
Abstract
Background
Stroke is one of the most widespread reasons for acquired adult disability. Recent experimental studies have reported the beneficial influence of Wii Fit-based feedback on improving overall balance and gait for stroke survivors.
Methods
We conducted a systematic review of the literature using the following keywords to retrieve the data: feedback, biofeedback, stroke, visual, auditory, tactile, virtual reality, videogame rehabilitation, Nintendo Wii stroke, videogame stroke, exergame stroke, Nintendo Wii rehabilitation, balance, and gait. A review and meta-analysis of RCTs regarding Wii Fit-based rehabilitation accompanied by conventional therapy effects on Berg Balance Scale (BBS), Timed Up and Go (TUG), functional reach test, and gait (speed) in stroke survivors was conducted.
Objective
To determine the impacts of Wii Fit-based feedback combined with traditional therapy on balance and gait in stroke survivors.
Results
22 studies were included. The meta-analysis results revealed statistically significant improvements in functional ambulation measured using TUG (p < 0.0001), balance measured using BBS (p = 0.0001), and functional reach test (p = 0.01), but not in gait speed (p = 0.32) following Wii Fit-based feedback. Regarding the types of feedback, significant differences were found in BBS scores when mixed visual and auditory feedback was used.
Conclusion
Wii Fit-based feedback has desired effects on improving balance in stroke patients, making it a suitable adjunct to physical therapy.
Background
Stroke is one of the most widespread reasons for acquired adult disability and a common cause of morbidity and hospitalization worldwide (Brea et al., 2013; Mustafaoğlu et al., 2018). Stroke patients frequently suffer from motor and sensory deficits, which can result in difficulties with mobility, balance, and impaired motor control (Oliveira et al., 2011). It is estimated that 80% of survivors possess upper extremity motor problems, influencing their daily living activities execution, society’s performance, and quality of life (Bosomworth et al., 2021; Duncan Millar et al., 2019; Schnabel et al., 2021). Additionally, changes in body alignment take place, demanding the inclusion of therapeutic approaches aimed at enhancing postural control and weight-bearing symmetry (Cano-Mañas et al., 2020; Tessem et al., 2007; Tyson et al., 2006). The use of intensive, repetitive, and task-oriented physical therapy strategies can improve motor function in stroke patients by promoting neuroplasticity and motor learning (Pollock et al., 2014). Repetitive task training, which involves carrying out functionally appropriate tasks with a high level of intensity, improves transfer ability, balance, the function of the lower extremities, and gait speed in stroke survivors (French et al., 2016; Langhorne et al., 2009).
Virtual rehabilitation is a new therapeutic method according to simulation workouts that apply the technology of virtual reality. Through these kinds of interventions, therapists could be able to design therapeutic regimens that promote the neurological elements of brain plasticity: repetitive, intensive, and task-oriented practices in encouraging circumstances, resulting in enhanced adherence to rehabilitation (Burdea, 2003). Furthermore, these workout modalities are creative and fun ways to exercise (Karssemeijer et al., 2019).
Virtual treatment using the Nintendo Wii—one novel biofeedback resource that is being established for training—in addition to traditional physical therapy intervention has been executed in previous literature on patients with variability in stroke commencement and varying stages of recovery (Chen et al., 2015; You et al., 2005) and has been proven that it could be applied as a strategy to raise functionality and activities of daily living. There is currently insufficient information to draw conclusions regarding the effectiveness of Nintendo Wii-based virtual therapy for chronically physically disabled people caused by stroke (Dos Santos et al., 2015; Marques-Sule et al., 2021). Wii Fit from Nintendo has been used by some researchers alongside traditional therapy regimens in post-stroke rehabilitation. In this context, several investigations demonstrate that the Wii might be an effective supplementary therapy to conventional treatment for improving functionality (Cheok et al., 2015) and upper limb motor function (Aramaki et al., 2019; Carregosa et al., 2018) in stroke patients. Nevertheless, balance-related outcomes reveal various findings (Cheok et al., 2015; Karasu et al., 2018).
Virtual reality’s observational learning capabilities can activate mirror neurons in the cortex. Patients who experienced sensory feedback during the virtual reality intervention were more likely to achieve the desired motor activity (Levin & Demers, 2021). The feedback can boost use-dependent cortical plasticity development, resulting in improved motor control. Additionally, virtual reality training-induced functional improvement could dramatically promote the confidence and self-efficacy of participants in a new environment. Also, another benefit of virtual reality is that it can reduce patient costs and save on labor (Demers et al., 2021).
A 2015 systematic review by Cheok et al. (2015) investigated the effectiveness of Nintendo Wii compared with no intervention or other exercise interventions in the rehabilitation of stroke adults; the authors stated that the addition of Wii Fit to routine rehabilitation in chronic stroke patients meaningfully resulted in improved performance in some variables but not in all physical measures. Likewise, another 2015 systematic review by Dos Santos et al. (2015) indicated that the Nintendo Wii could enhance an individual’s motor function, but the data regarding balance and functional independence were ambiguous. These conclusions demonstrate that Wii Fit-based intervention could be a supplemental therapeutic strategy, although the influence remains unclear. Despite achievements that have been documented in the study of the beneficial effects of Wii Fit-based feedback intervention in addition to conventional therapy on stroke, the findings are still controversial in this regard. Moreover, the limited number of high-quality investigations directly examining Wii-based feedback is unable to make any judgments on the most efficient impact on balance performance and gait ability.
ed number of meta-analyses on the use of the Nintendo Wii in the rehabilitation of stroke victims have been conducted (Cheok et al., 2015; Dos Santos et al., 2015; Iruthayarajah et al., 2017); nevertheless, the purposes of each one varied within these reviews. There is evidence to support conducting an updated meta-analysis because more randomized controlled trials (RCTs) have since been published. This update comprises data pooling for balance-related outcomes and gait speed previously not fulfilled due to inadequate outcome data. Therefore, the current meta-analysis aimed to update previous pooled analyses, utilizing only level 1 (RCT) evidence investigating Wii Fit-based feedback intervention on balance and gait in post-stroke adult patients.
