
Abstract
Purpose:
Several controversies in the optimal treatment of femoral neck fractures persist, together with large variations in clinical practice.
Methods:
A narrative literature review covering 4 current controversies in the surgical management of femoral neck fractures (total hip arthroplasty (THA) versus hemiarthroplasty (HA), cemented versus uncemented HA, internal fixation versus arthroplasty, operative versus non-operative) was performed. Available literature was balanced against annual trends in the management of femoral neck fractures from the public domain of several national registries (Sweden, Norway, The Netherlands, Australia and New Zealand).
Results:
For most controversies, the literature provides stronger evidence than is reflected by variations encountered in daily practice. Implementation of clinical evidence tends to lag behind and important differences exist between countries.
Conclusions:
Trends of clinical practice from national registries indicate that implementation of available clinical evidence needs to be improved.
Introduction
Each year 1–2 million patients around the world sustain a fracture of the hip which in general is treated with a surgical intervention. 1 Hip fractures are associated with 1-year mortality rates of up to 27% and show a 3-times higher risk of mortality compared to the general population. 2 Health-related quality of life, in both physical and psychosocial dimensions, is strongly affected in patients suffering from a fracture of the hip. 3 As such, the global burden on mortality, quality of life and healthcare costs in the expanding population of hip fracture patients is a major public health concern; annual healthcare costs associated with hip fracture surgery in the USA is estimated to be around $14 billion. 4
Hip fractures can be divided into fractures of the femoral neck and trochanteric fractures. In general trochanteric fractures are treated with internal fixation, whereas surgical treatment options for femoral neck fractures are less uniform and consist of internal fixation, hemiarthroplasty or total hip arthroplasty. 5 Despite the high incidence of these hip fractures and the associated health related and economic burden, there is limited consensus about the best treatment. This lack of consensus is particularly related to the subcategory of femoral neck fractures where, despite extensive research, there is controversy over the optimal treatment, as well as significant variations in clinical practice.
The aim of this study was to prioritise a number of controversies in the surgical treatment of hip fractures and in particular for femoral neck fractures. We reviewed the literature for the best available evidence on each controversy and establish whether trends in daily practice were evidence-based, using data from national registries around the world. It is beyond the scope of this manuscript to provide a true review and meta-analysis following PRISMA (Preferred Reporting Items for Systematic reviews and MetaAnalyses) guidelines; 6 instead, a narrative form is presented.
Materials and method
For this review 4 current controversies in the surgical management of femoral neck fractures were selected:
(1) Total hip arthroplasty versus hemiarthroplasty?
(2) Cemented versus uncemented hemiarthroplasty?
(3) Internal fixation versus arthroplasty (in ‘young elderly’)?
(4) Operative versus non-operative treatment?
For each controversy a literature search was performed using Pubmed from inception through July 2020 for available systematic reviews, (randomised controlled) trials (RCTs) and registry studies. In particular, consensus from available reviews and meta-analyses following PRISMA guidelines was used to discuss and summarise the best level of evidence regarding each controversy. 6 References from reviews and meta-analysis were analysed for missed (randomised controlled) trials and registry studies which were subsequently incorporated separately.
Besides a literature review on the best available evidence on each controversy, an attempt was made to obtain data on annual trends in the management of femoral neck fractures from the public domain of several national registries (Sweden, Norway, The Netherlands, Australia and New Zealand).7–10 For each controversy available national annual trends in clinical practice variation in the management of femoral neck fractures were elucidated. Subsequently, recommendations on each controversy obtained from the available literature were balanced against data on clinical practice from available national registers.
Results
Total hip arthroplasty or hemiarthroplasty?
