
Abstract
Objectives
The aim of the study was to investigate the effects of high-dose (HD) carvedilol treatment in client-owned cats with stage B1 obstructive hypertrophic cardiomyopathy (oHCM) where a standard dose (SD) had failed to adequately alleviate left ventricular outflow tract (LVOT) obstruction.
Methods
A prospective, interventional study was conducted in which cats underwent echocardiography, including evaluation of myocardial strain using speckle-tracking echocardiography. Myocardial injury was quantified using a cardiac troponin I (cTnI) assay. Echocardiographic variables and the cTnI level were compared before treatment and after SD and HD carvedilol treatment.
Results
LVOT velocity (LVOTV) decreased after SD compared with before treatment in all cats, but remained above 2.5 m/s after SD (before treatment 4.9 m/s [interquartile range [IQR] 4.3–5.0]; SD 4.3 m/s [IQR 3.9–4.7]), whereas HD decreased LVOTV to below 2.5 m/s in 10/11 cats (1.6 m/s [IQR 1.5–2.0]). Longitudinal strain was improved after SD and HD compared with before treatment (endocardial layer: before treatment 12.1% [IQR 9.6–15.8]; SD 20.0% [IQR 15.9–21.7]; HD 18.9% [IQR 12.9–22.8]; P = 0.003 and P = 0.006, respectively; epicardial layer: before treatment 9.4% [IQR 7.0–10.7]; SD 11.6% [IQR 10.0–12.7]; HD 12.5% [IQR 10.0–13.3]; P = 0.013 and P = 0.001, respectively). Circumferential strain demonstrated no changes. The cTnI level decreased after SD and HD compared with before treatment, and after HD compared with SD (before treatment 0.334 ng/ml [IQR 0.117–0.931]; SD 0.192 ng/ml [IQR 0.111–0.377]; HD 0.018 ng/ml [IQR 0.009–0.161]; P = 0.043, P = 0.043 and P = 0.043, respectively). No cats experienced adverse effects such as bradycardia or hypotension.
Conclusions and relevance
HD improved LVOTV, myocardial function and cTnI level without adverse effects in cats with stage B1 oHCM.
Keywords
Introduction
Hypertrophic cardiomyopathy (HCM) is a primary myocardial disease in cats. Pathologically, it is characterised by myocardial disarray, fibrosis and myocardial hypertrophy, which collectively contribute to the development of diastolic dysfunction. 1 Some cats with HCM have left ventricular outflow tract obstruction (LVOTO) with concurrent systolic anterior motion of the mitral valve, referred to as obstructive HCM (oHCM). The LVOTO causes pressure overload within the left ventricle (LV), resulting in a further worsening of myocardial hypertrophy, diastolic dysfunction and myocardial ischaemia. 2 In humans, the presence of LVOTO is considered a poor prognostic factor and treatment aims to relieve the obstruction. 3 In particular, a peak left ventricular outflow tract (LVOT) pressure gradient of 50 mmHg or more (corresponding to left ventricular outflow velocity [LVOTV] of 3.5 m/s) is considered to represent severe obstruction. Conversely, in cats, a previous study has reported that LVOTO does not impact survival. 4
Medical treatments, including beta (β)-blockers, calcium channel blockers, disopyramide and myosin inhibitors, have been reported to alleviate LVOTO in humans.5 –8 Of these, β-blockers are considered to be the first-line agents, and it is recommended that the dose is increased until the therapeutic goal of alleviating LVOTO is achieved. 9 In the American College of Veterinary Internal Medicine (ACVIM) guidelines, atenolol, a water-soluble β-blocker, may be considered for cats with HCM and severe LVOTO, although there is no definitive evidence linking dynamic LVOTO with increased mortality. 10 However, there is a lack of consistency among reports regarding the improvement in LVOTO, indicating that its effectiveness remains limited.11 –13 Furthermore, a previous study failed to demonstrate that atenolol delays the onset of heart failure or improves survival in cats with preclinical HCM, suggesting that its overall clinical effectiveness is limited. 14 In human medicine, lipid-soluble β-blockers are used preferentially over water-soluble agents such as atenolol.15,16 Of these, carvedilol is a fat-soluble, non-selective β-blocker, which improves myocardial remodelling, and has vasodilatory effects through blockade of alpha (α)1-receptors. 17
A previous retrospective study has reported that carvedilol was associated with improvement in LVOTO and myocardial function in cats with oHCM. 18 However, not all cats in that study demonstrated improvement in LVOTO, with non-responders reported to have more severe obstruction and myocardial dysfunction than those that responded to treatment. 19 These findings highlight potential variability in treatment response and provide a rationale for exploring alternative dosing strategies, including consideration of dose-titration principles applied in human medicine, in cats with more severe disease. 9 Although there are limited reports detailing carvedilol dosage in cats, a dose-dependent effect might be suggested. 20
Overall, this prospective study aimed to evaluate the efficacy of high-dose carvedilol in cats with severe oHCM (LVOTV ⩾3.5 m/s) that were non-responsive to a standard dose.
