
Abstract
Purpose
To describe the unexpected one-year course of a probable Tobacco Alcohol Optic Neuropathy (TAON) and the unprecedented Laser Speckle Flowgraphy (LSFG) assessment.
Case Report
A 49-year-old Caucasian man with no family history of visual impairment referred because of unilateral and painless visual acuity (VA) decrease in the right eye (RE). Also, color vision and visual evoked potentials were unilaterally altered. Optical coherence tomography (OCT), instead, revealed bilateral thinning of the macular ganglion cell inner plexiform layer. Funduscopy, intraocular pressure, pupillary shape/reactivity and ocular motility were normal. Blood testing revealed macrocytic/normochromic anemia and low levels of vitamin B2 and folic acid. The patient admitted heavy tobacco and alcohol intake for many years. After an initial compliance to the prescribed regimen, the patient quitted the vitamin intake and resumed his smoking and drinking habits. After a 13-month follow up the VA further reduced in the RE; the fellow eye preserved normal visual function despite the bilateral and progressive alterations of the OCT assessment. Both eyes underwent LSFG examination. All the conventional nets evaluated by the instrument (i.e., Mean Tissue, Mean All and Mean Vascular perfusion) were lower in the RE.
Conclusions
Based on patient's behavior, visual deficiencies and laboratory findings, we assumed that the patient suffered from TAON. Also after one year, however, a deep discrepancy between the strictly unilateral, progressive VA impairment and the bilateral, symmetrical OCT alterations persisted. The LSFG data clearly indicate that the perfusion of the two eyes differed, especially referring to tissular vascularization in the optic nerve head area of the RE.
Introduction
Tobacco alcohol optic neuropathy (TAON) also known as tobacco alcohol amblyopia, is an obsolete term for a rare condition characterized by visual impairment from tobacco and alcohol abuse, usually associated with nutritional deficiencies. Currently, a more precise term in use is nutritional optic neuropathy. It is generally attributed to the toxic effects of cyanide and B12 deficiency.1–3 Recent studies have shown that the disease includes various visual disturbances caused by toxins and nutritional deficiencies of B vitamins, copper, methionine, folic acid, and/or antioxidant carotenoids. Also, heavy smokers/alcoholics can develop a characteristic bilateral visual impairment called TAON. Typically, TAON causes fairly symmetrical visual loss that is painless, sub-acute, and bilateral. The related functional alterations often include dyschromatopsia, loss of contrast sensitivity at high frequencies, and central or centrocecal scotoma. Fundoscopy reveals progressive anomalies of the optic nerve head (ONH), until late atrophy. In TAON patients, a few optical coherence tomography (OCT) studies have described symmetrical thinning of the circumpapillary retinal nerve fiber layer (cpRNFL). This thinning tends to first involve the inferotemporal sector and then extend circularly.2,4,5 Also, TAON is a disease entity that is not only underdiagnosed but also often diagnosed at a stage when recovery of vision is not possible. Both genders and all races are equally affected, and all ages are susceptible. 7
Laser speckle flowgraphy (LSFG) is a relatively new technique for exploration of ONH perfusion in a clinical setting that is both patient friendly and yields real-time data.6,8 LSFG quantifies blood flow on the basis of speckle optic phenomena; the main output parameter is the mean blur rate (MBR), which is a measure of the relative blood flow velocity in arbitrary units.
Here, we present an atypical TAON case and describe the LSFG findings; the latter have never been reported for any TAON patient.
Case report
A 49-year-old Caucasian man was referred to our ophthalmology clinic (in the University Hospital of Parma, Italy) because of a unilateral and painless visual acuity decrease in the right eye (RE) that had commenced 4 days previously. The RE best-corrected visual acuity (BCVA) was 0.2 LogMAR (left eye [LE] 0.0 LogMAR); but intraocular pressure, pupillary shape and reactivity, and ocular motility were all normal. Fundoscopy yielded no significant finding, too. However, OCT revealed bilateral thinning of the macular ganglion cell inner plexiform layer (GCIPL) but the central retinal nerve fiber layer thickness was normal apart from borderline temporal sector thinning. The visual field (30–2 Swedish Interactive Testing Algorithm Standard of the Humphrey Field Analyzer II-I) revealed a mild foveal threshold decrease in the affected eye (RE 24 dB, LE 35 dB, Figure 2a, 2b). The RE visual evoked potentials (VEPs) exhibited reduced amplitudes and increased latencies at high frequencies (15 Hz) (Figure 1). The Farnsworth-Munsell Dichotomous D-15 test for color vision revealed protanopic anomalies specifically in the RE. There was no family history of visual impairment.