An important controversy in femoral neck fracture management concerns treatment with either total hip arthroplasty or hemiarthroplasty. There has been extensive research carried out to determine the best choice of arthroplasty in the treatment of femoral neck fractures. 2 systematic reviews regarding patients with a fracture of the femoral neck treated with either total hip arthroplasty (THA) or hemiarthroplasty identified 13 RCTs which had enrolled 1364 patients and 7 RCTs combined with 8 retrospective cohort studies with 1890 patients, respectively.11,12 Both reviews conclude there was a lower re-operation rate and a higher Harris Hip Score (HHS) after THA, whereas an overall higher risk of dislocation after THA is also reported,11,12. Furthermore, a separate RCT showed no difference in hip function and health-related quality of life, nor in re-operations and complications in octogenarians and nonagenarians. 13 2 recent registry studies focusing on treatment with hemiarthroplasty or THA reveal contradictory results in secondary procedures. Moerman et al. 14 found a higher, and Hansson et al. 15 a lower, chance of secondary procedures after total hip arthroplasty.
From these reviews and recent studies one may conclude that THA and hemiarthroplasty are both viable surgical treatment options for elderly patients with a femoral neck fracture. Clearly, the available literature falls short in discriminating between age-groups, which is also important in weighing the balance between total or hemi arthroplasty. This dilemma has been further elucidated by another recent landmark study (HEALTH Investigators et al. 16 ) in which 1495 randomised patients with a mean age of 79 years old failed to reveal clinically important advantages of total hip arthroplasty versus hemiarthroplasty. However, this study used a relatively short follow-up of 2 years and one may argue whether the conversion rate of hemiarthroplasty towards THA may increase with longer follow-up. 16 This assumption is, however, not supported by other studies with longer follow-up of hemiarthroplasty.17,18 In summary, the recent literature indicates that the benefits of THA over hemiarthroplasty for the surgical treatment of femoral neck fractures should not be overestimated and may in the best case probably be reserved for relatively young patients <70 years old.
