
Abstract
Purpose
To describe a new surgical technique involving the use of a human amniotic membrane (hAM) epiretinal patch to treat a primary macular hole retinal detachment (MHRD) in a highly myopic patient.
Methods
A 60 years old highly myopic man was referred to our clinic with a diagnosis of MHRD in his right eye. The patient was pseudophakic, with a visual acuity of counting fingers at the baseline evaluation. Pars plana vitrectomy was performed, a small retinotomy was created at the inner margin of the staphyloma, and membrane blue dual was used to obtain an adequate peeling of the inner limiting membrane. Then, a 1.5 mm diameter circular hAM patch was obtained and positioned over the macular hole with the chorion layer settled over the retina. After a complete fluid-air exchange, 20% sulfur hexafluoride gas was used as endotamponade, and the patient was asked to remain face down for three days.
Results
Four weeks after surgery, optical coherence tomography (OCT) scan showed the hAM patch, visualized as a distinct hyperreflective layer well integrated with the retina. Nine months after surgery, the macular hole was closed, the retina reattached, the hAM patch was adherent to the retina, and the patient presented a best-corrected visual acuity improved to 0.7 logMar. No postoperative adverse events were registered during the follow-up.
Conclusions
Epiretinal hAM implant could represent a novel surgical technique, feasible and easier compared to other current techniques used to treat MHRD in highly myopic patients.
Keywords
Introduction
Macular hole retinal detachment (MHRD) is one of the most vision-threatening complications in highly myopic patients. Although the pathogenesis is not entirely understood, some factors, such as the elongation of the axial length, the posterior staphyloma formation, the reduced chorioretinal adhesion due to posterior chorioretinal atrophy, increased tension in retinal vessels, tangential traction of the vitreous cortex and epiretinal membrane seem to be related.Fare clic o toccare qui per immettere il testo. 1 The surgical management of this pathology remains very challenging and various surgical methods have been carried out to achieve improvement of anatomic and functional outcomes.
Gonvers and Machemer in 1982 first introduced pars plana vitrectomy (PPV) and partial gas-fluid exchange for the management of MHRD, but the inability of the inelastic retina to conform to the concavity of the staphyloma and the poor adhesion between the neurosensory retina and the underlying atrophic retinal pigment epithelium (RPE) and choroid were major causes of failure. 2 Since then, various alternative methods have been proposed, including PPV with silicone oil tamponade, 3 macular buckling,Fare clic o toccare qui per immettere il testo. 4 vitrectomy with scleral imbrications, 5 PPV associated with macular buckling, Fare clic o toccare qui per immettere il testo.6,7 vitrectomy with inverted internal limiting membrane (ILM) flap Fare clic o toccare qui per immettere il testo. 8 or free ILM flap, 9 vitrectomy with autologous neurosensory retinal free patch transplantation. 10
However, dealing with flap techniques in high myopia can be challenging due to the difficulties to harvest remnants of ILM from the posterior pole or from the edges of the posterior staphyloma. The human amniotic membrane (hAM) is a readily available tissue that has already been used for many ophthalmic applications.
Recently, hAM subretinal implant has been proposed to treat recurrent macular holes (MH), especially in highly myopic eyes, and in MHRD with good functional and anatomical outcomes.Fare clic o toccare qui per immettere il testo. 11
However, hAM plug implant in the subretinal space could present possible intraoperative complications such as plug dislocation under the detached retina during the fluid-air exchange or the subretinal fluid drainage. Recent studies reported the epiretinal implant of different types of hAM in cases of recurrent myopic macular holes associated with retinal detachment achieving good results in terms of safety and visual outcome.12,13,14
The aim of the present study is to describe a new surgical technique involving the use of a hAM epiretinal patch to treat a primary MHRD in a highly myopic patient.