Methods
Study Design and Search Strategy
We used the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (Page et al., 2021) as a guide for our study and this report. To collect relevant papers related to biofeedback therapy in stroke patients, online databases of CINAHL Medical Science, Medline, PubMed, and Scopus were searched with a mixture of keywords of “feedback”, “biofeedback”, “stroke”, “visual”, “auditory”, “tactile”, “virtual reality”, “videogame rehabilitation”, “Nintendo Wii stroke”, “videogame stroke”, “exergame stroke”, “Nintendo Wii rehabilitation”, “balance”, and “gait”. The search strategy comprising all the items from database inception was developed until June 15, 2022. After the initial screening, systematic reviews, meta-analyses, and all references were also searched to find additional research. The final selection of included investigations was agreed upon by two authors according to the following criteria: (1) study design: RCTs and controlled trials of Nintendo Wii-based feedback rehabilitation published in the English language, excluding review articles, conference, abstracts, and study protocols; (2) comparison intervention: studies that applied conventional therapy and/or other exercise programs; (3) population: men and women (age ≥18 years) with stroke; (4) Outcome measures: the outcome measures were functional mobility (measured by timed up and go (TUG), balance (measured by the berg balance scale (BBS), functional reach test, and gait speed.
Data Extraction
We extracted the following data: author, year of publication, country, demographic characteristics of patients, types of feedback (visual, auditory, tactile), protocol applied in terms of time, frequency, and number of sessions, mean and standard deviation (SD) of relevant outcome measures, and methodological quality. Two authors (SMGD and NMR) independently extracted the mentioned data from each study. The third author (RA) resolved any disagreements.
Study Quality
We utilized an adapted Physiotherapy Evidence Database (PEDro) scale (Maher et al., 2003) to determine the study’s methodological quality, which is an 11-item questionnaire considered to collect data. The studies were independently rated by two investigators (SMGD and RA), and any controversy was resolved by consensus with a third investigator (NMR). The PEDro scale has been reported to be valid (De Morton, 2009) and reliable (Maher et al., 2003). The interpretation of quality scores is as follows: 9 to 10, excellent; 6 to 8, good; 4 to 5, fair; and less than 4, poor (Pang et al., 2006). Only those RCTs scoring ≥5 on the PEDro scale—a value considered to be of moderate to high quality (Moseley et al., 2002) —were entered for analysis.
Publication Bias
To qualitatively measure publication bias, funnel plots of the effect size were generated for each study group by Comprehensive Meta-Analysis software (version two; Biostat Inc, Englewood, New Jersey, USA). Funnel plot asymmetry was assessed using Begg and Egger tests, and a significant publication bias was deemed if the p value was <0.10 (Borenstein et al., 2021). We used the trim and fill computation to measure the effect of publication biases on the interpretation of the results (Borenstein et al., 2021).
Data Synthesis and Statistical Analysis
