
Abstract
Objectives
The aim of the present study was to evaluate the clinical efficacy of a modified perineal urethrostomy (PU) technique using preputial mucosa in male cats with recurrent urethral obstruction, and to assess the associated learning curve based on surgical proficiency and complication trends.
Methods
A total of 30 male cats with recurrent urethral obstruction treated between 2019 and 2024 were retrospectively reviewed. The modified PU involved reconstruction of the urethral stoma using preputial mucosa with partial dorsal skin anastomosis to enhance tissue stability. Postoperative urinary function and complications were assessed at 10, 21 and 60 days, and up to 3 years in selected cases. Surgical proficiency was analysed through a cumulative sum (CUSUM) analysis of operative time and complication incidence.
Results
All cats resumed voluntary urination within 48 h of surgery, and none exhibited persistent dysuria or urinary incontinence. Minor wound dehiscence occurred in two (6.7%) cats, and one (3.3%) cat developed a stomal stricture that resolved with balloon dilation; however, no revision surgeries were required. No cases of peristomal dermatitis or increased bacterial cystitis were detected. The median surgical time decreased from 71 mins in early cases to 54 mins in later procedures, and the CUSUM curve demonstrated a consistent decline in complication frequency, indicating progressive procedural mastery. Compared with previously reported stricture rates in the range of 7–9% for conventional Wilson-type PU techniques, our findings suggest that this modified technique results in lower complication rates and enhanced reproducibility, even in primary care settings.
Conclusions and relevance
This modified PU technique incorporating preputial mucosa provides stable urinary patency, low complication rates and favourable cosmetic results. By minimising direct mucocutaneous tension and preserving mucosal integrity, this approach may reduce the risk of stomal stenosis and postoperative infection. The procedure demonstrates a short learning curve and appears to be a reliable, anatomically sound alternative for managing recurrent urethral obstruction in cats.
Plain language summary
Some male cats suffer from a serious condition called urethral obstruction, which blocks their ability to urinate. When this happens repeatedly, surgery may be needed to create a new opening to allow urine to pass. This study looked at a modified surgical technique using tissue from the cat’s prepuce (the area surrounding the penis) to improve the outcome of this procedure, called perineal urethrostomy (PU). We reviewed the medical records of 30 male cats that had this modified surgery between 2019 and 2024. The new method used preputial tissue to form the new urinary opening. We checked how well the cats recovered, if they had any problems after surgery and how easy it was for surgeons to learn the technique. Most cats recovered well, with no problems urinating. Only one cat had a narrowing of the new opening and two cats had mild wound issues, but none needed another surgery. No increase in bladder infections or skin irritation was found. Over time, the surgery became faster and fewer problems occurred, showing that it is a learnable and reliable technique. This modified PU method seems to offer several advantages, including better healing, fewer complications and a more natural appearance. It may also help prevent infections and narrowing of the opening due to the special properties of the preputial tissue.
Keywords
Introduction
Urethral obstruction represents one of the most frequent and clinically significant urological emergencies in male cats. The condition commonly arises from the formation of struvite or calcium oxalate uroliths, accumulation of urethral plugs comprising mucus and cellular debris, or intraluminal inflammation secondary to urinary tract infections (UTIs). In addition to these mechanical causes, functional obstruction related to feline idiopathic or interstitial cystitis may provoke urethral spasm and transient luminal narrowing, further exacerbating disease severity.1,2
For cats experiencing recurrent or refractory obstruction, perineal urethrostomy (PU) remains the procedure of last resort to restore permanent urinary patency. 3 The Wilson technique continues to be regarded as the surgical standard and generally achieves satisfactory postoperative urinary function.4 –6 Nevertheless, subsequent long-term evaluations have revealed complications, including stomal stenosis, urine-induced peristomal dermatitis and recurrent bacterial cystitis, attributable to chronic exposure of the mucocutaneous junction and local mechanical tension.5,7 These limitations have prompted the development of multiple technical modifications aimed at improving both functional and cosmetic outcomes.8,9
Among these innovations, PU procedures incorporating preputial mucosa have demonstrated theoretical advantages by creating a non-haired, elastic mucosal interface that may minimise chronic irritation, enhance stoma visibility and preserve a more physiological urinary outflow. 10 A Japanese report published in 1982 documented four successful feline cases using this approach; 11 however, the description remains confined to the Japanese literature and is largely inaccessible internationally. A subsequent English-language study similarly introduced a PU technique using preputial mucosa but provided limited clinical data and no evaluation of its reproducibility or learning curve. 10 Consequently, there remains a paucity of rigorous, English-language evidence quantifying the clinical utility of this surgical modification in contemporary feline practice.
