
Abstract
Objectives
Postoperative stenosis of the urethral orifice is a potential complication of perineal urethrostomy (PU), often caused by inadequate periurethral dissection leading to craniocaudal tension on the stoma. The aim of this study was to evaluate the length of the urethra translated caudally at each step of the dissection of the penile urethra during PU.
Methods
Staged dissection for PU was performed on 14 male cat cadavers. Measurements of urethral length were recorded at each stage using digital callipers and standardised traction. Location of the bulbourethral glands (BUGs) relative to the caudal aspect of the ischium was documented. Descriptive statistics were performed.
Results
Each stage of dissection led to an increase in urethral translation length, with an overall mean increase of 17 ± 1.94 mm. The most significant increase occurred after blunt dissection of the fibrous attachments between the ventral surface of the urethra and the dorsal surface of the pubis, extending to the pubic brim, accounting for 43.1% of the total translation length. Ventral dissection resulted in a 3.9-fold increase in urethral translation length compared with dorsal dissection. After the final stage of dissection, BUGs were either level with the caudal edge of the ischium or below the ischium.
Conclusions and relevance
Ventral dissection of the fibrous attachments between the urethra and pelvis effected significant caudal translation of the urethra. This step is crucial for minimising tension on the final stoma and reducing the risk of postoperative stenosis for PU.
Introduction
Perineal urethrostomy (PU) is a surgical procedure commonly performed in male cats affected by recurrent urethral obstruction. PU is frequently utilised as a salvage procedure in cases where patients have not responded adequately to medical therapies. These cases may include multiple catheterisations as a result of recurrent feline lower urinary tract disease, penile/urethral trauma, urolithiasis and penile mass.1 –3 The PU approach creates a new and permanent opening at the more proximal pelvic urethra, which is nearly twice the diameter of the penile urethra, thereby reducing the risk of obstructions.4,5
Although PU has been shown to be an effective treatment option, it has a reported short-term complication rate of 13–62.2%, and a long-term complication rate of 14.3–31.8%.1 –3,6,7 Postoperative stenosis of the urethral orifice is a commonly reported complication, with a prevalence of 2.5–20%, often due to poor surgical technique.2,6 –10 In 2006, Phillips and Holt 10 reported that 8/11 cats required revision because of inadequate dissection of the penile urethra from its attachments at the ischium to the level of the bulbourethral glands (BUGs). In that study, excessive tension on the mucocutaneous junction apposition and suturing of narrower penile urethra subsequently led to contraction and the development of stenosis. 10
The long-standing recommendation for dissection to the level of the BUGs during PU is based on the quantitative evidence demonstrating that the urethra is wider at this location. 4 In addition, it has been suggested that urethral mobilisation after PU occurs through caudal translation rather than elongation by stretching; however, there is limited information on the extent of urethral translation achieved during dissection. 11 To the authors’ knowledge, there is no comprehensive description of the surgical technique for maximising caudal translation of the pelvic urethra at each stage of the dissection or identifying the key steps that maximise this translation. This information would be valuable to veterinary surgeons for precise technical execution of PU. Therefore, the aim of the present study was to measure and document the length of the urethra translated caudally at each step of the dissection of the urethra during PU, from the initial dissection of penile attachments to the final mobilisation. It is the authors’ impression that maximising urethral translation may lead to reduced craniocaudal tension on the stoma, aiding in accurate, tension-free mucocutaneous apposition, uncomplicated wound healing, and the formation of a patent and appropriately sized stoma. We hypothesised that the greatest increase in translation would occur after the blunt dissection of the ventral fibrous attachments between the urethra and the dorsal surface of the pubis, to the level of the pubic brim.
