
Abstract
Keywords
Introduction
Although macular hole (MH)–associated retinal detachment is uncommon, it is one of the most vision-threatening surgical entities frequently associated with pathologic myopia. The pathogenesis of MH-associated retinal detachment remains uncertain, but proposed mechanisms include tangential traction from vitreoschisis within the residual posterior vitreous cortex, a hardened internal limiting membrane (ILM), inverse traction from posterior staphyloma, and weakened retinal adherence from choroidal and retinal pigment epithelium atrophy. 1 Treating MH-associated retinal detachment is challenging, and there is currently no consensus on the preferred surgical approach.
Various surgical approaches have been attempted to improve anatomic success in achieving both retinal reattachment and MH closure, including macular buckling, pars plana vitrectomy (PPV) with different ILM peeling techniques, scleral imbrication, and combined vitrectomy with scleral imbrication. Among these, PPV combined with ILM peeling techniques, such as conventional ILM peeling, ILM flap insertion, or free ILM flap, has gained popularity and has been shown to improve both anatomic and visual outcomes. The surgical technique, however, remains challenging, particularly when attempting to peel and manipulate the ILM over a detached macula. The unpredictability of ILM flap positioning at the conclusion of surgery adds further complexity to this condition.
In this study, we report on 2 young patients who developed MH-associated retinal detachment and describe a sequential approach for their management. In addition, we provide an overview of literature-documented cases of MH-associated retinal detachment, including presentation, surgical management, and outcomes. The pathogenesis and surgical management options of MH-associated retinal detachment are also discussed.
Methods
A chart review was conducted for 2 patients who developed MH-associated retinal detachment. Data collected included age, sex, and ophthalmologic examination findings, including dilated fundus examination, optical coherence tomography (OCT), and best-corrected visual acuity (BCVA), as well as surgical procedures and outcomes. Written informed consent was obtained from all subjects before the study. Institutional research ethics board approval was obtained from the University of Toronto. This study adheres to the tenets of the Declaration of Helsinki.
For the literature review, we analyzed published reports of patients who developed MH with concomitant retinal detachment. PubMed was searched using the key terms “macular hole” and “retinal detachment.” Inclusion criteria were: (1) the paper was written or translated into English, (2) the patient had a confirmed diagnosis of MH-associated retinal detachment on ophthalmologic examination, and (3) BCVA at the time of MH-associated retinal detachment diagnosis and at final follow-up, as well as a description of surgical techniques, were reported. Cases in which patients had additional peripheral breaks were eligible for inclusion if the retinal detachments were associated with the MH. Neither of the 2 cases in our series had peripheral breaks; the retinal detachments were associated with the MHs and confirmed on OCT and ultra-widefield fundus imaging. The selected studies were used to provide an overview of surgical management options for MH-associated retinal detachment. Mean values are ± SD.
Results
Case 1
A 57-year-old woman had a past ocular history of laser in situ keratomileusis in both eyes for high myopia, vitrectomy surgery for MH in the right eye, amblyopia in the right eye, and a full-thickness MH (FTMH) of greater than 400 µm, classifying it as large per the International Vitreomacular Traction Study. 2 On examination, vision was counting fingers in the right eye and Snellen 20/60 in the left eye. She subsequently experienced rapid progression to MH-associated retinal detachment secondary to FTMH in the right eye (Figure 1, A and B). Scleral depression examination confirmed no peripheral retinal breaks.
