
Abstract
Clinical challenges:
Epileptic seizures are a relatively common neurological presentation in cats, yet determining the underlying cause can be challenging due to the broad range of differential diagnoses.
Diagnostic approach:
A systematic approach, including thorough history-taking, physical and neurological examination, and appropriate diagnostic testing, is critical to accurately identifying the underlying cause and guiding effective management strategies.
Audience:
This review is aimed at veterinarians who manage feline patients presenting with epileptic seizures and outlines their features and differentials, as well as a guide to diagnosis.

Introduction
Epileptic seizures are the ‘clinical manifestations of excessive or hyper-synchronous abnormal electrical brain activity’.1–3 Recurrent seizures are termed epilepsy, and epileptic seizures always localise to the fore-brain. 4 Reactive seizures are those caused by an extracranial cause, such as a toxin exposure or metabolic disease. 1 Structural epilepsy is when epileptic seizures are caused by intracranial disease, such as vascular, inflammatory, infectious, traumatic, anomalous, neoplastic or degenerative diseases. 1 A summary of the differential diagnoses for seizures in cats is given in Table 1.
Summary of differential diagnoses for seizures in cats

Signalment
A cat’s age and breed may influence the differential diagnosis. Anomalous and metabolic causes, as well as genetic diseases, should be considered in juvenile patients. Several different brain malformations have been reported in cats, including hydrocephalus, porencephaly and lissencephaly.5–11 In a study of adult cats, onset of epileptic seizures over the age of 7 years old was found to increase the odds of a diagnosis of structural epilepsy. 12 In the same study, pedigree cats were found more likely to be diagnosed with a structural underlying cause for their seizures. 12
History
A detailed history is essential in understanding the nature of a cat’s abnormal episodes and can help determine if they are epileptic seizures or other types of episodes, such as syncope, vestibular disease or paroxysmal dyskinesia (see ‘Distinguishing epileptic seizures and other types of episodes’ box). Videos are invaluable and always recommended.
A detailed description of the episode is not only helpful in understanding if it is an epileptic seizure but can also assist in determining the differential diagnosis. One study found that cats with salivation during an epileptic seizure were more likely to be diagnosed with idiopathic epilepsy, while cats vocalising during an epileptic seizure were more likely to be diagnosed with structural epilepsy. 12 Complex orofacial seizures (Video 7 in the supplementary material) are commonly seen in cats with limbic encephalitis, temporal lobe epilepsy and/or hippocampal necrosis.20–22 Cats with reactive seizures more commonly present with generalised seizures. 23
Similarly, other aspects of the patient’s history might support the need to perform further diagnostics to identify an underlying cause. Behavioural changes between seizures, such as altered interactions with people or other pets, increased or decreased vocalisation, reduced grooming, inappropriate toileting, head pressing or compulsive pacing/circling may suggest forebrain disease. A history suggestive of visual deficits may also be relevant. In some cases, signs consistent with hemineglect syndrome may be present, where the cat appears unaware of stimuli on one side of the body – for example, eating from only one side of the bowl.
Additional historical findings such as recent significant weight loss, gastrointestinal signs, inappetence or polyphagia, and polyuria/ polydipsia, may indicate systemic disease, including metabolic, infectious or neoplastic conditions. A known or suspected history of toxin ingestion should also be considered. Recent or previous head trauma may be relevant as post-traumatic epileptic seizures can develop. 24 In juvenile patients, abnormal behaviours and interactions, and an inability to follow age-appropriate training may be relevant. A thorough diet history should also be included, particularly as thiamine deficiency is a recognised cause of seizures. Thiamine deficiency may be associated with poorly processed or heat-treated diets, sulphite-preserved foods (such as certain pet meats) or diets containing thiaminase (eg, raw fish), all of which can interfere with thiamine availability or absorption. Finally, the patient’s vaccination status, travel history and lifestyle (eg, indoor/outdoor) should always be reviewed.