Data on annual trends from the public domain of the national registries of Sweden, Norway, the Netherlands, Australia and New Zealand were available to elucidate this controversy (Figure 1).7,8,10,19 Overall, data reveal that between 10% and 35% of femoral neck fractures are treated with a total hip arthroplasty. Within this range there appears to be an increasing trend in the use of THA versus hemiarthroplasty from 2010 onwards for most countries (Sweden, Norway, Australia and New Zealand) whereas for The Netherlands a slight decline appears to be present (Figure 1). Moreover, this data reveals wide differences in the use of THA versus hemiarthroplasty across countries since the number of patients treated with THA varies from a ⅓, a ¼ and a ⅕ in Sweden, The Netherlands and Norway, respectively (Figure 1). The observed increasing trend in the use of THA does not correspond with the available evidence in the literature where the superiority of THA is not supported. It will be interesting to follow these trends after the appearance of the recent landmark study. 16 Obviously, no firm conclusions can be drawn from registry data, but it seems safe to conclude that national trends in choosing total or hemiarthroplasty for treatment of femoral neck fractures do not correspond with the available evidence in the literature.
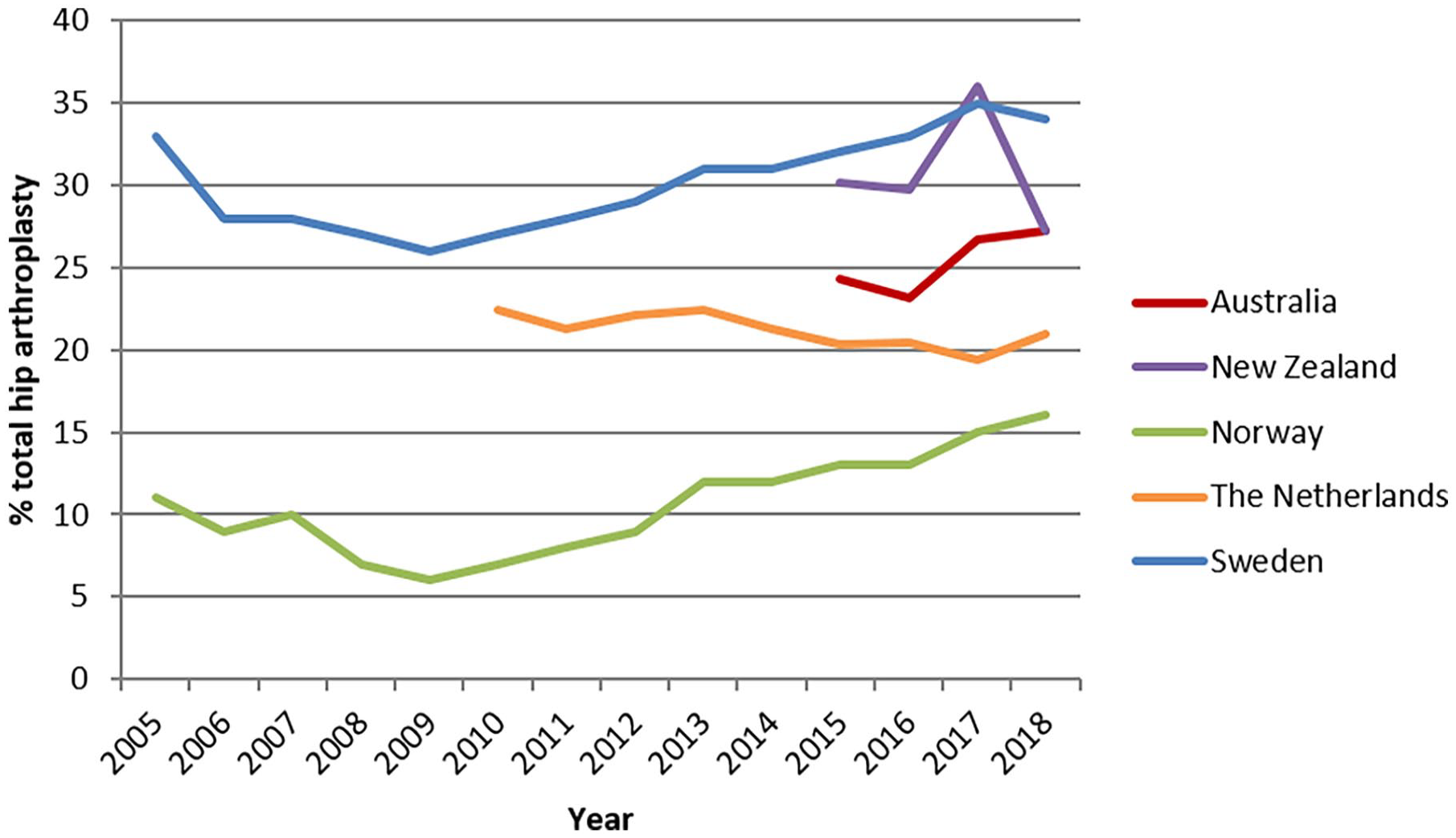
Rates of total hip arthroplasty as percentage of all arthroplasties (total hip arthroplasty plus hemiarthroplasty) as retrieved from data in national registries available on the public domain. Percentages use a scale of 0–40%.
The observed increase in use of THA suggests that many factors may play a role in surgical decision making. Comparing the extensive research performed regarding this controversy against data from national registries reveals a discrepancy between evidence in the literature and daily practice in several countries.
Cemented or uncemented hemiarthroplasty?
Another controversy in the treatment of femoral neck fractures is the use of cemented versus uncemented hemiarthroplasties. 2 recent systematic reviews regarding this topic identified 8 RCTs concerning 1577 patients and 9 RCTs combined with 20 observational studies concerning 42,046 patients,20,21 respectively. These studies show higher rates of periprosthetic fractures in uncemented hemiarthroplasties.20,21 No differences were found in terms of mortality, re-operation or hip function.
