
Abstract
Purpose
To describe the anatomical and functional outcomes following use of the inverted flap technique (IFT) to close idiopathic macular holes (MH) of diameter greater than 400 μm. To compare the changes in the macular microvascularization following surgery in operated and healthy fellow eyes.
Methods
Retrospective study of 24 patients who underwent vitrectomy and IFT for large MH closure. The main variables were closure pattern, best corrected visual acuity (BCVA) and recovery of the external limiting membrane (ELM) and ellipsoid zone (EZ). Foveal avascular zones (FAZ) and vessel and perfusion densities, obtained by OCT angiography scans, were compared with those in healthy fellow eyes.
Results
Complete MH closure was achieved in 95.8% (23/24) of patients 6 months after surgery. There was a significant improvement in postoperative BCVA, from 1.0 to 0.4 logMAR (p < 0.001). The most frequent closure pattern was 1a (62.5%, 15/24), followed by 2c (12.5%, 3/24). The closure pattern was not correlated with height, minimum or maximum diameters or macular hole index (MHI) (p > 0.05). ELM and EZ recovery occurred in 87.5% and 83.3% of cases, respectively. FAZ were smaller in operated eyes than in the fellow eyes (p = 0.012). There were no differences in the vessel or perfusion densities between the operated and fellow eyes (p > 0.05).
Conclusions
Use of the inverted flap technique for large MH closure provides a high rate of functional and anatomical recovery. We observed a reduction in the FAZ following surgery, with no differences in the macular microvascularization parameters, suggesting that the technique is safe.
Keywords
Introduction
Idiopathic macular holes (MH) are caused by anteroposterior traction forces during posterior vitreous detachment, and they become enlarged due to tangential forces of the vitreoretinal interface and to cellular proliferation over the internal limiting membrane (ILM). 1 MH size is defined as the minimum horizontal diameter measured by OCT and is the most important prognostic factor for anatomical recovery after surgery. Large MH (>400 microns) often lead to persistent loss of photoreceptors, defects in the retinal pigment epithelium (RPE) 2 and worse outcomes. 3 Closure of MH by the inverted flap technique (IFT), first reported by Michalewska et al., 4 leads to better closure rates and visual outcomes than with conventional ILM peeling.
Although ILM removal promotes MH closure, it can cause thinning of the inner retina and a reduction in retinal sensitivity. 5 OCT angiography (OCTA) enables the detection of foveal microvascular changes following conventional ILM peeling, particularly a reduction in the area of the foveal avascular zone (FAZ), as described in several studies.6–9 However, few studies have addressed the changes following use of the IFT to close large MHs. In the present study, we examined the anatomical and visual outcomes following use of the IFT to treat large idiopathic MHs, and we compared the foveal microvascular features in the operated and healthy fellow eyes.
Methods
This retrospective case series included 24 patients who underwent pars plana vitrectomy and inverted flap technique (IFT) to treat a large idiopathic MH (minimum diameter of over 400 microns). All surgeries were performed between 2018 and 2021 at the University Hospital of Santiago de Compostela (Spain). This study adhered to the principles of the Declaration of Helsinki, and approval was obtained from the institutional ethics committee. Informed consent was obtained from patients prior to their inclusion in the study.
Eyes with a unilateral idiopathic MH of minimum diameter more than 400 microns were included in the study. The exclusion criteria were as follows: patients with bilateral MHs, secondary MHs, high myopia (axial length > 26 mm), coadjuvant procedures during macular surgery (e.g., platelet-rich plasma), other macular disease, a follow-up period of under 6 months, and eyes with significant media opacities which prevented correct image acquisition (signal strength <7/10).
Standard preoperative assessments were performed in all patients, including best corrected visual acuity (BCVA), slit-lamp examination, dilated funduscopy and macular OCT. The minimum, maximum and basal diameters, and height of MHs were measured using the Heidelberg Spectralis® software. The macular hole index (MHI) was calculated by dividing the MH height by its basal diameter.