Materials and methods
This was a prospective, interventional study. All study procedures followed the Guidelines for the Care and Use of Animals of Nippon Veterinary and Life Science University. All study protocols were approved by the Ethics Committee for Animal Use of Nippon Veterinary and Life Science University Veterinary Teaching Hospital (approval number R2-4). Written informed consent for the use of the study data was obtained in advance from the owners of each cat.
Animals and study protocols
This study included cats that were diagnosed with stage B1 oHCM at our institution between April 2022 and July 2024. All cats underwent a complete physical examination, electrocardiography, thoracic radiography, non-invasive measurement of systemic blood pressure (oscillometric method, BP100D II; Fukuda ME) and transthoracic echocardiography. Cats were diagnosed with stage B1 HCM if the maximal LV wall thickness at end-diastole was 6 mm or greater and no moderate-to-severe left atrial enlargement was present (see below for detailed measurement methods). 10 In addition, cats with HCM were classified as having oHCM if echocardiography demonstrated systolic anterior motion of a mitral valve leaflet, based on the right parasternal long-axis view, the left apical five-chamber view or both, and continuous-wave Doppler-derived maximum LVOTV of 3.5 m/s or greater. 21 Since the LVOTV fluctuates continuously during the examination, LVOTV was assessed under two distinct physiological states during a single echocardiographic session. The highest and lowest values, defined as ‘excited LVOTV’ (LVOTVexcited) and ‘resting LVOTV’ (LVOTVrest), respectively, were used for subsequent statistical analyses. Cats were excluded from the study if they had systemic hypertension (systolic systemic blood pressure ⩾160 mmHg), hyperthyroidism, dehydration or were diagnosed with other cardiovascular diseases that could cause myocardial hypertrophy. None of the cats included in the study were receiving β-blockers before the start of the study. After the diagnosis of oHCM (defined as pre-treatment), all cats were started on treatment with carvedilol at a standard dose (SD) of 0.2–0.3 mg/kg q12h, and they were re-checked within 1 month (defined as SD). 20 In this study, cats whose maximum LVOTV did not reach 2.5 m/s (LVOT pressure gradient <25 mmHg) after initiating SD carvedilol administration were defined as suboptimal responders. When maximum LVOTV did not reach the therapeutic goal of under 2.5 m/s on the SD of carvedilol, the dose was increased to 150–200% of the initial SD. 22 The efficacy assessment of high-dose (HD) carvedilol was conducted at least 2 weeks after increasing the dose (defined as HD). At the time of presentation, some cats were receiving medications other than β-blockers. No new medications were initiated during the study period; all pre-existing treatments were maintained at the same dosages throughout the duration of the study.
Standard echocardiography
Two-dimensional and Doppler echocardiographic examinations were performed by a single operator (RS) using an echocardiographic system equipped with a 12 MHz transducer (Vivid E95 Ultra Edition; GE Healthcare). During the examination, lead II electrocardiography was performed and displayed on the images. All examinations were conducted without sedation, and video recordings of five consecutive cardiac cycles were obtained. The recorded data were analysed using an offline workstation by a single well-trained operator (HK) who was blinded to the treatment status during the analysis.
