
Abstract
Introduction:
Venous stenosis or occlusion related to an intracardiac device is a well-known complication of that procedure. There are numerous studies tried to determine predictors of venous stenosis or occlusion; however, most of them investigate the venous system prior to device upgrade, generator replacement, or transvenous lead extraction. Therefore, we aimed to assess the prevalence and determine the predictors of venous stenosis or occlusion following first transevnous cardiac device implantation.
Methods:
Observational, prospective study included 71 consecutive patients admitted for first transvenous cardiac device implantation. All patients were followed up for 6 months after operation.
Results:
Implanted device systems comprised cardioverter defibrillator (n = 26), single-chamber or dual-chamber pacemakers (n = 34), and biventricular pacemakers (n = 11); 88.5% of implantable cardioverter defibrillator leads were single-coils and 11.5% were dual-coils. The incidence of venous stenosis or occlusion within 6-month follow-up was 21.1%. Multivariate logistic regression showed that only diabetes or prediabetes (p = 0.033, odds ratio: 0.17, 95% confidence interval: 0.04–0.87), prolonged procedure time (p = 0.046, odds ratio: 4.54, 95% confidence interval: 1.01–20.12), and perioperative complications (p = 0.021, odds ratio: 7.04, 95% confidence interval: 1.35–36.85) were predictors of venous stenosis or occlusion.
Conclusion:
Prolonged implantation time (>60 min) and perioperative complications are associated with an increased risk of venous stenosis or occlusion, whereas diabetes and prediabetes significantly reduce the risk of venous stenosis or occlusion.
Keywords
Introduction
The number of pacemakers (PM) and implantable cardioverter defibrillators (ICD) implanted in the Europe and worldwide continues to increase. 1 In 2014 alone, the mean PM and ICD implantation rate in the participating European Society of Cardiology (ESC) countries was 605 units per million inhabitants. 2 Venous stenosis or occlusion (VSO) related to an intracardiac device is a well-known complication of that procedure. 3 The unobstructed contact of transvenous leads with the vein endothelium plays a major role in the pathophysiology of this phenomenon, which subsequently results in permanent inflammation, lead endothelialization, narrowing of the vessel and, in severe cases, complete vein occlusion.4–6 These obstructions are commonly asymptomatic due to venous collateral formation7–9 but can also lead to symptoms such as ipsilateral arm edema, parasthesia, and pain. Various management strategies have been employed, including anticoagulation, lead extraction, percutaneous venoplasty with or without stenting, and surgical bypass.6,10,11 However, no consensus regarding the optimal treatment of this problem exists.
There are numerous studies tried to determine predictors of VSO; however, most of them investigate the venous system prior to device upgrade, generator replacement, or transvenous lead extraction.3,6,12–14 Therefore, we aimed to assess the prevalence and determine the predictors of VSO following first transvenous cardiac device implantation.
Methods
Observational, prospective study included 71 consecutive patients admitted for the first transvenous cardiac device implantation. Patients who had undergone VSO in the past were excluded from the analysis. Subclavian vein puncture technique was used for lead insertion in 46 patients and cephalic vein cutdown in 42 patients. All procedures were ultrasound-guided using an 8 MHz micro-convex ultrasound probe (Philips Healthcare, Andover, MA). There were 56 Silicone Rubber insulated leads, 21 co-polymer silicone- polyurethane (Optim) and 1 with polyurethane insulation. The study was approved by the local Ethics Committee, and written informed consent was obtained from all the patients.
Prior to the operation and 6 month after cardiac device implantation, a Doppler ultrasonography of the ipsilateral access vein was performed by experienced echocardiographers (all certified with the second degree accreditation in echocardiography of the Echocardiography Working Group of the Polish Cardiac Society) who regularly place ultrasound-guided central venous catheters. Variables examined for association with VSO are shown in Tables 1 and 2. Perioperative complications included pneumothorax, hemothorax, subcutaneous emphysema, and lead dislodgment.
Baseline clinical characteristic, antiplatelet therapy and anticoagulation of the study subjects by presence of endpoint.