The same routine examinations were performed postoperatively at one week, two weeks, one month, three months, six months and one year after surgery. We only compared preoperative and 6-month postoperative data to simplify the analysis. MH closure patterns 10 and recovery of the external limiting membrane (ELM) and ellipsoid zone (EZ) were determined by examination of from OCT scans at 6 months after surgery. Macular 3 × 3 mm OCTA scans (Zeiss Cirrus® HD-OCT 5000) were obtained at least six months after surgery in both eyes. The built-in AngioPlex™ software automatically measured the area (mm2) of the foveal avascular zone (FAZ) and quantified the perfusion density (PD) and vessel density (VD) of the superficial capillary plexus. VD is defined as the total length of perfused vasculature per unit area (mm−1), while PD is the total area of perfused vasculature per unit area (%). PD and VD were analyzed in the different Early Treatment of Diabetic Retinopathy Study (ETDRS) subfields (central 1 mm, inner -paracentral region-, full 3 mm). Manual adjustments were performed in some cases of erroneous FAZ detection.
Surgical technique
The surgery consisted of 25-gauge pars plana vitrectomy (PPV) and posterior hyaloid separation, followed by creation of a temporal internal limiting membrane (ILM) flap as reported by Michalewska et al. 11 Trypan blue and/or brilliant blue-G dyes were used to assist ILM peeling. Simultaneous cataract phacoemulsification and IOL implantation were performed when indicated. Vitreous fluid was replaced with sulphur hexafluoride (SF6) at the end of the procedure. All of the procedures were performed by the same senior retina surgeon (MJBT). Patients were instructed to maintain a face-down posture for 5–7 days. Dexamethasone and ciprofloxacin eyedrops were prescribed and tapered off over the first month after surgery.
Statistical analysis
All data were entered into a Microsoft Excel 2021 spreadsheet (Microsoft Corporation, Redmond, WA). The statistical analysis was conduced using the Statistical Package for Social Sciences software version 22.0 (SPSS Inc., Chicago, IL, USA). Qualitative data were compared using Chi-squared tests, and quantitative data were compared using the Mann-Whitney test. Paired variables were analysed using the Wilcoxon test. Differences in variables were considered statistically significant at P < 0.05. Continuous variables are expressed as median (range) and categorical data are presented as frequencies and proportions.
Results
A total of 37 patients were reviewed for eligibility and 24 patients with large unilateral MHs were included in the study. The mean age was 72.9 (7.2) years. Ten (41.7%) patients were male and 14 (58.3%) were female. Thirteen (54.2%) of the operated eyes were right eyes, and 11 (45.8%) were left eyes. Four (16.7%) patients had diabetes (but no diabetic retinopathy), three (12.5%) had undergone previous cataract surgery and one (4.2%) had controlled glaucoma. The mean axial length (AXL) was 23.6 (0.7) mm. 17 (70.8%) patients underwent combined phaco-vitrectomy, while 7 (29.2%) underwent PPV alone. Preoperative measurements included a mean maximum MH diameter of 1042.5 (315.4) microns, minimum diameter of 535.0 (150.5) microns, height of 429.5 (57.5) microns and MHI of 0.45 (0.16).
MH closure was detected at 7 days days postoperatively, with a 95.8% (23/24) closure rate at 6 months. The most frequent closure pattern was type 1a (62.5%, 15/24), followed by 2c (12.5%, 3/24) (Table 1). Recovery of ELM and EZ was observed in 87.5% and 83.3% of patients respectively (Figure 1). No correlations between the type of closure and the height, maximum and minimum diameters and MHI of MHs were observed (p > 0.05, Kruskal-Wallis test). BCVA improved in 22 patients (91.7%) and worsened in 2 patients (8.3%) following surgery (Figure 2). A significant improvement in BCVA was observed at 6 months after surgery, increasing from a median value of 1.0 (range 0.6–2.3) to 0.4 (range 0–2.0) logMAR (p < 0.001, Wilcoxon test).