Methods
A 60 years old caucasian man was referred to our clinic at the University of Bologna Hospital with a diagnosis of MHRD in his right eye. The patient was pseudophakic, with an axial length of 29.94 mm, calculated using the IOL-Master 700 (Carl Zeiss Meditec, Jena, Germany) biometer. A complete ophthalmic examination was performed preoperatively, and the best-corrected visual acuity (BCVA) was counting fingers in his right eye. The patient underwent an Optical Coherence Tomography (OCT) scan (Spectralis Heidelberg Engineering GmbH, Heidelberg, Germany) that confirmed the diagnosis of MHRD. Ultra-wide field images were taken using Optos Silverstone (Optos PLC, Dunfermline, UK) (See Figure 1). The study protocol adhered to the tenets of the Declaration of Helsinki. Written informed consent, including consent to publish, was obtained from the participant. Ethical approval from the local Institutional Review Board “Comitato Etico di Area Vasta Emilia Nord” was not required for this study.
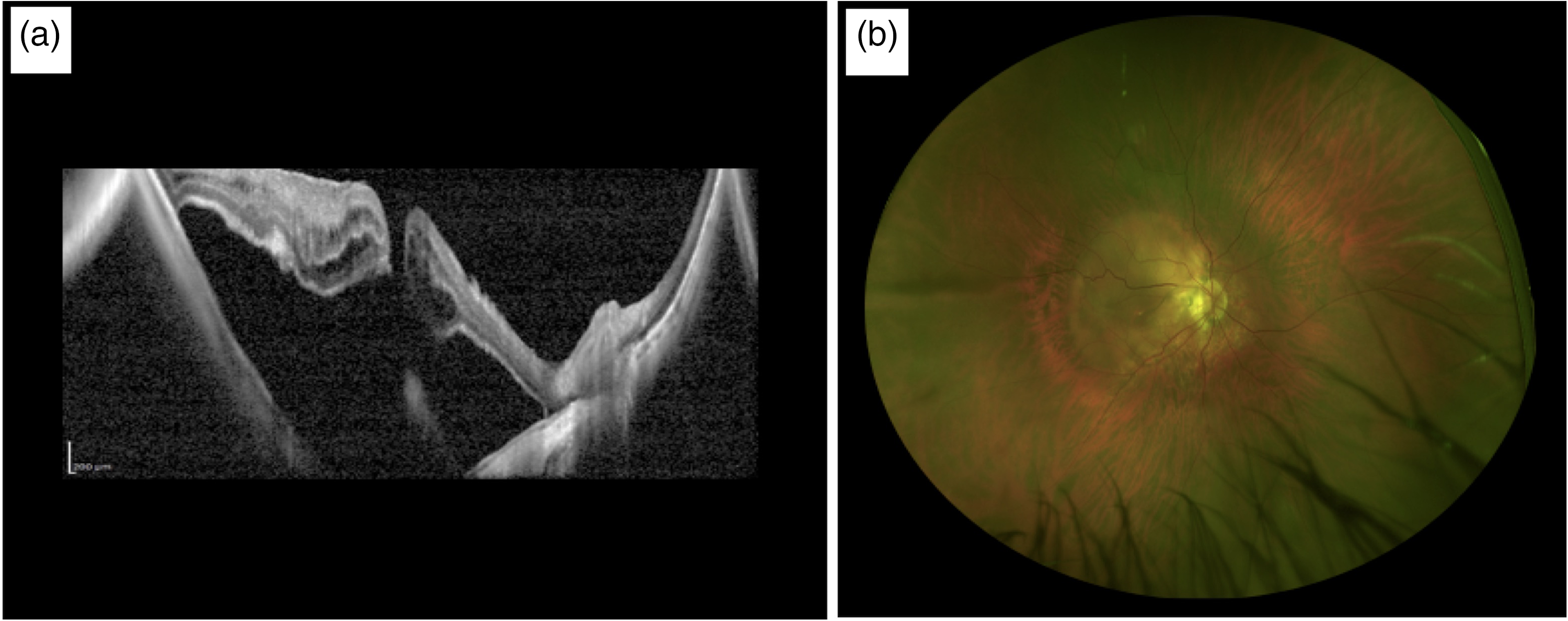
Pre-operative assessment. a) Optical coherence tomography (OCT) scan shows the presence of macular hole retinal detachment (MHRD) in the right eye of a highly myopic patient. b) Ultra-wide field color image of the right eye is shown.
