
Abstract
Objectives
Cerebrospinal fluid (CSF) analysis is used in the diagnostic investigation of cats with epileptic seizures. The aim of this retrospective study was to evaluate the diagnostic value of CSF analysis in cats with epileptic seizures that have unremarkable brain MRI or only hippocampal signal changes.
Methods
Unremarkable brain MRI or MRI studies with signal alterations in the hippocampus only in cats with suspected epilepsy and CFS analysis performed at the Small Animal Internal Department or Diagnostic Imaging Department at Vetmeduni Vienna, Austria, between 2011 and 2017 were reviewed. Total nucleated cell count, total protein, blood contamination and cytology data from CSF analysis were evaluated.
Results
In total, 87 cats were included. Seventy cats (80.5%) had unremarkable MRI, five (5.7%) had hippocampal signal changes with contrast enhancement and 12 (13.8%) had hippocampal signal changes without contrast enhancement. Overall, four cats (4.6%) had abnormalities on CSF analysis; all (100%) had an increased total nucleated cell count (22 cells/μl, 7 cells/μl, 6 cells/μl and 6 cells/μl, respectively), and no cat had increased total protein (100%), although in one cat total protein was not evaluated. Three of these cats had unremarkable MRI and one had hippocampal signal changes without contrast enhancement. The median duration of epileptic signs prior to the MRI study was 2 days.
Conclusions and relevance
Our results show that, in our cohort of epileptic cats with unremarkable brain MRI or with hippocampal signal changes, CSF analysis was usually normal. This should be considered before performing a CSF tap.
Introduction
Seizures are a common neurological manifestation in cats, with an estimated 1-year prevalence of 0.2% in primary care veterinary practices in the UK and 3.5% in a referral hospital population in Austria.1,2 MRI and cerebrospinal fluid (CSF) analysis are often used in the diagnostic approach for cats with epileptic seizures.
Previous studies in dogs have shown that performing CSF analysis in those with suspected idiopathic epilepsy and unremarkable MRI rarely reveals significant abnormalities.3,4
To our knowledge, there has been no similar study evaluating the diagnostic value of CSF analysis in epileptic cats with unremarkable brain MRI.
This retrospective study aimed to identify how often epileptic cats with unremarkable MRI scans or just hippocampal signal changes have abnormalities on CSF analysis.
Materials and methods
Patients
Brain MRI and CSF data of feline epilepsy patients presented to the Small Animal Internal Department or the Diagnostic Imaging Department at Vetmeduni Vienna, Austria, between June 2011 and December 2017 were reviewed. The following inclusion criteria were used for patient database research and all were mandatory for study selection: brain MRI was performed because of a history of recurrent seizures; MRI of the brain was unremarkable or only hippocampal signal changes were detected; and CSF analysis was performed.
Recorded basic patient information included age, sex, neuter status, CSF total nucleated cell count (TNCC), CSF red blood cell (RBC) count, CSF total protein (TP), CSF cytology (if performed) and the result of the histopathological examination (if available). Based on the clients’ descriptions of seizures and presentations, the cats were classified as having focal epileptic seizures only, focal and secondary generalised seizures, generalised seizures only or an unknown type of seizure. Orofacial seizures are focal seizures and were not specifically evaluated.
Every cat in the study had minimal basic blood analysis, including haematology and biochemistry with glucose, creatinine, urea, TP, albumin, alkaline phosphatase, alanine aminotransferase and electrolytes. In most of the cases, aspartate aminotransferase, glutamate dehydrogenase, creatine kinase, cholinesterase and bile acid were also measured. These data were not specifically collected or evaluated.
MRI scan interpretation
MRI was performed with a 1.5 Tesla MRI scanner (Siemens Magnetom Espree; Siemens Healthcare) with the cats in ventral recumbency under general anaesthesia (premedication: butorphanol 0.2 mg/kg, midazolam 0.2 mg/kg and alfaxalone 1 mg/kg; induction: propofol or alfaxalone; maintenance: inhalation anaesthesia with sevoflurane; infusion: isotonic whole electrolyte solution 5 ml/kg/h).
The MRI protocol used initially included three sequences (sagittal T1-weighted [T1W] in three dimensions, transverse T2-weighted [TW2] and a transverse T2W fluid attenuated inversion recovery [FLAIR]), which were completed during the study following the MRI protocol provided in Table 1.