Maximal LV wall thickness was measured using B-mode imaging as the thickest wall of the end-diastolic LV in the right ventricular long- and short-axis views. The left atrium:aorta ratio was measured using B-mode imaging in the right parasternal short-axis view at the base level of the heart. In addition, in the right parasternal short-axis view at the level of the chordae tendineae, end-diastolic interventricular septal thickness (IVSd [mm]), end-diastolic LV posterior wall thickness (LVPWd [mm]), end-diastolic LV internal dimension (LVIDd [mm]), end-systolic LV internal dimension (mm) and fractional shortening were obtained using B-mode imaging. The relative left ventricular wall thickness (RWT) was calculated as follows: 23

In the left apical four-chamber view, the peak velocities of the early diastolic and late diastolic trans-mitral waves (E and A waves, respectively) were measured using the pulsed-wave Doppler method. The E:A velocity ratio was then calculated. If the E and A waves were completely fused, data from those cats were excluded from statistical analysis. The peak velocity of early diastolic mitral annular motion was obtained at the septal and lateral mitral annulus using tissue Doppler imaging. In the left apical five-chamber view, LVOTV was measured using the continuous-wave Doppler method. The minimum LVOTV value obtained by repeated measurements was defined as LVOTVrest, whereas the maximum LVOTV value was defined as LVOTVexcited.9,24 No specific interventions were applied to obtain the LVOTVexcited.9,24
Two-dimensional speckle-tracking echocardiography
Two-dimensional speckle-tracking echocardiography (STE) analysis was performed as an indicator of detailed myocardial function. 25 LV circumferential deformation was evaluated using images of the LV at the level of the papillary muscles in the right parasternal short-axis view, whereas LV longitudinal deformation was assessed in the left apical four-chamber view. Longitudinal and circumferential strains (SL and SC, respectively) were measured in the endocardium, epicardium and the whole layer of the LV wall. In addition, the endocardial:epicardial strain ratio (Endo:Epi) was calculated for each measurement. 26 For all statistical analyses, the mean values from three consecutive cardiac cycles, obtained from high-quality images, were used.
Cardiac troponin I measurement
As the cardiac biomarker that reflects myocardial injury, the serum cardiac troponin I (cTnI) concentration was measured. Venous blood samples were collected on the same day as echocardiography and sampling was performed three times (before treatment and after SD and HD treatments). Whole blood was immediately placed into a serum separation tube and centrifuged at 3000 g for 15 mins at 4°C. The serum samples were stored at –80°C. The cTnI concentration was measured using a chemiluminescence immunoassay method and was outsourced to an external laboratory (Fujifilm Vet Systems). This assay utilised high-sensitivity methodology and the reference interval (RI) was defined as below 0.121 ng/ml.
Statistical analysis
All variables are presented as median and interquartile range (IQR). Statistical analyses were performed using a commercially available software (R 2.8.1; https://www.r-project.org/). Data normality was assessed using the Shapiro–Wilk test. For comparisons among the pre-treatment and SD and HD treatment values, repeated measures ANOVA was performed if the data were normally distributed and the Friedman test was used for non-normally distributed data. If a statistically significant difference was detected, multiple comparisons were conducted using paired t-tests for normally distributed data or the Wilcoxon signed-rank test for non-normally distributed data. Regarding cTnI, since there were missing data in some cases, we performed unpaired three-group comparisons (Kruskal–Wallis test) and the following multiple comparisons (Steel–Dwass test). Correlation analyses using Spearman’s correlation coefficient for non-normally distributed data between the cTnI concentrations and each variable were conducted, including data from pre-treatment and after SD and HD treatments. Statistical significance was set at P <0.05.
Results
In this study, 24 cats diagnosed with stage B1 oHCM met the inclusion criteria. Of these, one was excluded because the owner declined treatment. SD carvedilol treatment was initiated in 23 cats. Four cats responded to SD carvedilol (LVOTVexcited <2.5 m/s), and 19 were then treated with HD carvedilol. Furthermore, eight cats were excluded for the following reasons: requiring additional treatments other than carvedilol (n = 6) and missing data (n = 2). Finally, 11 cats were enrolled in this study (Figure 1).