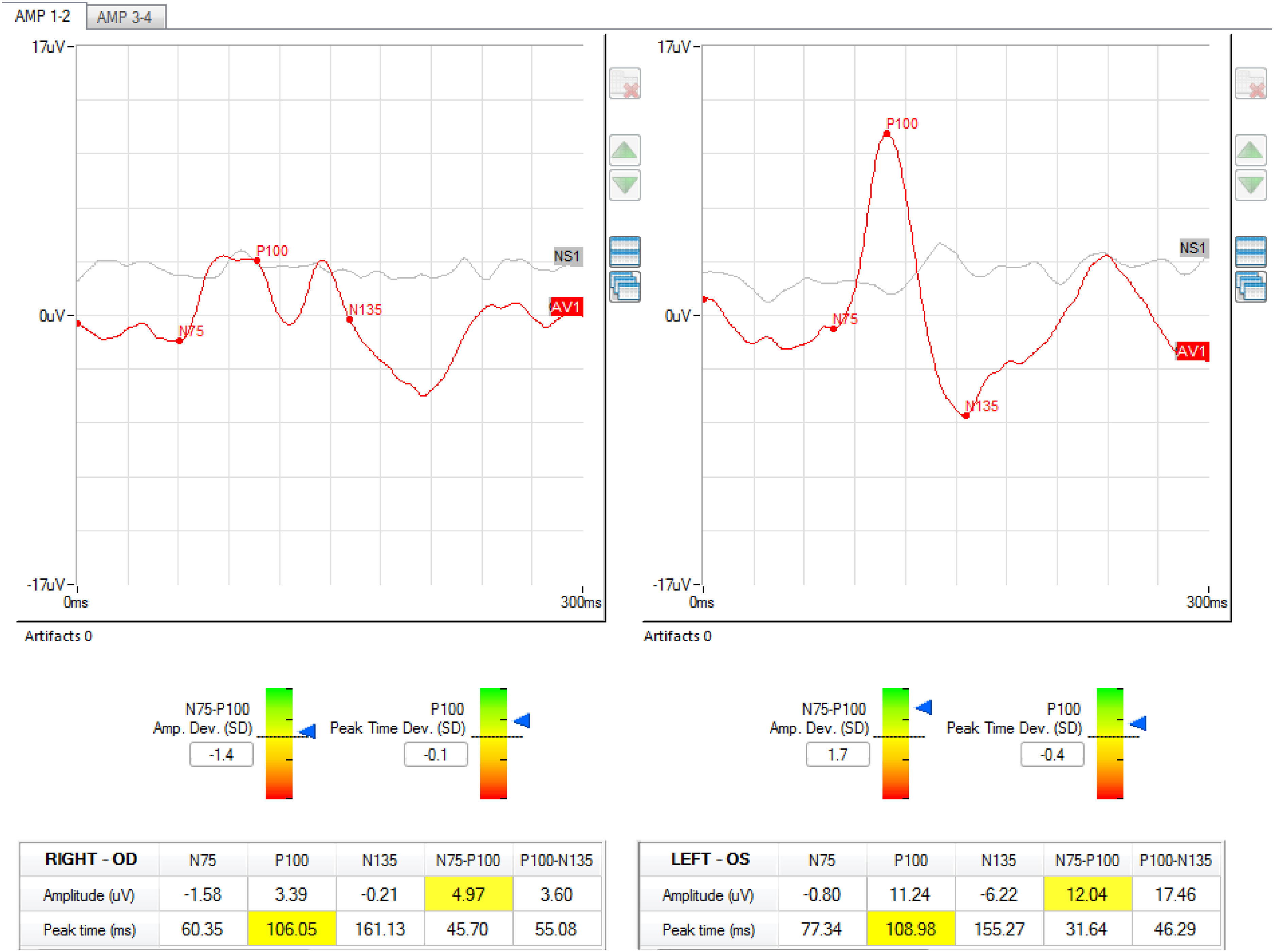
Visual evoked potentials results at the beginning of the follow up. The right eye registration (left side) showed reduced amplitudes and increased latencies.