We performed 2 separate analyses in the current review. Effect sizes were calculated to compare the effects of Wii Fit-based feedback rehabilitation versus conventional therapy on the improvement of balance-related outcome measures (i.e., time of TUG, score of BBS, and functional reach test) and gait performance. After considering the overall effect sizes, subgroup analyses were performed according to types of feedback (visual, mixed visual and auditory). The effect size of any outcomes was summarized by computing the mean difference (MD) between the experimental and control conditions at baseline and after intervention for all included RCTs. Due to the similar methods of reporting techniques for outcomes, MD with a 95% confidence interval (CI) was used. The baseline mean was subtracted from the after intervention mean, and the change in SD was calculated using study group subject numbers in conjunction with group p-values or 95% CI, where the change in mean and SD was not reported. If the RCTs had more than one post-intervention assessment period, only the data collected at the end of the intervention period were involved in the meta-analysis. We evaluated the heterogeneity among the RCTs using the I2 statistic, with values >50% considered to show significant heterogeneity. (Higgins et al., 2003) A meta-analysis was conducted using forest plots and considered to have a 5% level of significance to demonstrate the significance of the results. We conducted this meta-analysis using Review Manager 5.4.1 (The Nordic Cochrane Centre, Copenhagen, Denmark).
Results
Study and Participant Characteristics
Initially, we found 752 papers from PubMed, Medline, CINAHL Medical Science, and Scopus databases and by hand searching. After duplicate titles and the exclusion of papers according to abstract and title were removed, 32 full-text papers remained for screening. 10 other papers were excluded due to the following reasons: (a) included healthy participants (Agmon et al., 2011; Bateni, 2012; Bieryla & Dold, 2013; Cone et al., 2015), (b) systematic review (Cheok et al., 2015; Felipe et al., 2020), (c) included no stroke patients (Padala et al., 2017), (d) lack of access to data (Fritz et al., 2013), (e) intervention not Wii (Zhang et al., 2020), and (f) the control group participated in a similar intervention (Bower et al., 2014). Twenty-two papers met our inclusion criteria and were included in the review (PRISMA flow diagram; Figure 1). Study selection represented by PRISMA flowchart.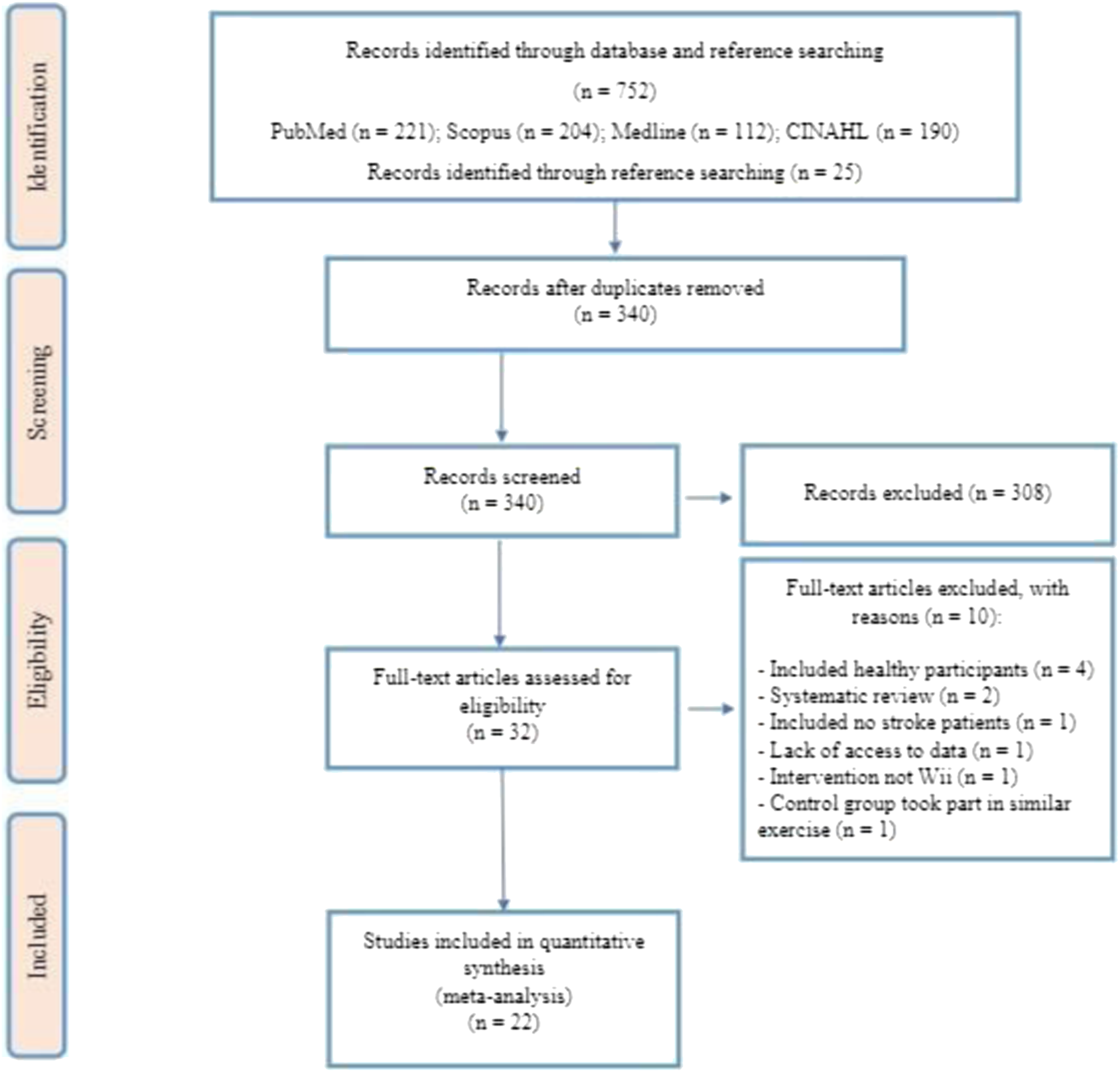
Studies were conducted in the Republic of Korea (7), Spain (3), Taiwan (3), Italy (2), Brazil (1), Cyprus (1), Germany (1), Israel (1), Malaysia (1), Pakistan (1), and Turkey (1). The 22 included RCTs had 648 patients, 328 (∼51%) participants in the experimental group, and 320 (∼49%) in the control group. The included studies were published between 2011 and 2022.
Description of Included Articles
Characteristics of Included Studies.
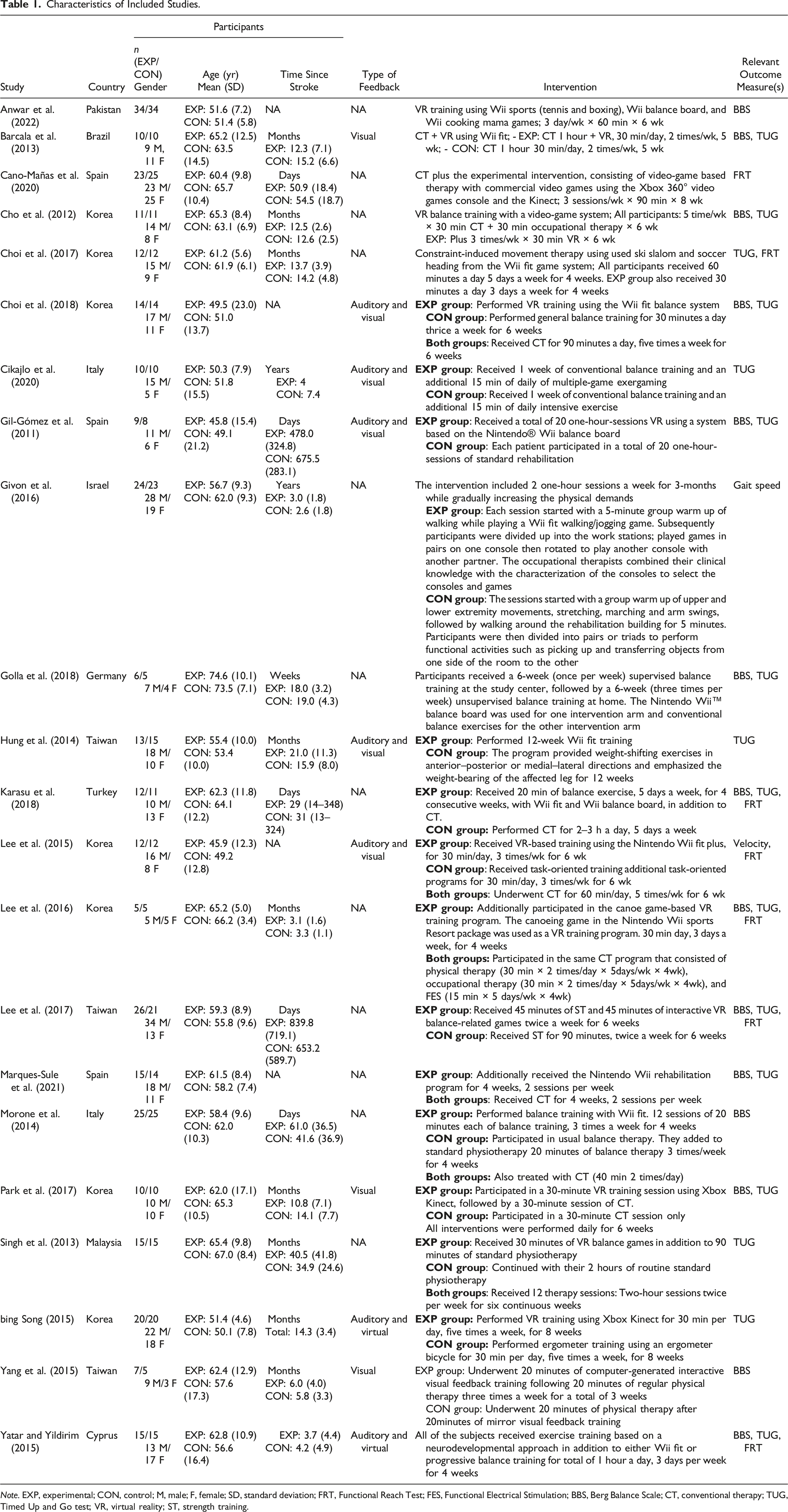
Note. EXP, experimental; CON, control; M, male; F, female; SD, standard deviation; FRT, Functional Reach Test; FES, Functional Electrical Stimulation; BBS, Berg Balance Scale; CT, conventional therapy; TUG, Timed Up and Go test; VR, virtual reality; ST, strength training.
