
Abstract
Introduction:
Radiolucent lines occasionally develop around the proximal aspect of fully hydroxyapatite (HA)-coated tapered femoral stems after total hip arthroplasty (THA). It was hypothesised that distal wedging of stems may predispose to proximal radiolucent line formation, which may negatively impact clinical outcome.
Methods:
All primary THA performed with a collarless fully HA-coated stem that had a minimum of 1 year of radiographic follow-up were identified in a surgical database (n = 244). Radiographic measures of proximal femoral morphology and femoral canal fill at the middle and distal thirds of the stem were analysed for association with the presence of proximal radiolucent lines. Linear regression was used to explore any association between radiolucent lines and patient reported outcome measures (PROMs), available in 61% of patients.
Results:
Proximal radiolucent lines developed in 31 cases (12.7%) at final follow-up. Dorr A femoral morphology and increased canal-fill at the distal ⅓ of the stem correlated with the development of radiolucent lines (p < 0.001). No correlation was observed between pain or PROMs and the presence of proximal radiolucent lines.
Discussion:
We observed an unexpectedly high incidence of proximal femoral radiolucent lines about collarless fully HA coated stems. Distal-only implant wedging in Dorr A bone may compromise proximal fixation. Although this finding did not correlate with short-term outcomes, the long-term clinical impact requires further study.
Introduction
Biologic fixation without cement in total hip arthroplasty (THA) requires mechanical stability of the interface between viable host bone and the implant surface. 1 Once osseointegration occurs, cementless femoral fixation has proven durable. 2 Among the various materials and surface treatments available to promote osseointegration, hydroxyapatite coating applied by plasma spray has been extensively used and excellent clinical outcomes have been reported.3–7 Hydroxyapatite (HA)-coated titanium tapered wedge stem designs are available in proximally coated and fully coated configurations.8,9 Both designs have advocates and excellent published outcomes in the majority of patients. 10
In a fraction of patients, however, mismatch between implant and bone geometry results in distal wedging and inadequate proximal contact between implant and cortical bone. Despite achieving initial implant stability, these stems are vulnerable to proximal micromotion. Prior research has shown that osseointegration of proximally HA-coated implants may fail when distal wedging occurs and the coated proximal portion of the implant lacks cortical support.3,11 Failure of osseointegration can produce thigh pain and result in early revision. Modern proximally HA-coated implants have been redesigned to reduce the incidence of this phenomenon. 12 Nevertheless, it may not be possible to design a single implant profile that will reliably avoid distal-only wedging in Dorr Type A anatomy and yet reliably achieve sufficient distal support in Dorr Type C anatomy. 13
Theoretically, fully HA-coated tapered stems may protect against this mode of fixation failure. However, it has not been demonstrated whether the stability achieved by distal wedging of fully HA-coated tapered stems is sufficient to reliably promote osseointegration and achieve durable fixation. 9
Proximal radiolucent lines (RLL) have been demonstrated to develop around a subset of fully-HA coated tapered stems. 14 While these interface demarcations imply a lack of proximal osseointegration, distal osseointegration may be present. Indeed, we have observed this finding to develop during one year after implantation in patients with and without associated hip or thigh complaints. It is nevertheless possible that isolated distal osseointegration of fully HA-coated tapered femoral implants might predispose to thigh pain or even potentially late stem fracture, which has been reported with distal fixation of cylindrical stems. 15
In the current investigation, we retrospectively reviewed a cohort of patients receiving fully HA-coated, tapered wedge, collarless stems in order to ascertain: (1) the prevalence of proximal radiolucent lines; (2) demographic and anatomic factors contributing to occurrence of this radiographic finding; and (3) any association with patient-reported outcome measures (PROMs) or hip area pain. It was hypothesised that distal wedging of stems may predispose to proximal radiolucent line formation, which may negatively impact clinical outcome.
Materials and methods
Following Institutional Review Board (IRB) ethics review and approval, all primary THA performed by 3 surgeons at a single institution from 2010 to 2015 were identified using an administrative database (n = 1775). All cases performed with a collarless fully HA-coated, single taper wedge stem were reviewed (n = 546). THAs performed for proximal femur fracture were excluded (n = 73), leaving 473 elective primary THAs. We excluded 6 cases known to have undergone femoral component removal <1 year after implantation, including 4 for prosthetic joint infection and 2 for periprosthetic femur fracture. We further excluded cases with <1-year radiographic follow-up (n = 223). This left 244 fully HA-coated femoral components in 195 patients with minimum 1-year radiographic follow-up. Mean follow-up for these cases was 2 years (range 1–6 years).