Besides the RCTs incorporated in these reviews, a further 2 well-performed RCTs were encountered which revealed better function after cemented hemiarthroplasty and no differences in mortality, re-operations or complications.22,23 The favourable results in cemented hemiarthroplasty shown in systematic reviews and RCTs are also supported by registry studies from The Netherlands, Norway and Finland. These registry data report higher rates of re-operations in uncemented hemiarthroplasties.24–26
A potential disadvantage of cemented hemiarthroplasty may be an increased risk of cardiopulmonary events due to the occurrence of pulmonary embolism, leading to more intraoperative deaths in comparison to uncemented hemiarthroplasty. 27 However, the literature doesn’t report a higher 1-month and 1-year mortality rate for cemented hemiarthroplasties.20–26,28,29
Again, annual trends from the public domain of national registries were obtained, resulting in available data from Sweden, Norway, the Netherlands, Australia and New Zealand to elucidate on this controversy.7,8,10,19 In particular, for Sweden and Norway, complete follow-up registry data were available over the past 10 years. Overall, from 2012, a rapid decline in the percentual use of uncemented hemiarthroplasty could be observed (Figure 2). Remarkable differences between countries still apply with a peak in use of uncemented hemiarthroplasties of around 35% for both the Netherlands and Norway around 2012, whereas for Sweden this percentage declined, from <5% towards the eventual discarding of this type of implant after 2016. Limited data from Australia and New Zealand (2015–2018) match with the observed strong decline of uncemented hemiarthroplasties after 2012 in other countries.
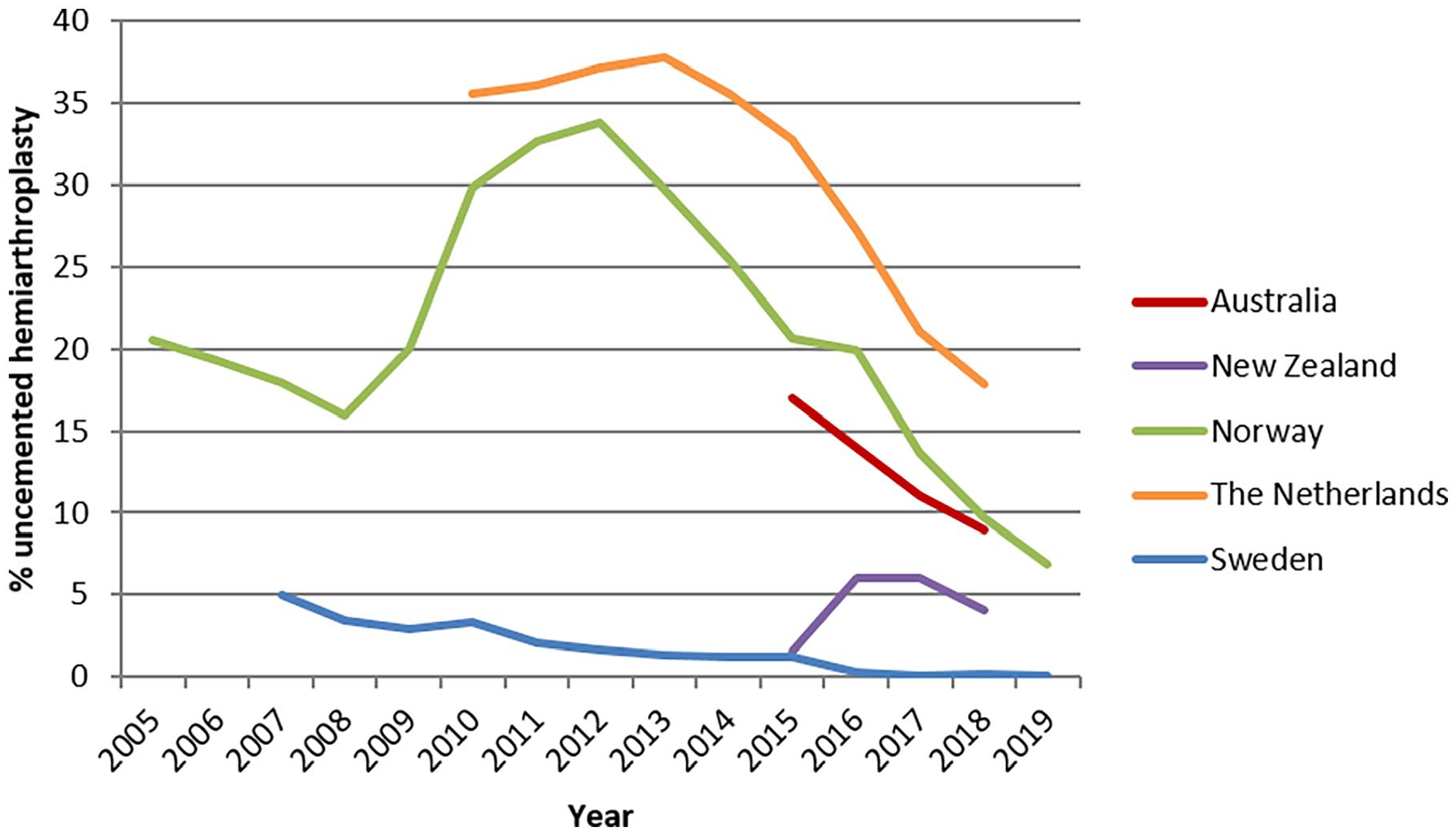
Rates of uncemented hemiarthroplasty as percentage of all hemiarthroplasties (cemented plus uncemented) as retrieved from data in national registries available on the public domain. Percentages use a scale of 0–40%.