Outcome Measures
Functional Mobility
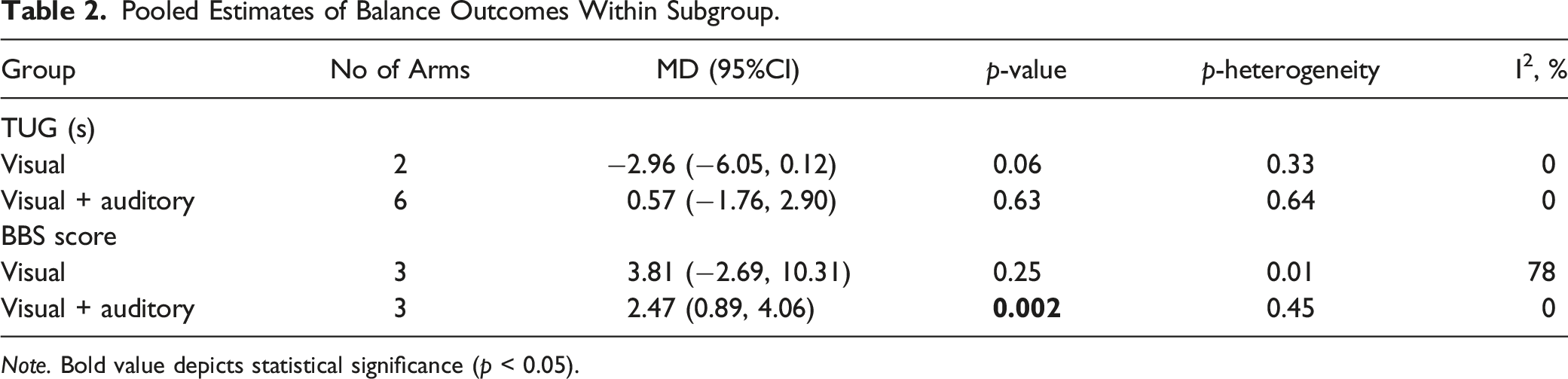
16 RCTs (Barcala et al., 2013; Park et al., 2017; Cho et al., 2012; Choi et al., 2018; Choi et al., 2017; Cikajlo et al., 2020; Gil-Gómez et al., 2011; Golla et al., 2018; Hung et al., 2014; Karasu et al., 2018; Lee et al., 2017; Lee et al., 2016; Marques-Sule et al., 2021; Park et al., 2017; Singh et al., 2013; Yatar & Yildirim, 2015) providing a total of 399 patients (205 participants in the experimental groups and 194 participants in the control groups), reported changes in functional mobility (measured by TUG) as an outcome measure. Random-effects model revealed statistically significant improvements in TUG test after Wii Fit-based feedback rehabilitation (MD = −0.83 s; 95% CI: −1.24 to −0.41; p < 0.0001, Figure 2). Subgroup analyses by types of feedback are provided in Table 2. These analyses revealed no significant improvements in studies that used visual (MD = −2.96 s, 95% CI: −6.05 to 0.12; p = 0.06, two studies) or mixed visual and auditory (MD = 0.57, 95% CI: −1.76 to 2.90; p = 0.63, six studies) modes of feedback. Effect size (95% CI) of Wii Fit-based feedback rehabilitation on TUG by pooling data from 16 studies comparing Wii Fit-based feedback versus standard care using random effects meta-analysis (n = 399). Pooled Estimates of Balance Outcomes Within Subgroup. Note. Bold value depicts statistical significance (p < 0.05).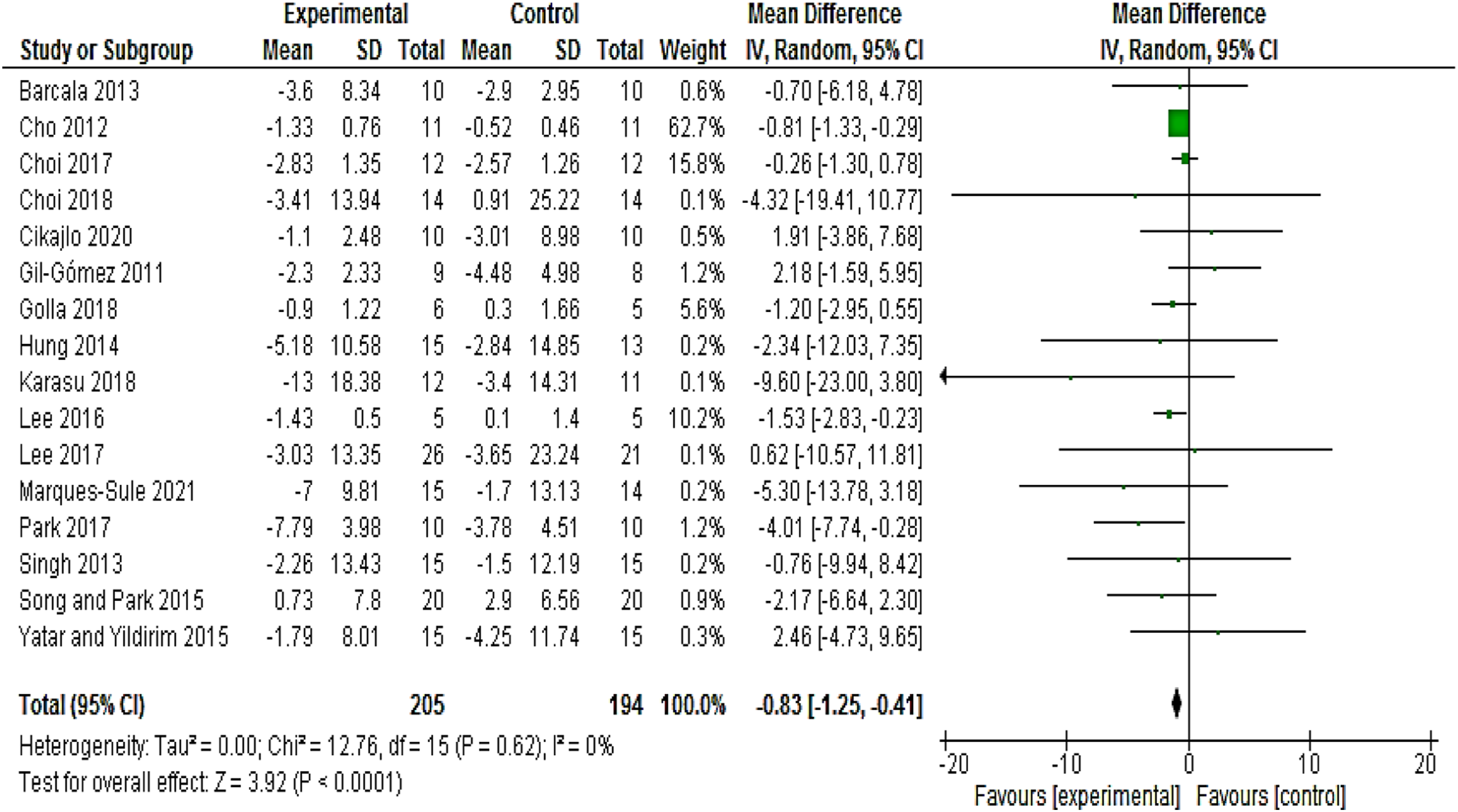