Materials and methods
This cadaveric study was conducted at a single institution and involved male cat cadavers, each of which had died or been euthanased for reasons unrelated to this study. All cadavers were obtained post mortem from the University of Queensland, and ethical approval for the study was granted by the university’s Animal Ethics Committee (2023/AE000760). Pertinent data, including body weight, breed and neuter status, were collected. The cadavers were frozen and subsequently thawed at room temperature before dissection.
Each cat was positioned in sternal recumbency between two secured Perspex platforms. Two Steinmann pins were placed in predrilled holes within the Perspex, each through the mid-diaphysis of the femur, ensuring immobilisation during dissection and urethral measurements. After immobilisation, an elliptical incision was performed through the skin and subcutaneous tissue around the scrotum and prepuce. A pair of Allis tissue forceps was placed on the preputial attachments at the distal tip of the glans of the penis to apply traction on the urethra when taking urethral measurements.
All PU procedures and measurements were performed by a single board-certified surgeon using the modified technique described by Wilson and Harrison. 12 Staged dissection of the urethra was performed as described below, with the goal to exteriorise the BUGs to their maximum extent. The length of the urethral tract was measured using digital callipers and recorded during each stage of dissection of the penile and pelvic urethra. After each stage of dissection, a force of 2 N was applied to the Allis tissue forceps using a digital force gauge, which was held parallel to the pelvic floor. This was performed to straighten the urethra and obtain the most accurate measurement without grossly stretching the urethral tissue. The first measurement was obtained after dissection of the subcutaneous tissue, and once the loose connective tissue that surrounds the penis had been dissected free from the penis. This measurement was taken from the caudal edge of the ischial tuberosity to the tip of the glands, which was then divided by two to obtain a second measurement. This point along the urethra was marked by the placement of a circumferential ligature and used as a reliable landmark for measurement (Figure 1). This measurement (S0) was subtracted from each subsequent measurement, so that gross increase in urethral translation was reported. After each stage of dissection, the length between the caudal aspect of the ischium and the urethral suture was obtained (Figure 2). The penile urethra was lifted dorsally to expose the ventral attachments. The stage 1 (S1) measurement was taken after transection of the ventral penile ligament (Figure 3). The stage 2 (S2) measurement was taken after transection and release of the ischiocavernosus muscle and ischiourethralis muscle from their insertion on the ischium (Figure 4). The stage three (S3) measurement was taken after intrapelvic finger dissection of the fibrous attachments located between the urethra and the dorsal surface of the pubis was performed, to the level of the pubic brim (Figure 5). The stage 4 (S4) measurement was obtained after transection of the connective tissue located lateral and cranial to the ischiocavernosus muscle (Figure 6). The penile urethra was then retracted ventrally to expose the dorsal urethra. The stage 5 (S5) measurement was taken after transection of the superficial dorsal connective tissue and the retractor penile muscle (Figure 7). The stage 6 (S6) measurement was taken after transection of the remnant connective tissue located along the cranial aspect of the BUGs (Figure 8). These steps are summarised in Table 1.