This modified PU procedure was originally designed to minimise direct contact between the urethral mucosa and skin, thereby reducing the risk of long-term complications, such as recurrent obstruction and dermatitis. The author learned this surgical approach during clinical training and has performed the modified PU technique in 30 cats between 2019 and 2024.
The limited dissemination of this modified PU technique in the international literature represents a potential gap in the current knowledge of veterinary urology. Therefore, this study was designed to address this gap by providing a comprehensive clinical evaluation of a modified preputial mucosa PU technique performed in a primary care setting. The modification was intended to minimise direct contact between urethral and cutaneous tissues, thereby reducing tension-related complications such as stenosis and dermatitis while preserving local mucosal integrity. The objective of this study was to retrospectively evaluate the postoperative urinary function, complication rates and surgeon’s learning curve in 30 consecutive feline cases to determine the reproducibility and potential clinical advantages of this technique in everyday practice.
Materials and methods
Animals
This retrospective observational study evaluated 30 male cats with recurrent urethral obstruction that were treated using a modified PU technique at a primary care veterinary hospital in Chiba, Japan, between April 2019 and April 2024. The inclusion criteria were male cats of any age that had experienced more than one episode of urethral obstruction. There were no exclusion criteria. All cases were managed by the same surgeon.
Anaesthesia and preoperative management
Premedication consisted of midazolam (0.2 mg/kg IM, Dormicum; Maruishi Pharmaceutical), butorphanol tartrate (0.15 mg/kg IM, Vetorphale; Meiji Seika Pharma) and medetomidine hydrochloride (20 µg/kg IM, Domitor; Nippon Zenyaku Kogyo). General anaesthesia was induced and maintained with isoflurane (Toa Pharmaceuticals) in oxygen. Intravenous fluids were administered throughout the procedure, adjusted according to hydration status and electrolyte balance.
For perioperative analgesia, meloxicam (0.3 mg/kg SC, Metacam 0.5% injectable; Boehringer Ingelheim) was administered preoperatively. In addition, buprenorphine (0.02 mg/kg IM or transmucosally q12h, Lepetan; Otsuka Pharmaceutical) was provided for 4 days postoperatively.
Positioning and surgical preparation
Cats were positioned in ventral recumbency with the pelvis elevated. The perineal region was clipped and aseptically prepared using a povidone–iodine solution. A purse-string suture was placed in the anus to prevent intraoperative faecal contamination.
Surgical technique
A midline elliptical skin incision was made extending from the caudal margin of the prepuce to approximately 2 cm ventral to the anus (Figure 1a). The incision converged dorsal towards the preputial orifice. The penis was carefully dissected free from the preputial mucosa, with maximal preservation of the mucosal surface (Figure 1b). In two intact males, castration was performed concurrently. The penis was then reflected dorsally as in the standard Wilson technique, 4 and the adjacent connective tissue was sharply dissected. The ischiocavernosus muscles were transected to allow caudal traction of the urethra to expose the bulbourethral glands (Figure 1c). The retractor penis muscle was elevated and excised.