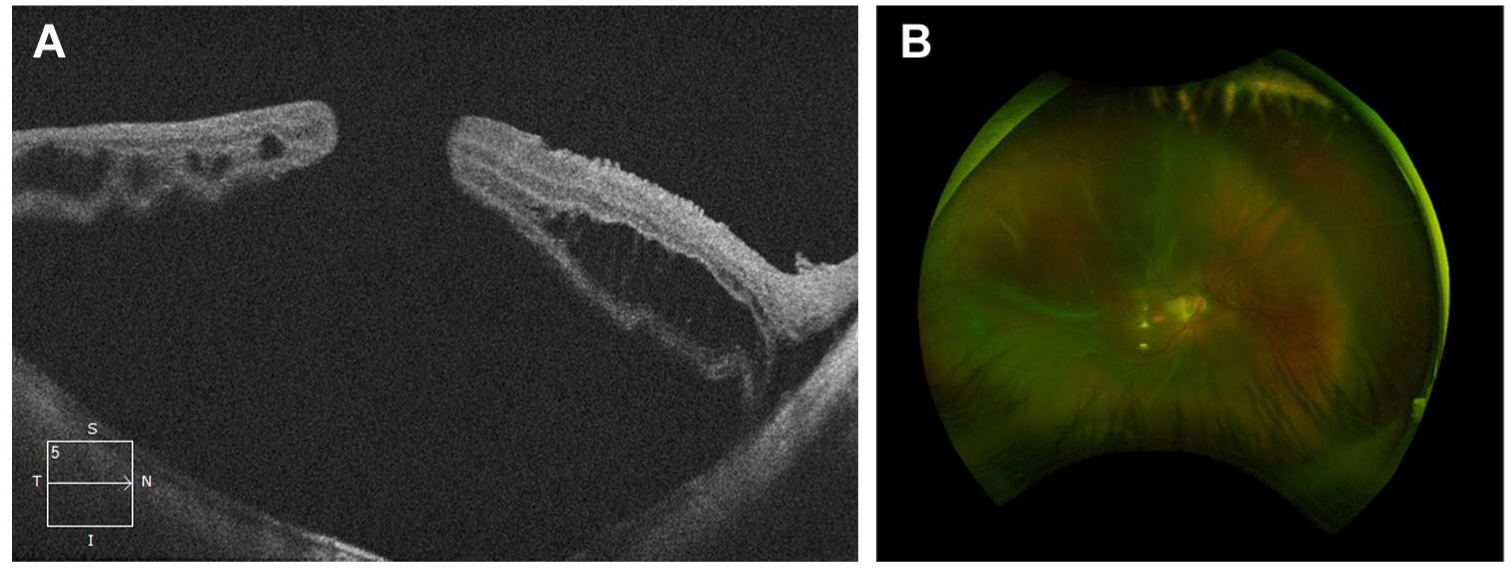
(A) Macular optical coherence tomography of the right eye showing retinal detachment associated with macular hole and subfoveal posterior staphyloma. (B) Fundus photo of the right eye showing retinal detachment with full-thickness macular hole.
A decision was made to perform pneumatic retinopexy with sulfur hexafluoride tamponade and subsequent face-down positioning to reattach the retina and macula before proceeding to vitrectomy surgery. The aim was to convert the macula-off total retinal detachment to an isolated MH. On day 5 following pneumatic retinopexy, the retina was completely reattached with a persistent MH (Figure 2, A and B), and the patient was scheduled for PPV. With limited ILM available secondary to pathological myopia and previous ILM peel surgery, an amniotic membrane was used to gently plug the MH. At 1-year follow-up, visual acuity (VA) was 20/200 OD and 20/30 OS. The retina was reattached with MH closure (Figure 2, C and D), and no vitreomacular traction was present postoperatively.
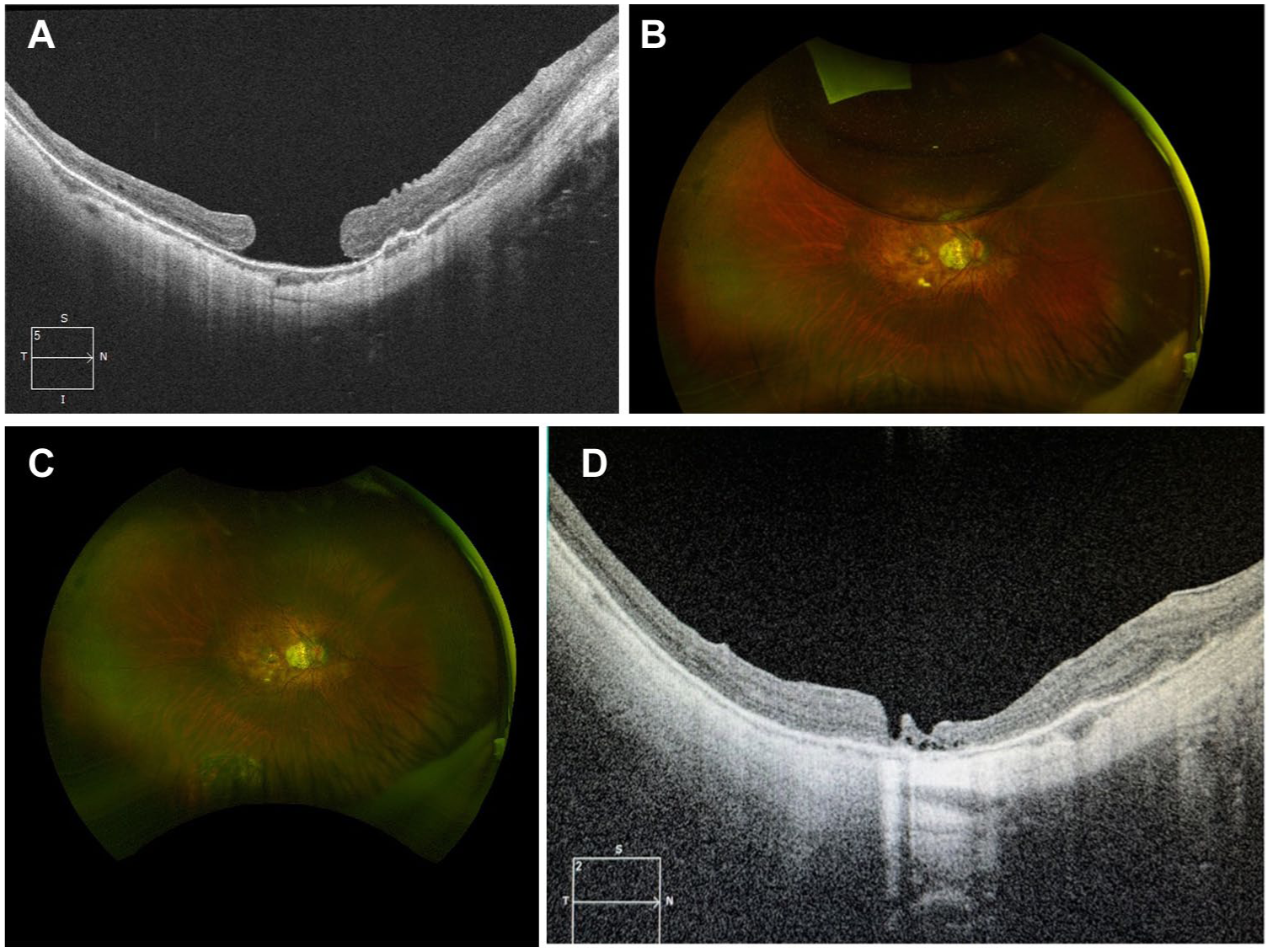
(A) Macular optical coherence tomography (OCT) of the right eye after pneumatic retinopexy showing reattached retina with macular hole (MH). (B) Fundus photo of right eye after pneumatic retinopexy, demonstrating