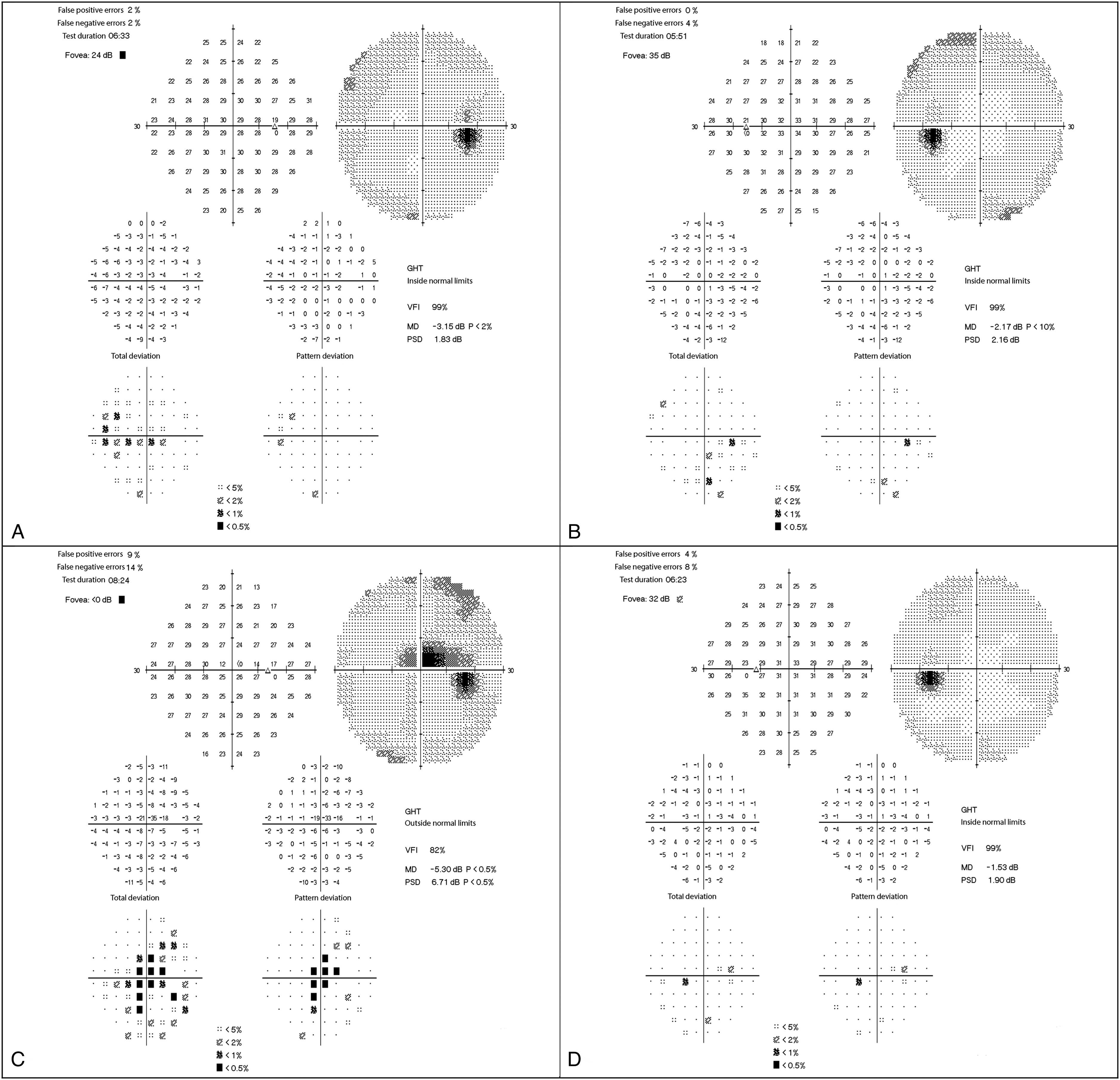
(A-D): Composite of the 30:2 visual fields of the A) right eye and the B) left eye of the patient at the beginning of the follow up and of the C) right eye and D) left eye after a 13-month follow up. At the first evaluation, the only finding was a mild decreased foveal threshold in the right eye. After 13-months, the foveal threshold of the right eye was absent and a central-centrocecal visual field defect was evident. The left eye was not affected at any stage of the follow up.