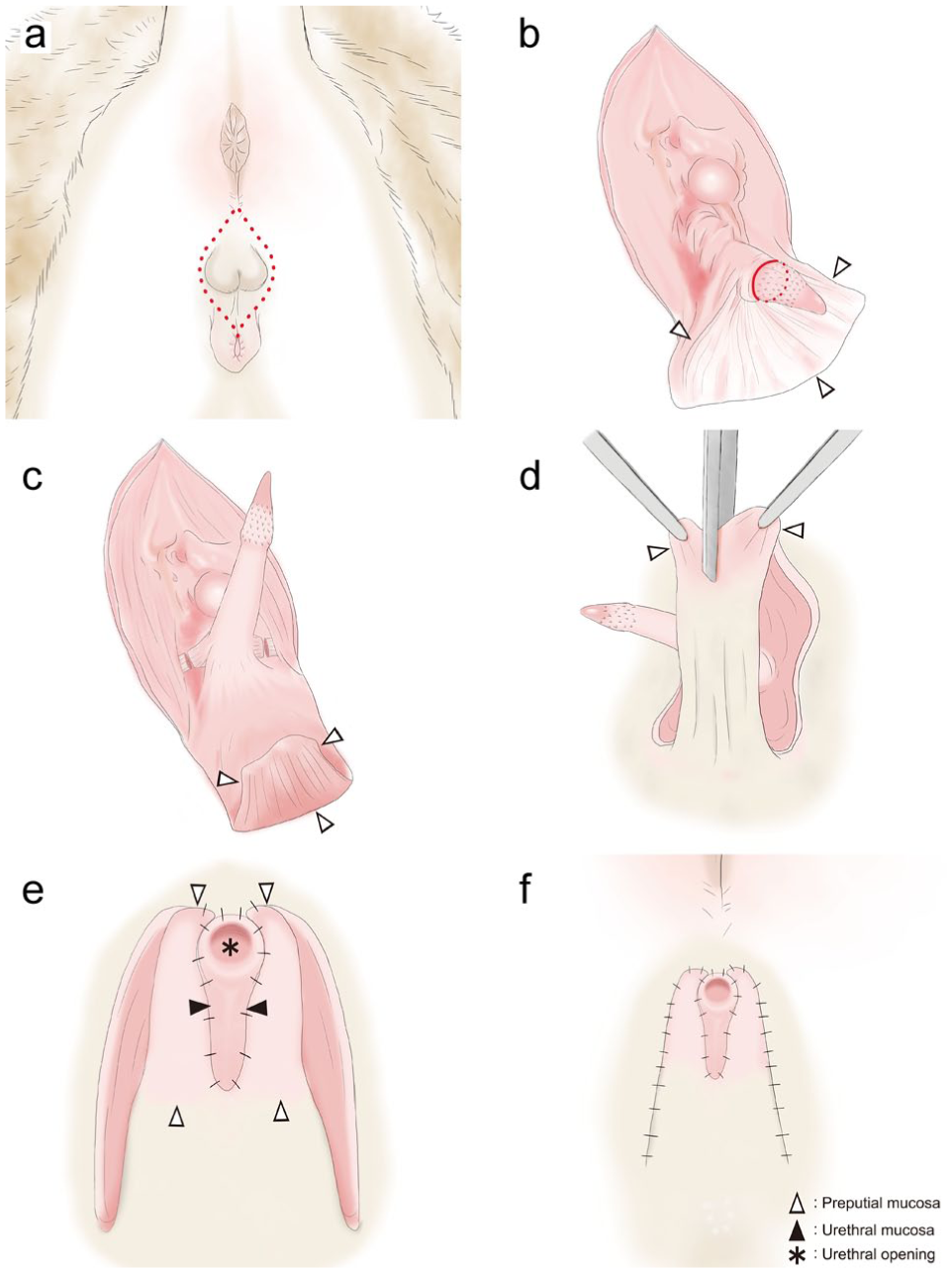
Step-by-step illustration of the modified perineal urethrostomy procedure using preputial mucosa in a male cat: (a) preoperative view of the perineal region. The red dotted line indicates the planned elliptical skin incision; (b) the dissection line between the penis and preputial mucosa is indicated by red solid and dotted lines. The dissection was designed to preserve as much preputial mucosa as possible; (c) transection of the ischiocavernosus muscles and exposure of the bulbourethral glands; (d) the preputial mucosa is retracted bilaterally and bisected vertically along the midline; (e) the dorsal urethral mucosa is first sutured to the overlying skin to stabilise its position. Each side of the preputial mucosa is then sutured to the corresponding edge of the urethral mucosa using simple interrupted sutures; and (f) the final stoma is reconstructed in layers as follows: urethral mucosa, preputial mucosa and skin. The completed stoma immediately after surgery demonstrates a satisfactory cosmetic appearance. △ = preputial mucosa; ▲ = urethral mucosa; * = urethral opening
Ventral dissection between the pelvic urethra and the pelvic symphysis was performed to permit gentle mobilisation of the urethra and reduce tension at the anastomotic site. The urethra was incised longitudinally from the external urethral orifice to the level of the pelvic urethra, confirming that a 10 Fr catheter could pass smoothly through the lumen. The distal third of the penis was ligated using 3-0 absorbable monofilament suture (Monodiox; Alfresa Pharma) and excised. The incised preputial mucosa was divided longitudinally at the midline (Figure 1d) and retracted laterally. The urethral mucosa was first anchored dorsally to the overlying skin to stabilise its position. Each side of the preputial mucosa was then sutured to the corresponding edge of the urethral mucosa using 4-0 or 5-0 absorbable monofilament sutures (Monodiox; Alfresa Pharma) in a simple interrupted pattern (Figure 1e). Finally, the preputial mucosa was sutured to the skin to create a layered stoma, comprising – from inner to outer – urethral mucosa, preputial mucosa and skin (Figure 1f).