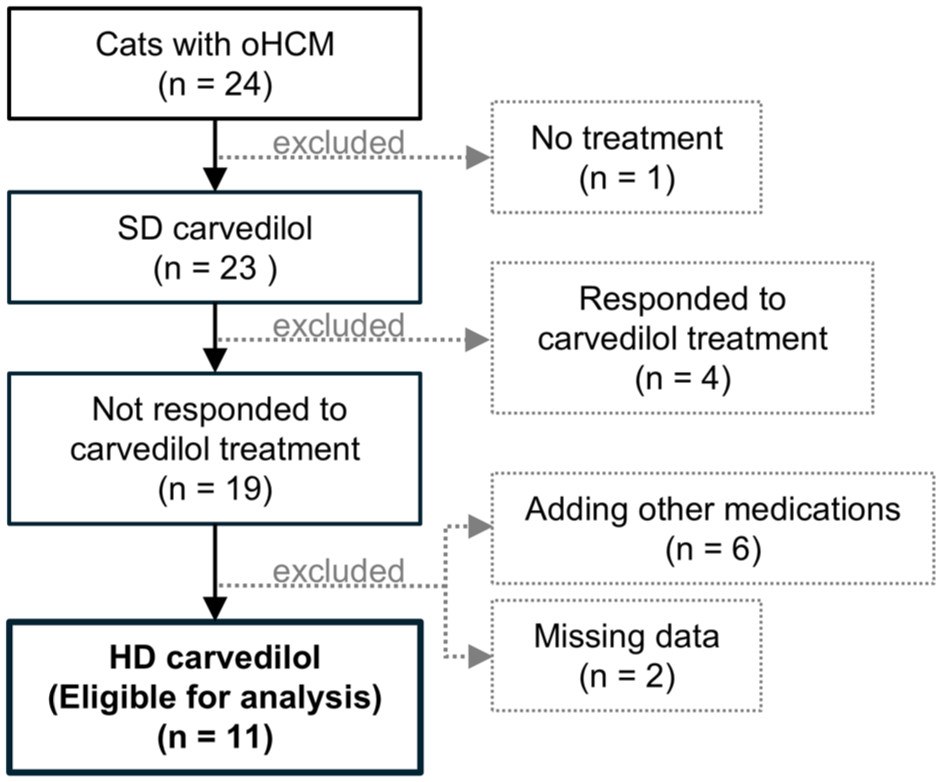
Flow diagram showing the eligible cases with obstructive hypertrophic cardiomyopathy and reasons for exclusion. HD = high-dose carvedilol treatment; oHOCM = obstructive hypertrophic cardiomyopathy; SD = standard-dose carvedilol treatment
Clinical profiles
The clinical characteristics are presented in Table 1. The median times required to determine the therapeutic effects of SD and HD carvedilol were 17 and 53 days, respectively. Heart rate (HR) decreased after HD treatment compared with before treatment and after SD treatment. There were no changes in body weight or systemic blood pressure. Three cats in this study had received prior medical treatment from their referring veterinarians before being enrolled. The breakdown was as follows: one cat received benazepril, clopidogrel and phenobarbital; the second cat received benazepril and torasemide; and the third cat received spironolactone and clopidogrel.
Clinical characteristics of 11 cats with hypertrophic cardiomyopathy
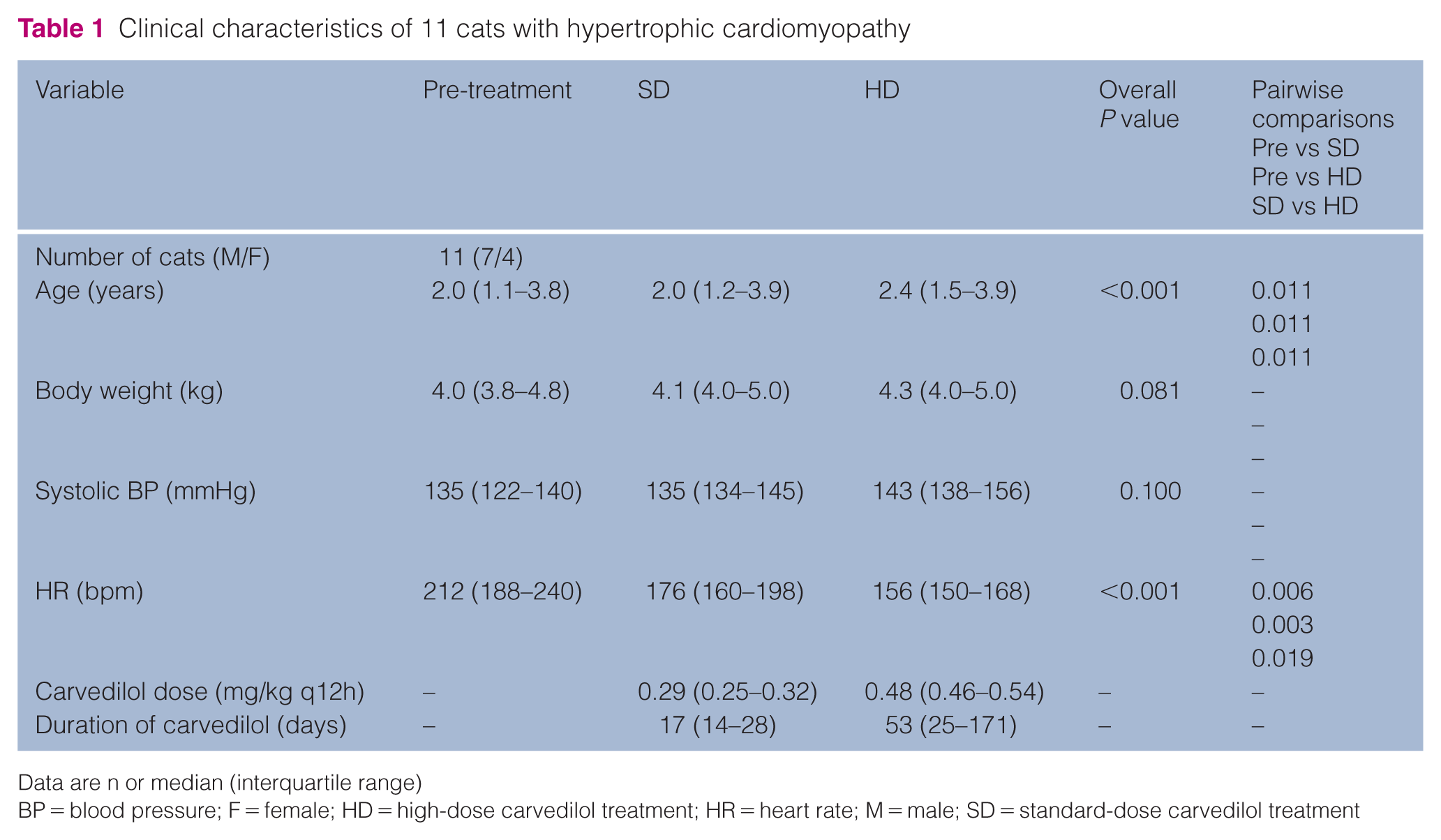
Data are n or median (interquartile range)
BP = blood pressure; F = female; HD = high-dose carvedilol treatment; HR = heart rate; M = male; SD = standard-dose carvedilol treatment
Of the 11 cats with oHCM, five were asymptomatic before treatment, while six presented with clinical signs such as a decrease in activity or appetite and open-mouth breathing. After SD carvedilol, clinical signs in all six cases were alleviated but persisted to some degree. After HD carvedilol, 5/6 cases achieved complete resolution of clinical signs; the remaining case showed decreased frequency of open-mouth breathing.