Urethral ligature was placed serving as a landmark for subsequent measurements of translation. The top of the image corresponds to the dorsal aspect of the cat

Measuring urethral length between the caudal ischium and urethral suture. The top of the image corresponds to the cranial aspect of the cat
Transection of ventral penile ligament. The top of the image corresponds to the dorsal aspect of the cat

Transection of ischiocavernosus and ischiourethralis muscle. The top of the image corresponds to the dorsal aspect of the cat

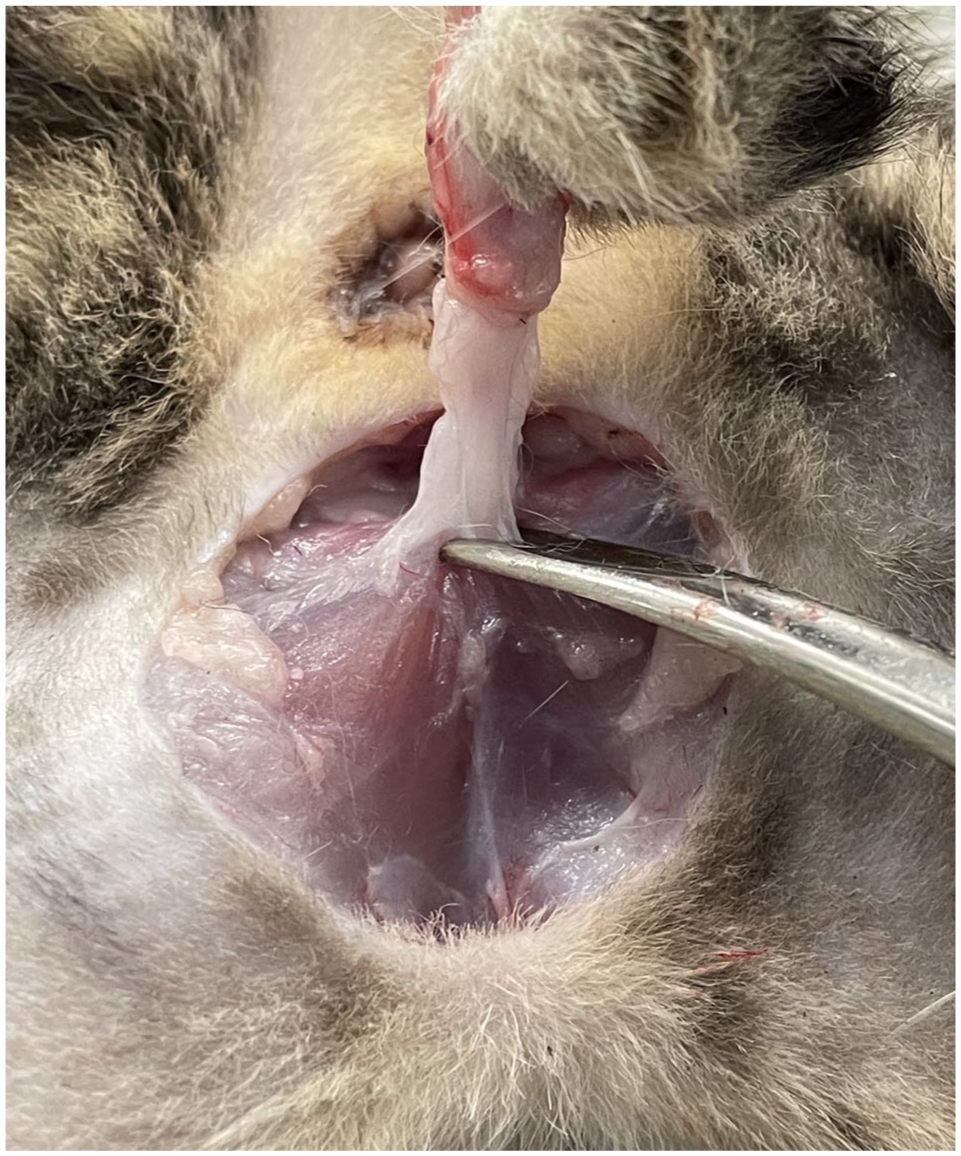
(a) Fibrous attachments between the urethra and dorsal surface of the pubis and (b) after blunt intrapelvic dissection of the fibrous attachments. The top of the image corresponds to the dorsal aspect of the cat

(a) Connective tissue lateral and cranial to the ischiocavernosus and ischiourethralis muscle and (b) after transection of the connective tissue. The top of the image corresponds to the dorsal aspect of the cat

Transection of superficial dorsal connective tissue and retractor penile muscle. The top of the image corresponds to the dorsal aspect of the cat

(a) Transection of remnant connective tissue along the cranial aspect of the bulbourethral glands and (b) the urethra at the end of the dissection. The top of the image corresponds to the dorsal aspect of the cat
Stages of perineal urethrostomy dissection