Physical and neurological examination
A thorough physical and neurological examination should be performed in every cat who presents with epileptic seizures. In parallel with the patient’s history, signs of systemic illness on physical examination may help to identify possible systemic or multifocal causes. Cats with seizures secondary to a metabolic cause will often also have systemic signs of this disease. Similarly, certain infectious and neoplastic causes can be multifocal rather than being limited to the forebrain. In addition, blood pressure measurement is recommended to rule out hypertension. Fundic examination can also be useful, offering insight into possible signs of an infectious (eg, uveitis, chorioretinitis) or degenerative disease (eg, retinal atrophy) or retinal haemorrhage secondary to hypertension.25–27

The neurological examination should evaluate the mental status, behaviour, posture, gait, proprioception, spinal reflexes and cranial nerves, as well as the presence of any neck or back pain. Abnormal findings on the neurological examination that are not consistent with forebrain disease alone would be indicative of a multifocal central nervous system disorder and therefore further investigations would be recommended. Furthermore, abnormal neurological examinations during the interictal period have been associated with structural epilepsy in cats. 12 However, transient changes can occur in the postictal period, so examination should be repeated when the postictal phase has resolved, if possible. Postictal changes may include ataxia, visual or hearing deficits, polydipsia, polyphagia and behavioural changes such as aggression.3,28 The physical and neurological examination is also crucial to determine if there are signs of increased intracranial pressure that may require immediate treatment, such as bradycardia, hypertension, irregular breathing and loss of physiological nystagmus. 29
Metabolic screening
Haematology and serum biochemistry should be performed to investigate for metabolic causes of seizures such as hepatic or renal encephalopathy, hypertriglyceridaemia, polycythaemia vera or severe anaemia.23,30 Pre- and postprandial serum bile acid testing can support the diagnosis of a portosystemic shunt or other forms of hepatic impairment. Ammonia testing is also recommended, especially if hepatic disease is suspected, but transient postictal increases in ammonia concentrations have been described in epileptic cats without liver disease. In such cases, a repeat measurement 3 days post-seizure may be informative. 31 Thyroid hormone testing should be performed to rule out hyperthyroidism. Electrolytes should also be evaluated to rule out abnormalities that can cause seizures, such as hypoglycaemia, hyperglycaemia, hypocalcaemia, hypomagnesaemia, hyponatraemia, hypernatraemia and hypokalaemia. 4 Thiamine deficiency can cause seizures in cats, among other signs. 32 Investigation of serum vitamin B12 levels might be recommended in some cases to rule out hypocobalaminaemia. Urine metabolic screening may help detect some lysosomal diseases or inborn errors of metabolism, particularly methylmalonic aciduria, which has been reported in cats; this should be reserved for cases with a high index of suspicion, however. 33 The most common cause of reactive seizures in cats is intoxication, presumed or confirmed, and blood tests may remain unremarkable. 23
Advanced imaging