Surgical technique
Surgery was undertaken under subtenon anesthesia, using a 23-gauge vitrectomy (EVA; DORC Dutch Ophthalmic Research Center International BV- Zuidland- The Netherlands) setting, and a 27-gauge chandelier. A complete pars plana vitrectomy (PPV) was performed, and triamcinolone acetonide was injected into the vitreous cavity to ensure a complete posterior vitreous detachment. In the superior area at the inner margin of the staphyloma, a small retinotomy with a 25-gauge endodiathermy probe was performed. Subsequently, a small bubble of perfluorocarbon (PFCL) was injected and membrane blue dual (DORC Dutch Ophthalmic Research Center International BV- Zuidland- The Netherlands) was used to stain the ILM. However, the peeling of the ILM was insufficient to obtain an inverted flap due to the thin and friable ILM. A 1.5 mm diameter of circular hAM patch was obtained with a dermal punch (Disposable Biopsy Punch, Kai Medical, Solingen, Germany), with the aim of covering the macular hole. Once the PFCL was removed, the patch was inserted through the trocar and positioned over the hole with the chorion layer over the retina. Inside the vitreous chamber, the chorion layer of the hAM plug was determined by identifying the sticky side of the plug using a serrated forceps (GRIESHABER® MAXGRIP® Forceps Alcon Surgical, Inc, Houston, Tex). Then, PFCL