MRI parameters

TE = time of echo; TR = time of repetition; FoV = field of view; T1W = T1-weighted; 3D = three-dimensional; SE = spin echo; T2W = T2-weighted; FLAIR = fluid-attenuated inversion recovery; GRE = gradient echo; DWI = diffusion-weighted imaging; ADC = apparent diffusion coefficient
Slice thickness varied only slightly with body weight (2–3 mm).
For the contrast series (T1W transverse and three-dimensional sagittal), 86/87 cats received contrast agent (gadolinium/gadoteric acid 0.2 ml/kg [Dotarem 10 ml solution for injection, 279.32 mg/ml; Guerbet]).
The MRI criterion for hippocampal changes was the subjective T2 and FLAIR hyperintensity elevations of the hippocampi compared with the grey matter of the adjacent temporal lobe or pathological contrast uptake of the hippocampi. Included MRI studies were initially evaluated by several radiologists in the department and re-evaluated by a second-year radiology resident (BAL) according to the following criteria: subjective evaluation of the hippocampi (T2 and FLAIR signal alterations, volume changes, contrast enhancement relying on post-contrast T1W MRI and the subtraction images) and detection of other brain lesions besides hippocampal changes (no other changes were evident).
CSF analysis
CSF was collected from the cerebellomedullary cistern following MRI study under the same anaesthesia. Samples were collected in a plain tube and examined immediately at the Central Laboratory of the Vetmeduni Vienna or by a board-certified neurologist/senior neurologist at the clinic. Both neurologists used the same CSF analysis technique.
TNCC was evaluated with a Fuchs–Rosenthal counting chamber using Samson solution. A CSF cytological cytospin evaluation was performed if the TNCC showed 5 cells/μl. TP was measured using a Cobas c 501 analyser (Roche Diagnostics) with the Biurett calorimetric method. RBC count was evaluated using a Combur-9 Test HC strip (Roche Diagnostics), with the following possible results: –, + (~5–10/µl), ++ (~25/µl), +++ (~50/µl) and ++++ (~250/µl).
Pleocytosis was defined using our laboratory’s reference intervals (RIs): TNCC >5 cells/µl and TP >480 mg/l without severe blood contamination (RBC values of ~50/µl, ie, +++ and above). Cats with increased TNCC and severe blood contamination were excluded from the study due to the inability to objectively evaluate the elevated cell count.
Statistical analysis
Data were recorded in a Microsoft Excel spreadsheet. The descriptive statistical analysis was performed by the first author. Descriptive statistics included measures of frequency (count and percentage), measures of central tendency (mean) and measures of dispersion (interquartile range [IQR]).
Results
Ninety cats met the initial inclusion criteria. Three cats with increased TNCC and severe blood contamination were excluded from the study. A total of 87 cats were included in the final study cohort. Seventy cats (80.5%) had unremarkable MRI, five (5.7%) had hippocampal signal changes with contrast enhancement and 12 (13.8%) had hippocampal signal changes without contrast enhancement.
Forty-seven of the cats were female (54%), 41 of which were neutered and six entire. Forty cats were male (46%), 37 of which were neutered and three entire.
Age at presentation to the clinic ranged from 3 to 161 months (median 50). Exact age at presentation was unavailable in three cats.
Twenty-four cats (27.6%) were presented with focal seizures only, 17 cats (19.5%) had a history of focal and secondary generalised seizures, 43 cats (49.4%) had generalised seizures only and in three cats (3.4%) the type of seizure was unknown.
CSF analysis was performed at the central laboratory in 77 cases, while 10 cats were evaluated at the clinic. Median TNCC was 0.6 cells/µl (IQR 0.3–1.6). Median TP concentration was 109 mg/l (IQR 82–136). Six cats were excluded from the statistical analysis of TP because there was not enough material for testing in four cats or due to negative results using a Combur-9 Test HC strip (Roche Diagnostics) at the clinic in two.
The CSF was contaminated with blood in 65 cases (74.7%). From these samples, 25 were contaminated (+ [38.5%]; 15 ++ [23.1%]; 16 +++ [24.6%]; nine ++++ [13.8%]). Data on blood contamination were unavailable for four cats.
TNCC was increased in four cats (4.6%); of these, three had only a borderline increase in TNCC (7 cells/µl, 6 cells/µl and 6 cells/µl, respectively) and one had mildly increased TNCC (22 cells/µl). The four cats with mild pleocytosis were not tested for leucine-rich glioma-inactivated 1 (LGI1) antibodies. 5 TP was within the RI for all cats evaluated for TP. In four cats, the TP evaluation was not available. All cats with pleocytosis (if available) had an epileptic seizure within the 72 h before CSF collection. More information on cats with CSF changes is provided in Table 2.