Once reactive seizures have been ruled out, advanced imaging can be considered to investigate for possible intracranial causes of epileptic seizures (Figures 1–3). CT may be more accessible, can be performed under sedation and is effective for detecting certain types of neoplasia. CT is also useful in trauma cases for identifying skull fractures and acute haemorrhage; however, in general the definition of the brain on CT is poor. MRI typically is more costly, requires a general anaesthetic and is more time-consuming, but offers much better soft tissue resolution, providing excellent definition of the brain and meninges; furthermore, in addition to structural causes, it can also identify changes consistent with metabolic and neurodegenerative diseases.32,34 MRI is therefore the imaging modality of choice for most epileptic cats.
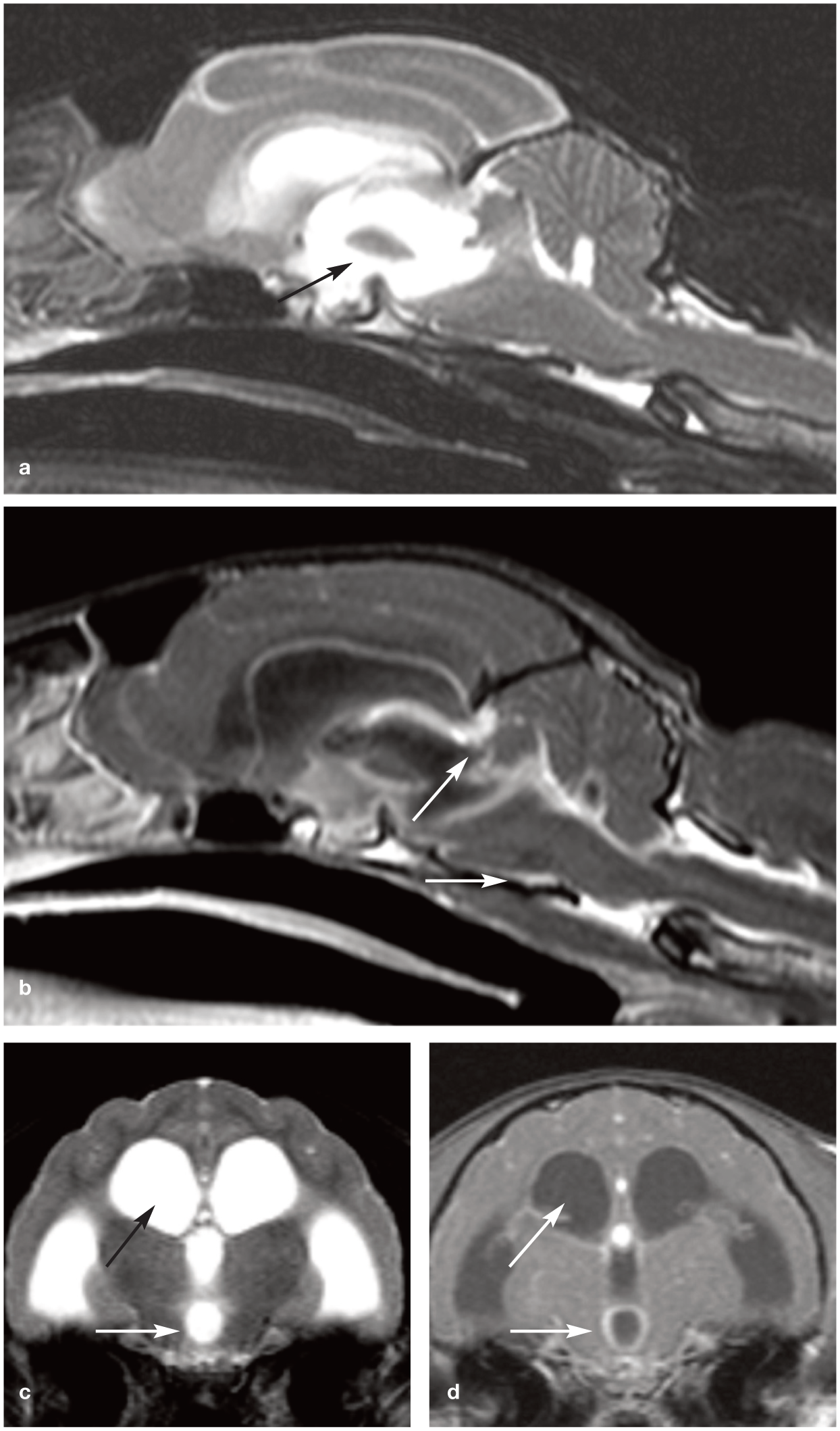
MRI of a cat diagnosed with central nervous system feline infectious peritonitis (FIP). T2-weighted midline (a) sagittal and (c) transverse images demonstrate marked dilation of the third and lateral ventricles, consistent with obstructive hydrocephalus (black arrow). Post-contrast T1-weighted (b) sagittal and (d) transverse images show contrast enhancement surrounding the third and lateral ventricles (white arrows) following intravenous gadolinium administration. These findings are indicative of pyogranulomatous meningoencephalitis associated with FIP. The cat exhibited intermittent central vestibular signs and seizures, likely secondary to increased intracranial pressure. FIP should be considered in particular in cats <2 years or >9 years of age presenting with compatible neurological signs

CT imaging of a 12-year-old spayed female cat diagnosed with an intracranial meningioma. (a) Pre-contrast transverse image reveals marked calvarial hyperostosis (white arrows). Post-contrast (b) transverse, (c) dorsal and (d) sagittal images following intravenous administration of iohexol demonstrate heterogeneous contrast enhancement of the intracranial mass (black asterisk). Surgical resection of the tumour was successful, with the cat surviving for 4.5 years postoperatively

MRI of a 9-year-old cat diagnosed with an intracranial meningioma. (a) Sagittal T2-weighted image reveals brain swelling with caudal transtentorial herniation of the cerebellum (white arrow) and hyperintensity of the cervical spinal cord suggestive of increased intracranial pressure. (b) Dorsal T2-weighted image shows the intracranial mass with a hypointense centre (white arrow) and (c) transverse T1-weighted postcontrast image reveals homogeneous contrast enhancement following gadolinium administration. While MRI offers excellent soft tissue resolution, it is less sensitive than CT for detecting osseous changes such as calvarial hyperostosis
Cerebrospinal fluid analysis
Depending on the findings on advanced imaging, cerebrospinal fluid (CSF) sampling may be indicated. This can be particularly helpful in inflammatory or infectious diseases, although some neoplastic processes (eg, lymphoma) can also be detected from CSF. CSF analysis can help determine whether inflammation is present; however, results are often non-specific for the underlying disease process. On occasion, infectious organisms (eg, Cryptococcus species) or neoplastic cells may be visualised, although the latter is uncommon even in cases of central nervous system lymphoma. For cats presenting with epileptic seizures, collection of CSF from the cerebellomedullary cistern (cisterna magna) is typically preferred. In one study, only 4.6% of cats with normal brain or only hippocampal changes on MRI had abnormal CSF findings. 35 Contraindications of CSF sampling include signs of raised intracranial pressure, skin infection, coagulopathy and cervical vertebral instability. 36 It is important to note that CSF collection carries inherent risks, including the potential for inadvertent damage to neural structures; therefore, the decision to pursue sampling should always be made after carefully weighing the risks against the expected diagnostic benefit.