In the original version of this modified PU, the preputial mucosa circumferentially enveloped the urethral mucosa (360° coverage). In the present study, the method was refined to simplify the procedure and enhance mechanical stability. Specifically, the dorsal 30° of the urethral stoma was sutured directly to the perineal skin, while the remaining 330° was apposed to the preputial mucosa. This modification was based on intraoperative observations of the relative fragility and limited width of the preputial flap, as well as the predominantly ventral direction of urine outflow.
Upon completion, the anal purse-string suture was removed. All cats were fitted with an Elizabethan collar for 3 weeks postoperatively. Absorbable suture material was used in all cases; however, cats that tolerated handling had the cutaneous sutures removed on postoperative day 10.
Broad-spectrum antimicrobial therapy comprising cefotaxime (Claforan for Injection; Sanofi) or enrofloxacin (Baytril 2.5% Injection; Elanco Japan) was administered for 5 days postoperatively. Although these antimicrobials do not conform to current first-line prophylactic recommendations, their use reflected the prevailing clinical practice in Japanese primary care settings at the time of this study. The surgical site was cleaned twice daily during hospitalisation to maintain asepsis.
Postoperative monitoring and evaluation
Clinical healing was defined as the absence of wound dehiscence, dysuria, urinary incontinence, stomal stenosis or peristomal dermatitis at postoperative days 10 and 21 and at the 2-month evaluation. All 30 cats were examined at least once within 21 days postoperatively, with none lost to follow-up during this period. A total of 15 cats were re-evaluated at approximately 2 months, whereas the remaining 15 did not return after the 21-day examination. The longest postoperative follow-up recorded in a single case in this series was 3 years 3 months. Blinded outcome assessment was not possible because the surgeries and follow-up assessments were performed by the sole veterinarian in a primary care facility.
Data collection and statistical analysis
The following variables were recorded for each cat: age, body weight, number of previous urethral obstructions, surgical time, duration of hospitalisation, and presence or absence of complications. Complications included wound dehiscence, transient urinary retention, stomal stenosis and peristomal dermatitis.
To assess the influence of surgical experience, cases were grouped chronologically as early (cases 1–10), middle (cases 11–20) and late (cases 21–30). Surgical time and complication frequency were compared among groups using one-way ANOVA followed by Tukey’s post hoc test. A cumulative sum (CUSUM) analysis was performed to evaluate the learning curve, with plotting of the cumulative deviations of each operative time from the mean. The CUSUM analysis was performed using an expected baseline complication rate of 17%, which served as the decision interval for assessing performance trends. A downward trend in the CUSUM curve indicated progressive procedural efficiency and stabilisation of outcomes. All statistical analyses were performed using EZR software, version 1.55 (Saitama Medical Center, Jichi Medical University). The data analyst was not blinded because the analysis was performed by the veterinarian who performed the procedures.
Results
The study cohort comprised 30 male cats with a median age of 5 years (range 1–13) and median body weight of 4.9 kg (range 3.1–7.6). All cats had a documented history of one to four prior episodes of urethral obstruction (median three). Of the cats, 28 were neutered, while two were intact; 27 cats were kept strictly indoors, while three had both indoor and outdoor access. The predominant breed was domestic shorthair (n = 19), followed by Munchkin (n = 4), Norwegian Forest Cat (n = 4), Russian Blue (n = 2) and Bengal (n = 1). The underlying aetiologies of urethral obstruction or stricture were medically refractory idiopathic lower urinary tract disease (n = 21), urolithiasis (n = 4) and iatrogenic urethral trauma secondary to catheterisation (n = 5).