retinal reattachment. (C) Fundus photo of the right eye following pars plana vitrectomy (PPV), showing retinal reattachment and MH closure. (D) Macular OCT of the right eye following pneumatic retinopexy and PPV, demonstrating reattached retina and MH closure with amniotic membrane.
Case 2
A 54-year-old woman had a past ocular history of bilateral laser in situ keratomileusis 20 years prior for pathological myopia (–10 D). She presented with a 5-day history of flashes and floaters in the left eye, along with a 1-day history of decreased vision, with VA of Snellen 20/500 OD and 20/100 OS. OCT confirmed a macula-off retinal detachment secondary to FTMH in the left eye (Figure 3). Scleral depression examination confirmed no other peripheral retina breaks. Pneumatic retinopexy with sulfur hexafluoride gas was performed, and by day 4 post-procedure, the macula was reattached with a persistent MH (Figure 4, A and B). The patient subsequently underwent PPV with membrane peel, inverted ILM flap, and sulfur hexafluoride endotamponade in the left eye, resulting in successful MH closure at follow-up (Figure 4). Final VA was Snellen 20/60 OS.
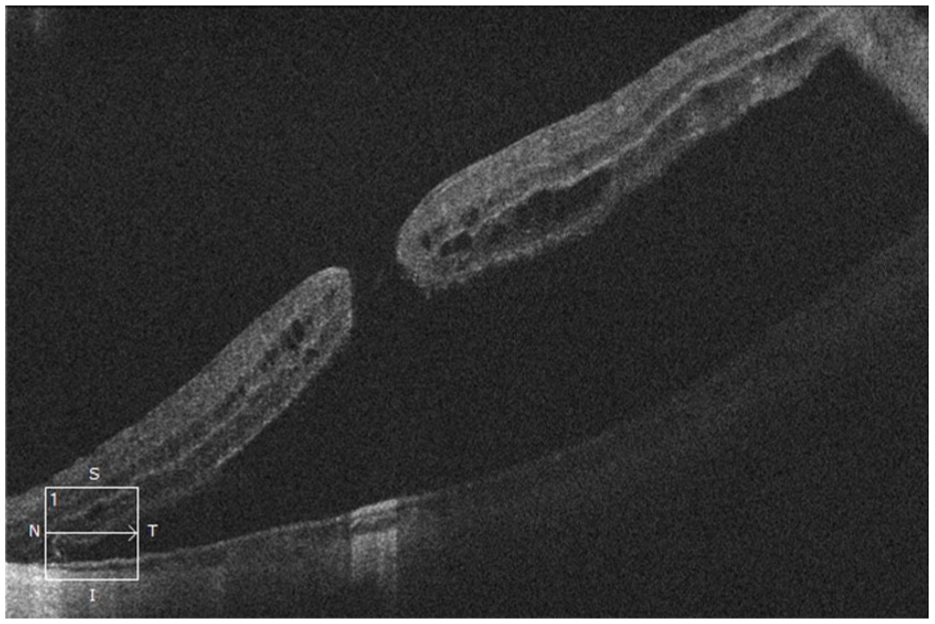
Macular optical coherence tomography of the left eye showing retinal detachment associated with macular hole.