cTnI concentrations
Table 2 shows the cTnI results for each cat with oHCM before and after carvedilol treatment. Before treatment, the cTnI concentrations in 8/10 cats exceeded the RI (median 0.334 ng/ml [IQR 0.117–0.931]). Although the cTnI concentrations at the SD and HD assessments were lower than before treatment (SD 0.192 ng/ml [IQR 0.111–0.377; HD 0.018 ng/ml [IQR 0.009–0.161), only the value at the HD assessment showed statistical significance (before vs SD P = 0.043; before vs HD P = 0.043; SD vs HD P = 0.043). Of the 11 cats, seven were within the RI after HD carvedilol treatment.
cTnI concentrations of 11 cats with hypertrophic cardiomyopathy

cTnI = cardiac troponin I; HD = high-dose carvedilol treatment; ND = no data; SD = standard-dose carvedilol treatment
Conventional echocardiography
The standard echocardiographic parameters are shown in Table 3. IVSd, LVPWd and the maximum wall thickness decreased after SD and HD treatment compared with values before treatment. The LVOTVrest of one cat was below 3.5 m/s at study inclusion; however, the LVOTVexcited was above 3.5 m/s. Although LVOTVrest decreased to below 2.5 m/s in seven cats with OHCM, all cats still had an LVOTVexcited of 2.5 m/s or higher after SD carvedilol treatment. However, HD carvedilol significantly decreased LVOTVrest and LVOTVexcited to below 2.5 m/s in 10 cats with oHCM (Figure 2a,b).