Corresponding with the increasing evidence favouring cemented hemiarthroplasty, an overall decline in the use of uncemented hemiarthroplasty is clearly visible after 2012. Nevertheless, large differences in the absolute percentage of uncemented hemiarthroplasty remain, ranging from 20% in the Netherlands in 2018 up to the end of its use in Sweden at that time. The reason for this continuing use of uncemented hemiarthroplasties, despite convincing evidence, is unclear. It is possible the use of uncemented hemiarthroplasty is influenced by other (non-medical) factors such as efficiency, since a shorter operation time is found in uncemented hemiarthroplasty.20,21,23,30
Internal fixation or arthroplasty (in ‘young elderly’)?
The type of surgical treatment of femoral neck fractures has been widely analysed. However, the choice of treatment with either (hemi)arthroplasty or internal fixation is an ongoing controversy in the literature. Systematic reviews involving internal fixation versus (hemi)arthroplasty, concerning 14 RCTs and 2 RCTs combined with 1 observational study,31,32 respectively, show better results after both types of arthroplasty in terms of secondary interventions, complications and function.31,32 These conclusions have also been confirmed by other well-performed RCTs,33–36 which were not incorporated in the systematic reviews above. These perceived benefits of arthroplasty have to be balanced against the main benefit of internal fixation, preservation of the native hip joint. As such, the patient’s age appears to play an important role in weighing the respective potential benefits of an arthroplasty versus internal fixation. The literature appears to be conclusive for patients >70 years of age; this group of patients can best be treated with a hemiarthroplasty.33–36 Obviously, the potential benefits of preservation of the native hip joint only apply to younger patients and as such internal fixation is preferred over arthroplasty for patients <60 years old. 37
Treatment of femoral neck fractures in the age group of 60–70 years is still most controversial and unfortunately, the literature is scarce. 37 A study involving patients between 55 and 70 years, using data from the Norwegian Hip Fracture Register, showed a re-operation rate of 27% in patients treated with internal fixation compared to 2.8% and 3.8% after THA and hemiarthroplasty, respectively. In addition, patient-reported outcome measures reported better results after arthroplasty. 5 From these high failure rates and inferior patient satisfaction after internal fixation one may support arthroplasty for this relatively young age group. Nevertheless, proponents of internal fixation could argue that in cases of failure of internal fixation of femoral neck fractures, a THA can still be used as a salvage procedure. However, this option is not without a downside. An important aspect of good clinical practice is not to “burn any bridges” and it is well recognised that THA as a salvage procedure after a failed osteosynthesis has higher rates of revision and complications compared to THA in femoral neck fractures as an index procedure.38–40
Clearly, there is a lack of high-quality evidence for the best treatment for femoral neck fractures in particular in the age group 60–70 years. The limited results available in the literature raise the question of whether this group of patients does indeed benefit from preservation of the hip joint or whether this theoretical advantage is generally overestimated. This group of patients should be counselled about the relatively high risk of failure of internal fixation and the potentially higher risk of complications after THA as a salvage procedure, but must also understand that hip replacement is not a panacea. Shared decision making should be encouraged between clinician and patient with appropriate documentation of the risks and benefits of each option. Well performed future studies in this population may provide more evidence to support decision making for this group of patients.