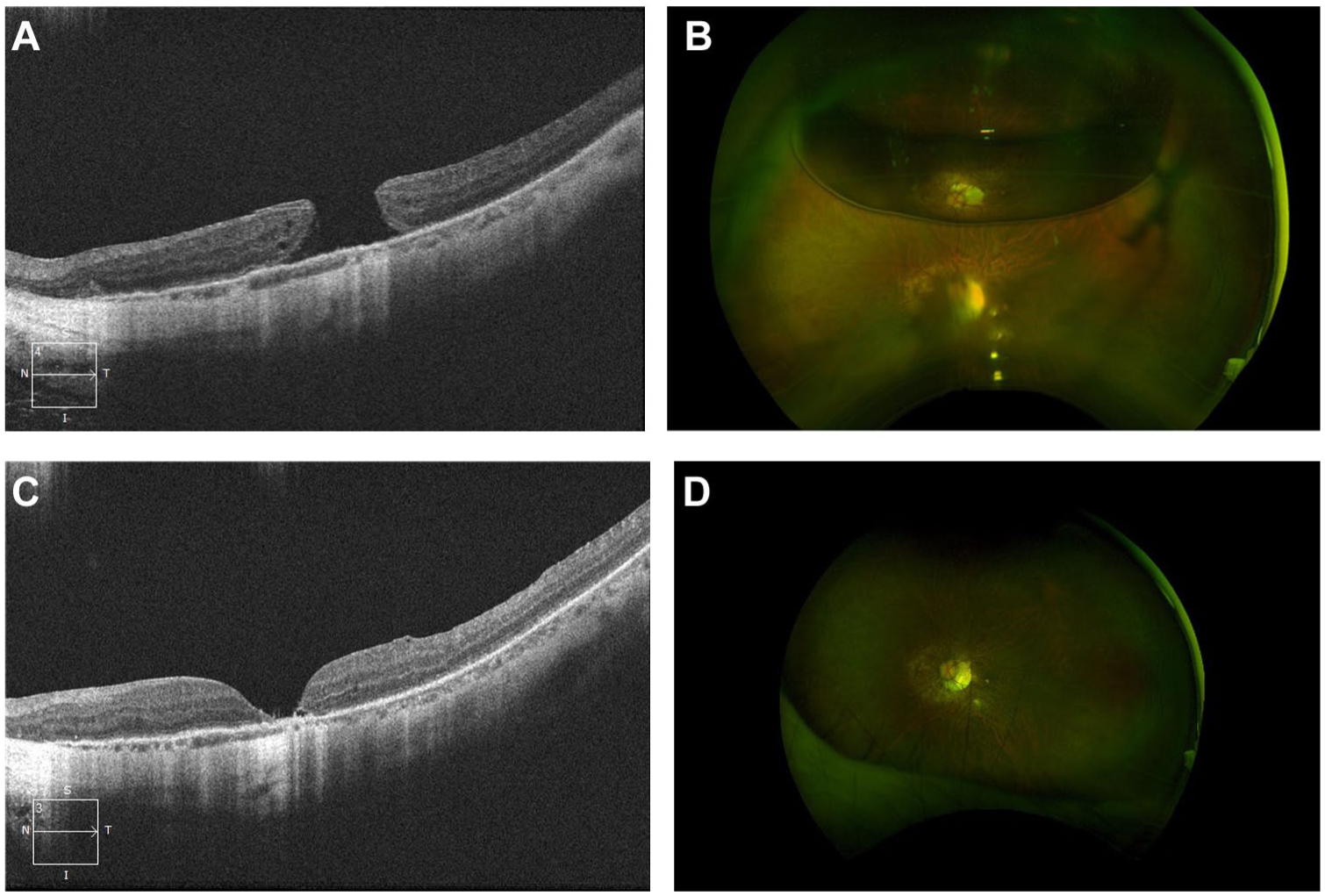
(A) Macular optical coherence tomography (OCT) of the left eye following pneumatic retinopexy showing retinal reattachment but persistent full-thickness macular hole (MH) with epithelial proliferation. (B) Fundus photo of the left eye after pneumatic retinopexy demonstrating retinal reattachment. (C) Macular OCT of the left eye demonstrating MH closure following pars plana vitrectomy (PPV). (D) Fundus photo of the left eye following PPV, demonstrating retinal reattachment and MH closure.