Balance
14 RCTs (Anwar et al., 2022; Barcala et al., 2013; Cho et al., 2012; Choi et al., 2018; Gil-Gómez et al., 2011; Golla et al., 2018; Karasu et al., 2018; Lee et al., 2016, 2017; Marques-Sule et al., 2021; Morone et al., 2014; Park et al., 2017; Yang et al., 2015; Yatar & Yildirim, 2015) providing a total of 394 patients (204 participants in the experimental groups and 190 participants in the control groups), reported changes in balance (measured by BBS) as an outcome measure. Statistically significant improvements were found for BBS after Wii Fit-based feedback rehabilitation (MD = 3.76; 95% CI: 1.84 to 5.68; p = 0.001, Figure 3). Subgroup analyses by the types of feedback revealed significant improvements in BBS score for studies used mixed of visual and auditory feedback (MD = 2.47, 95% CI: 0.89 to 4.06; p = 0.002, three studies) but not for studies used only visual feedback (MD = 3.81, 95% CI: −2.69 to 10.31; p = 0.25, three studies; Table 2). Effect size (95% CI) of Wii Fit-based feedback rehabilitation on BBS score by pooling data from 14 studies comparing Wii Fit-based feedback versus standard care using random effects meta-analysis (n = 394).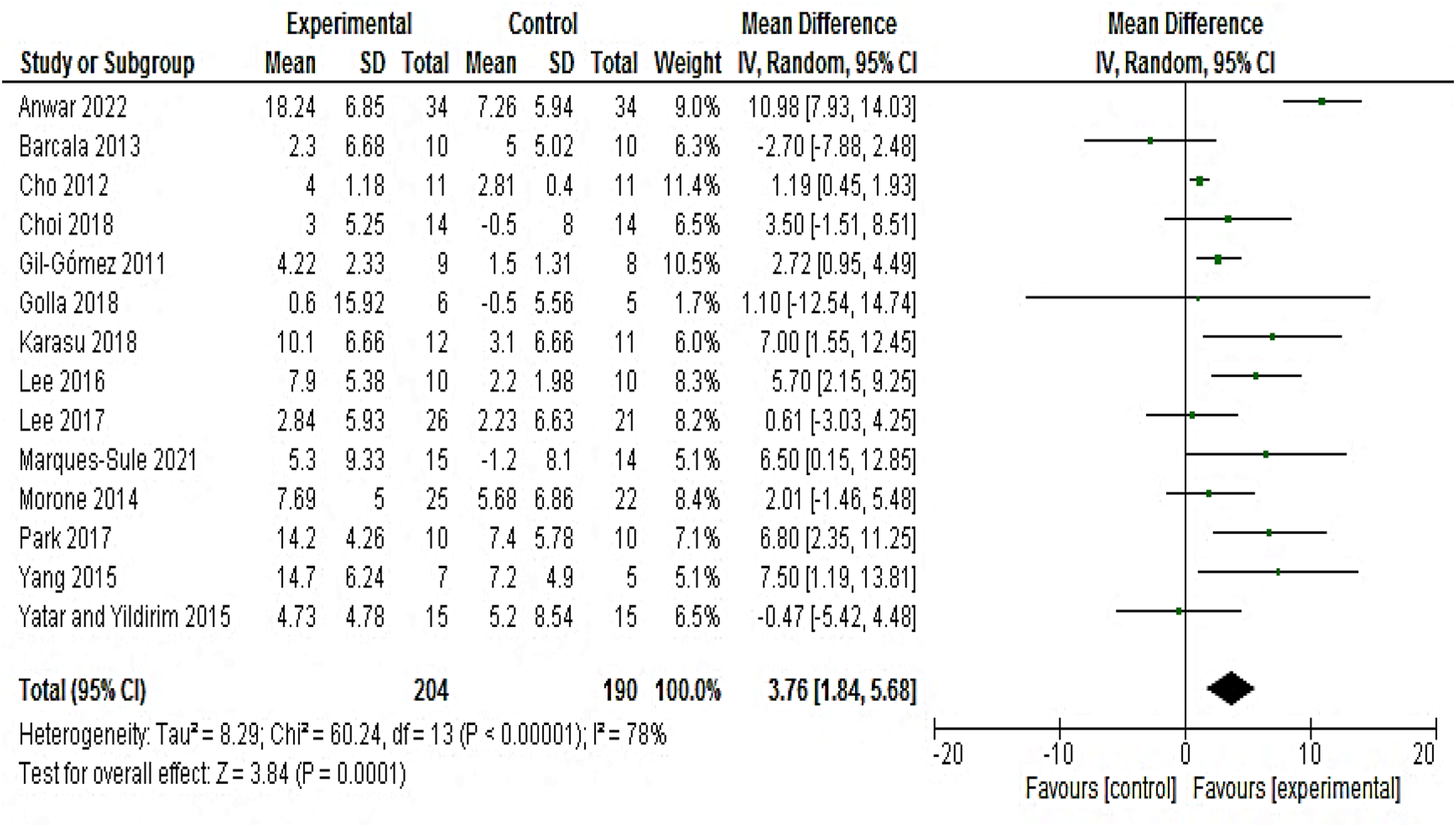
Functional Reach Test