Signalment, seizure type, time between the last seizure and MRI, MRI findings, cerebrospinal fluid (CSF) cytology, histopathological findings, other diseases and diagnostic screening before MRI in the four cats with abnormalities on CSF analysis
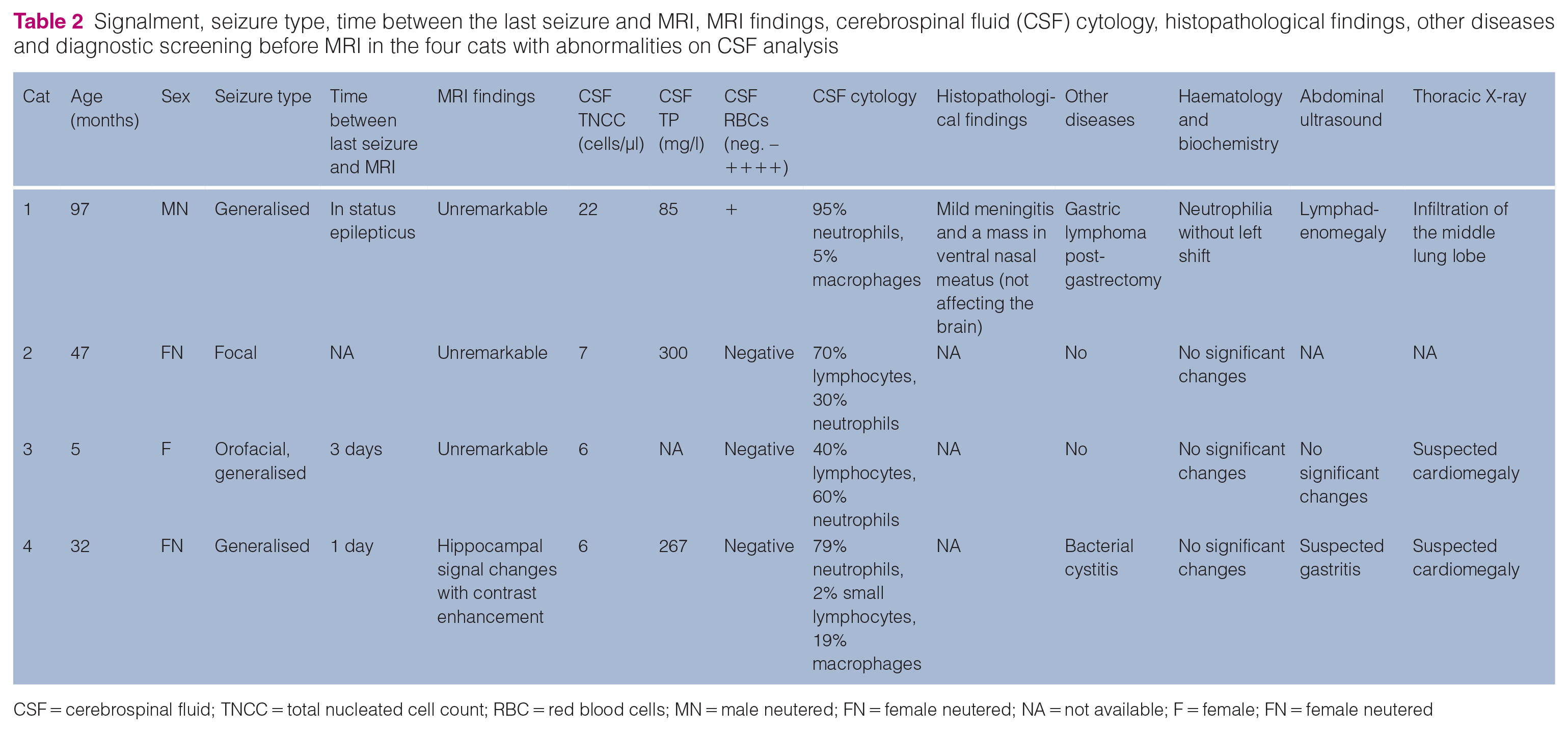
CSF = cerebrospinal fluid; TNCC = total nucleated cell count; RBC = red blood cells; MN = male neutered; FN = female neutered; NA = not available; F = female; FN = female neutered
Histopathology was performed on 11 cats. Of cats with CSF pleocytosis, only one underwent a necropsy and was diagnosed with meningitis of unknown origin. Of the remaining cats with no CSF changes, hippocampal necrosis was confirmed in two cases, as well as hippocampal sclerosis in two cases. Other diagnoses included another meningitis of unknown origin, lysosomal storage disease, encephalitis and non-suppurative leptomeningitis. There were no changes in the brains of two cats. Ten of 11 cats had unremarkable MRI, and one cat had hippocampal signal changes with contrast enhancement (one with confirmed hippocampal necrosis).