was reinjected to stabilize the patch, and endolaser was performed around the retinotomy. A complete fluid-air exchange was obtained, at the beginning keeping the extrusion needle away from the macula at the superior margin of the PFCL bubble, then over the retinotomy and subsequently over the optic disc. At the end of the operation, the air was replaced with 20% sulfur hexafluoride gas (Fluoron GmbH, Germany) (See Figure 2 and Figure 3). Postoperatively, the patient was asked to remain face down for three days after surgery.
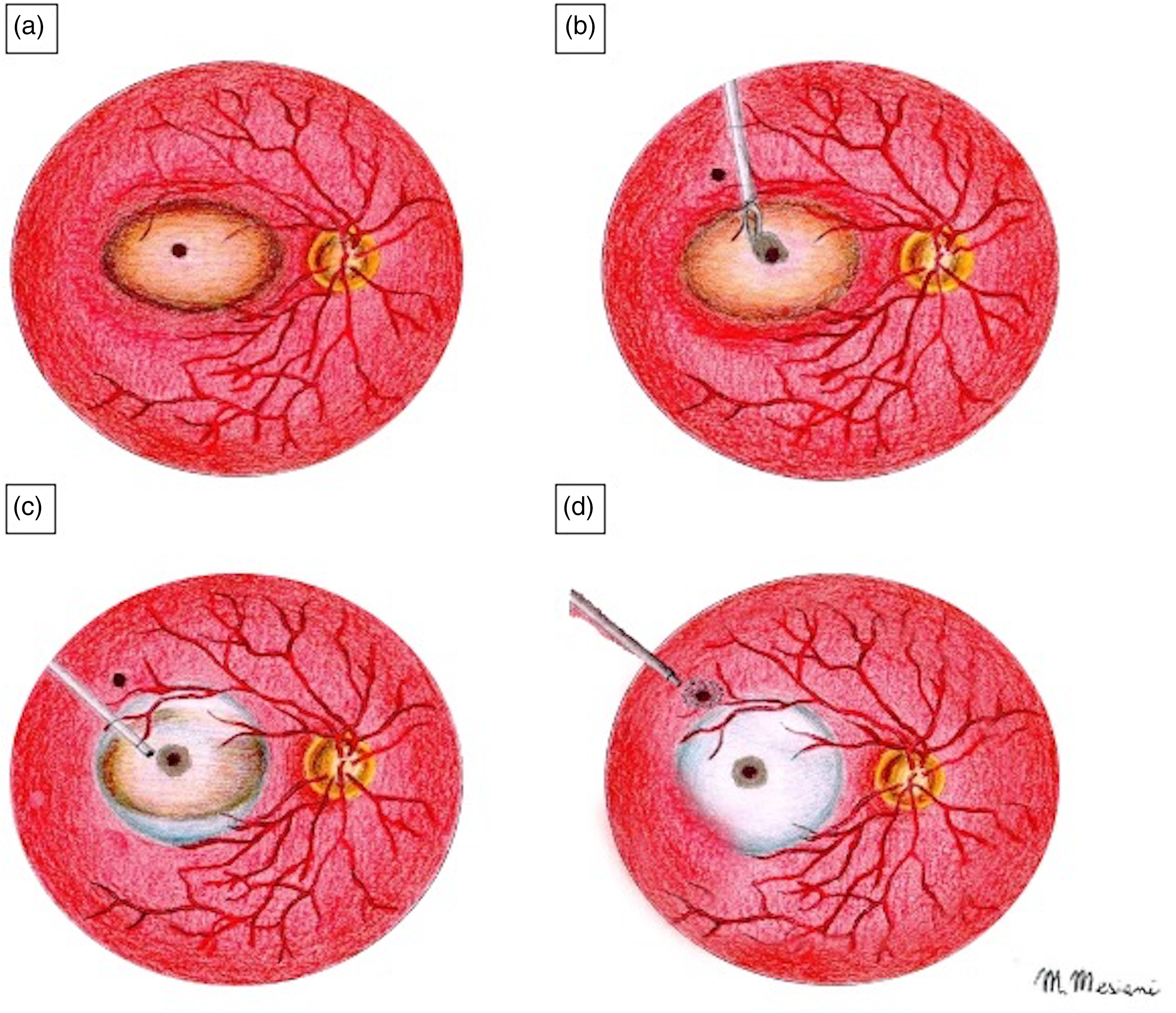
Illustration of the surgical technique. a) Graphical representation of the macular hole retinal detachment (MHRD). b) After internal limiting membrane (ILM) removal and the creation of a small retinotomy in the superior temporal mid-peripheral retina at the inner margin of the staphyloma, a 1.5 mm diameter of circular human Amniotic Membrane (hAM) patch was obtained and positioned over the hole with the chorion layer over the retina. c) Perfluorocarbon (PFCL) gas was injected in order to stabilize the patch d) Endolaser of the retinotomy and a complete fluid-air exchange were performed, keeping the extrusion needle away from the macula at the margin of the PFCL bubble. At the end of the operation, the air was replaced with 20% sulfur hexafluoride gas.