Literature Review
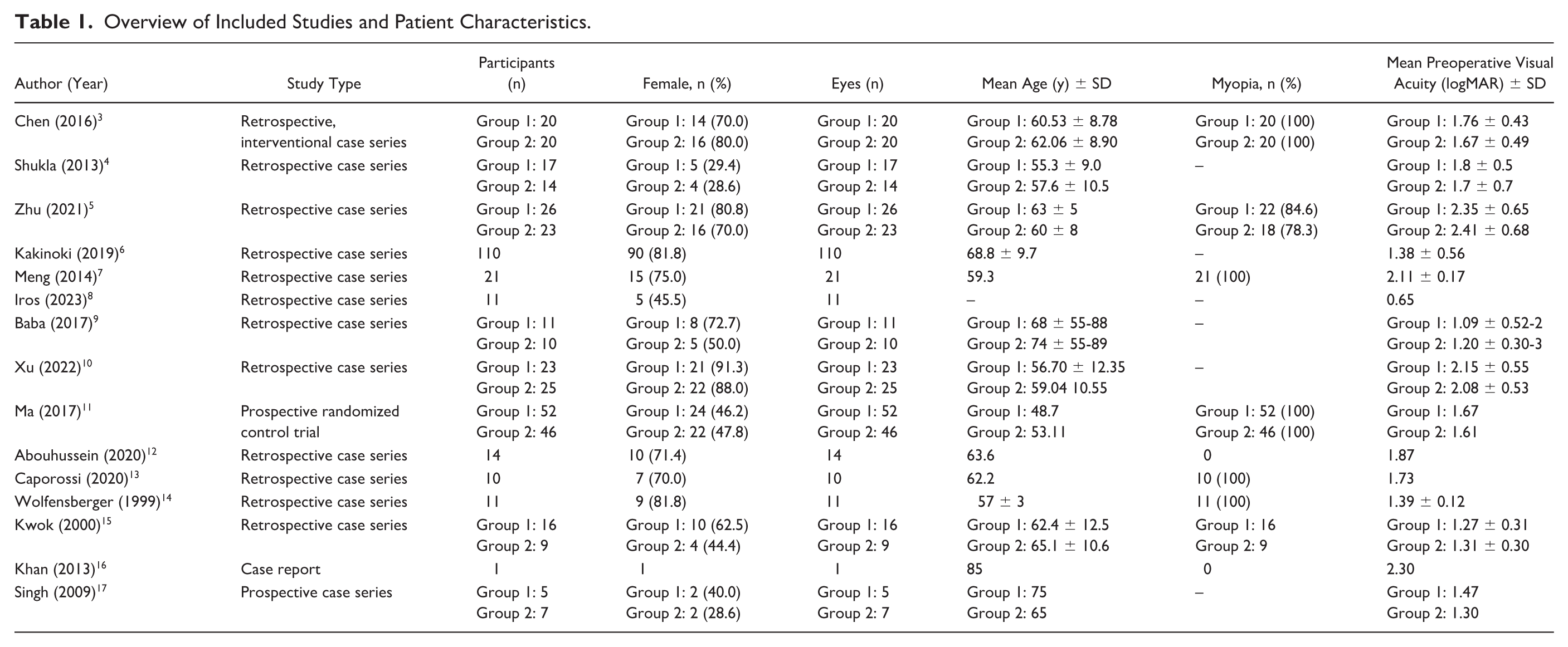
Our review consisted of 15 studies reporting on 502 cases (502 eyes) of MH-associated retinal detachment (Table 1).3–17 Of these, 65.0% (333/502) were female, with a mean age of 60.9 ± 6.9 years. Most cases were myopic (224/248 [90.3%]). The mean axial length of included eyes was 31.8 ± 7.8 mm. The mean VA prior to surgical intervention was 1.67 ± 0.38 logMAR. All patients underwent PPV to repair the retinal detachment. Eight eyes (1.6%) initially underwent vitrectomy to repair the retinal detachment, followed by a second surgery with ILM peel to close the MH.