The patient denied drug/medication use but revealed that he has smoked approximately 40 cigarettes/day for 20 years combined with excessive alcohol consumption, in particular he confirmed a daily intake of beer (500 mL; 4–6% [v/v] alcohol); white wine (1,000 mL 12–14% [v/v] alcohol); liqueur (100 mL 25% [v/v] alcohol); and red wine (500 mL 12–14% [v/v] alcohol), accompanied by a poor diet completely devoid of fruit and vegetables. Blood analyses revealed macrocytic/normochromic anemia and low levels of vitamin B2 (130μg/L; normal range: 137–370 μg/L) and folic acid (2.2ng/L; normal range:3.1–19–9ng/L). We found no infectious or autoimmune disease that might affect the optic nerve, no elevation of any inflammatory marker, and no SARS-CoV2 or HIV infection. Brain magnetic resonance imaging was normal. The patient refused genetic evaluation. We suspected TAON and prescribed oral vitamins (200 mg B1, 300 mg B6, 1,000 mg B12, and 400 μg folic acid/day). Over the next 3 months, the patient assured us that he took the vitamins regularly and reduced his alcohol and tobacco consumptions. At the 4-month follow up, the BCVAs did not change significantly (0.24 LogMAR in the RE and 0.0 LogMAR in the LE), and neither did the OCT or visual-field data. At the last evaluation (13 months after the first visit), however, the patient reported that he resumed his high alcohol intake and ate little. The RE BCVA fell to 1.0 LogMAR but the LE remained at 0.0 LogMAR; intraocular pressure was normal. The visual field test was also altered in the RE, showing a central-centrocecal scotoma, and normal in the LE (Figure 2c, 2d). The funduscopic aspect of RE ONH was unaltered and similar to that of the fellow eye (Figure 3a). OCT confirmed the bilateral and symmetrical thinning of the macular GCIPL (Figure 3b) and that of the cpRNFL in the sole temporal sector (Figure 3c); both areas were thinner than the baseline values. Color testing revealed a shift to deuteranopic anomalies in the RE. During this latter visit, both eyes were subjected to LSFG (LSFG-RetFlow; NIDEK) (Figure 3d). Briefly, in color-scale maps, regions of higher blood flow appear white/red and regions of lower blood flow appear blue/black. An elliptical rubber band centered on the ONH yields the mean blur rates (MBRs) of the entire area and of each quadrant. The LSFG parameter mean vascular (MV) is the average MBR of all white/red pixels regions, thus those of the larger vessels supplying the retina (i.e., the vascular area). The LSFG parameter mean tissue (MT) is the average MBR of all blue/black pixels regions, thus of areas with microvascular networks supplying the ONH (i.e., the tissue area). The parameter mean all (MA) is the mean MBR of all pixels included in the delineated area. All three parameters were lower in the RE than in the LE, in particular −20% for MT, −17% for MV, and −13% for MA. RE perfusion was lower than that of the LE in all the four quadrants of the eye; the largest difference was noted between the MT of the inferior and temporal quadrants of the two eyes (–27 and −29%, respectively).
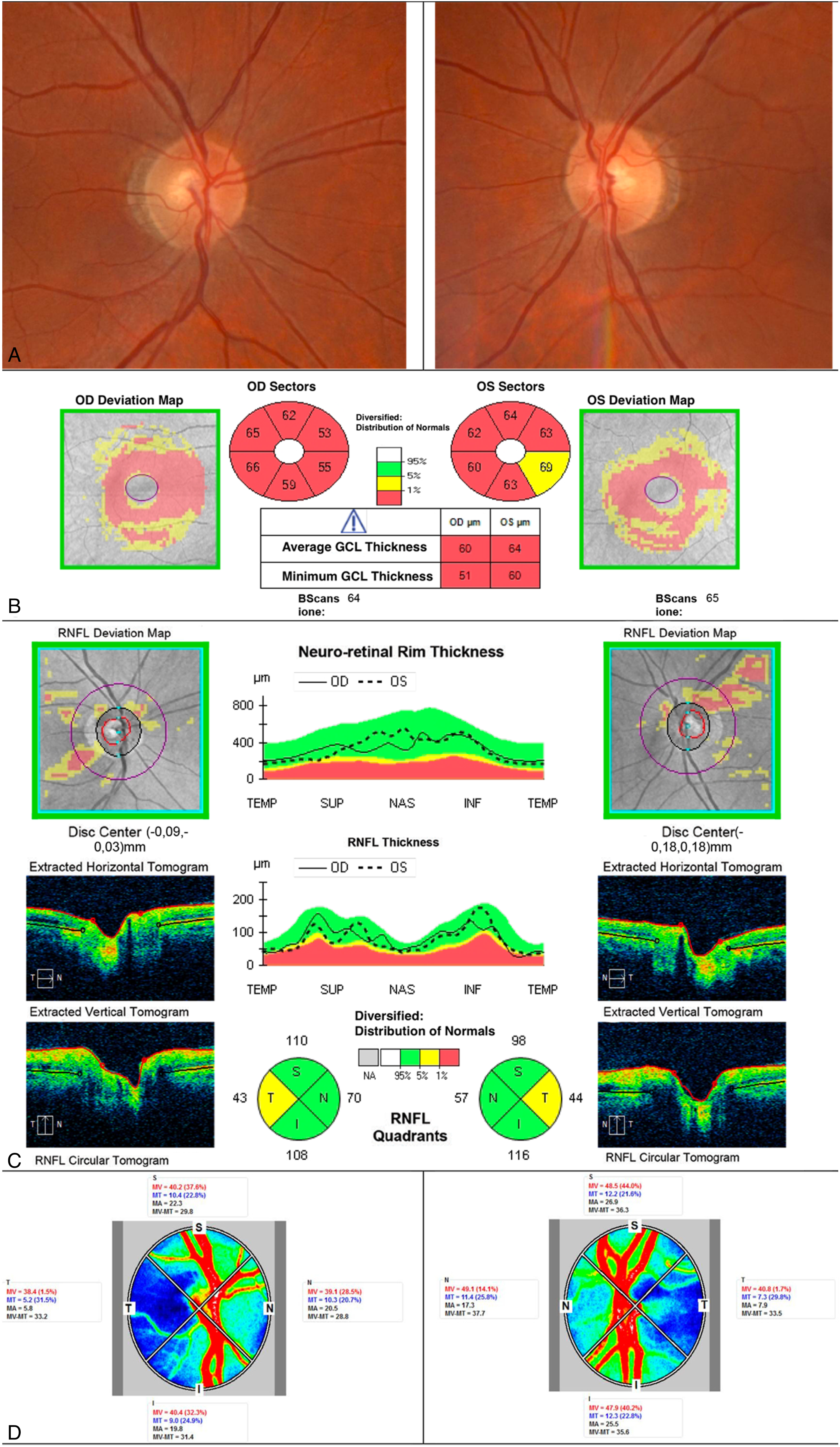
(A-D): Composite of clinical and instrumental findings at the end of the follow up (13 months after admission). A) optic nerve head regular funduscopic aspect; B) optical coherence tomography of the macular ganglion cell inner plexiform layer showing a bilateral, symmetrical severe thinning; C) optical coherence tomography of the circumpapillary retinal nerve fiber layer showing a borderline thinning in the sole temporal sector in both eyes; D) laser speckle flowgraphy (LSFG) assessment showing a reduced perfusion in the right eye chiefly affecting the microvascular networks (MT).