Of the cats, 28 resumed voluntary urination within 24 h of surgery, and the remaining two voided spontaneously by postoperative day 2. No cats exhibited persistent dysuria or urinary incontinence; all 30 cats in the study cohort exhibited satisfactory healing by postoperative day 21. Once spontaneous urination resumed, all cats produced a strong, continuous urine stream without signs of discomfort.
Minor wound dehiscence occurred in two (6.7%) cats, both of which had accompanying superficial wound infection. The dehiscence was limited to the junction between the preputial mucosa and the surrounding skin, and all cases were successfully managed with local wound care and antimicrobial therapy based on culture and susceptibility results, achieving complete healing before 21 days by secondary intention without revision surgery. Three cats had transient urinary retention that resolved within 48 h with supportive management. Stomal stenosis developed in one (3.3%) case, whereas peristomal dermatitis was not observed in any case. The stenosis was unrelated to any wound dehiscence and resulted from self-trauma after premature removal of the Elizabethan collar at home. It was successfully corrected by balloon dilation under anaesthesia without further surgical intervention.
Although the modified PU technique differs from the original design by directly suturing the dorsal aspect of the urethral stoma to the perineal skin rather than to preputial mucosa, no cats experienced long-term stenosis or peristomal dermatitis (Figure 2).

Postoperative appearance of the perineal urethrostomy site over time in a representative case: (a) immediately after surgery; (b) postoperative day 10: no signs of inflammation or wound dehiscence are visible; and (c) 3 years after surgery: the stoma remains cosmetically favourable with no evidence of stenosis or peristomal dermatitis
The median surgical time was 71 mins (mean ± SD 73.5 ± 14) in the early group (cases 1–10), 54 mins (mean 54.9 ± 6) in the middle group (cases 11–20) and 56 mins (54 ± 7) in the late group (cases 21–30). One-way ANOVA revealed a significant difference in surgical time among the three groups (P = 0.00018). Tukey’s post hoc comparisons demonstrated significantly longer surgical times in the early group than in the middle (P = 0.0008) and late groups (P = 0.0005), whereas the difference between the middle and late groups was not significant (P = 0.9864) (Figure 3).

Surgical time across chronological groups. Comparison of surgical time among three groups of modified perineal urethrostomy cases categorised chronologically as early, middle and late. Each dot represents an individual cat. Horizontal bars indicate median values and error bars denote SD. Surgical time decreased significantly from the early to the middle and late groups (P <0.05). *P <0.05
The incidence of complications – defined as wound dehiscence, transient urinary retention, stomal stenosis or peristomal dermatitis – was 30% (n = 3) in the early group, 30% (n = 3) in the middle group and 0% (n = 0) in the late group. A CUSUM analysis was performed to assess the progression of surgical proficiency. The CUSUM curve demonstrated a consistent downwards trajectory with increasing case number, stabilising after approximately 20 cases (Figure 4). This trend indicated progressive refinement of the PU technique and a reduction in complication frequency with accumulated operative experience, suggesting a short and achievable learning curve.

Cumulative sum (CUSUM) analysis of surgical complications in 30 consecutive cats that underwent the modified perineal urethrostomy. The CUSUM score peaked at case 15 and subsequently decreased, stabilising at approximately case 20, indicating a reduction in complication rates and the presence of a measurable learning curve
Discussion
Two major postoperative complications of PU in cats – stomal stenosis and ascending bacterial cystitis – remain significant challenges affecting long-term surgical outcomes.5,6 The present study evaluated the clinical efficacy of a modified PU technique incorporating preputial mucosa to mitigate these complications while maintaining the functional and structural stability of the urethral stoma.
Traditional PU techniques, such as the Wilson method, are frequently associated with postoperative narrowing of the urethral stoma and urine-induced peristomal dermatitis.5,6 Although the incidence of these complications tends to decline with surgical experience, their occurrence can be clinically significant and may require revision surgery. Excessive tension at the mucocutaneous junction and limited tissue elasticity are recognised as major predisposing factors for these complications. PU can result in cranial displacement of the pelvic urethra, likely caused by cranial traction from the bladder, 12 and may lead to suture line distortion, inwards invagination or exposure of the pelvic urethra to the external environment.