A search of data on annual trends from the public domain of national registries resulted in only limited data from Norway, Australia and New Zealand to elucidate on the treatment of femoral neck fractures with either hemiarthroplasty or internal fixation.7,8 Registry data from the Netherlands and Sweden were not available since these registries report no data concerning internal fixation.9,10 In the Netherlands, The Dutch Hip Fracture Audit started in 2016 to also collect data for internal fixation in hip fractures. 41 Unfortunately, no valid data could be obtained from this registry since available data proved incomplete due to its recent start-up and to be biased because of the concomitant inclusion of trochanteric fractures. More specifically, data from Norway reported on comprehensive changes in the use of internal fixation versus (hemi)arthroplasty (Figure 3). In 2005 in Norway almost half of femoral neck fractures were treated with internal fixation whereas, following a rapid decline, only 3% of femoral neck fractures were treated with internal fixation in 2019. The rising use of (hemi)arthroplasty in this registry data is in accordance with the favourable results of arthroplasty compared to internal fixation. However, this data does not solve the controversy in the age group of 60–70 years since it includes patients of all ages. In contrast to data regarding both type of arthroplasty and the use of cement in hemiarthroplasty, data with regard to internal fixation versus arthroplasty is poorly represented in national registers. Further data is needed to solve the controversy for patients between 60 and 70 years old.
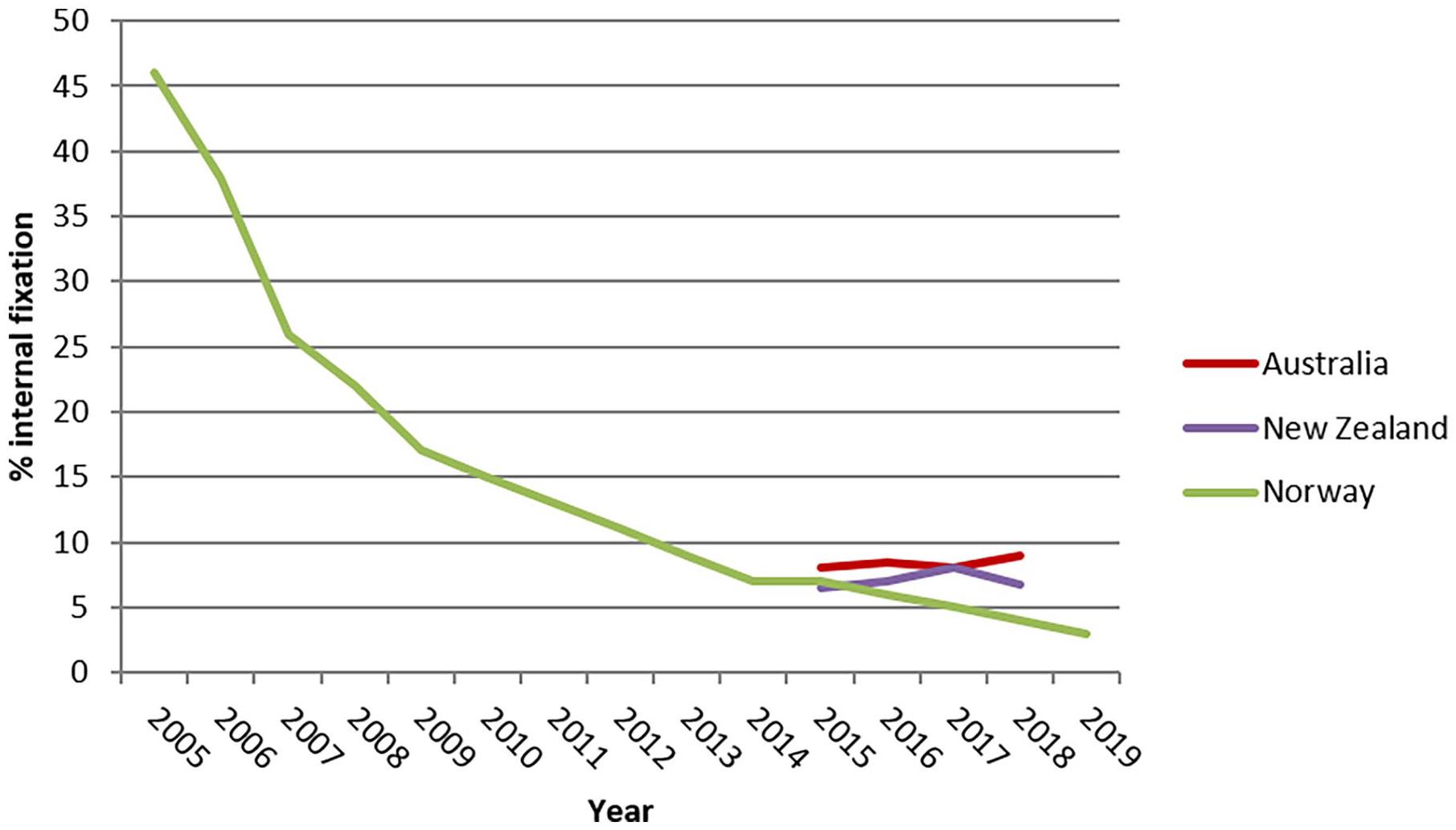
Rates of internal fixation as percentage of all types of treatment (internal fixation plus hemi(arthroplasty)) as retrieved from data in national registries available on the public domain. Percentages use a scale of 0–50%.
Operative or non-operative treatment?
The aims of treatment in the frail elderly population with a femoral neck fracture should focus on pain relief and early mobilisation. The postoperative overall 1-year mortality rate in these hip fracture patients is as high as 27%, 2 and in specific groups, such as those patients with end-stage dementia, mortality may be as high as 55% within 6 months. 