Hospital records were reviewed to collect patient age, gender, BMI, diagnosis, laterality, surgical approach, and femoral stem type (with numerical size). The study population was 63% male with a mean body mass index (BMI) of 28.4 kg/m2 (Table 1). Osteoarthritis was the diagnosis in 95% of cases. A direct anterior approach was used for 73% of cases, while a posterior approach was used in 27%.
Demographics and surgical approach.
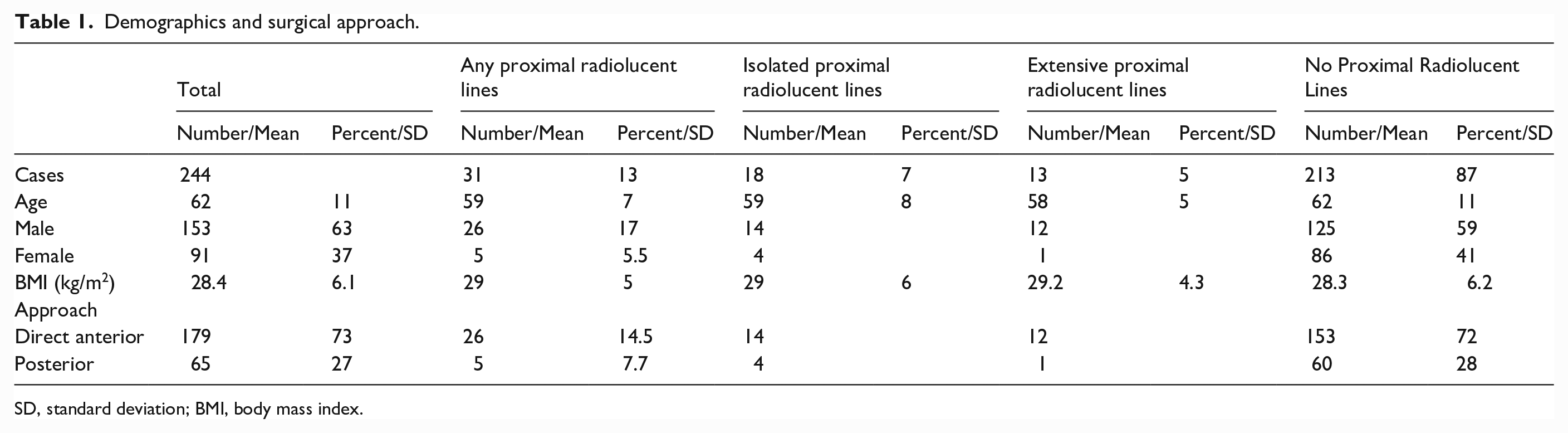
SD, standard deviation; BMI, body mass index.
Femoral implants
A wide variety of femoral implants from diverse manufacturers were utilised during the study period. The following fully HA-coated implants were included in this analysis: Metafix (Corin Group, Cirencester, UK; n = 76), Corail (DePuy Synthes, Raynham, MA, USA; n = 67), Novation Element (Exactech, Inc., Gainesville, FL, USA; n = 41), AMIS (Medacta International, Castel San Pietro, Switzerland; n = 39), and Avenir (Zimmer Biomet, Warsaw, IN, USA; n = 21).
Perioperative protocol
Posterior THAs were instructed to follow traditional hip precautions for 6 weeks after surgery, whereas no positional restrictions were placed on direct anterior THAs. With the exception of this difference between approaches, all procedures followed standardised operative and postoperative protocol. Mobilisation with physical therapy was performed within 24 hours after surgery and weight-bearing was allowed as tolerated with use of crutches or walker as needed and ambulation was progressed based on patient comfort.
Radiographic assessment
In-office x-rays were routinely obtained at 2 weeks, 6 weeks, 6 months, 1 year, 2 years and 5 years postoperative. Hips with minimum 1-year radiographic follow-up (n = 244) underwent radiographic analysis on the Picture Archiving and Communication System (PACS) at our institution (Synapse; Fujifilm Medical Systems, Stamford, CT, USA). Morphometric information regarding each host femur was obtained from preoperative radiographs as described by Cooper et al. 3 Proximal femoral bone morphometry measurements were calculated including morphological cortical index (MCI), canal bone ratio (CBR), canal calcar ratio (CCR) and canal flare index (CFI) (Figure 1).16–19 Increased MCI, increased CFI, and decreased CCR all indicate a smaller diameter canal relative to the femoral metaphysis, consistent with Dorr A femoral morphology. Increased CBR indicates thicker diaphyseal cortex relative to the femoral canal, also typical of Dorr A morphology.The first high-quality postoperative office radiograph was reviewed for “canal fill” at the middle and distal thirds of the stem. Canal fill was calculated by dividing the diameter of the stem by the endosteal diameter of the femoral canal at the midportion of each measured segment.