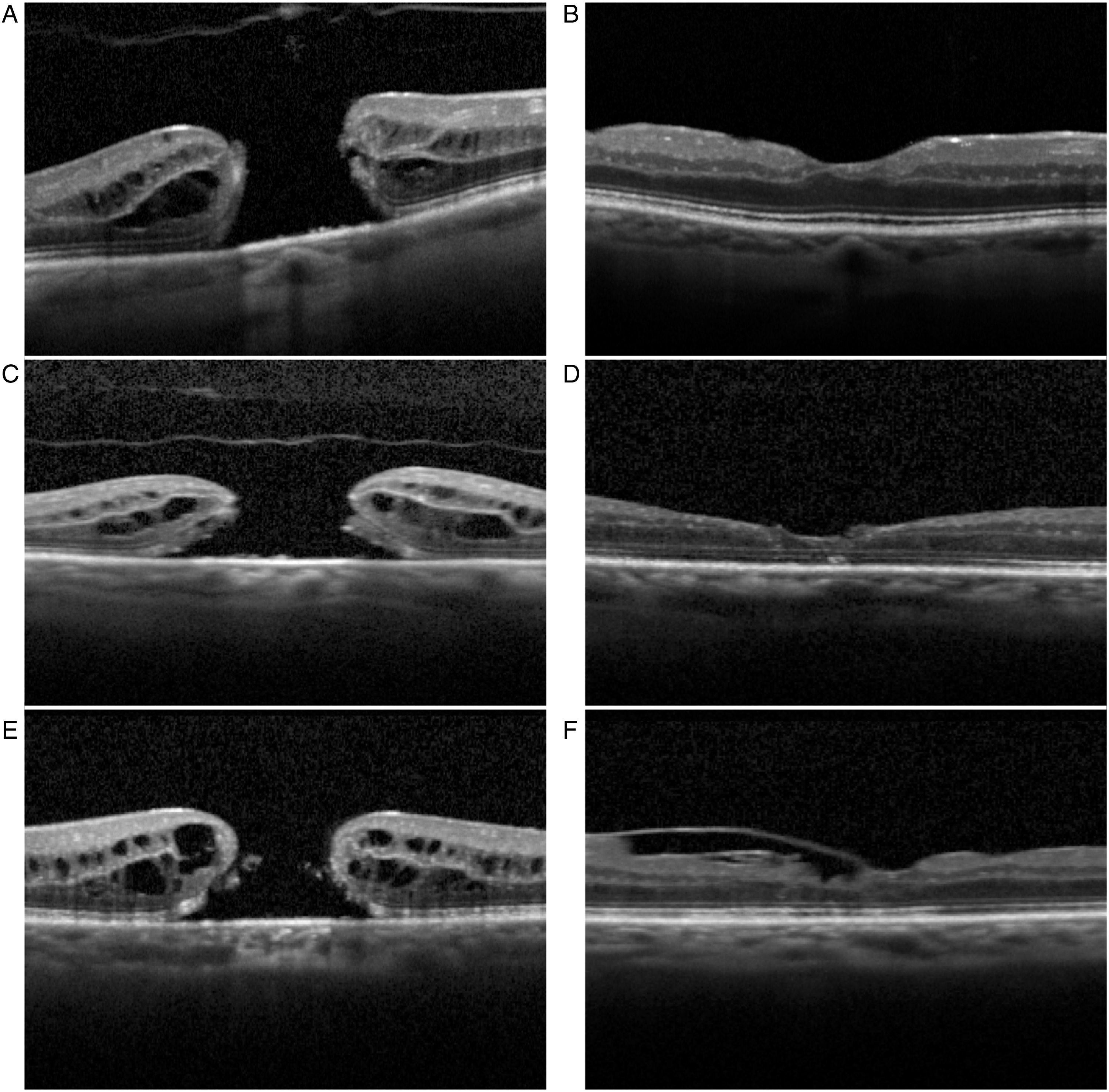
Preoperative and 6-month postoperative OCT scans of macular holes of >400 microns, showing complete ELM and ez recovery (type 1a closure pattern) (A, B); interruption of the internal layers (type 1c closure pattern) (C, D); and ILM flap scaffolding with reconstitution of outer layers (type 2c closure pattern) (E, F).