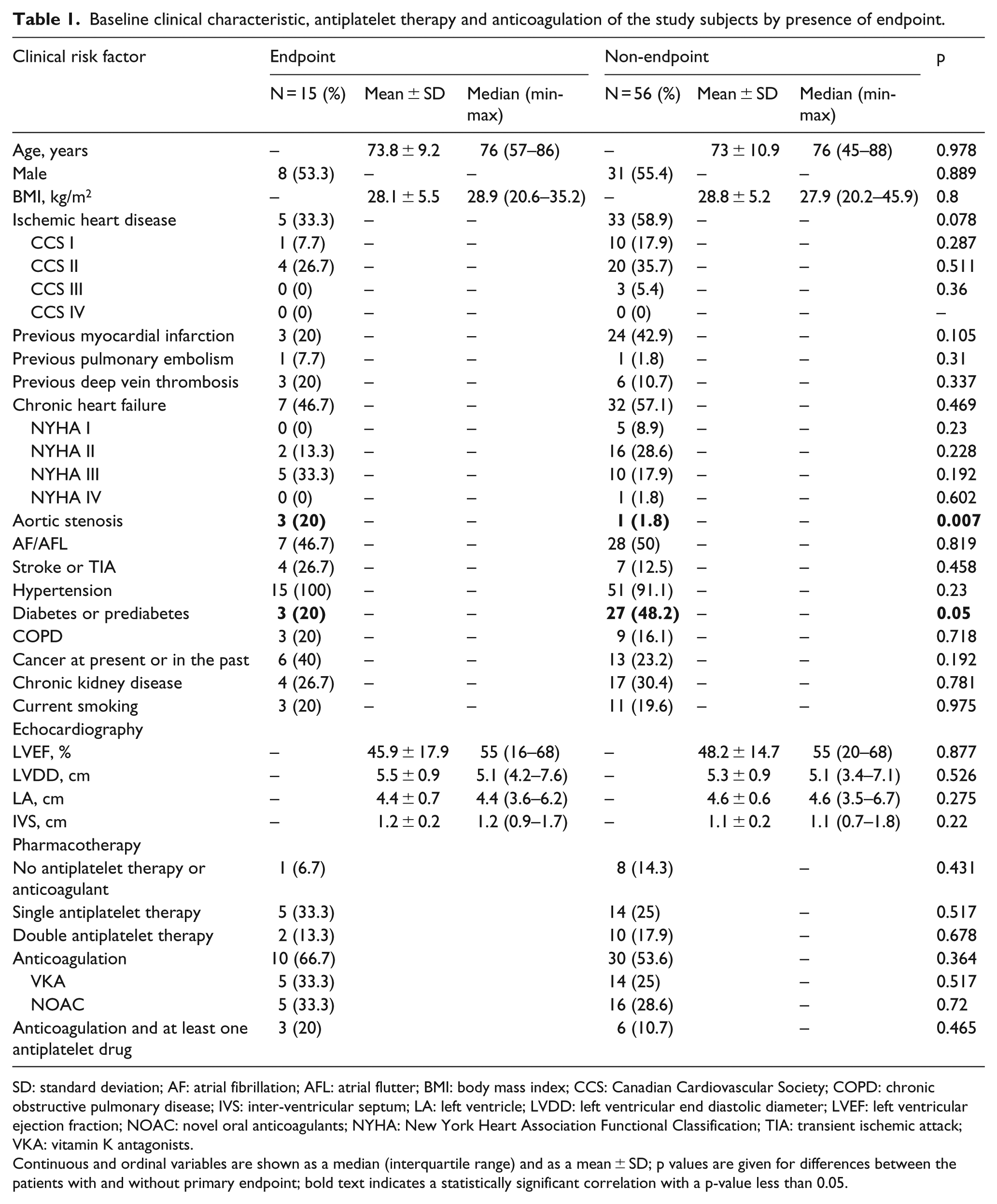
SD: standard deviation; AF: atrial fibrillation; AFL: atrial flutter; BMI: body mass index; CCS: Canadian Cardiovascular Society; COPD: chronic obstructive pulmonary disease; IVS: inter-ventricular septum; LA: left ventricle; LVDD: left ventricular end diastolic diameter; LVEF: left ventricular ejection fraction; NOAC: novel oral anticoagulants; NYHA: New York Heart Association Functional Classification; TIA: transient ischemic attack; VKA: vitamin K antagonists.