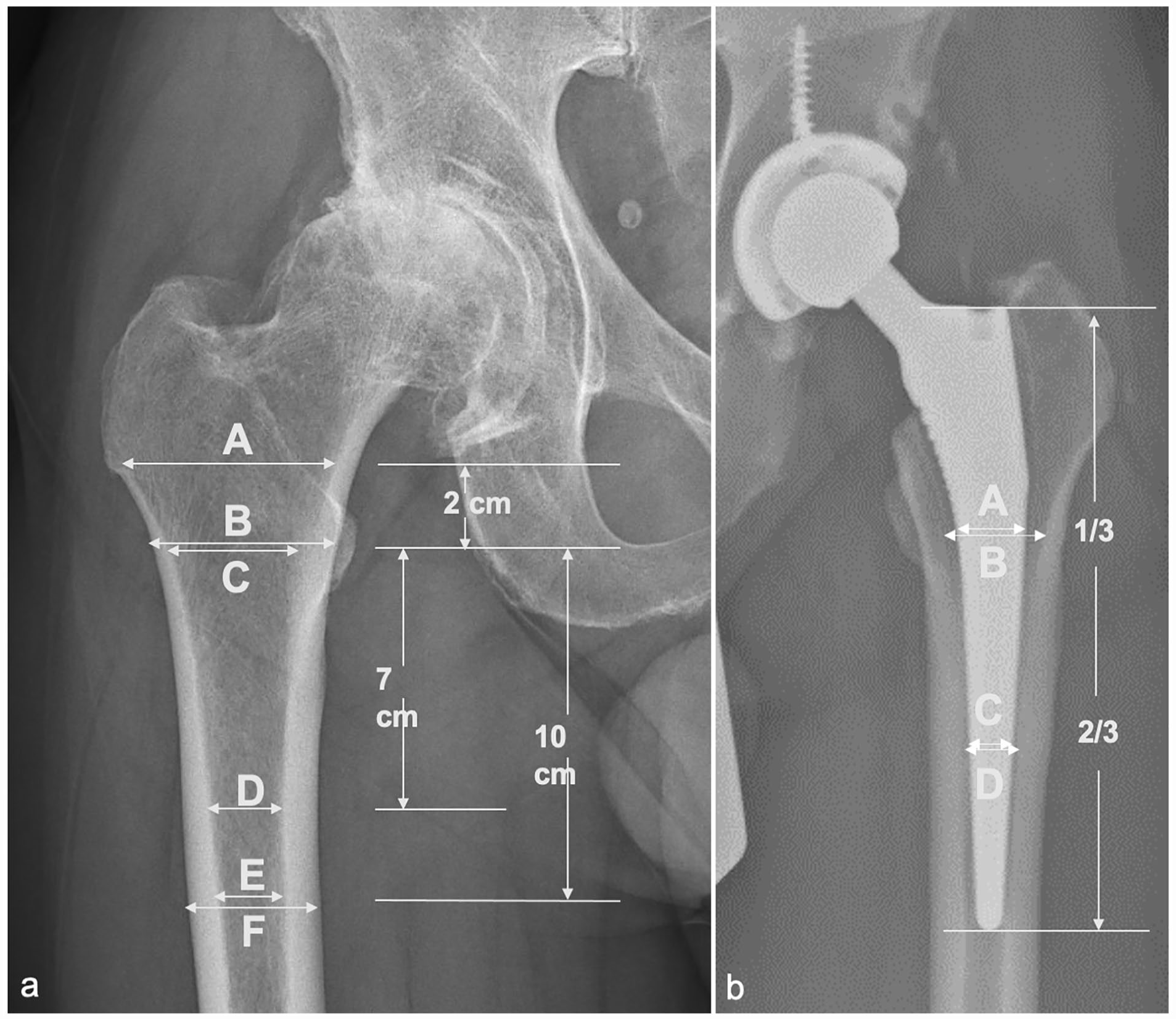
(a) Radiographic parameters for proximal femoral morphometry. Canal calcar ratio (CCR) = E/C; canal flare index (CFI) = A/E; morphological cortical index (MCI) = B/D; canal bone ratio (CBR) = E/F. (b) Femoral stem canal fill. Femoral stem canal fill at the middle ⅓ of the stem (A/B) and at the distal ⅓ of the stem (C/D).