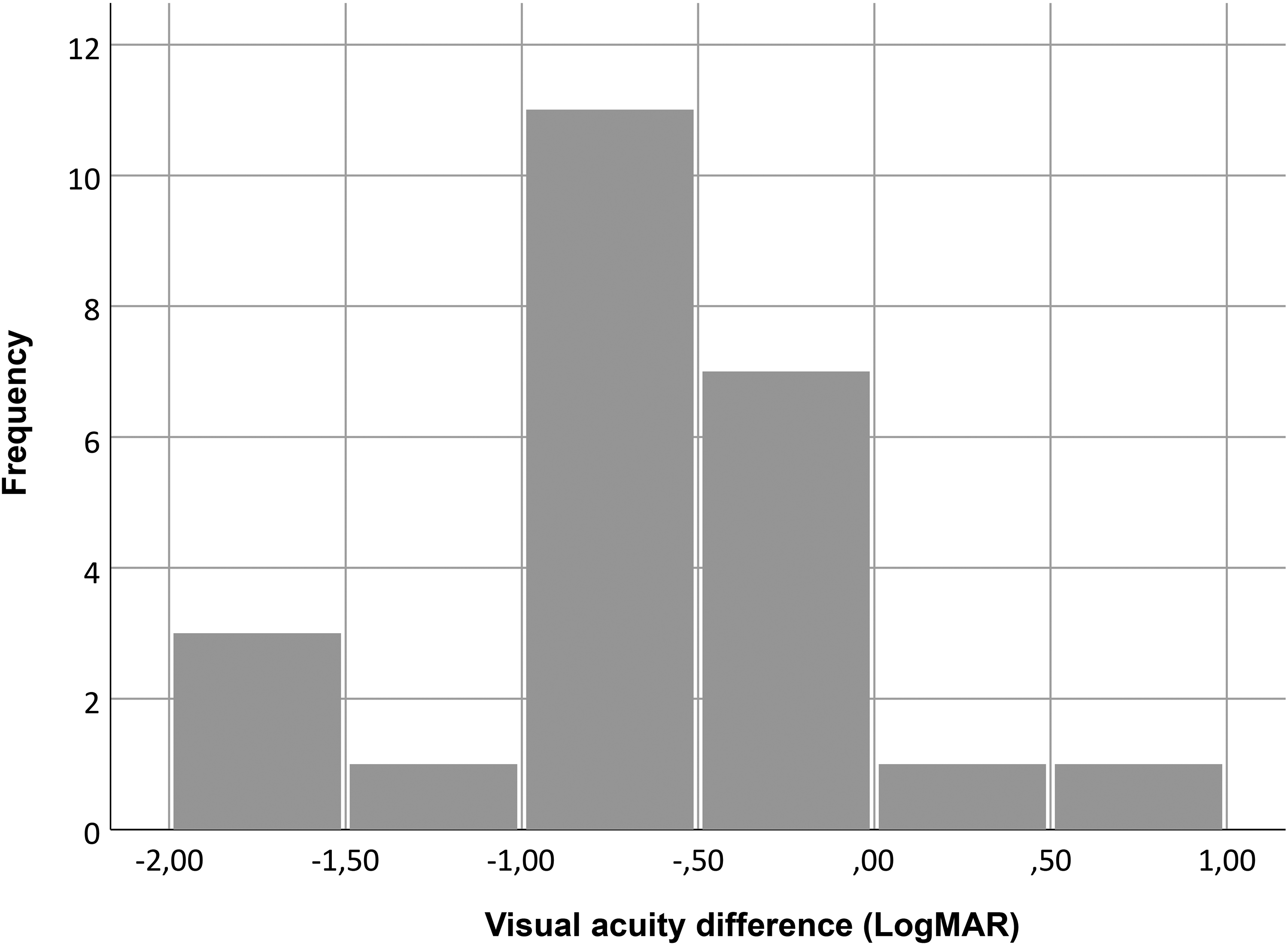
Histogram showing changes in visual acuity 6 months after surgery.
Macular hole closure patterns in our series.