After each stage of dissection, the Allis tissue forceps attached to the distal tip of the penile glans were suspended by the gravitational pull of the forceps, and it was observed whether the BUGs were above, level with or below the ischium.
Descriptive statistics were performed as appropriate and collected data reported as mean ± SD.
Results
A total of 14 male cat cadavers were obtained for the study. Nine cats were entire and five were castrated. The breeds represented were domestic shorthair (n = 13) and domestic mediumhair (n = 1). The median body weight was 3.07 kg (range 1.84–6.37).
Each stage of dissection resulted in an increase of length of urethral translation (Table 2). The mean increase in translation length after S1 was 1.67 ± 0.62 mm (Table 3). After S2, the translation length increased by a mean of 1.71 ± 0.78 mm. S3 resulted in a mean increase of 7.35 ± 1.9 mm. The mean increase after the dissection of S4, S5 and S6 was 2.76 ± 1.02 mm, 1.63 ± 0.86 mm and 1.89 ± 1.17 mm, respectively. The overall mean increase in urethral translation length was 17 ± 1.94 mm.
Baseline values of male cat cadavers and measurements recorded during stages of perineal urethrostomy

Bulbourethral glands (BUGs) positioned above the ischium
BUGs positioned level with the caudal margin of the ischium
BUGs positioned below the ischium
Change in length of urethral translation between each stage of dissection

The greatest increase in urethral translation was observed at S3, which accounted for 43.1% of the total length (Table 4). This increase occurred after the dissection of the fibrous attachments between the urethra and the dorsal surface of the pubis. In contrast, the smallest increase in urethral translation was recorded at S5, contributing only 9.7% to the total length.
Percentage change in length (%) of urethral translation between stages of dissection