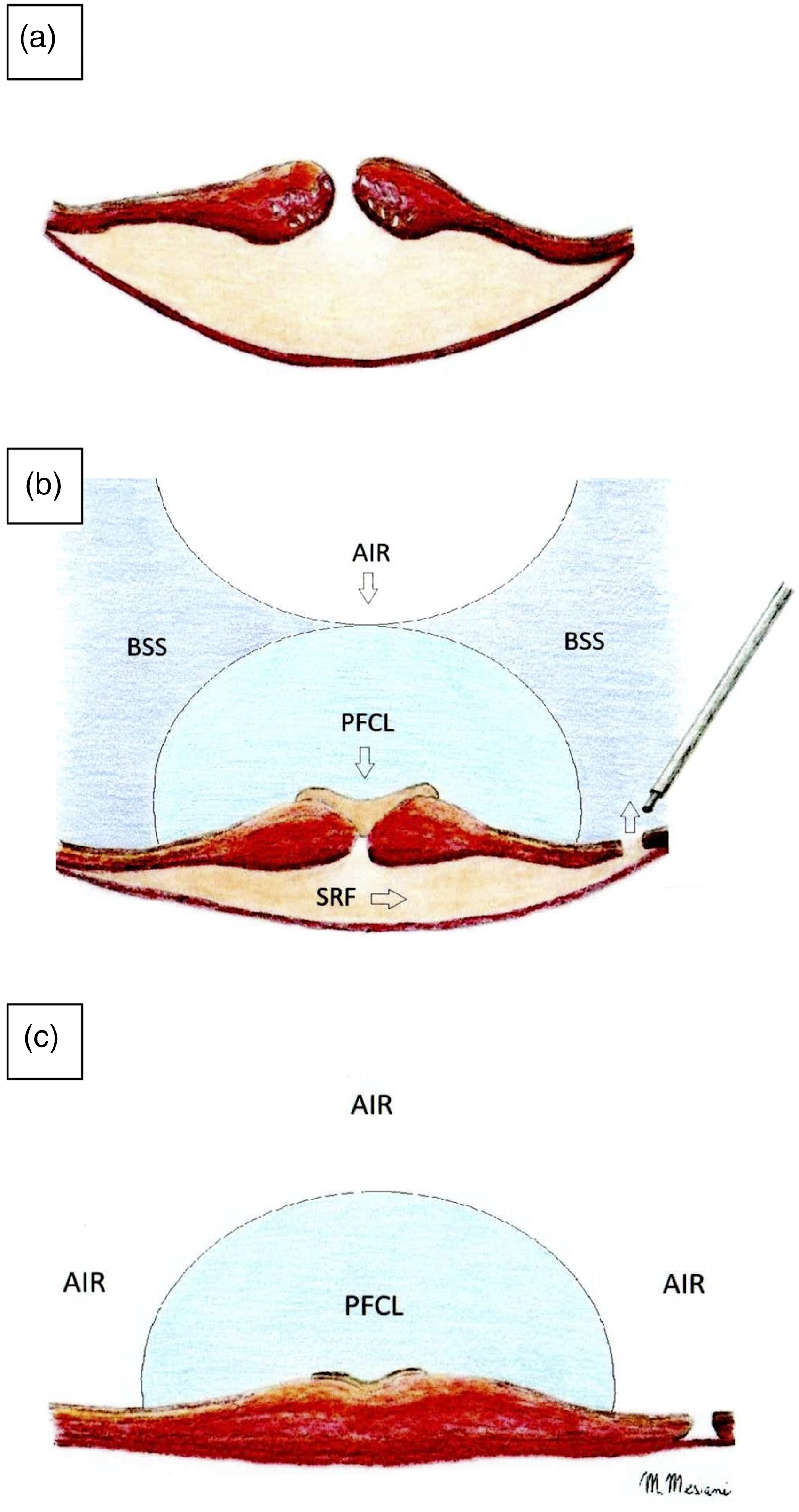
Details of the fluid-air exchange. a) Cross-sectional image of the macular hole retinal detachment (MHRD). b) and c) show the complete fluid-air exchange, keeping the extrusion needle away from the macula at the margin of the Perfluorocarbon (PFCL) bubble in order to obtain a complete reabsorption of the subretinal fluid.
Results
Four weeks after surgery, the OCT scan showed the hAM patch, visualized as a distinct hyperreflective layer well integrated with the retina. Moreover, the macular hole was closed, and the retinal was reattached with a shallow residual amount of subretinal fluid. (See Figure 4b). The last follow-up visit was performed at 9 months, confirming the macular hole closure, the reattachment of the retina, and the adhesion of the epiretinal hAM patch, with a BCVA improved to 0.7 logMar. (See Figure 4B, 4C and 4D). No postoperative adverse events were registered during the follow-up.