Overview of Included Studies and Patient Characteristics.
All remaining eyes underwent combined surgery to repair MH-associated retinal detachment in a single procedure (Table 2). A total of 6.0% (33/502) underwent encircling scleral band buckle in addition to PPV, and 9.0% (46/502) underwent macular buckle in addition to PPV. A 23-gauge system was used in most cases (282/315 [89.5%]). Silicone oil was the tamponade agent used in nearly half of cases (204/450 [45.3%]). Indocyanine green was used to stain the ILM in 56.0% (195/344) of eyes, while Brilliant Blue G staining was used in 31.1% (107/344). Conventional ILM peeling was performed in 58.7% (295/502), an ILM flap inverted and then inserted into the MH in 10.6% (53/502), ILM peeled and inserted into the MH in 5.0% (26/502), and an ILM flap inverted and covering the MH in 11.0% (55/502). In 7.0% (36/502), laser photocoagulation was applied around the MH following vitrectomy. Lastly, 5.0% (24/502) underwent MH closure with an amniotic membrane plug.
Surgical Techniques for Management of MH Retinal Detachment in the Literature.
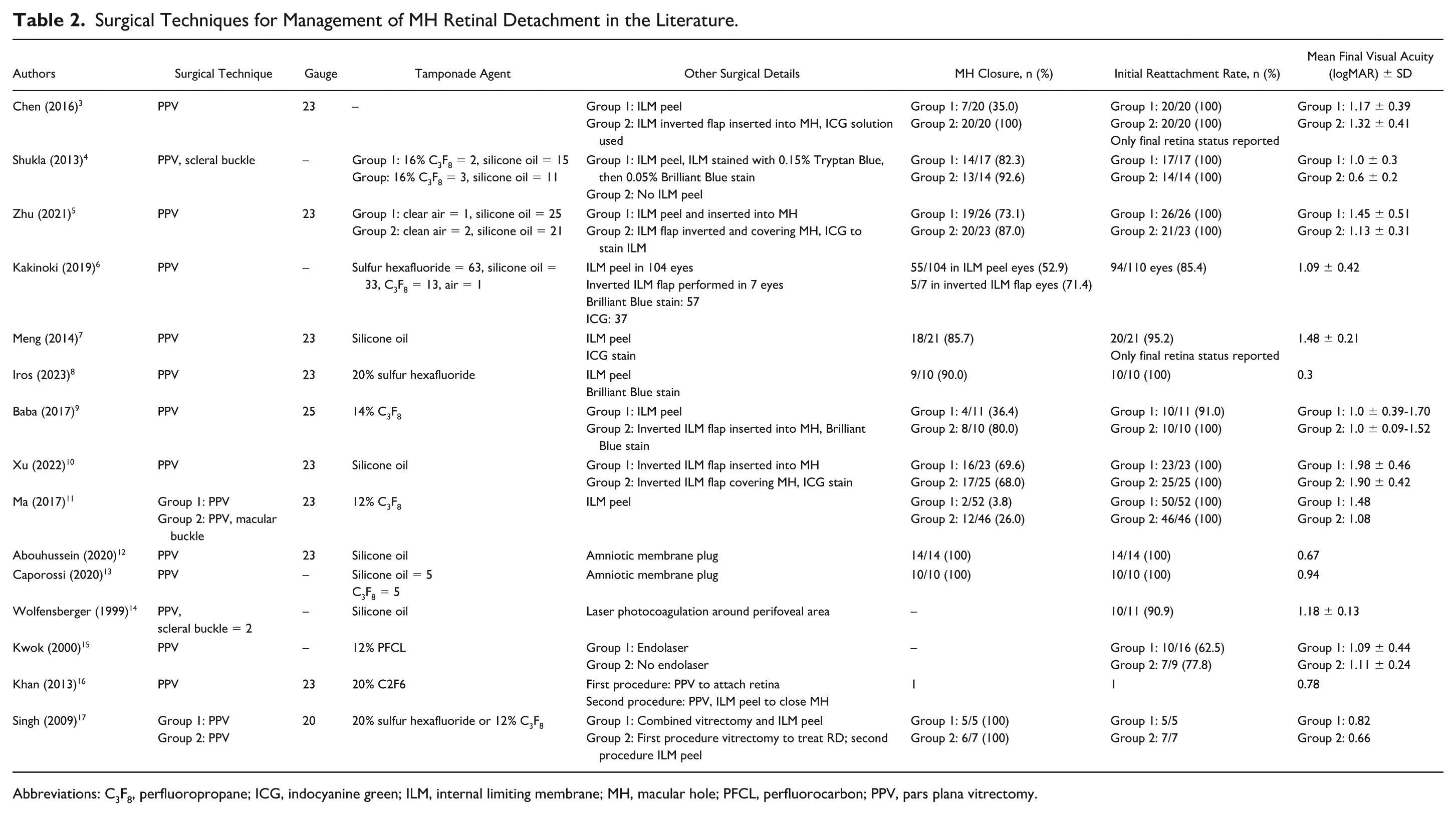
Abbreviations: C3F8, perfluoropropane; ICG, indocyanine green; ILM, internal limiting membrane; MH, macular hole; PFCL, perfluorocarbon; PPV, pars plana vitrectomy.