When grouping the stages into ventral dissection (S1, S2, S3, S4) or dorsal dissection (S5 and S6), overall average translation lengths were 13.49 ± 2.38 mm (79.6%) and 3.52 ± 1.45 mm (20.4%), respectively. Ventral dissection resulted in a 3.9-fold increase in urethral translation length compared with dorsal dissection.
After S1 and S2, the BUGs were consistently positioned above the caudal margin of the ischium in all cadavers (Table 2). After S3, in 7/14 cadavers, the BUGs were aligned with the caudal edge of the ischium. By S4, this alignment was observed in 12/14 cadavers. At S5, the BUGs were located below the ischium in 6/14 cadavers, while in the remaining eight cadavers they were at the same level as the caudal aspect of the ischium. At S6, the BUGs in 10/14 cadavers were positioned below the ischium, with the remaining four still level with the caudal margin.
Discussion
This study documented the length of urethral translation during each stage of soft tissue dissection in PU on male cat cadavers. We hypothesised that the greatest percentage of urethral translation length would occur during the dissection of the ventral fibrous attachments between the urethra and dorsal aspect of the pubis, after transection of the ischiocavernosus and ischiourethralis muscles. In the present study, intrapelvic blunt dissection of the fibrous attachments located between the urethra and the dorsal surface of the pubis to the level of the pubic brim allowed for the largest increase in urethral translation (43.1% of the total length translated); therefore, we accepted our hypothesis. The results of the present study addressed a knowledge gap in the current literature by highlighting the importance of ventral dissection in achieving the greatest translation in urethral length, which may reduce tension on the stoma and lower the risk of postoperative stenosis after PU.
Creating a tension-free stoma during PU is critical for preventing postoperative stenosis. 10 The reported prevalence of postoperative stenosis has varied widely, from as high as 20% to as low as 2.5% in more recent reports.2,6 –9 The variation in stenosis rates may be due to differences in surgical experience or subtle variations in technique, leading to inadequate dissection and caudal translation. Without adequate caudal translation, increased craniocaudal tension on the stoma may lead to ischaemia, excessive inflammation and a higher risk of dehiscence resulting in overproduction of granulation tissue from secondary intention healing.13 –15 This, in turn, may exacerbate tissue scarring, ultimately increasing the risk of stenosis. 15 This complication may then lead to adverse clinical outcomes, with stenosis-related euthanasia reported in up to 14.2% of affected cats.1,2,6,16 This study showed that ventral dissection accounted for 43.1% of the overall caudal urethral translation, underscoring its importance in reducing tension on the stoma.
A long-standing recommendation when performing a PU is to dissect to the level of the BUGs because of the wider urethral diameter at this location and therefore optimisation of stoma size.4,5 A stoma that accommodates an 8 Fr or larger catheter intraoperatively has been recently reported to have a lower risk of stenosis (6%) compared with a stoma size of less than 8 Fr (44%). 9 This highlights the importance of adequately exposing the pelvic urethra to optimise stoma size. However, the literature offers limited details regarding the specific dissection steps needed to achieve this exposure, particularly the ventral dissection between the urethra and the pubis. Existing studies that do mention this step provide little to no objective measurement of its value.17 –19 In our study, after transecting the dorsal connective tissue and retractor penile muscle, the BUGs in all the cadavers were located either at or below the level of the ischium. These findings suggest that, with thorough soft tissue dissection, particularly ventrally, the BUGs should routinely lie at or below the level of the ischium. This is consistent with the descriptions of PU technique by Wilson and Harrison. 12 This finding may help to reduce the need for excessive caudal traction on the urethra to achieve apposition when dissection is inadequate, which can increase tension at the mucocutaneous junction.
Periurethral dissection must be performed with careful attention to the regional neurovascular structures, namely the pelvic neural plexus, pudendal nerve and urethral vasculature.20,21 Dorsal dissection, in particular, carries a risk of neurovascular trauma due to the proximity of these structures.20,22,23 In this study, dorsal dissection beyond the level of the BUGs resulted in an additional 10.7% increase in caudal urethral translation. Although this increase is substantial and may be necessary in select cases to achieve a tension-free stoma, it must be balanced against the increased risk of iatrogenic injury. Conversely, ventral intrapelvic dissection has been shown to be safe. In a case series by Sackman et al, 22 dissection to the level of the pubic brim had no effect on urinary incontinence or urodynamic functions. As noted by Fletcher, 20 this may be due to the relative absence of critical neurovascular structures in this region. Therefore, ventral dissection offers a safe and often sufficient approach for achieving the necessary urethral translation. However, when additional mobilisation is required, dorsal dissection can offer a meaningful increase in caudal translation. In such cases, the added translation achieved through dorsal dissection may be essential for creating a stoma under minimal tension, thereby reducing the risk of postoperative complications.
This study has several limitations. First, the cadavers were thawed from frozen, which may not fully reflect the biomechanical properties of fresh tissue in clinical cases. Therefore, future research to verify the findings in fresh cadavers should be performed before drawing definitive conclusions. Second, PU was performed in sternal recumbency without a urethral catheter in place and in a specific procedural sequence based on the authors’ preferences. Future research replicating the dissection in dorsal recumbency, as recently described by Watson et al, 24 would be valuable. In addition, ventral blunt dissection was guided by intraoperative judgement and tactile feedback, limiting the reproducibility of this step. Variability in periurethral tissue composition between castrated and intact males may also have influenced outcomes. The empirically derived traction force of 2 N and the weight of the Allis tissue forceps may have led to stretching of the urethral tissue and affected our measurements; however, the method was standardised in all cases and we consider the impact to be negligible. Finally, the medical history of the cadavers, including any lower urinary tract disease, was unknown and could have affected tissue characteristics, dissection dynamics and measurements.
Conclusions
This feline cadaveric experimental study demonstrated that each stage of dissection performed during PU contributed to caudal translation of the penile and pelvic urethra. The greatest length of caudal translation was achieved after ventral dissection of the fibrous attachments between the urethra and the pelvis. The findings of this study are relevant to veterinary surgeons performing PU, as they offer objective guidance for optimising surgical technique with the aim of reducing stoma tension and minimising the risk of postoperative stenosis.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.