, TC, LDL-C, HDL-C, TG, serum urea, serum creatinine, and GFR are presented in Table 2. The average duration on dialysis varied between 3 and 146 months with a median of 13 (6.3–64.5) months (Table 2). The CVR estimated by the FRS ranged from less than 1% to more than 30% with a median of 12.3% (4.9–24.4) (Table 2). Twenty dialyzed patients (45.5%) had a low risk of CVD, 10 (22.7%) a moderate risk, and 14 (31.8%) presented a high risk of CVD (Table 1).
Correlation between cardiovascular risk and other parameters.
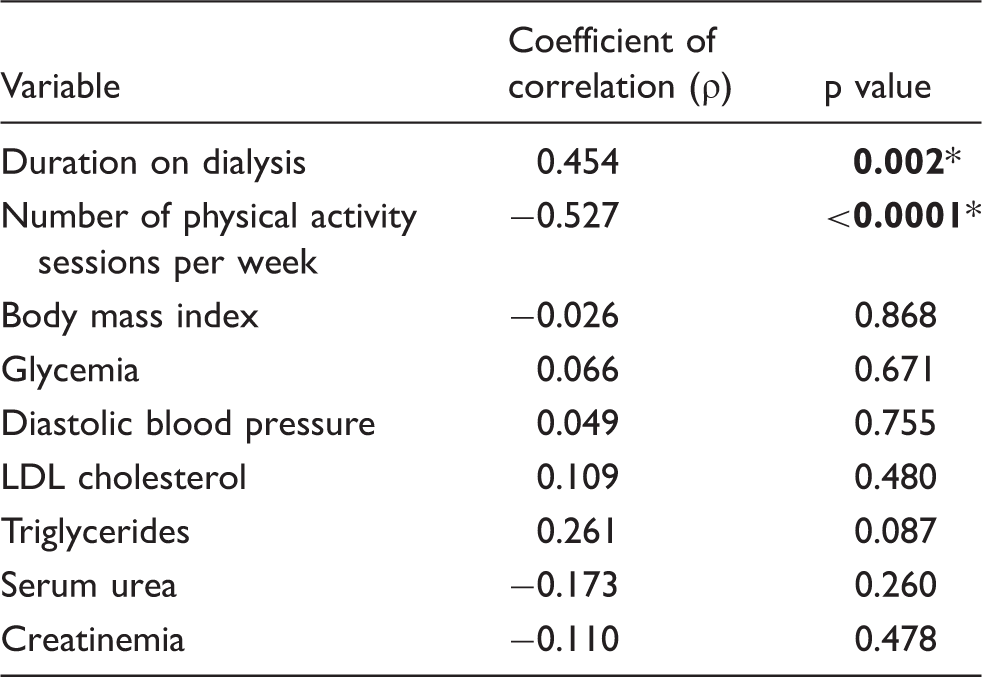
p value <0.05. Bold values in these tables represent those with a p value less than 0.05.
Univariable and multivariable linear regression analyses.
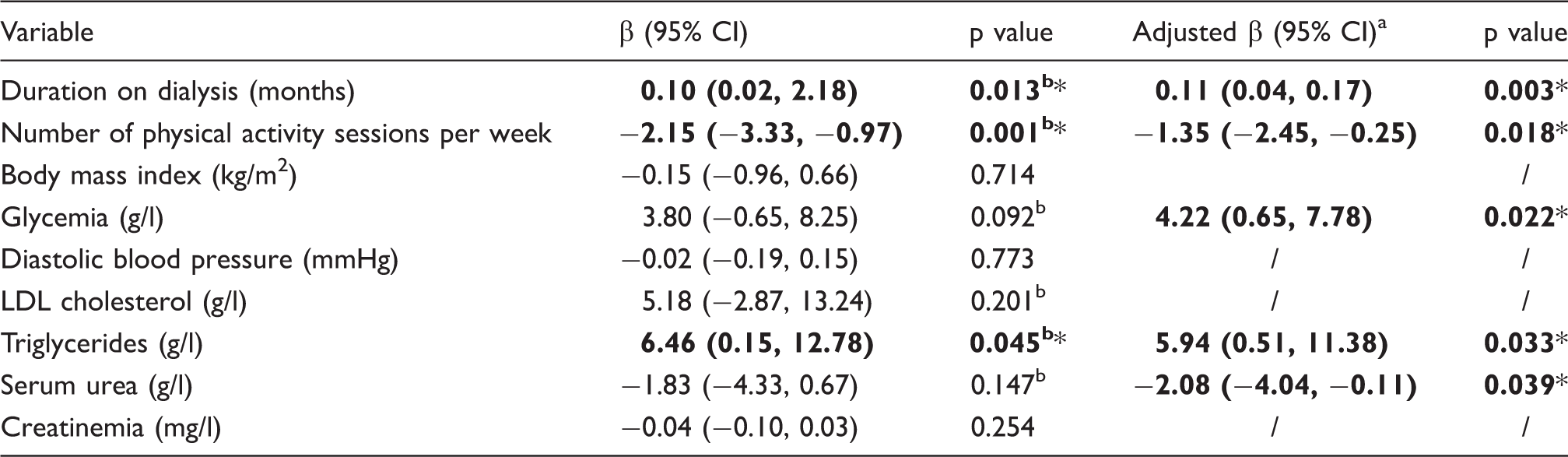
Using a backward selection process, LDL cholesterol was removed from the first model; here are presented results of the second (final) model, with R2 = 0.502, adjusted R2 = 0.441; p < 0.0001.
All these variables had a p < 0.25 in univariable analyses and were thus introduced in the initial multivariable model.
p < 0.05.
CI: confidence interval. Bold values are significant results, that is those with a p value less than 0.05.