The overall MH closure rate was 63.9% (298/466), while the initial success rate of retinal reattachment was 95.1% (443/466). Eyes that received amniotic membrane plug achieved 100% MH closure (24/24), followed by ILM inverted flap inserted into the MH (44/53 [83.0%]), ILM inverted flap covering the MH (42/55 [76.4%]), ILM peeling and insertion into MH (19/26 [73.1%]), and conventional ILM peel (167/295 [56.6%]).
This was a retrospective chart review of 2 cases with MH-associated retinal detachment managed with a sequential surgical technique. In addition, a literature review was conducted to summarize management strategies for patients with MH-associated retinal detachment. The case report described 2 patients, both in their fifth decade of life with a history of pathological myopia, who developed retinal detachment secondary to FTMH. Initial treatment involved pneumatic retinopexy to reattach the retina, thereby converting emergent MH-associated retinal detachment into elective MH cases. Subsequent management of the MHs included PPV combined with either amniotic membrane plug or inverted ILM flap techniques to achieve hole closure.
The literature review encompassed 502 cases involving 502 eyes with MH-associated retinal detachment. Most cases occurred in females, consistent with prior reports indicating a higher prevalence of MH among females. 18 A total of 90% of eyes were myopic. All eyes underwent PPV for treatment of MH-associated retinal detachment, with some cases also undergoing scleral buckle or macular buckle.4,11,14 Less than 2% of eyes underwent sequential vitrectomy to repair the retinal detachment, followed by a second procedure with ILM peel to close the MH. The remaining eyes underwent combined MH-associated retinal detachment repair. Conventional ILM peeling was performed in most cases, while the next most common procedures were inverted ILM flap either inserted into or covering the MH. In a minority of cases, an amniotic membrane plug was used to close the MH.12,13 Two studies reported the use of laser photocoagulation around the MH following vitrectomy. The overall MH closure rate was 64.0%, with 100% closure in eyes that received an amniotic membrane plug. The retina was reattached in 95.0% of cases.
MH-associated retinal detachment is a significant complication of highly myopic eyes, characterized by posterior outpouching of the globe and elongation of the ocular axial length. The occurrence of MH in highly myopic eyes has been attributed to several factors, including tangential traction by the vitreous cortex, centripetal force from the ILM, retinal thinning, and the formation of posterior staphyloma. 19 Posterior vitreous detachment, particularly when causing vertical traction at the posterior segment, is also believed to significantly contribute to retinal detachment. 20
In the literature review, more than half of patients undergoing surgical repair of MH-associated retinal detachment had an ILM peel performed during the initial procedure. However, performing an ILM peel over a detached macula poses a significant challenge. Manipulating the ILM to plug the MH or to position a flap over it, particularly during air-fluid exchange, can also be difficult. The final position of the ILM flap may remain unpredictable at the conclusion of surgery. Although not always required, the decision to drain subretinal fluid, either through the preexisting MH or via drainage retinotomy, adds further complexity. Endolaser photocoagulation around the drainage site may inadvertently damage the retina or choroid and induce local inflammation. Collectively, these challenges underscore the complexity of managing MH-associated retinal detachment and emphasize the importance of careful surgical technique.