The most recent available radiographs, performed at least one year postoperatively, were also inspected for the presence of RLLs at the femoral implant-bone interface. Radiolucent lines were characterised by location according to the 14 Gruen zones on antero-posterior and lateral radiographs (Figure 2). Patients with RLLs spanning one or more of the proximal Gruen zones (1,7,8 or 14) formed the first outcome group, labeled “any proximal lucency”. Radiolucent lines that spanned only 1 or 2 proximal Gruen zones (1,7,8 or 14) were considered “isolated proximal” femoral radiolucent lines. 3 Radiolucent lines affecting 3 or 4 proximal Gruen zones and those extending into the proximal half of Gruen zones 2, 6, 9 or 13 were classified as “extensive proximal.” We also looked for RLLs that were distal only, both proximal and distal, or circumferential.
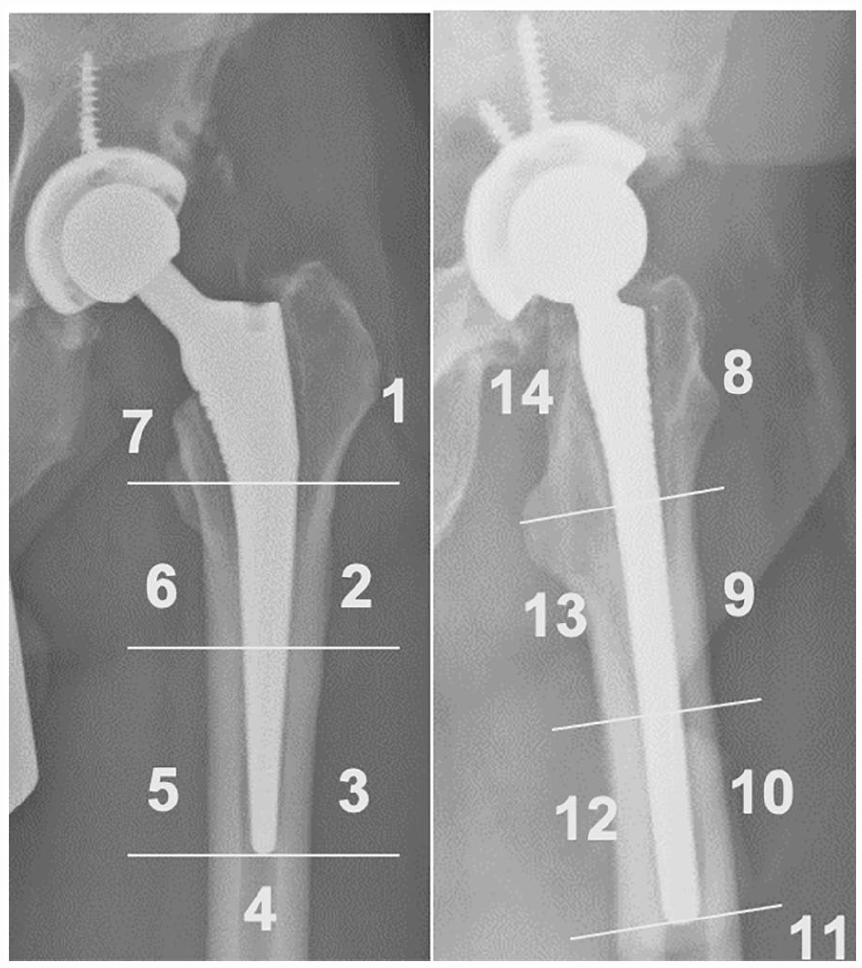
The location of radiolucent lines was described using the 14 Gruen Zones. Radiolucent lines affecting Gruen Zone 1,7,8, or 14 were considered proximal femoral radiolucent lines.
A subset of 20 radiographs were read by 2 reviewers ZPB, MUJ. Intraclass correlation coefficient (ICC) for measurements of stem fill was 0.72 and kappa value for identification of radiolucent lines was 1.0. This was considered acceptable agreement between the 2 observers, so the remainder of the radiographs were divided for analysis.