Discussion
Our results showed 54.5% of the study population presenting a moderate or high risk of CVD. Besides, longer duration on dialysis, lower number of weekly physical activity sessions, higher levels of FPG, higher titers of serum TGs, and lower levels of serum urea before dialysis seemed to significantly increase dialyzed patients’ risk of CVD. Therefore, it can be inferred from these results that healthy lifestyle habits (healthy diet, regular physical activity) may substantially contribute in curtailing the current or future burden of CVD among our patients on HD.
The study design added to this small sample size precludes us from claiming that the factors we have raised are real independent risk factors significantly influencing our patients’ risk of CVD. Our response rate was low; the non-respondents claimed having been used to taking part in such studies, but have never received their results back before, justifying thus their anger and refusal to be enrolled anymore, despite all explanations and convincing attempts by the research team. We were incapable of increasing the sample size, being limited by financial constraints as the study benefited from no funding. Larger and better designed studies are warranted to better assess the global risk of CVD among HD patients and identify all associated risk factors in our context. In the absence of locally developed tools to assess the risk of CVD, we used the FRS which may lack to accurately assess the CVR in African populations as they may present different patterns of CVD as compared with Western countries [24]. Furthermore, the FRS was developed for the general population rather than for HD patients; therefore, it can underestimate the CVR. Moreover, the hospital-based and unique recruitment site natures of this study hinder perhaps the generalizability of our results to the entire HD population of the country.
Nonetheless and to the best of our knowledge, this is the first study in Cameroon and the Central-African Region dedicated to assessing the risk of CVD in HD patients and related influencing factors. We used strong and rigorous statistical procedures to analyze our data. Our results give an insight into the picture of risk of CVD in Cameroonian HD patients, which could be translatable to other SSA countries; they constitute the starting point for further researches in the region and can be used to improve HD patients’ management.
This study showed that longer duration on dialysis is likely to augment the risk of CVD. Indeed, it was observed that each new month spent in dialysis could lead to a 0.11% increment in the risk of CVD. On the contrary and intriguingly, we found that a 1 g/l rise in the serum urea levels before dialysis would be accompanied by a 2.1% reduction in the risk of CVD, whereas we were expecting the inverse to occur. The small sample size of this study alongside its design could explain these results, though we need longitudinal data to better elucidate this point.
This study consolidates existing evidence that physical activity is a paramount contributor for CVD prevention. Indeed, we learn from this study that each one-increase in the number of physical activity sessions per week could result in a 1.35% reduction in the risk of CVD. People who are physically inactive have an incremental risk of all-cause mortality in comparison to those who have at least 150 min of moderate-intensity physical activity per week, or equivalent, as recommended by World Health Organization (WHO) [25]. Regrettably, SSA countries are currently going through an epidemiological transition, and rapid urbanization with decrease in physical activity levels or increase in sedentary lifestyle seems to play an important role in this transition [26–28]. It is therefore high time strong measures be taken by local Governments to promote physical activity in SSA.
This study confirms the influence of FPG levels on the risk of CVD [18,19,29]. There is body of evidence demonstrating that DM is a known risk factor for CVD. It has been shown indeed that those individuals with diabetes have a 2 - to 4-fold augmented risk of developing cardiovascular events than their counterparts of the same age and sex without diabetes [29]. Likewise, people with prediabetes, a precursor to DM also have an increased risk of developing CVD [30]. We believe that HD patients should be screened for prediabetes or DM and adequate measures taken to prevent progression to DM or delay the onset of DM complications.
Moreover, dyslipidemia, which is defined as elevated levels of serum TC and/or TGs, is a well-established traditional risk factor for atherosclerotic coronary artery disease in the general population and more so in patients with CKD [13]. In fact, findings from the present study indicate that each 1 g/l increment in serum TGs titers would lead to a 5.94% augmentation in the risk of CVD. Treatment of dyslipidemia with lipid-lowering medications is considered a plausible strategy for reducing CVD in dialysis patients, but this is not to be done on a systematic basis [13]. We need studies in SSA to underpin such a recommendation with strong local evidences.
Conclusion
Around 55% of our hemodialyzed study population presented a moderate or high risk of CVD. Duration on dialysis, number of physical activity sessions per week, FPG, serum TGs, and serum urea levels may impact our HD patients’ risk of CVD. Accordingly, they should be encouraged to adopt healthy lifestyles including healthy diets and the practice of a regular moderate-to-vigorous physical activity. Additionally, lipid-lowering medications could be discussed in case of dyslipidemia. Notwithstanding, we need further studies to better characterize the risk of CVD and influencing factors among SSA patients suffering from end-stage CKD and undergoing maintenance HD.
Footnotes
Acknowledgments
The authors are most grateful to all those who have voluntarily accepted to take part in this study. Additionally, they acknowledge all the personnel of the dialysis unit of the Yaoundé University Teaching Hospital as well as the Laboratory of Biochemistry for their help in collecting the data and performing biochemical assays. Doctor Sandra Ayuk Tatah is also to be thanked for having taken a substantial time to critically review and revise the manuscript. Data will be made available by the corresponding author upon request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
An ethical clearance was delivered by the Ethical Review Board of the Catholic University of Central Africa based in Yaoundé, Cameroon (Number 0132/2016), and an authorization was obtained from the administrative authorities of the Yaoundé University Teaching Hospital. We enrolled only people who volunteered to participate; they signed the consent form in this respect.
Guarantor
JRNN is the guarantor for this study.
Contributorship
VJAM, DBTA, JRNN, and FFK conceived and designed the study. DBTA and VJAM collected the data and performed the analyses. JRNN analyzed, interpreted the data and drafted the manuscript. VJAM, JRNN, DBTA, and FFK critically reviewed and revised the manuscript. All authors approved the final version of the manuscript.