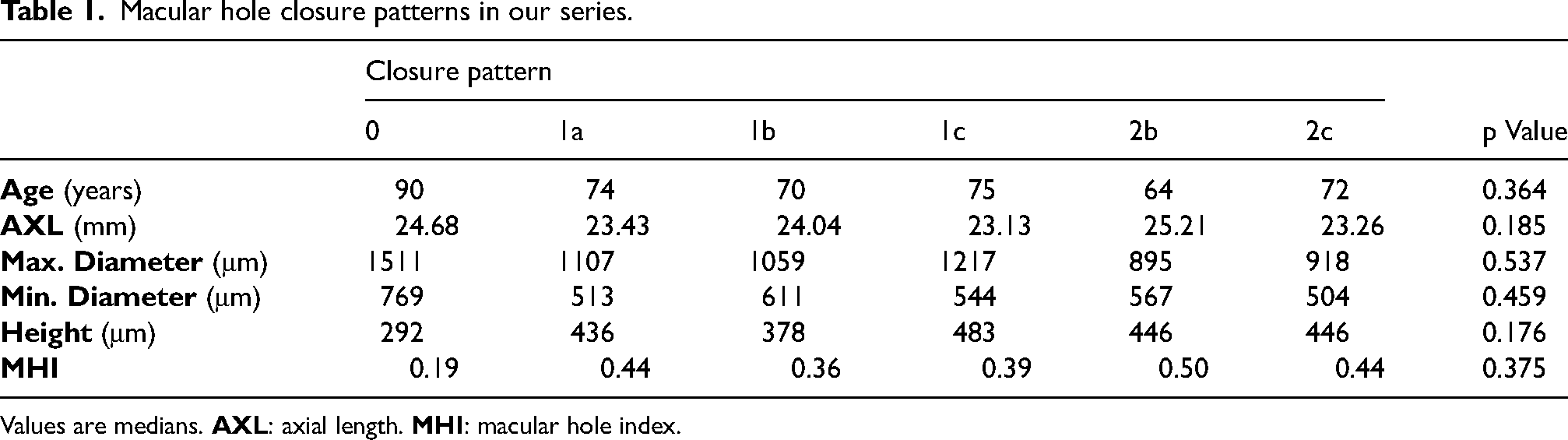
Values are medians.
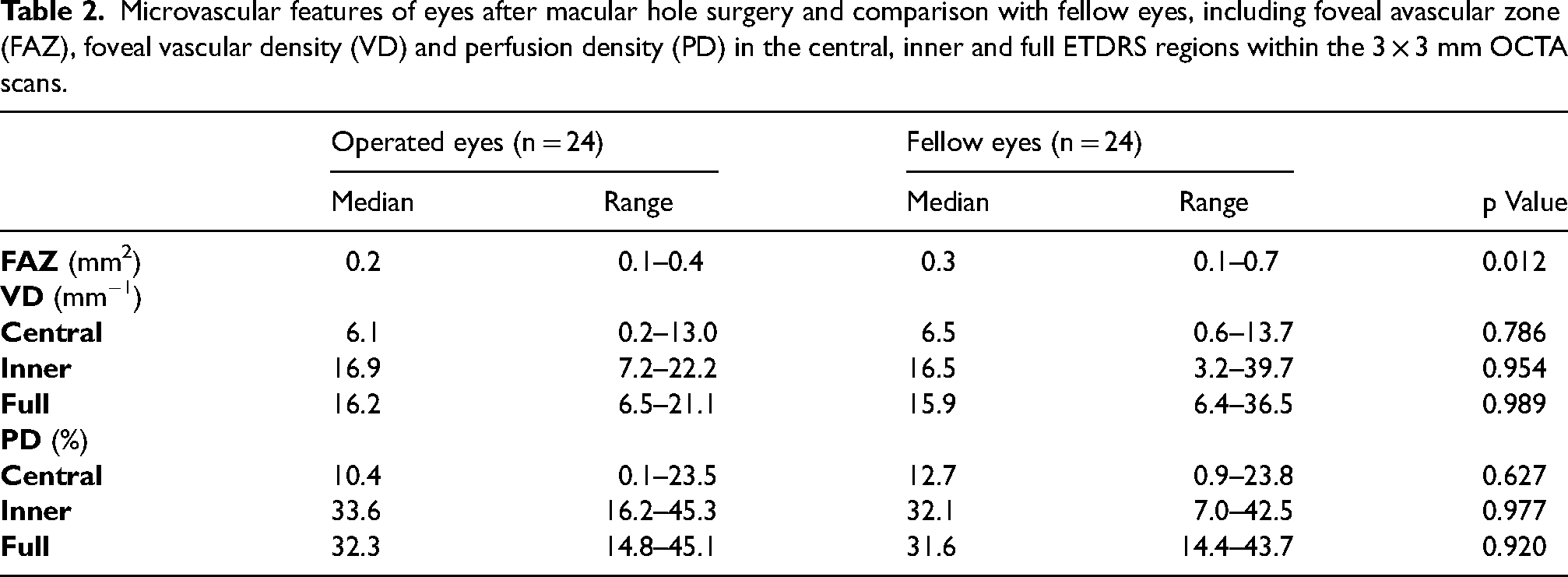
FAZ, VD and PD after surgery and in the fellow eyes are reported in Table 2. FAZ was lower in the operated eyes than in the fellow eyes (p = 0.012, Wilcoxon test) (Figure 3). There were no differences in the VD or PD of the operated eyes compared to the fellow eyes (p > 0.05, Wilcoxon test).
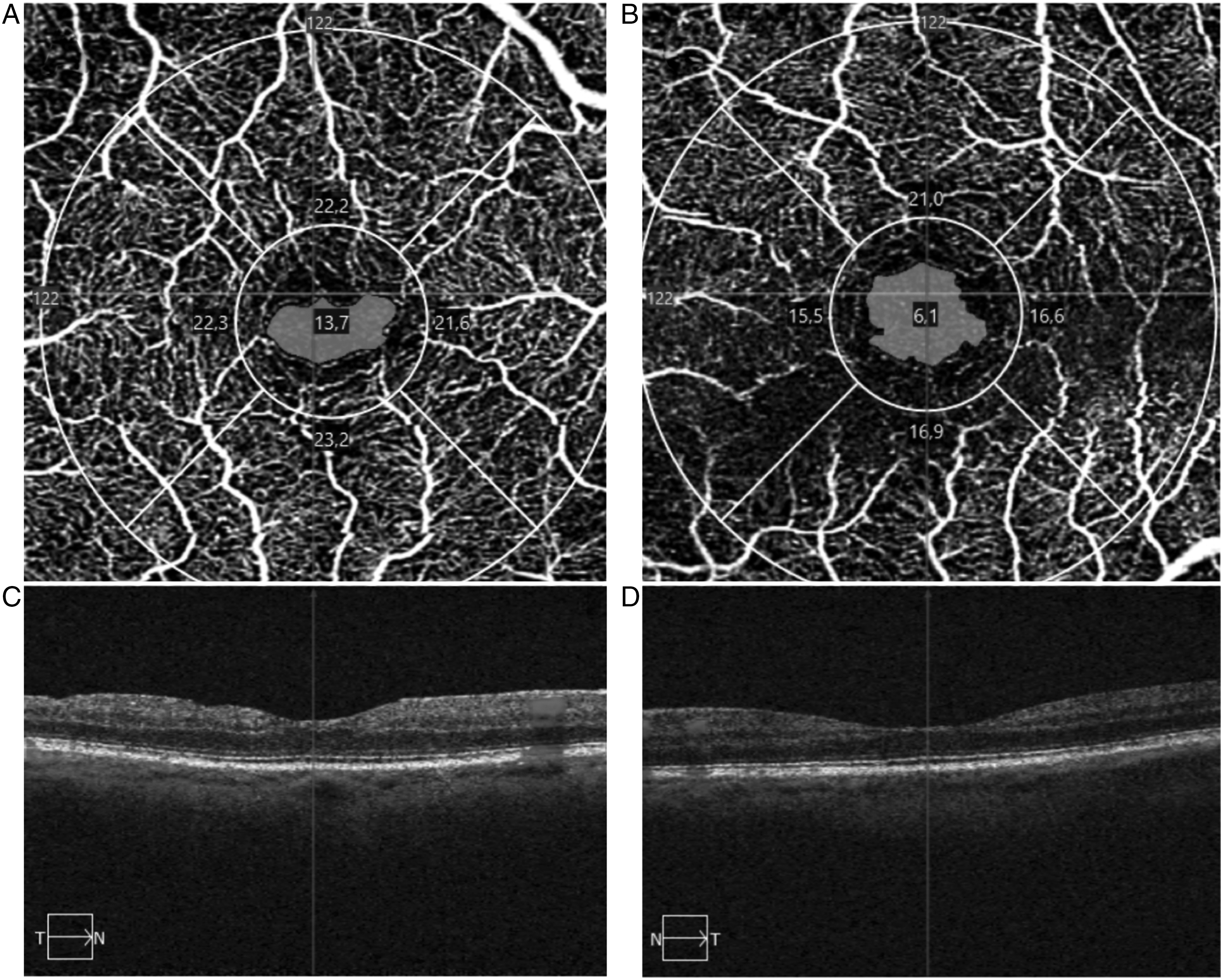
Macular 3 × 3 mm OCTA scans showing a smaller FAZ in the operated eye (A) than in the healthy fellow eye (C). Horizontal macular OCT scans of the operated eye (C) and the fellow eye (D).
Microvascular features of eyes after macular hole surgery and comparison with fellow eyes, including foveal avascular zone (FAZ), foveal vascular density (VD) and perfusion density (PD) in the central, inner and full ETDRS regions within the 3 × 3 mm OCTA scans.
Discussion
In the present study we observed good visual outcomes and a high rate of MH closure and EZ and ELM recovery in eyes with large MHs treated with the IFT. Post-operative OCTA scans revealed a decrease in the FAZ area, but no differences in the vessel and perfusion densities of the foveal superficial capillary plexus, relative to the healthy fellow eyes.