Clinical assessment
Patient-reported outcome measures (PROMs) were collected utilising an online patient education and engagement platform designed to support rehabilitation [FORCE Therapeutics, New York, NY]. PROMs included Hip Disability and Osteoarthritis Outcome Score for Joint Replacement (HOOS Jr.), Veteran’s RAND 12-Item Health Survey (VR-12) both physical and mental component scores (PCS, MCS), and University of California at Los Angeles (UCLA) activity score.20–22 Using the online portal, patients were also asked if they had hip-area pain (defined as groin, thigh or side of hip pain), and asked to rate their level of pain from 0 to 10 at the current time, at its best, and at its worst. Surveys were completed at >1 year follow-up by 148 of the 244 patients with minimum 1-year radiographic follow-up, defining the study cohort for investigation of clinical outcomes in the setting of proximal radiolucent lines.
Statistical analysis
Univariable logistic regression was performed for the outcomes of: (1) any proximal radiolucent line; (2) isolated proximal; and (3) extensive proximal radiolucent lines. Predictor variables were age, gender, BMI, surgical approach, measures of femoral morphology (MCI, CBR, CCR, CFI), and canal fill at the middle and distal thirds of the stem, along with the brand of femoral stem. We also compared canal-fill between cases performed with anterior and posterior approaches. Multi-variable regression was performed using a stepwise-backward method for the largest outcome group – patients with any proximal radiolucency given sufficient number within this subgroup.
Univariable linear regression was performed for each PROM (HOOS Jr., VR-12 PCS, VR-12 MCS, and UCLA activity score) with any, isolated or extensive proximal femoral radiolucent lines as predictor variables.
Results
7 of the 473 elective THAs are known to have undergone femoral revision (1.5%). 6 of these patients with early femoral implant removal prior to 1-year follow-up were excluded from radiographic and clinical analysis; 2 were revised for early periprosthetic femoral fracture (1 patient at 94 days and 1 at 47 days) and 4 were revised for infection within the first year. There was 1 femoral revision >1 year after surgery. The patient had radiolucent lines in all 4 proximal Gruen zones but none in the distal Gruen zones at 1.4-year follow-up. It was later determined that this patient was revised at an outside hospital. The indication for surgery, date of revision and surgical findings are not known. 2 cases had re-operations for infection but retained their femoral components, and three had re-operations for recurrent dislocation but retained their femoral components. The total re-operation rate was 2.5%.
Of the 244 cases with minimum 1 year follow-up who underwent radiographic review, 31 (12.7%) had proximal femoral interface radiolucent lines (Table 1). 18 cases (7.4%) had isolated proximal radiolucent lines affecting 1 or 2 proximal Gruen zones: 10 in zone 1, 1 in zone 7, 11 in zone 8, and 6 in zone 14 (Supplelmental Table 1). 13 (5.3%) had extensive proximal radiolucent lines affecting 3 or 4 Gruen proximal zones (Supplemental Table 1). Of the 13 cases with extensive proximal radiolucent lines, 7 had extension int o the proximal portion of the middle Gruen zones, most commonly Gruen Zone 2 (n = 5). All radiolucent lines were confined to the proximal half of the prostheses. There were no distal radiolucent lines and no cases had circumferential radiolucent lines. Mean radiographic follow-up was 2 years (standard deviation [SD] 1.1 years).
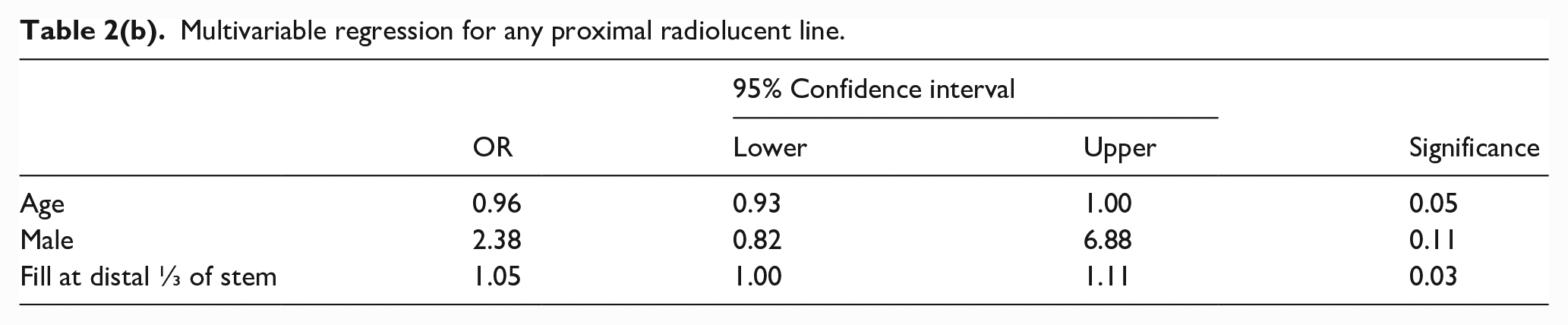
The association between patient demographics and the occurrence of RLLs was also explored. Younger age approached a significant association with the development of any proximal radiolucent lines (odds ratio [OR] 0.97, p = 0.06) (Table 2(a) and 2(b)). On univariable testing, male sex associated with the incidence of any proximal radiolucent lines (OR 3.85, p = 0.01) (Table 2(a)). Surgical approach did not significantly associate with the development of proximal radiolucent lines (any, isolated, or extensive) (Table 2(a) and Supplemental Material Tables 2 and 3, respectively), although non-significant trends were noted for higher rates of proximal radiolucent lines (OR 2.04, p = 0.16) and extensive proximal radiolucent lines (OR 4.60, p = 0.15) with the anterior approach.