Seven RCTs (Cano-Mañas et al., 2020; Choi et al., 2017; Karasu et al., 2018; Lee et al., 2015, 2016, 2017; Yatar & Yildirim, 2015) providing a total of 206 patients (105 participants in the experimental groups and 101 participants in the control groups) reported changes in functional reach test as an outcome measure. Statistically significant improvements were found for functional reach test after Wii Fit-based feedback rehabilitation (MD = 2.43 cm; 95% CI: 0.50 to 4.35; p = 0.01, Figure 4). Effect size (95% CI) of Wii Fit-based feedback rehabilitation on functional reach test by pooling data from seven studies comparing Wii Fit-based feedback versus standard care using random effects meta-analysis (n = 206).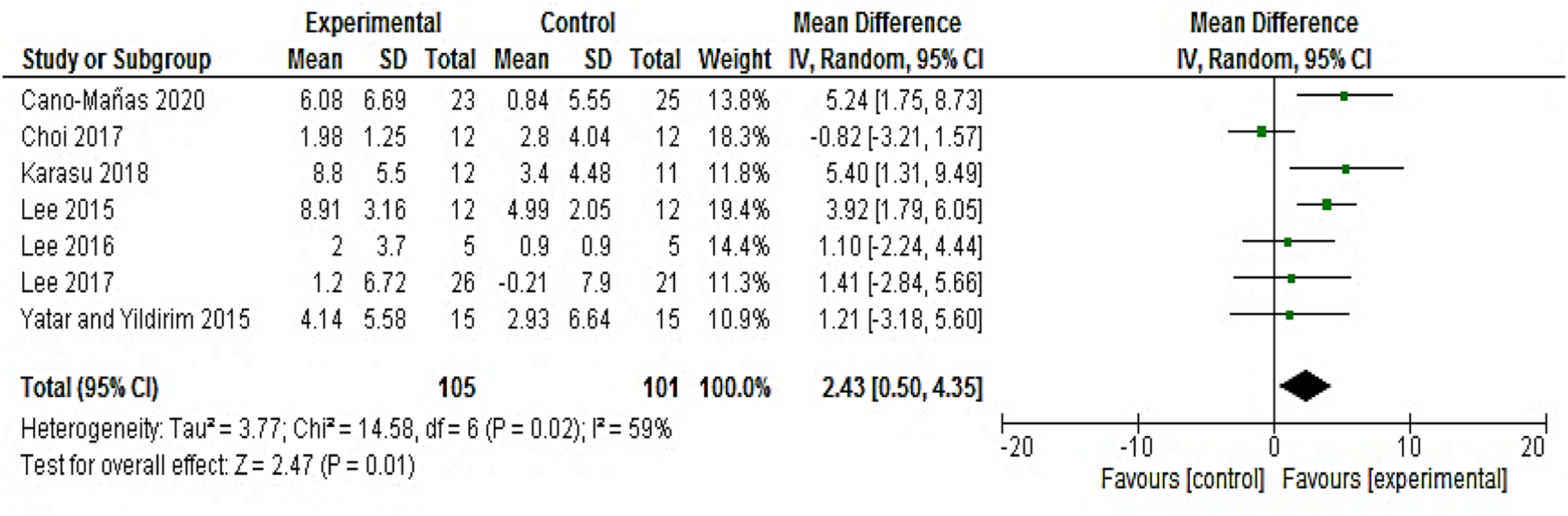
Gait Speed
Two RCTs (5 arms; Givon et al., 2016; Lee et al., 2015) providing a total of 143 patients (72 participants in the experimental groups and 71 participants in the control groups) reported changes in gait speed as an outcome measure. The random-effects model revealed no statistically significant improvements in gait speed after Wii Fit-based feedback rehabilitation (MD = 0.08 m/s; 95% CI: −0.08 to 0.24; p = 0.32, Figure 5). Effect size (95% CI) of Wii Fit-based feedback rehabilitation on gait speed test by pooling data from two studies comparing Wii Fit-based feedback versus standard care using random effects meta-analysis (n = 143). ECNB, eyes-closed narrow base; ECWB, eyes-closed wide base; EONB, eyes-open narrow base; EOWB, eyes-open wide base.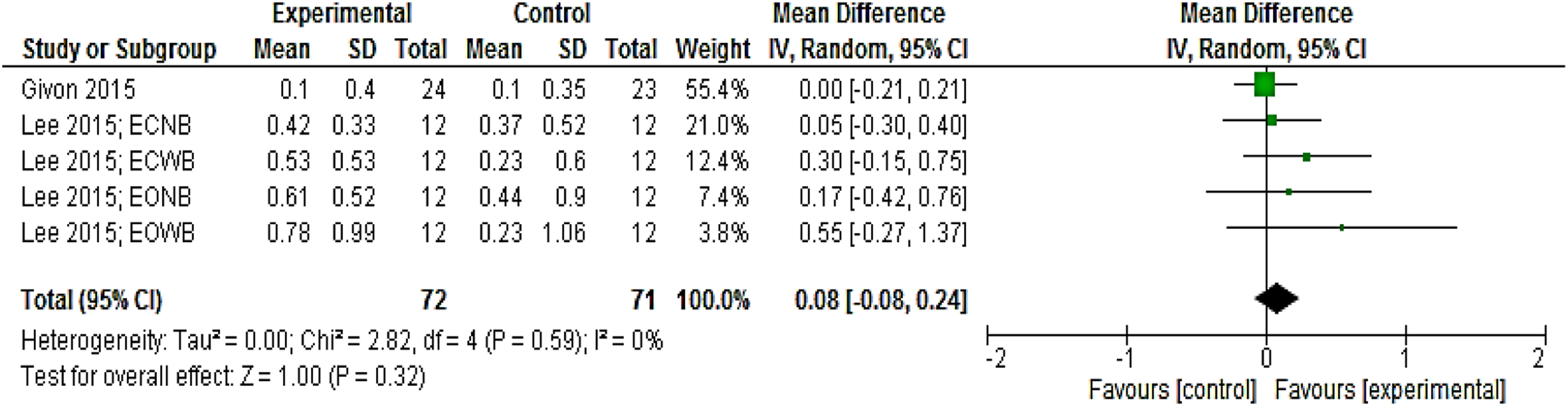
Quality Assessment
Studies that Meet the Criteria of the PEDro Scale.