Results of measurement of echocardiographic variables in 11 cats with stage B1 hypertrophic cardiomyopathy

Data are median (interquartile range)
e′ = peak velocity of early diastolic mitral annular motion; E:A = ratio of the peak early diastolic and late diastolic trans-mitral wave velocities; E vel = peak early diastolic trans-mitral wave velocity; FS = fractional shortening; HD = high-dose carvedilol treatment; IVSd = end-diastolic interventricular septal thickness; LA:Ao: left atrium:aorta ratio; LV = left ventricle; LVIDd = end-diastolic left ventricular internal dimension; LVOTV= left ventricular outflow tract velocity; LVPWd = end-diastolic left ventricular posterior wall thickness; RWT = relative left ventricular wall thickness; SD = standard-dose carvedilol treatment
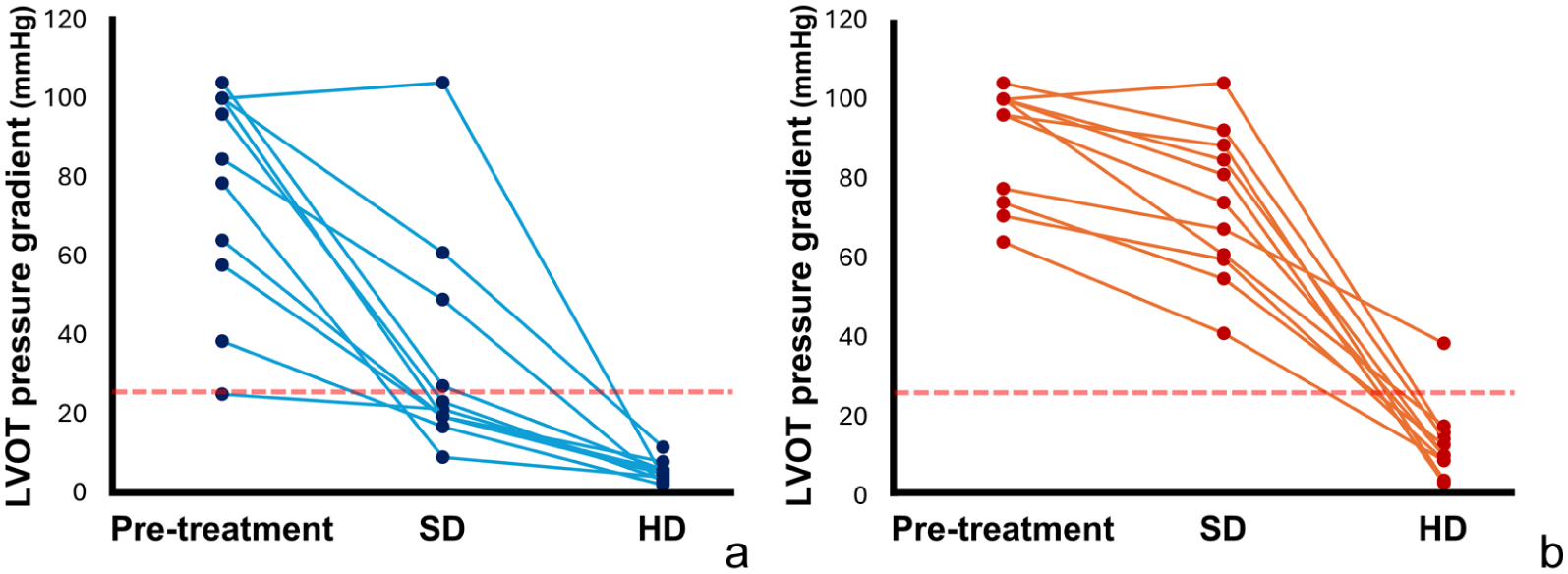
Line graphs showing the change in LVOT pressure gradient calculated from the LVOTV of 11 cats with obstructive hypertrophic cardiomyopathy over the treatment course. (a) LVOT pressure gradient calculated from LVOTVrest; (b) LVOT pressure gradient calculated from LVOTVexcited. Red dashed lines show the value of the treatment goal in this study (LVOT pressure gradient <25 mmHg). HD = high-dose carvedilol treatment; LVOT, left ventricular outflow tract; LVOTV = left ventricular outflow tract velocity; LVOTVexcited = maximum LVOTV value; LVOTVrest = minimum LVOTV value; SD = standard-dose carvedilol treatment
Two-dimensional speckle-tracking echocardiography
Two-dimensional STE parameters are shown in Table 4. The endocardial and epicardial SL were improved after SD or HD treatment compared with before treatment. However, no difference was observed after SD and HD treatment. The SC in the endocardial, epicardial and whole layers were not different before treatment and after SD and HD treatments.