Continuous and ordinal variables are shown as a median (interquartile range) and as a mean ± SD; p values are given for differences between the patients with and without primary endpoint; bold text indicates a statistically significant correlation with a p-value less than 0.05.
Risk factors associated with cardiac device implantation procedure in groups of patients with and without endpoint.
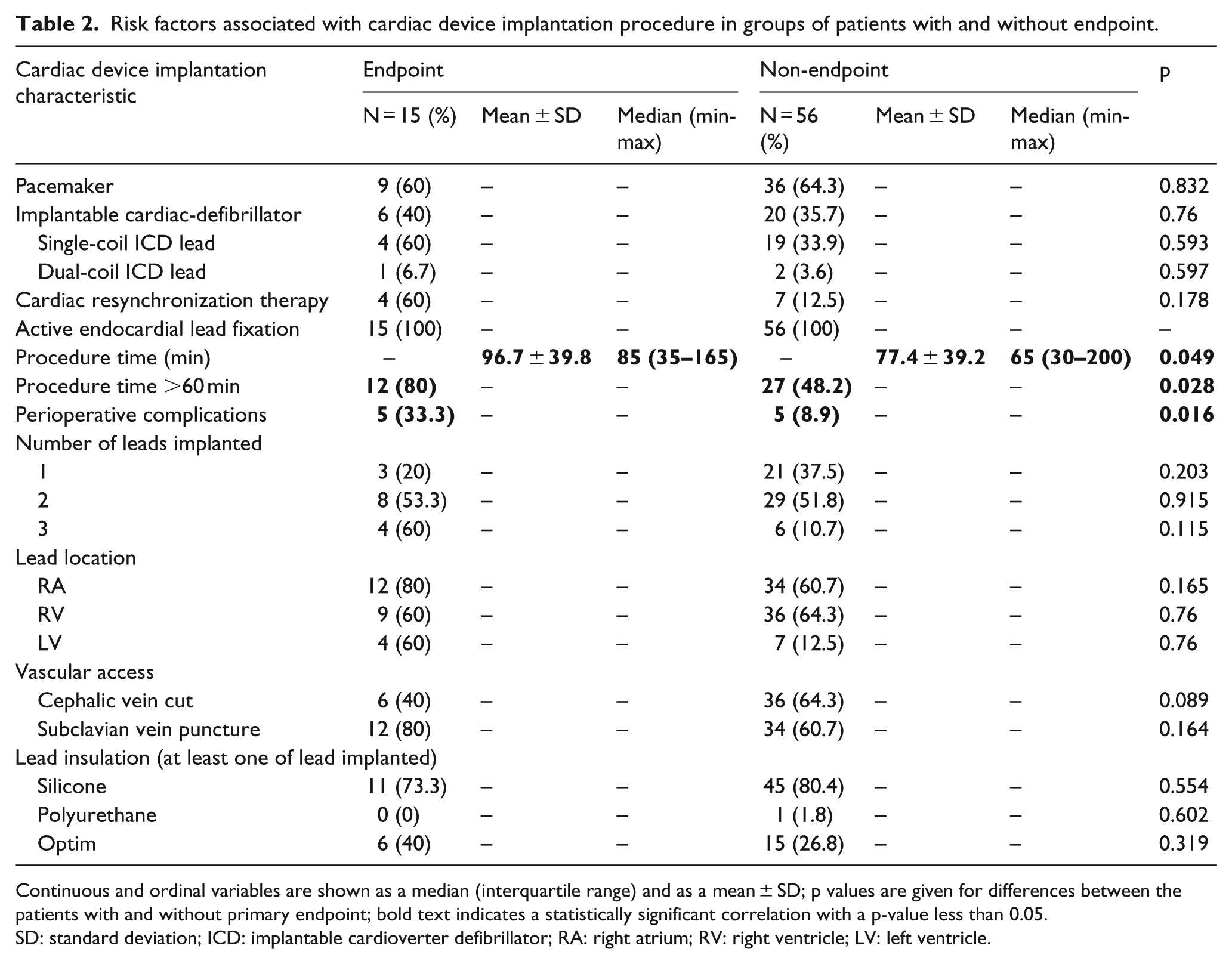
Continuous and ordinal variables are shown as a median (interquartile range) and as a mean ± SD; p values are given for differences between the patients with and without primary endpoint; bold text indicates a statistically significant correlation with a p-value less than 0.05.