Univariable regression for any proximal radiolucent line.
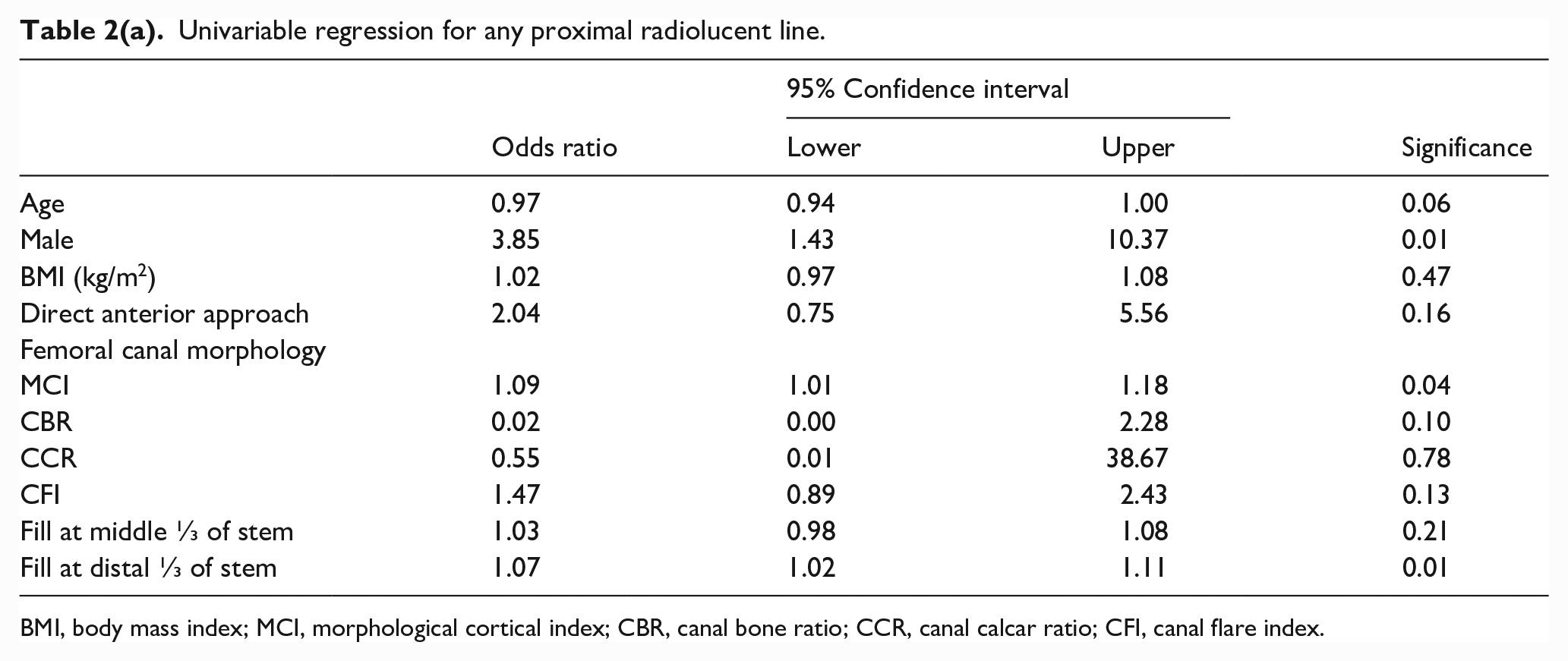
BMI, body mass index; MCI, morphological cortical index; CBR, canal bone ratio; CCR, canal calcar ratio; CFI, canal flare index.