Myocardial strain values in 11 cats with stage B1 hypertrophic cardiomyopathy

Endo:Epi = endocardial:epicardial ratio; HD = high-dose carvedilol treatment; SD = standard-dose carvedilol treatment
Correlation analyses
The cTnI concentrations showed positive correlations with LVOTVrest and LVOTVexcited. In particular, LVOTVexcited had a stronger correlation with the cTnI concentrations than LVOTVrest. In addition, the cTnI concentrations were negatively correlated with SL in all layers, but not with SC. Furthermore, SL in the epicardium was negatively correlated with LVOTVrest and LVOTVexcited (Table 5).
Correlations between cardiac troponin I concentration, left ventricular outflow tract velocity and myocardial strain in 11 cats with stage B1 hypertrophic cardiomyopathy

cTnI = cardiac troponin I; LVOTV = left ventricular outflow tract velocity
Discussion
The present study demonstrates a dose-dependent effect of carvedilol in alleviating LVOTO in cats with stage B1 oHCM for which SD carvedilol treatment was insufficiently effective. In addition, HD carvedilol treatment reduced the cTnI concentrations, suggesting less myocyte damage and improved clinical signs, possibly due to the alleviation of LVOTO. These beneficial effects were observed without causing excessive reduction in myocardial function or hypotension through the negative inotropic, negative chronotropic and vasodilating effects of carvedilol. These results suggest that HD carvedilol may provide a therapeutic option for cats with stage B1oHCM refractory to SD carvedilol treatment.
The commonly used dosage of carvedilol in cats is in the range of 0.1–0.3 mg/kg q12h.20,22 This study observed that HD carvedilol treatment achieved a dose-dependent alleviation of LVOTO in cats with oHCM, which was not attained with SD carvedilol. Although HD carvedilol treatment raises concerns about the side effects of excessive bradycardia and α1-blockade-induced hypotension, these were not observed in any cat after HD carvedilol treatment in this study. Therefore, HD carvedilol (up to 0.5–0.6 mg/kg q12h) could be considered acceptable in cats with stage B1 oHCM, similarly to humans. 27
Although no cats exhibiting excessive bradycardia were observed, the HR (median 156 beats/min) observed in HD could be considered clinically bradycardic. 28 However, the reduction in HR observed with carvedilol was associated with prolonged diastolic filling time and ejection acceleration time, which may contribute to the improvement of LVOTO and lead to haemodynamic stabilisation. Furthermore, IVSd, LVPWd and maximal LV wall thickness were reduced after SD and HD carvedilol treatments compared with the pre-treatment values. These morphological improvements in the LV might also be attributed to the alleviation of LVOTO and pressure overload by carvedilol, owing to its unique α1-blocking action and pleiotropic effects not found with atenolol. Although α1-blockade-induced hypotension was not observed, it is also possible that the reduction in myocardial wall stress contributed to the improvement in myocardial wall thickness.
Carvedilol decreased LVOTV in a dose-dependent manner, accompanied by a decrease in cTnI concentrations. Although the effects of carvedilol on cTnI concentrations in humans with oHCM have not been well documented, recent clinical trials of cardiac myosin inhibitors have demonstrated that relief of LVOTO is associated with a reduction in cTnI concentrations. 8 Notably, cTnI concentrations have been shown to increase again after drug washout, supporting a direct relationship between LVOTO severity and ongoing myocardial injury. These findings suggest that myocardial injury, reflected by elevated cTnI concentrations, is at least partly driven by the haemodynamic burden of LVOTO. Accordingly, although this study could not clarify the mechanisms underlying the results of cTnI, the reduction in cTnI concentrations observed in the present study may potentially reflect decreased myocardial stress secondary to LVOTO alleviation in cats with oHCM. In addition, in cats, elevated cTnI concentration is a known poor prognostic factor, and higher cTnI concentrations have been reported in oHCM compared with non-oHCM.29 –31 From this perspective, therapeutic strategies aimed at alleviating LVOTO may have clinical relevance; however, the clinical significance of this reduction and its impact on long-term prognosis remain to be elucidated in future studies.