SD: standard deviation; ICD: implantable cardioverter defibrillator; RA: right atrium; RV: right ventricle; LV: left ventricle.
The primary endpoint in this study was device-related VSO defined as a greater than 50% luminal narrowing. For veins accessible to direct insonation, the criteria of noncompressibility, visualization of echogenic intravascular mass, and absence of respiratory variation were used (subclavian vein). For veins inaccessible to direct insonation, the criterion of monophasic flow at the stenosis site with no retrograde wave or no color signal or flow in the vessel lumen was used (middle part of subclavian, brachiocephalic vein) to detect VSO.15,16
The diabetes mellitus was diagnosed based on American Diabetes Association guidelines 17 by demonstrating any one of the following:
Fasting plasma glucose level ⩾7.0 mmol/L (126 mg/dL);
Plasma glucose ⩾11.1 mmol/L (200 mg/dL) 2 h after a 75 g oral glucose load as in a glucose tolerance test;
Casual plasma glucose ⩾11.1 mmol/L (200 mg/dL) with symptoms of high blood sugar.
Continuous variables are expressed as mean ± SD and median (minimal and maximal value). Categorical variables are presented as an exact number and percentage of the whole analyzed group. Differences between two groups for continuous variables were tested by the Mann–Whitney U-test. The comparisons of categorical variables were analyzed using χ2 independence test. Two-way tables were assessed with the χ2 test with Yates correction. Multivariate logistic regression analysis was performed to determine predictors of VSO by entering all predictors with p values <0.1 in univariate analysis into a forward stepwise model (Table 3). Spearman’s rank correlation coefficient was used to discover the strength of a link between two sets of data to exclude factors significantly correlated. A p value <0.05 was defined as statistically significant.
Multivariate logistic regression model predicting venous stenosis or occlusion.
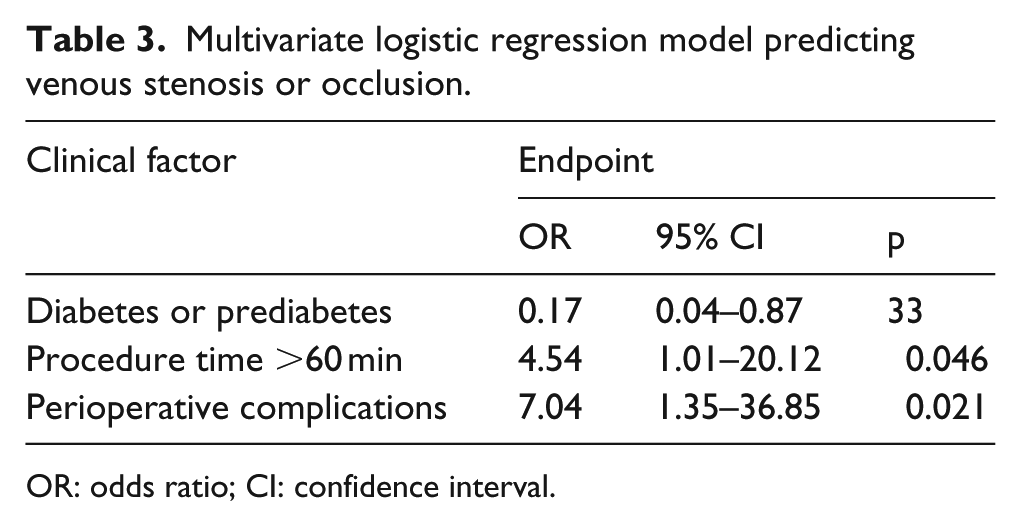
OR: odds ratio; CI: confidence interval.