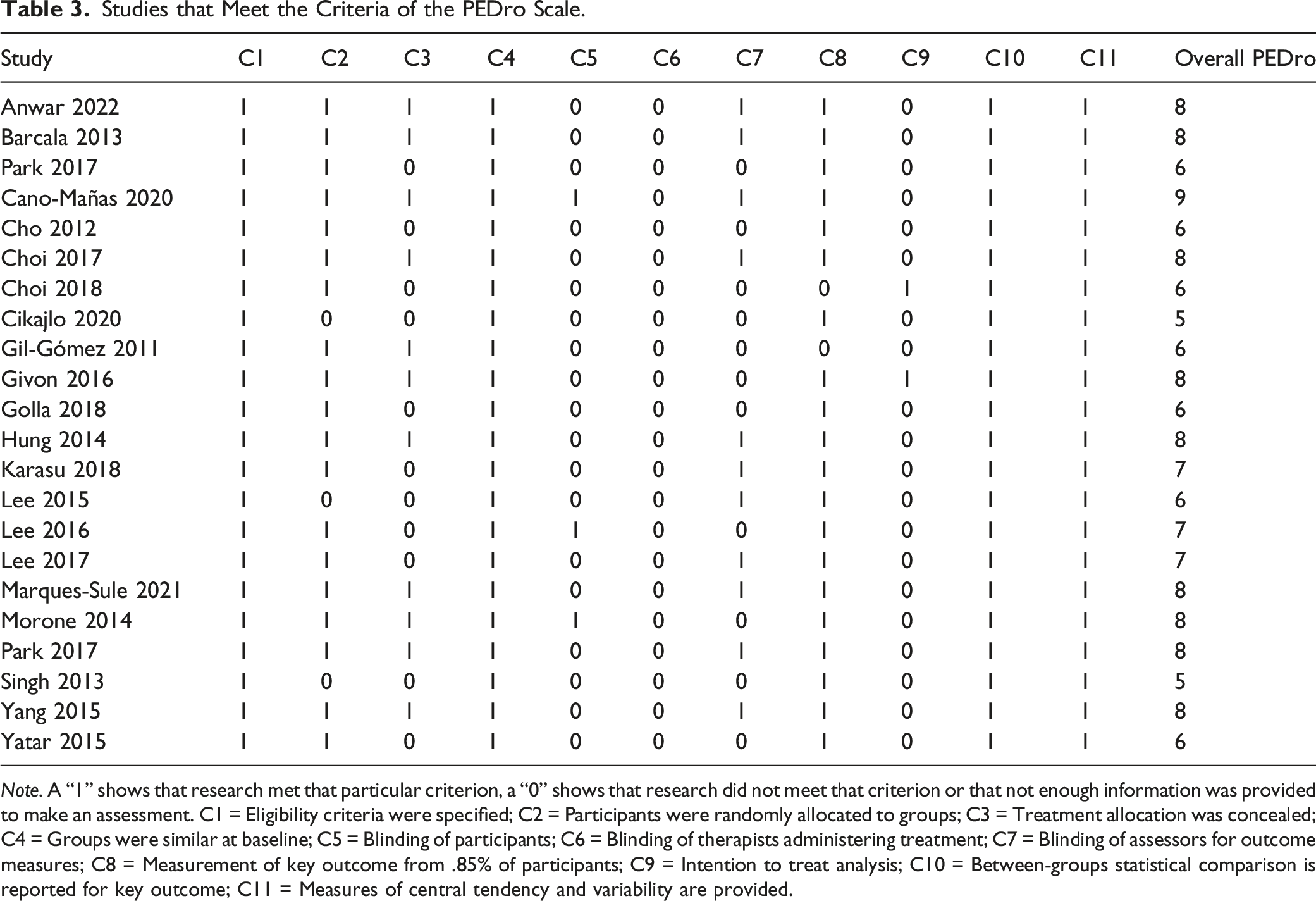
Note. A “1” shows that research met that particular criterion, a “0” shows that research did not meet that criterion or that not enough information was provided to make an assessment. C1 = Eligibility criteria were specified; C2 = Participants were randomly allocated to groups; C3 = Treatment allocation was concealed; C4 = Groups were similar at baseline; C5 = Blinding of participants; C6 = Blinding of therapists administering treatment; C7 = Blinding of assessors for outcome measures; C8 = Measurement of key outcome from .85% of participants; C9 = Intention to treat analysis; C10 = Between-groups statistical comparison is reported for key outcome; C11 = Measures of central tendency and variability are provided.
Publication Bias
Funnel plots including Egger regression tests (p > 0.05 for all) for the different analyses did not suggest publication bias, nor did Duval and Tweedie’s trim and fill computation change the results (see Supplementary Figures S1-S4).
Discussion
The present systematic review and meta-analysis aimed to update previous pooled analyses, using only level 1 RCT evidence that evaluated the effect of Wii Fit-based feedback interventions on balance performance and gait ability in adults after stroke. Our primary analysis demonstrates that Wii Fit-based feedback interventions compared to standard rehabilitation care had a significant effect on TUG, BBS, and functional reach test. Through merged data analysis, it was discovered that mixed visual and auditory feedback offers meaningful improvements in balance (measured by BBS) compared to a single type of feedback (i.e., visual). In relation to gait ability, we found that gait speed did not significantly improve following Wii Fit-based feedback programs.
In general, Wii Fit-based feedback interventions appear to be more effective at promoting rehabilitation in chronic stroke patients with impaired balance than conventional rehabilitation approaches. A number of conceivable mechanisms that could explain these improvements in performance, in accordance with related theories presently available, are learning, reversal of learned nonuse, and skill training (Kleim et al., 2002; Remple et al., 2001; Taub et al., 1994).