The present 2 cases illustrate the use of pneumatic retinopexy as a quick, office-based procedure to facilitate retina reattachment without the need for retinotomies or enlargement of the MH. Using this sequential approach, emergent and complex cases of MH-associated retinal detachment were effectively transformed into elective MH cases, which were then repaired with traditional PPV combined with either an inverted ILM flap or amniotic membrane technique. Blankenship and Ibanez-Langlois 21 described the use of intravitreal gas exchange to reattach the retina in 19 eyes. In that study, 12 retinas were successfully reattached with the initial exchange, while 4 retinas required subsequent exchange or PPV for reattachment. Similarly, Menchini et al 22 reported the use of pneumatic retinopexy followed by postoperative positioning in 9 eyes with retinal detachment owing to MH. Of these, 7 eyes (77.8%) achieved reattachment within a mean of 3 days, with associated improvement in VA. The 2 eyes that did not reattach had visible vitreous strands adherent to the posterior pole.
Since the introduction of PPV for treating MH-associated retinal detachment, several additional techniques have been developed, including silicone oil tamponade, epiretinal membrane peeling, ILM peeling, and the inverted ILM flap. Among these, PPV combined with intraocular gas or silicone oil tamponade and ILM peeling are the most widely used procedures for MH-associated retinal detachment, as demonstrated in our literature review. The reported closure rate of MH-associated retinal detachment following vitrectomy and ILM peel ranges from 35.0% to 70.0% after a single procedure, consistent with our findings.9,23–27
Additional techniques include the inverted ILM flap, which can be positioned to cover or insert into the MH. The concept involves peeling the ILM while preserving a portion of the tissue at the edge of the MH; the peeled segment is then folded back, either covering or inserted into the MH after trimming. 10 Human amniotic membrane patches have also been used to treat MH coexistent with retinal detachment. In complex MH surgeries, the use of amniotic membrane is supported by its anti-inflammatory, antifibrotic, and tissue-regenerating properties. Human amniotic membrane functions as a basement membrane substrate that supports cellular growth, 12 and it also expresses cytokines and growth factors that promote epithelization, reduce adhesions, and enhance healing.
Our study demonstrates a stepwise surgical technique for treating MH-associated retinal detachment, using preoperative pneumatic retinopexy to reattach the retina and macula and thereby convert an emergent complex MH-associated retinal detachment into an elective MH case. This approach facilitates retinal reattachment, provides greater control of the ILM, avoids the need for perfluorocarbon liquids, minimizes trauma to the nerve fiber layer, and allows better control of inverted flap techniques or amniotic membrane allocation. We acknowledge that this technique may not be the treatment of choice for all patients, as it requires 2 procedures rather than 1 and prolonged postoperative positioning. Nonetheless, this study highlights an alternative surgical approach to managing MH-associated retinal detachment that is not well documented in the literature.
We recognize that a case series of only 2 patients may appear limited. However, owing to the rarity of retinal detachment with MH and the specific inclusion criteria of our study (MH-associated retinal detachment cases managed with pneumatic retinopexy followed by PPV), it was challenging to identify additional cases. This highlights the significance of our report. Our objective was not to claim superiority or equivalence of this technique over standard procedures, but rather to present a potential management option that our team has successfully used.
This technique may offer a viable alternative for converting MH-associated retinal detachment into a more manageable MH surgery, which could be beneficial for clinicians encountering similar cases. Further studies with larger sample sizes are needed to rigorously evaluate this approach before it can be considered for widespread adoption. Nonetheless, this strategy may help surgeons simplify the management of MH-associated retinal detachment by first converting it to MH alone. Future research should focus on comparing outcomes of the sequential approach of pneumatic retinopexy followed by PPV vs PPV alone for the management of MH-associated retinal detachment.
Conclusions
This study presents a sequential approach for MH-associated retinal detachment using preoperative pneumatic retinopexy, demonstrating favorable outcomes in a limited case series. The accompanying literature review provides an overview of current surgical strategies for MH-associated retinal detachment. While acknowledging the limitation of a small sample size, this report suggests that preoperative gas placement may be a beneficial addition to the management of MH-associated retinal detachment. Further research with larger cohorts and comparative analyses is required to validate the efficacy and safety of this innovative technique and to inform the continued evolution of vitreoretinal surgery.
Footnotes
Ethical Approval
This case report was conducted in accordance with the Declaration of Helsinki. The collection and evaluation of all protected patient health information was performed in compliance with the Health Insurance Portability and Accountability Act. Ethical approval for this study was obtained from the University of Toronto Research Ethics Board.
Statement of Informed Consent
Informed consent was obtained prior to the procedures, including permission for publication of all photographs and images included in this report.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received no financial support for the research, authorship, and/or publication of this article.