42 Nevertheless, operative treatment is still performed on nearly all patients with a femoral neck fracture since non-operative treatment has the reputation of resulting in persistent pain, major patient discomfort, high risk of pneumonia and early death.43,44 However, there is a lack of well-performed studies to support these assumptions, particularly patient discomfort, and for a small group of very fragile patients the risk of mortality is very high irrespective of the choice of treatment.43,44
Only 1 single systematic review focuses on operative and non-operative treatment of hip fractures. 43 This review found only 7 non-randomised studies and concludes there are increased 1-year mortality rates after non-operative treatment. None of these studies, however, reported on patient participation in the choice of treatment, pain, subsequent quality of life or perceived patient discomfort. RCTs are not available since randomisation between operative and non-operative treatment would not be feasible in this group of patients. As such, in the available studies non-operative treatment resulted in a significantly increased mortality rate; however, prolonging life may not be in a patient’s best interest or be the best choice for the very frail and elderly. Currently, there is a 2-arm non-randomised multi-centre prospective cohort study comparing the outcome of operative versus non-operative treatment of hip fractures in frail institutionalised patients who are either malnourished, have mobility issues or severe comorbidities (American Society of Anesthesiologists (ASA) class 4 or 5). 45 To the best of our knowledge this is the first study in which the option of non-operative treatment is actively offered to a selective group of frail patients. Besides 1-year mortality rates, pain and perceived patient comfort are also important outcome parameters. Knowing that early death can be expected in this study, quality of dying is also assessed using a validated outcome score. 46
The start of this FRAIL-HIP study suggests the time has come to explore non-operative care for hip fractures as a viable treatment option for a selected group of frail patients with limited life expectancy, for whom comfort and pain are more relevant than survival. Such an approach can only succeed with close collaboration with ortho-geriatric trauma care.