Normal CSF is clear, colourless and largely acellular with fewer than five nucleated cells/μl considered within normal limits. Protein concentration should be below 27 mg/dl in a cisternal sample. 37 Increased turbidity may indicate a highly cellular sample; xanthochromia can reflect previous haemorrhage and red discolouration is often attributable to iatrogenic blood contamin-ation. 36 Albuminocytological dissociation, characterised by increased protein concentration without an increase in nucleated cells, is a non-specific finding that can be seen in many conditions, including inflammatory, vascular, neoplastic and degenerative processes. Increased nucleated cell counts and cytological evaluation can be very useful, particularly in the diagnosis of inflammatory or infectious diseases. 36 Ideally, CSF must be analysed shortly after collection, and so for externally analysed samples it is recommended to contact the laboratory to discuss their preferred collection tubes and fixation method.
Infectious disease testing
Infectious disease testing such as bacterial culture or PCR – for example, for feline infectious peritonitis (FIP) or Toxoplasma gondii – can be performed on CSF (non-invasive testing for T gondii can also be performed through serology). Fungal testing, such as for Crypto -coccus gattii or Blastomyces dermatitidis, may be relevant depending on the geographical location and travel history. Aberrant parasitic migration, particularly of Cuterebra species, although it can also occur with heartworm (Dirofilaria immitis), can result in neurological signs including epileptic seizures.38,39 Although feline immunodeficiency virus (FIV) and feline leukaemia virus (FeLV) can affect the brain and have been commonly listed as
possible causes of epileptic seizures in cats, there are no published reports supporting this. However, both FIV and FeLV can compromise the immune system, thus increasing the risk of clinically relevant infections, and they appear to be associated with the development of lymphoma, which can affect the central nervous system.40–55 Therefore, checking the FeLV/FIV status of the patient is also recommended. Finally, urine analysis and culture and sensitivity may be useful as there may be an association between bacteriuria and encephalopathy in cats, with epileptic seizures also reported in these cases. 56
Genetic testing
Genetic tests are available for lysosomal storage diseases that may cause epileptic seizures in cats, such as glycogenosis and gangliosidosis.57,58
Key Points
✜ Collecting a detailed medical history is essential for understanding the nature of seizures and seizure-like episodes.
✜ A thorough physical and neurological examination should be performed in every cat who presents with epileptic seizures. As transient changes can occur in the postictal period, neurological examination should be repeated, if possible, when the postictal phase has resolved.
✜ El Metabolic screening should be performed to start with to investigate for extracranial causes.
✜ El Advanced imaging, such as CT or MRI, should be performed to investigate for possible intracranial causes once reactive seizures have been ruled out.
✜ Infectious disease testing and CSF analysis can also help to determine the underlying pathology.
✜ El Genetic testing for lysosomal storage diseases may be useful in juvenile patients of certain breeds.
✜ Epilepsy of unknown origin (‘idiopathic epilepsy’) is a common cause of epileptic seizures in cats and is diagnosed by the exclusion of other diseases.
Footnotes
Supplementary material
Video 1: Simple focal seizures in a cat.
Video 2: Complex focal seizures in a cat.
Video 3: Generalised tonic-clonic seizure in a cat.
Video 4: Myoclonic seizures in a cat.
Video 5: Absence seizure in a cat.
Video 6: Feline audiogenic reflex seizures.
Video 7: Complex orofacial seizure in a cat.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author of this commissioned Clinical Spotlight review received an honorarium; as for all JFMS articles, this Clinical Spotlight article went through peer review.
Ethical approval
This work did not involve the use of animals and therefore ethical approval was not specifically required for publication in JFMS.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. For any animals or people identifiable within this publication, additional informed consent for publication was obtained.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.