Results
A total of 71 patients (39 men; mean age 73.8 ± 9.2 years in patients with VSO, 73 ± 10.9 years in patients without VSO) were included in this study. Detailed patient characteristics are summarized in Table 1. Implanted device systems comprised cardioverter defibrillator (n = 26), single-chamber or dual-chamber PM (n = 34), and biventricular pacemakers (n = 11); 88.5% of ICD leads were single-coils and 11.5% were dual-coils. The incidence of VSO within 6-month follow-up was 21.1%.
Patients with VSO more often had aortic stenosis, prolonged procedure time (>60 min) and perioperative complications than patients without VSO (0.007, 0.028, and 0.016, respectively). Diabetes or prediabetes was observed among 3 (20%) patients with VSO and 27 (48.2%) patients without VSO (p = 0.049). There were no differences in anticoagulation or antiplatelet treatment between both groups.
Multivariate logistic regression showed that only diabetes or prediabetes (p = 0.033, OR: 0.17, 95% confidence interval (CI): 0.04–0.87), prolonged procedure time (p = 0.046, OR: 4.54, 95% CI: 1.01–20.12), and perioperative complications (p = 0.021, OR: 7.04, 95% CI: 1.35–36.85) were predictors of VSO. The area under the curve (AUC) statistic for model comparison was significantly (0.889) with sensitivity of 80% and specificity of 69.6% (Figure 1).
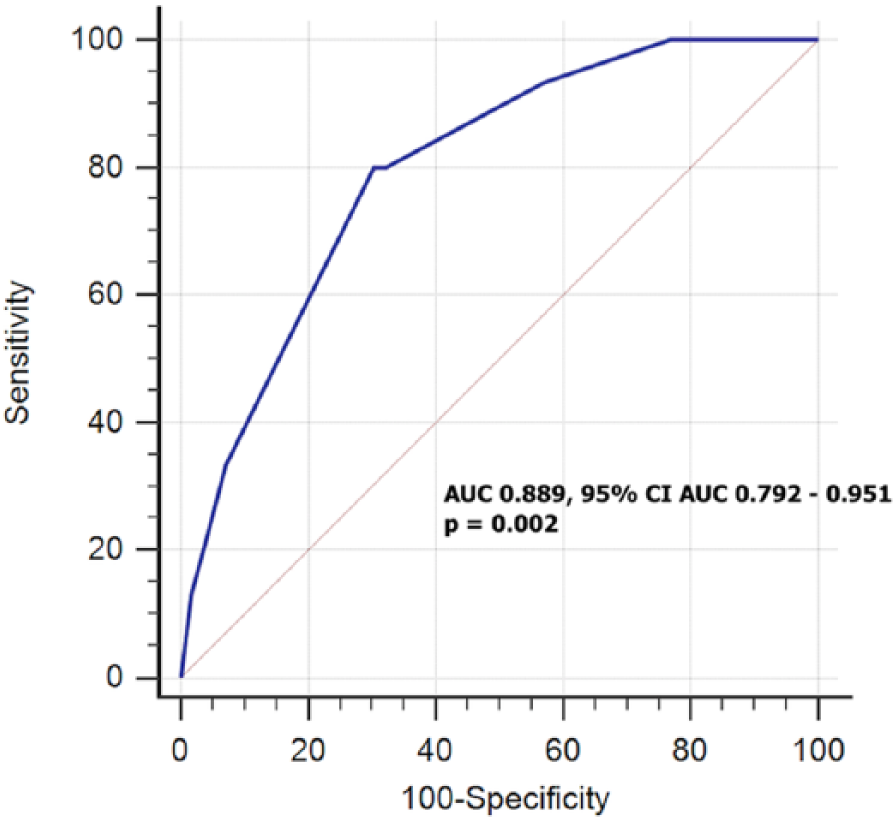
Receiver operating characteristic curve for multivariate logistic regression model predicting venous stenosis or occlusion.