Michalewska et al. 4 first described the inverted flap technique (IFT), designed with the aim of improving the treatment outcomes for large MHs, in which closure rates were lower than for smaller MHs. Instead of completely removing the ILM, these researchers proposed peeling the ILM up to the temporal margin of the MH in order to create a flap which would be transposed nasally to cover the MH. ILM removal liberates perifoveal tangential forces and provides a scaffolding for cellular proliferation, promoting MH closure. 12 Our 95.8% closure rate after IFT is consistent with the rates reported in other studies. Michalewska et al. 4 described a closure rates of 98% for large MHs (relative to 88% with conventional ILM peeling). Several studies have confirmed the effectiveness of IFT and have described modifications to the original technique. Shin et al. 13 obtained a closure rate of 83% using a single-layer ILM flap (instead of the double layer described originally). Michalewska et al. 11 also developed a modified technique in which only the temporal ILM is peeled, with similar results. Andrew et al. 14 described folding part of the ILM inside the MH, and reported complete closure in all of the 24 eyes studied. We only considered patients who underwent the ‘cover’ technique, which requires less manipulation of the flap that the ‘fill’ technique, and also provides better visual outcomes.
Michalewska et al. 4 found that the most common closure pattern following IFT was a U pattern, which is often associated with better visual outcomes. Previous studies report MH closure according to the outdated U, V and W closure patterns. New surgical techniques and SD-OCT technology have lead to reclassification of closure patterns. 10 In our series, the most frequent closure pattern was type 1A (62.5%), showing reconstitution of the banded anatomy throughout all of the retinal layers. In the type 2 pattern, as the flap is placed to cover the MH void, in some cases some tissue interrupts the banded anatomy despite the MH being formally closed. This type of closure is not found after conventional ILM peeling.