Histological investigations in humans have demonstrated that preputial mucosa contains abundant elastic fibres within the dartos muscle layer, providing a compliant, shock-absorbing buffer against tensile stress. 13 Although species-specific differences exist, a comparable biomechanical function may be expected in feline tissue. In the present modification, interposing preputial mucosa between the urethral and cutaneous layers may serve as an elastic interface that dispersed mechanical tension and preserved the contour and patency of the stoma.
In addition to mechanical complications, the increased incidence of bacterial cystitis reported after conventional PU is a persistent concern.5,6,10 In the present study, no postoperative increase in cystitis was observed. A plausible explanation is that partial cranial retraction of the urethral mucosa within the stoma may protect the pelvic and mid-urethral epithelium from continuous environmental exposure. Chronic mucosal irritation is known to induce squamous metaplasia, leading to reduced mucus production and loss of innate antimicrobial protection. 14 By preserving intact transitional epithelium, the modified PU technique used in the present study may help maintain mucosal immune defence and prevent infection. 15 The absence of peristomal dermatitis in the present series may further contribute to reduced local inflammation and scarring, which are recognised risk factors for bacterial infection. 16 However, postoperative UTIs may have been underdetected, as no active surveillance urine cultures were performed and follow-up was limited to 21 days in half of the cases. Given that UTIs can remain a lifelong risk after PU, longer term monitoring would be required to confirm the true incidence.
When compared with previously published outcomes, the present findings appear favourable. Reported restenosis or stricture rates after conventional PU are in the range of 7–9% in long-term studies.5,6 In contrast, the stenosis rate observed in the present cohort was 3.3%, and no cat required surgical revision. Although 15/30 cases were evaluated only within the short-term follow-up period, this result suggests that the modified PU approach achieves comparable or superior patency and long-term tissue stability relative to standard techniques. However, postoperative stenosis may have been underdetected in this cohort, as the average onset reported in previous studies (eg, 71 days in the Phillips and Holt 17 study) occurs well beyond the 21-day follow-up available for half of the cases. Therefore, the low incidence observed here should be interpreted with caution, and longer term monitoring would be required to confirm the true rate of delayed-onset stenosis. The low incidence of infection and absence of dermatitis in the present study further support its structural and physiological advantages.
A progressive improvement in surgical performance was evident with increasing experience. The operative time decreased significantly after approximately 10 cases, while the CUSUM analysis revealed a steady downwards trend that stabilised after approximately 20 cases, signifying reduced complication frequency and improved procedural consistency. These results indicate that the learning curve for this technique is relatively short and that the procedure can be mastered efficiently in a primary care environment (Figure 4).
The one case of restenosis was attributed to self-inflicted trauma after premature removal of the Elizabethan collar after discharge. This event prompted a revision of postoperative management protocols at the author’s institution, with the period of Elizabethan collar use extended to 3 weeks. Since the implementation of this policy, no further cases of restenosis have occurred, underscoring the importance of strict postoperative care in preventing wound complications.
The present study has several limitations. As a retrospective investigation of surgeries performed by a single surgeon in a primary care setting, the findings may not be fully generalisable. Furthermore, the analgesic protocol comprising meloxicam and buprenorphine was limited compared with multimodal approaches that include local blocks or continuous opioid infusions. However, this analgesic regimen was chosen considering the practical constraints of a primary care environment and the temperament of feline patients. In addition, the follow-up period was inconsistent among cases, with limited long-term observation for some cats. As a result, both postoperative UTI and delayed-onset stenosis may have been underdetected, particularly given that active surveillance urine cultures were not performed and that stenosis is reported to occur much later (eg, 71 days in the Phillips and Holt 17 study) than the available follow-up in many cases. Prospective, multicentre studies with extended follow-up are warranted to validate the durability and broader applicability of this modified PU technique.
Conclusions
The modified PU technique incorporating preputial mucosa achieved functional outcomes equivalent to those of conventional methods, while demonstrating a lower incidence of postoperative complications, including stomal stenosis and bacterial cystitis. These reductions in the risks of complications may result from the provision of biomechanical buffering and preservation of mucosal integrity. These findings suggest that the modified PU technique provides both structural and physiological advantages that may enhance long-term surgical success in cats with recurrent urethral obstruction. The combination of low complication rates, favourable cosmetic outcomes and a short learning curve suggests that this approach represents a reliable and reproducible alternative to conventional PU methods for the management of recurrent urethral obstruction in cats.
Footnotes
Author note
The data supporting the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.