Discussion
Considering the prevalence of VSO among patients undergoing first cardiac device implantation, we must take into consideration (1) the utilized venous visualization method and (2) the definition of venous stenosis/occlusion. The assessment of vein patency is most often performed by contrast venography, which is considered the gold standard. 6 However, there exist other equally alternative methods such as venous Doppler ultrasound with sensitivity and specificity over 90%.18,19
In the present study VSO was detected in 21.2% of patients. The previous studies reported similar incidence of that complication except for few authors who identified VSO in higher percentage of patients from 37.5% to 64%.8,19,20 The substantial differences among authors depend more on the criteria which were used to define VSO in the presence of endocardial leads rather than the lead dwell time or method of venous visualization.
The association of venous stenosis and the number of leads has also been an area of controversy. Goto et al., 7 Oginosawa et al., 12 and Bracke et al. 14 found no association between venous stenosis and the number of leads present. Our results are consistent with their results. However, other investigators disagreed with this finding. Van Rooden et al., 18 Haghjoo et al., 11 and Bulur et al. 21 found a significant association between venous stenosis and having multiple leads in their series.
The most important result of our study is the protective value of diabetes or prediabetes against the development of VSO. Such an observation has been reported in the Boczar et al. study. In patients with endocardial leads, diabetes was proved in multivariate analysis to be the only protective factor against the development of VSO (OR = 0.473; p = 0.010). 20
Implantation of leads triggers a series of host reactions at the injury site that include acute and chronic inflammation, granulation tissue development, and fibrous capsule formation. However, adverse foreign body reaction that invariably occurs adjacent to implant devices is poorly characterized in the diabetic environment. Socarrás et al. investigated the influence of this condition on the abnormal tissue healing response in polyether–polyurethane implants placed subcutaneously in normoglycemic and streptozotocin-induced diabetes in rats. Implants removed 10 days after implantation were assessed by determining the components of the fibrovascular tissue (angiogenesis, inflammation, and fibrogenesis). In implants from diabetic rats, fibrous capsule thickness and fibrovascular tissue infiltration were reduced in comparison with implants from non-diabetic rats. However, the number of vessels in the fibrovascular tissue from diabetic rats was decreased when compared with vessel numbers in implants from non-diabetic animals. Overall, all inflammatory parameters, that is, macrophage accumulation-N-acetyl-β-D-glucosaminidase (NAG) activity, tumor necrosis factor (TNF)-α, and monocyte chemotactic protein (MCP)-1 levels, increased in intraperitoneal implants after diabetes induction as well as profibrogenic cytokine transforming growth factor β1 (TGFβ-1) level. 22 In consequence, diabetes affects the cellular response to tissue injury and delays wound healing. We assume that these effects may contribute to a decreased risk of venous stenosis in patients with indwelling endocardial leads. Undoubtedly, this phenomenon requires further investigation. 23
To the best of our knowledge, our study is the first to investigate the multivariable prediction model for VSO. The risk factors included in that model may increase the power of identification of high-risk patients with VSO.
The presented study is single-center and nonrandomized. Its limitation is the narrow size of the assessed population. That is why we did not distinguish prediabetes and diabetes, to increase their predictive value of VSO. Nevertheless, previous studies on VSO in the presence of endocardial leads were conducted in a comparable number of patients and without control group. Moreover, our study population is homogeneous as all of patients underwent their first cardiac device implantation and were assessed exactly at 6 months postoperatively. Another limitation of our study is single image approach to diagnose VSO. However, color Doppler ultrasonography as a non-invasive method is characterized by high sensitivity (80%) and a specificity (90%–100%) for detecting VSO.18,19 Moreover, we have no collected data regarding complications details and their relation to procedure time, as well as type of vein of what trauma occurred. The extended procedure time was not associated with intraprocedural complications, but with technical problems such as difficulty in the preparation of the cephalic vein, subclavian vein puncture, searching for better electrical stimulation parameters, poor cooperation of the patient. With extended procedure time, the risk of vein trauma increases and may influence on patients’ prognosis in terms of the VSO. Another limitation is the fact that no attempt was done to study the ratio between the caliber of the vein and the caliber of the device inserted. In conclusion, prolonged implantation time exceeded 60 min and perioperative complications are associated with an increased risk of VSO, whereas diabetes and prediabetes reduce the risk of VSO.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by scientific grant of Polish Cardiac Society.