We observed a significant improvement in BCVA, which increased from a median value of 1.0 logMAR preoperatively to 0.4 logMAR after surgery. Visual outcomes with IFT were also superior to those obtained with other techniques, as shown in several studies. In a prospective randomized study, Vélez-Montoya et al. 15 reported that IFT leads to faster visual recovery than conventional ILM peeling for large MH. Rizzo et al. 16 compared IFT with conventional ILM peeling and found that visual function only improved in the the IFT group after surgery. A meta-analysis by Gu et al. 17 concluded that IFT is functionally and anatomically superiority compared to other techniques, with closure rates of 95% with IFT (87% with other techniques) and visual improvement in 75% of patients (57% with other techniques). In our series, two patients (8.3%) had worse postoperative BCVA: one with an open MH and one who had a complete anatomical recovery. Visual function may not be fully restored following IFT even in the presence of complete anatomical recovery. This could be explained by the persistence of small defects in the ELM and EZ, although these may improve over time. 18 However, ELM and EZ defects have been described to be less frequent following IFT compared to other techniques. 19
Tangential forces present in MHs are hypothesized to cause a rarefied vascular network around the MH, prior to treatment. 20 ILM removal has been suggested to damage the retinal vasculature, and lower VDs have been described after conventional ILM peeling for MH closure than before surgery7,9,21 and relative to healthy fellow eyes, 8 particularly in the deep capillary plexus (DCP). When creating an ILM flap, the temporal parafoveal area that was peeled also showed lower VD in the DCP than in the nasal parafovea. 22 Nevertheless, Baba et al. reported an increase in VD after ILM peeling for MHs. 6 We did not find any differences in VD or PD between operated and fellow eyes. This may be explained by the smaller area that is peeled during IFT than in conventional ILM peeling, resulting in less mechanical trauma. As we used the AngioPlex™ software to quantify microvascular features, we did not have data on the deep capillary plexus (DCP). However, analysis of the superficial capillary plexus (SCP) seems to be more accurate and provides better diagnostic efficacy.23,24
We found that the FAZ was smaller in the operated eyes than in the fellow eyes. The FAZ may become smaller after surgery as tissues contract centrally and the MH is closed. 21 This occurs with both conventional ILM peeling and IFT. 21 Michalewska et al. 22 reported a decrease in FAZ after IFT, in eyes with small, medium and large MHs. Cho et al. 7 and Kim et al. 9 reported smaller FAZ after ILM peeling than in healthy fellow eyes. However, Demirel et al. 8 described a larger FAZ in eyes operated using the same technique.
The main limitations of this study were its retrospective nature and small sample size. Further developments in OCT angiography analysis may enable more precise detection of microvascular changes. Changes in macular microcirculation cannot be solely attributed to the specific surgical technique, as they may have occurred during development of the MH. OCTA scans obtained prior to the development of the MH would be necessary to clarify this aspect.
In summary, IFT provides a high rate of visual and anatomical recovery in eyes with large MHs. The FAZ area is smaller in operated eyes than in healthy fellow eyes. No changes were observed in parafoveal vascular density were observed, relative to fellow eyes, suggesting that the IFT is a safe technique causing minimal trauma.
Supplemental Material
sj-docx-1-ejo-10.1177_11206721231173004 - Supplemental material for Foveal microvascular features following inverted flap technique for closure of large macular holes
Supplemental material, sj-docx-1-ejo-10.1177_11206721231173004 for Foveal microvascular features following inverted flap technique for closure of large macular holes by David Lamas-Francis, Carmen Antía Rodríguez-Fernández, Manuel Bande and María José Blanco-Teijeiro in European Journal of Ophthalmology
Supplemental Material
sj-docx-2-ejo-10.1177_11206721231173004 - Supplemental material for Foveal microvascular features following inverted flap technique for closure of large macular holes
Supplemental material, sj-docx-2-ejo-10.1177_11206721231173004 for Foveal microvascular features following inverted flap technique for closure of large macular holes by David Lamas-Francis, Carmen Antía Rodríguez-Fernández, Manuel Bande and María José Blanco-Teijeiro in European Journal of Ophthalmology
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Summary statement
In this retrospective study we show that the use of the inverted flap technique to treat large macular holes provides a high rate of functional and anatomical recovery. A smaller FAZ was observed in the operated eyes, but the macular microvascularization parameters did not seem to be affected.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.