So far, data from the national registries are not available regarding this controversy.
Discussion
Despite the high incidence of femoral neck fractures and the extensive research performed worldwide, the best treatment for femoral neck fracture patterns in different patients remains unclear. These controversies exist partly due to a lack of evidence; however, variation in daily practice was also encountered in various national registries where consensus proved to be available from the literature. Obviously, the process of obtaining consensus or maintaining controversies is complex and many factors are involved.
Controversies versus clinical practice in registries
Treatment with either hemiarthroplasty or total hip arthroplasty is extensively discussed in well-performed high quality studies. The rise in the use of THA in daily practice as reported in several national registries is, however, not supported by evidence demonstrating THA to be superior to hemiarthroplasty.7,8,10–16,19 Conversely, the literature indicates that potential benefits from THA over hemiarthroplasty are likely to be overestimated.
Similarly, a clear consensus in the literature favours the results of cemented hemiarthroplasty over uncemented hemiarthroplasty.20–26 This consensus is represented by a steep decline in the use of uncemented hemiarthroplasty after 2012 as demonstrated in trends from registry data. However, the continued use of uncemented hemiarthroplasty in up to 20% of cases is reported in some countries in 2018.7,8,10,19
Another persisting controversy concerns treatment with either (hemi)arthroplasty or internal fixation. From the literature, there appears to be consensus for older (>70 years) and younger (<60 years) patients favouring (hemi)arthroplasty and internal fixation, respectively.31–36 However, the most appropriate treatment for patients between 60–70 years remains controversial since preservation of the normal hip joint is often aimed for whereas failure rates of internal fixation are high and THA is at higher risk of complications if performed as a salvage procedure after fixation failure.5,38–40 Unfortunately, this controversy in patients between 60–70 years cannot be solved with registry data since no data are available concerning specific age groups. Future studies with focus on this difficult age group of 60–70 years in combination with the option of differentiation between age groups in national registries may help to obtain improved consensus for the best treatment for patients of 60–70 years.
Lastly, the controversy regarding the best treatment of frail elderly patients with limited life expectancy is ongoing as evidence is limited. The few available studies have focused on an increased early mortality rate in non-operative treatment whereas a focus on optimal pain relief and patient comfort may be more relevant to this group than prolonged survival. The increasing interdisciplinary collaboration in ortho-geriatric trauma care can improve the delivery of patient-centered care and offer shared decision making when possible and could consider non-operative palliative care for the most fragile patients.
In this study important discrepancies were encountered between evidence from the literature and daily clinical practice as represented in several national registries. Consensus from even high-quality evidence only partly reflects the daily practice reported in national registries and there are differences between countries. The implementation of evidence-based daily practice proves to be complex. Several factors, such as personal or national preferences and non-medical incentives, also play a role.
The controversies are dealt with in a literature review and did not follow the PRISMA guidelines for a systematic review. This approach was knowingly undertaken since all 4 controversies are rather broad in nature and an approach following the PRISMA guidelines would have demanded 4 separate and lengthy manuscripts. Instead, the aim of this review was to provide a concise overview of the literature and to balance these findings with available data on daily practice from different national registries. For this reason, the literature search focused on available systematic reviews added to missed RCTs. Secondly, registry data presented in this review were mainly obtained from graphics in annual registry reports available in the public domain and there was mostly no access to the source data. This is inevitable for the type of research performed and comes with the limitations (and benefits) which apply to all research performed with data from national registries.
In conclusion, this review reveals that controversies in the management of femoral neck fractures persist. Irrespective of conclusive consensus in the literature, data from trends in clinical practice from national registries suggest that clinical evidence is not adequately integrated into daily practice. We feel that studies in which clinical evidence is balanced against daily practice, such as in this narrative review, are important in order to monitor to which extent evidence-based practice is incorporated into clinical practice and to what extent differences between countries exist. Exploring treatment trends in national registries balanced against the best available evidence stimulates discussion about whether differences are justified or not. This will lead to an improvement in implementation and will reduce inconsistencies in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.