Discussion
The first peculiarity of the presented case was the discrepancy between the severe and strictly unilateral visual acuity deficiency, and the OCT findings bilaterally and symmetrically outside the normative range. We assumed that the patient suffered from TAON, given his behavior and the laboratory data. This diagnosis combined with the VEPs results could explain the baseline RE optic neuropathy and visual loss. One year after initial assessment, when the patient resumed his high alcohol and tobacco consumptions, both the unilateral visual defects (affecting principally visual acuity and color vision) and bilateral retinal nerve fiber layer thinning progressed. On fundoscopy, however, both the affected and the fellow ONH were normal. Patient's risk factors can also support an associated unilateral vascular insufficiency, while a pure ischemic optic neuropathy is difficult to infer. This essentially because: 1) the lack of the typical clinical signs of the acute phase during initial evaluations; the long-term normal aspect of the ONH. 2) The trend of the visual loss in the RE, which stopped when the patient began the vitamins supplementation limiting his alcohol and tobacco consumptions and significantly progressed as the patient resumed an unhealthy nutritional regimen. Therefore, we thought to a very atypical course of TAON, or an episode of ischemic optic neuropathy against a background of early bilateral TAON progression.
The second peculiarity noted concerns the LSFG data, which clearly indicate that the perfusion of the two eyes differed, especially the extent of tissular vascularization (MT) in the ONH area of the RE. This is the first such finding in a case of probable TAON. We believe that the original findings of the presented case could be of major interest despite some limitations, such as the lack of genetic investigations.
Conclusions
Physicians treating complex optic nerve anomalies may wish to gather and possibly comment on such atypical evidences. The reported LSFG findings might support the consideration of this technology among neuro-ophthalmological investigations. LSFG is an innovative, powerful, and real-time evaluating tool that offers potentially very meaningful data otherwise difficult to collect. Because of the originality of the technique, however, the interpretation of these data needs to be refined, especially based on the evidence obtained over time from both normal subjects and different retinal, choroidal, and optic nerve diseases. Particularly in suspected optic neuropathies we strongly encourage to perform an LSFG examination starting from the first clinical evaluation. Baseline blood flow status and possible subsequent variations in one or all the considered anatomical districts could help the diagnostic and prognostic work up.
Footnotes
Acknowledgemets
Consent for publication
The Local Ethical Committee “Area Vasta Emilia Nord (AVEN)” does not require official approval for the publication of single case reports. Written informed consent to publish information and images included in this report was obtained from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article