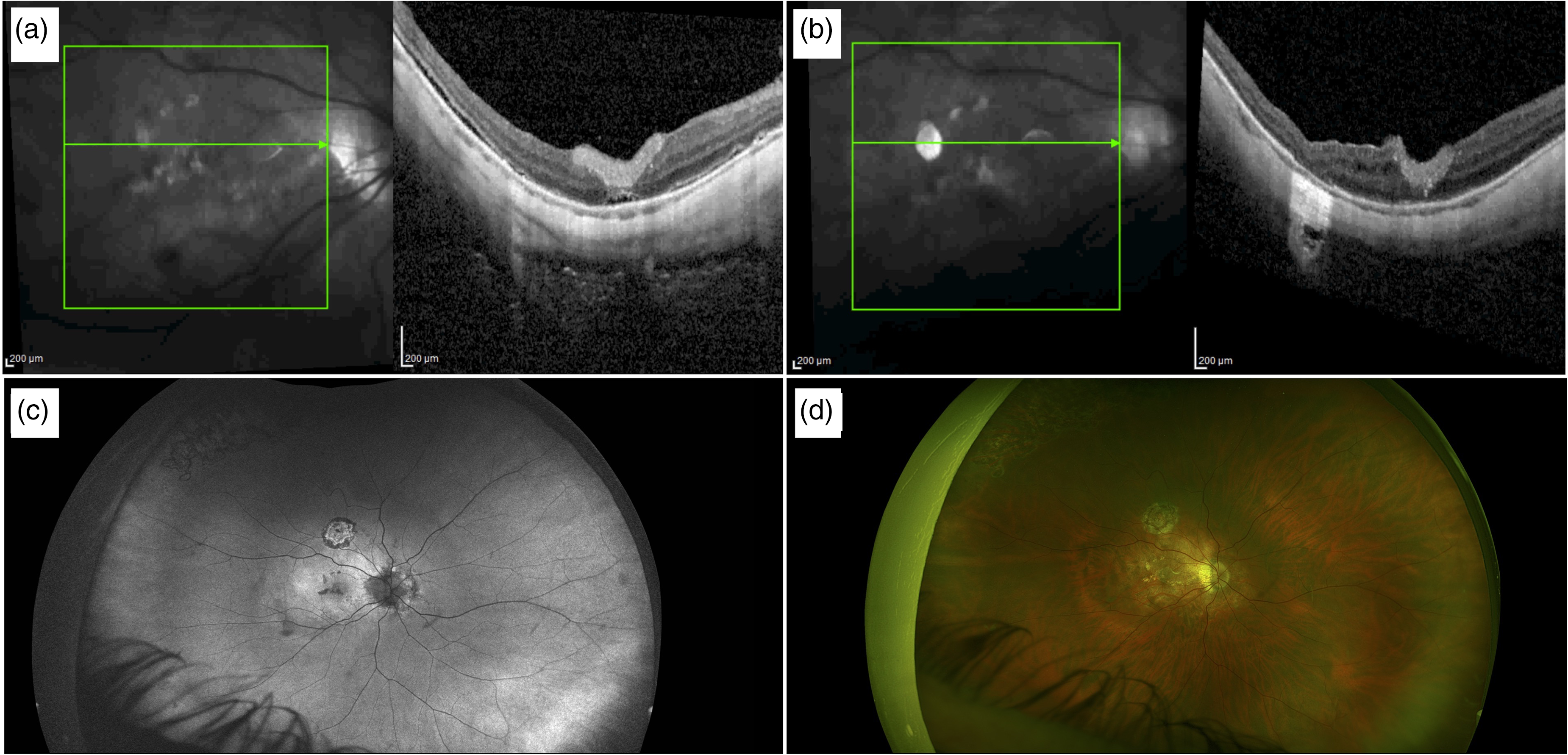
Post-operative assessment. a) Optical coherence tomography (OCT) scan performed four weeks after surgery showed the presence of the human Amniotic Membrane (hAM), visualized as a distinct hyperreflective layer well integrated with the retina. The macular hole was closed, and the retinal was reattached with a shallow residual amount of sub-retinal fluid. b) OCT scan performed nine months after surgery showed the macular hole closure, the reattachment of the retina, and the adhesion of the epiretinal hAM patch, with reabsorption of the subretinal fluid. c) and d) Ultra-wide-field fundus autofluorescence and color images nine months after surgery are shown.