Multivariable regression for any proximal radiolucent line.
Measurements of bone morphology in patients with and without proximal radiolucent lines are demonstrated in Supplemental Table 4. Morphological cortical index (mean 3, SD 0.5) and canal flare index (mean 4.2, SD 0.7) were greatest in patients with extensive proximal femoral radiolucent lines. Higher CFI demonstrated a statistically significant correlation with the presence of extensive proximal radiolucent lines (Supplemental Table 3). A higher MCI correlated with the presence of any proximal radiolucent lines (Table 2(a), p = 0.04).
Femoral canal fill at the distal third of the implant was greatest in patients with isolated proximal radiolucent lines (mean = 90.0% fill, SD 6.0%) and lowest in patients with no proximal radiolucent lines (mean 81.7%, SD 11.3%) (Supplemental Table 4). Increasing canal fill at the distal ⅓ of the implant correlated with the presence of radiolucent lines in any of the proximal Gruen zones (Table 2(a)). This association persisted on multi variable testing while controlling for age and gender (Table 2(b)). Average canal fill at the middle and distal thirds of stems was more uniform in anterior approach cases (85.7 ± 7.45 and 86.4 ± 8.14%, respectively) compared to posterior approach cases (80.4 ± 8.34 and 73.2 ± 12.6%, respectively). Radiolucent lines formed about all brands of femoral stem and did not associate with any specific brand (p = 0.08) (Supplemental Table 5).
Of the 244 cases with 1 year of radiographic follow-up, 148 cases (61%) completed PROMs at minimum 1 year follow-up. Median clinical follow-up time for these patients was 3.7 years (SD 1.3 years). The presence of proximal radiolucent lines (any, isolated or extensive) did not associate with pain, HOOS Jr., VR-12 PCS, VR-12 MCS, or UCLA activity scores on univariate analyses (Supplemental Tables 6 and 7, respectively).
Discussion
At minimum 1-year radiographic follow-up, we observed proximal radiolucent lines around approximately 13% of collarless fully-HA coated tapered stems. Similar proximal radiolucent lines were noted in 16 of 86 cases (19%) in 1 series of fully HA-coated tapered stems implanted through a posterior approach, 14 and 17 of 323 cases (5%) in another series in which a direct lateral approach was used and weight-bearing was restricted for 3 months postoperatively, 4 but risk factors and clinical significance were not explored in either study. The former study concluded that extensive coating may give reliable fixation despite proximal micro-movement during loading but did not investigate any association with PROMs. Prostheses in our study were implanted through anterior (73%) or posterior (27%) approaches. All patients were provided with walking aids and allowed to advance weight-bearing as tolerated throughout the recovery process. Patients were able to mobilise and discontinue walking aids earlier after the anterior approach THA. 23 Earlier unprotected weight-bearing may have influenced implant osseous integration. It has also been proposed that challenges achieving adequate femoral exposure and performing femoral bone preparation with the anterior approach may result in malposition or undersizing of the femoral stem, and increased risk of early femoral loosening. 24 Irrespective of approach, a lack of templating and undersizing of CORAIL stems has been associated with the development of RLLs.25,26 While we did not identify a significant association between surgical approach and the development of proximal radiolucent lines, a trend towards more proximal radiolucent lines with the anterior approach was observed. Although this trend warrants further investigation, our incidence of proximal radiolucent lines with predominant use of the anterior approach was intermediate between the prior reports with posterior and lateral approaches, despite allowing immediate weight bearing. To avoid undersizing and malposition of the femoral component, the authors template all cases and use intra-operative fluoroscopy in anterior-approach cases. Canal-fill measurements showed no trend towards undersizing femoral stems with the anterior approach in our study, indeed mean canal fill was slightly greater with the anterior approach.
Proximal radiolucent lines were associated with higher morphological cortical index and canal flare index, objective markers of Dorr type A femoral anatomy. They were also associated with increased canal fill at the distal third of the stem. In combination, these findings support our hypothesis that proximal radiolucent lines may occur as a result of distal wedging in the absence of adequate proximal support. Another recent study noted an association between bone morphology and radiographic outcomes of fully HA-coated femoral stems, finding less reliable osseo-integration (evidenced by absence of spot welds, absence of calcar atrophy and/or femoral component migration >5 mm) to be associated with Dorr A anatomy. 27 Although D’Ambrosio et al. 27 did not report proximal radiolucent lines, both their study and ours found less optimal radiographic findings at the fixation interface with Dorr A anatomy.