The addition of Wii to conventional therapy appears to be secure and linked to sustained participation in ongoing rehabilitation when added to standard physiotherapy programs (Cheok et al., 2015). Our results reveal that Wii Fit-based feedback interventions significantly affected TUG (as a dynamic balance factor). These results are compatible with the results, who noted that the addition of Wii to standard care led to a significant improvement in TUG performance when compared with standard care alone (Cheok et al., 2015). The effect size obtained for TUG (−0.83 sec) in our meta-analysis was similar to the effect size obtained by Gary and colleagues (−0.8 sec). However, it was smaller than the minimal detectable change of 2.9 seconds for TUG performance in chronic patients with stroke (Flansbjer et al., 2005). Therefore, this finding may be explained by chance or measurement error.
Iruthayarajah et al. (2017) performed a systematic review and meta-analysis on the effectiveness of virtual reality interventions for enhancing balance in chronic stroke patients. In total, 20 investigations were selected that evaluated the Nintendo® Wii Fit balance board, treadmill training and virtual reality, and postural training using virtual reality. They observed that among all virtual reality intervention types, there was no significant improvement in either the BBS or TUG in favor of the Wii Fit intervention (Iruthayarajah et al., 2017), which is inconsistent with our findings. Another meta-analysis investigating whether balance or gait training utilizing virtual reality is more effective compared to conventional balance or gait training in post-stroke patients suggested that virtual reality training is more effective compared to balance or gait training alone for improving balance (time of TUG and BBS score) or gait ability (speed) in these patients. Nevertheless, these researchers assessed all types of virtual reality interventions (de Rooij et al., 2016).
Wii Fit intervention is a virtual reality technology that affects the learning of actual activity and allows a boost in training intensity, delivering 3-dimensional feedback through visual, sensory, and auditory stimulation. There is a wide range of explanations for the additional benefit that virtual reality has over most currently available standard therapies. A high degree of repetition and variety are used to develop patient-specific motor training in virtual reality. The physiological underpinnings of motor learning are repetitive training (French et al., 2016). In addition to repetitive training, diversity in practice is crucial for motor learning, considering that it will strengthen the ability to adjust to new situations (Imam & Jarus, 2014). A further benefit of using virtual reality is that it allows therapists to deliver personalized training where the patient’s demands and characteristics can be readily considered when determining the training exercises' level of difficulty and intensity (Merians et al., 2006). Exercises that are required for optimal learning can be given to stroke patients under controlled constraints (Fung et al., 2006; Moreira et al., 2013). Furthermore, in virtual reality training such as Wii Fit, individuals can receive more feedback on their performance than in real-world practice.
It is widely accepted that feedback enhances the rate of learning (Holden, 2005) and that stroke patients profit from therapies with augmented feedback (Winstein et al., 1999). It has been demonstrated that providing individuals with stroke with visual stimuli can assist them in improving their balance (Barclay-Goddard et al., 2004; Walker et al., 2016). Finally, it is believed that using virtual reality will promote activity adherence and enjoyment while reducing perceived exertion (Sveistrup, 2004). The individual and the intervention may impact how motivated and engaged participants are during a virtual reality intervention. However, none of the RCTs included in the current meta-analysis evaluated motivation.
Notably, people with stroke underperform balance when walking; hence, improvement in it would be of great assistance to them. Most patients deem playing games a fun activity in their leisure time. Regular conventional therapy was discovered to be dull for individuals and less adorable (Aramaki et al., 2019). The findings of our study will assist therapists in using virtual reality to rehabilitate post-stroke patients. When a patient attempts to use his muscles, his coordination with the brain improves. In an upright position, most of the postural muscles are engaged. On the other hand, conventional physical therapy is passive, which causes sluggish improvement. Postural muscles should be considered in treatment regimens. Stroke can occasionally directly impact the patient’s capacity to control the surrounding environment. Therefore, it is challenging to maintain balance when you are not sure about your position in the surroundings (Kim et al., 2015; Lee et al., 2019; Noveletto et al., 2018). This review demonstrated how virtual reality helps stroke patients regain functional independence.
Our meta-analysis identified several limitations that should be considered when interpreting the findings in patients who are post-stroke. First, we only evaluated 22 studies, and 14 of them have small sample sizes (n < 30), demonstrating that more studies with larger sample sizes are required to deliver more convincing results. Second, the wide inclusion and variety of the included RCTs bring some limitations with them. The demographics of stroke patients in the included RCTs varied, particularly in terms of the large range in time since stroke. The impact of virtual reality intervention was predicted to be higher in individuals early following stroke since brain plasticity and structural reorganization are higher early after lesions (Felling & Song, 2015), and endogenous recovery after stroke has been documented to achieve a plateau in a 6-month period (Kwakkel & Kollen, 2013). Third, the included investigations in the current study compared the addition of Wii Fit to standard therapy versus isolated standard therapy. Due to the experimental group receiving longer-term rehabilitation, this may have established a bias in favor of the experimental group. Finally, the results of this review are limited to gait and balance outcomes, specifically BBS scores, TUG scores, functional reach test scores, and gait speed; hence, its generalizability in terms of outcome measures is in doubt. We decided to include these uniform outcome measures to carry out a valuable meta-analysis.
Conclusion
Wii Fit-based feedback is a feasible regimen for post-stroke patients. The addition of Wii Fit interventions to conventional therapy sessions resulted in statistically significant improvements in balance but not in gait speed. Until additional large-scale trials are available to confirm the effectiveness of Wii Fit-based feedback in stroke rehabilitation, Wii Fit appears to be a supplemental, promising, and safe strategy for stroke rehabilitation with improved long-term observation.
Supplemental Material
Supplemental Material - Wii Fit-Based Biofeedback Rehabilitation Among Post-Stroke Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trial
Supplemental Material for Wii Fit-Based Biofeedback Rehabilitation Among Post-Stroke Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trial by Seyedeh Maryam Ghazavi Dozin, Nasser Mohammad Rahimi, and Reza Aminzadeh in Biological Research for Nursing
Footnotes
Author Contributions
Nasser Mohammad Rahimi contributed to acquisition, analysis, and interpretation drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Reza Aminzadeh contributed to conception and design drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Seyedeh Maryam Ghazavi Dozin contributed to conception and design drafted manuscript critically revised manuscript gave final approval agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.