Discussion
Surgery for MHRD is still a challenge and the visual results may be poor despite successful anatomical closure of macular hole and retinal reattachment.
Encouraging outcomes have been described with ILM free flap and neurosensory retinal free patch transplantation despite some critical issues. The purpose of these techniques was to apply a substrate to close the MH, prevent fluid from passing through the hole into the subretinal space, and allow tissue proliferation to achieve retinal restoration. Collecting ILM tissue for an autologous flap in the peripheral macula is difficult in myopic MH because of the concomitant posterior staphyloma and poor staining of ILM. Additionally, even an experienced surgeon may struggle to hold the flap in place during surgical maneuvers or fluid-air exchange. The autologous retinal patch is a more difficult surgical technique, as it requires longer surgical time and it presents a higher rate of intraoperative or postoperative complications, such as retinal detachment and vitreous hemorrhage.
On the other hand, the hAM is a basement membrane with anti-angiogenic and anti-inflammatory properties, well known in anterior segment reconstructive surgery. The application of the hAM in vivo for vitreoretinal pathologies, especially for the treatment of macular holes, is more recent and has demonstrated the induction of a recovery process involving the external retinal layers, such as the external limiting membrane and the ellipsoid zone. The advantages of the hAM plugs are the easy availability of the tissue, and the possibility to choose the required size with a cutaneous punch, depending on the size of the macular hole.
Caporossi et al. proposed the application of the hAM in subretinal space in patients with MHRD and they obtained complete retinal reattachment with MH closure in all of their cases. 11
A recent study by Moharram et al. reported for the first time the use of hAM in an epiretinal position in cases of recurrent retinal detachment secondary to myopic macular holes. 12 Then, Garcin et al. described the use of large diameter epiretinal lyophilized hAM in a cohort of 10 patients with recurrent or persistent macular holes associated or not with retinal detachment, reporting satisfactory visual recovery at one year. 13 Moreover, Qiao et al. reported an improvement in visual acuity in almost 90% of patients treated with an epiretinal hAM patch for MHRD in highly myopic patients following failed primary surgery. 14
Epiretinal implant of the hAM plug could be technically easier compared to subretinal implant and could present less possible intraoperative complications, such as plug dislocation within the subretinal space during the fluid-air exchange or during the subretinal fluid drainage. Furthermore, in our opinion, crucial differences are relevant in the present surgical technique compared to the previous abovementioned studies of hAM epiretinal implants.12,13,14 Creating a retinotomy could represent a substantial improvement. Instead of draining through the macular hole as performed by Moharram et al., indeed, a retinotomy allows the aspiration of the subretinal fluid in a less traumatic way, avoiding the risk of enlarging the macular hole or inadvertently touching the subfoveal RPE. Moreover, once the hAM is in place, the fluid-air exchange initially through the retinotomy and then at the margins of the PFCL bubble reduces any fluid turbulence which could determine a displacement of the implant (see
Limitations of this technique include the short follow-up to date on a limited number of cases. Our results show that this new surgical technique has the potential to improve visual function in MHRD in highly myopic patients. Further randomized controlled clinical studies involving a larger number of patients are needed to determine the impact this surgical technique could have in managing MHRD. In conclusion, hAM epiretinal implant could represent a novel surgical technique, feasible and easier compared to other current techniques used to treat primary MHRD in highly myopic eyes.
Conclusions
hAM epiretinal implant could represent a novel surgical technique, feasible and easier compared to other current techniques used to treat primary MHRD in highly myopic eyes.
Supplemental Material
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported in this publication was supported by Italian Ministry of health, RC-2023-2778765.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.