This study attempted to evaluate LVOTO in resting and excited states. The SD carvedilol treatment resulted in an improvement in both LVOTVrest and LVOTVexcited compared with before treatment; however, none of the cats reached the target treatment value of 2.5 m/s for LVOTVexcited. In contrast, HD carvedilol treatment led to a further improvement in LVOTVrest and enabled 10/11 cats to reach this target for LVOTVexcited. These findings suggest that assessing only LVOTVrest might underestimate the severity of LVOTO in cats with oHCM and that LVOTVexcited could reveal the potential severity of obstruction. In humans with oHCM, when the resting pressure gradient is below 30 mmHg, it is recommended that the pressure gradient is reassessed during a stress test. 9 There is currently no consensus regarding optimal assessment methods for dynamic obstruction in cats, and exercise- or pharmacologically induced stress testing is not clinically practical in this species. Consequently, sympathetic stimulation during examination, which may provoke increases in LVOTO in cats, could be considered analogous to stress testing in humans, facilitating the identification of latent obstruction and associated haemodynamic burden. In addition, the stronger correlation with the cTnI concentrations observed in LVOTVexcited than in LVOTVrest suggest that LVOTVexcited may better reflect myocardial injury than LVOTVrest in cats, which is one of the reasons why assessment using LVOTVexcited is important.
The pre-treatment SL was lower than the range obtained from normal cats in a previous study. 25 These results are consistent with those of previous studies showing that a decrease in SL has been observed in humans and cats with early-stage HCM.32,33 In addition, improvements were observed with carvedilol in the SL of the epicardial and endocardial layers. Moreover, negative correlations were observed between the cTnI concentrations and SL in the whole, endocardial and epicardial layers, but no such correlations were observed for SC. Our results indicate that carvedilol might improve longitudinal myocardial function and protect myocardial cells in cats with oHCM through the alleviation of LVOTO.
In contrast, there were no significant changes between pre- and post-treatment SC. Circumferential motion plays an important role in the pump function of patients with heart disease and it is considered to compensate for the impairment of longitudinal motion.34,35 Our results for SC were not consistent with those of a previous study, in which SC improved after carvedilol treatment. 18 A possible reason for this conflict is that the improvement in SC due to alleviation of LVOTO was counteracted by the dose-dependent negative inotropic effects of carvedilol. Even so, carvedilol did not worsen SC, but rather improved SL, suggesting that carvedilol improved overall myocardial function in cats with oHCM.
This study had several limitations that should be considered when interpreting the results. The small sample size and the absence of a control group, such as cats with non-oHCM, render the findings less definitive. Therefore, large-scale, placebo-controlled investigations are warranted in future research. Another consideration is the potential for selection bias, as only cats that responded to carvedilol were included. In humans with oHCM, there are cases that show non-responsiveness to β-blockers.9,24 Therefore, similar cases may exist in cats, in which case further intensification of treatment might be necessary. In addition, the cut-off value for LVOTO was set at 3.5 m/s, and only cats with ACVIM stage B1 oHCM were included. Therefore, further studies that include cats with more advanced disease are required to evaluate the efficacy of HD carvedilol in feline oHCM. The variability in the duration of carvedilol administration may also have influenced the results. The absence of uniform evaluation time points after carvedilol initiation, especially for the HD cohort, introduces a confounding variable that limits the precise assessment of the pure carvedilol treatment effect. Similarly, the effect of other medications should be considered. This study included cats that were prescribed drugs other than carvedilol. Although no changes in medications were made during the study period, other than carvedilol, this was likely to be a confounding factor. Finally, the absence of a pathological diagnosis is another limitation. The diagnosis of HCM was based on echocardiographic findings, and all examinations were performed by a single specialist.
Conclusions
This study demonstrated the clinical efficacy of HD carvedilol in cats with oHCM, when treatment with SD carvedilol did not improve LVOTO. The alleviation of LVOTO was associated with improvements in myocardial hypertrophy, myocardial cell injury and myocardial function. Although the lack of a control group limits definitive conclusions, our results might provide clinical evidence for the safety and potential benefit of dose escalation in cats with stage B1 oHCM.
Footnotes
Author note
The data sets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was partially supported by the Japan Society for the Promotion of Science (grant numbers 22K05995 and 25K09425).
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.