The mismatch between implant and Dorr A bone morphology highlighted here may be addressed by improvements in surgical technique or implant design. Reaming of diaphyseal bone may allow implants to reliably achieve optimal proximal support, and is recommended by certain manufacturers for Dorr A femora. Alternatively, customised implant selection may achieve more uniform support by matching individual bone morphology. Some proximally-coated tapered implants are available with both standard and reduced distal geometries; 28 such a modification might be helpful here. Distal-only wedging might also be reduced by current trends towards shortening implants, increasing sizing density and adding collars to enhance proximal support when calcar contact is achieved. Proximal-distal mismatch may also be mitigated with cemented femoral fixation.
The presence of proximal radiolucent lines in patients with collarless fully HA-coated tapered wedge stems was not associated with short-term clinical outcomes. Nevertheless, as a substantial subset of our patients did not complete PROMs, we cannot exclude the possibility that short-term clinical consequences might exist. Furthermore, our findings do not preclude the potential for long-term consequences. Although we are not the first to report this finding, its clinical significance has not been clearly addressed by previous investigations.10,11,27 Proximal radiolucent lines have been associated with hip area complaints when present around fully HA-coated primary hip stems of a fit-and-fill geometry. 29 The discrepancy between these results and ours may relate to differences in stem design but we remain vigilant for the evolution of symptoms in our patients.
Proximal radiolucent lines were present in some patients with pain and might reflect the underlying cause of symptoms. Nevertheless, many affected patients were asymptomatic and the presence of proximal radiolucent lines did not correlate with hip or thigh pain in our analysis. These data suggest that this finding alone does not establish fixation failure or indicate need for revision surgery, indeed, distal osseous integration may be present. However, x-rays at a singular time-point were reviewed, and the potential for progression of radiolucent lines with stem failure is unknown and worthy of further investigation. Longer, 10-year follow-up studies have reported conflicting results on the association of hip-area pain with proximal RLLs about CORAIL stems.25,26 We acknowledge that a minimum threshold of proximal support may be needed for patients to remain asymptomatic, and that this threshold may vary across patients based on activity and demand. Patients presenting with pain and proximal femoral radiolucent lines warrant further diagnostic investigation of both femoral fixation and other possible sources of pain, as well as vigilant longitudinal follow-up to understand if the radiolucent lines may progress distally.
This study was carried out at a single institution by surgeons with similar training and perioperative protocols, which may limit generalisability. Multi-centre, prospective studies may provide more rigorous investigation. Although the variety of femoral implants studied introduces a confounding variable, our identification of this phenomenon across a broad range of brands increases the generalisability of our findings. Incomplete follow-up, a common limitation of retrospective research performed in urban teaching hospitals, limited the power of our comparisons and may have introduced bias. Development of radiolucent lines is multi-factorial, and a larger sample size could have allowed for a more robust multi-variable analysis. Nevertheless, the number of patients identified with and without this finding was sufficient to establish demographic and morphologic risk factors.
Conclusions
To our knowledge, this is the first study specifically focused on evaluating proximal radiolucent lines around collarless fully HA-coated femoral stems. These lines, observed in 13% of cases, occurred primarily in patients with Dorr A anatomy with tight distal canal fill, which likely limited proximal cortical contact and may have limited proximal osseointegration.
Our investigation revealed no association between proximal radiolucent lines and pain or PROMs at short term follow-up. We would not diagnose fixation failure based on this finding alone, and hip pain in the presence of proximal radiolucent lines clearly warrants further evaluation of the prosthetic joint. Prospective, multi-centre studies may be useful to elucidate the significance of these findings.
Supplemental Material
sj-pdf-1-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-1-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-10-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-10-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-11-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-11-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-12-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-12-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-13-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-13-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-2-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-2-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-3-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-3-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-4-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-4-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-5-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-5-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-6-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-6-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-7-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-7-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-8-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-8-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Supplemental Material
sj-pdf-9-hpi-10.1177_11207000231178269 – Supplemental material for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned?
Supplemental material, sj-pdf-9-hpi-10.1177_11207000231178269 for Proximal radiolucent lines around fully hydroxyapatite-coated tapered femoral stems: should we be concerned? by Zachary P Berliner, Muhammad Umar Jawad, Chelsea Matzko, H John Cooper, Jose A Rodriguez and Matthew S Hepinstall in HIP International
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.