Discussion
We aimed to investigate whether it is of value to perform CSF analysis in cats that do not have structural brain changes on MRI.
CSF taps are associated with risks, including iatrogenic brainstem injury and subarachnoid haemorrhage; the requirement of experienced personnel, prolonged anaesthesia duration and increased costs could also be considered in the diagnostic approach.6–9
Performing CSF analysis in humans is not recommended in epilepsy investigations unless signalment (infants aged <6 months) or history and clinical signs are suggestive of infectious causes. 10 Currently, CSF analysis in dogs is required as a part of the tier II criteria for diagnosing idiopathic epilepsy by the International Veterinary Epilepsy Task Force with the goal of excluding inflammatory disease and/or infections. 11 As yet, there is no consensus on the diagnostic approach for epilepsy in cats.
In favour of the fact that a CSF tap can be helpful in patients with a normal MRI, it has been reported that 7% of dogs with a normal MRI had meningoencephalitis of unknown origin. 12 Also, in a study that evaluated the MRI findings in 14 cats with meningoencephalitis, four (29%) did not show MRI changes. The remaining cats were diagnosed with feline infectious peritonitis (n = 3) and histiocytic encephalitis (n = 1). 13 Similarly, in a study that evaluated the MRI features of lymphoma involving the nervous system in cats, intracranial MRI lesions were present in 22/31 cats (71%). In this study, CSF analysis was abnormal in 20/25 cats (80%), although the CSF cytology was in the diagnostic range for lymphoma in only five cats. 14 It is worth mentioning that MRI is not 100% sensitive or specific, although a sensitivity of up to 94.4% and a specificity of up to 95.5% for detecting brain abnormalities in dogs have been reported. 15 It seems likely that these numbers in cats are lower due to their smaller brain size. 16
Only a few systemic studies have evaluated CSF in dogs with unremarkable MRI findings, and, to our knowledge, no studies have evaluated the same in cats. In a previous study, mild abnormalities on CSF analysis were identified in 10.6% of dogs with suspected idiopathic epilepsy and a normal MRI. 4 These results are also in agreement with another study, where only negligible abnormalities on CSF were found in 15% of dogs with suspected idiopathic epilepsy and a normal MRI. 3 The findings did not lead to a change in the diagnosis or management of these cases.
MRI signal changes in the hippocampal region of cats are frequently consistent with hippocampal necrosis on histopathology. They may also be caused by other pathologies, including hippocampal sclerosis, oedema, inflammation, ischaemia or a combination of these.17–22 Moreover, epileptic seizures may cause an altered MRI signal postictally, but documented feline cases are rare.23,24 In cats with postictal MRI changes, CSF analysis results are expected to be unremarkable or show only very mild postictal pleocytosis. 25
Cats with solely hippocampal MRI signal changes are an important proportion of feline epileptic patients, but this is also a problematic group. This originates from the ‘cause-or-consequence’ problem, as the seizure itself may cause a hippocampal pathology. The International League Against Epilepsy has not determined whether hippocampal sclerosis is a non-specific result of primary epileptogenic lesions or if it is coexistent. 26 The issue is controversial and both possibilities are likely to be partially true. Therefore, we decided to include this group, as such cats with seizures do not have clear structural aetiological changes in the brain. These cats may be included in the group of idiopathic epilepsy with suspected postictal changes. However, the absence of neurological signs postictally is an important requirement for this diagnosis. Some authors prefer to use ‘epilepsy of unknown origin’ instead of ‘idiopathic epilepsy’, as a genetic aetiology cannot be confirmed in cats and the use of this term is also more appropriate for this group.11,27,28
In our study, one histopathological examination was performed on a cat with hippocampal signal changes. The result confirmed hippocampal necrosis.
CSF pleocytosis was found in 4.6% of all cats. TNCC was only borderline increased in 3/4 cases with suspected idiopathic epilepsy as a final diagnosis. This corresponds with the SD of the normal distribution curve for RIs. Only one cat had mild pleocytosis (22 cells/μl), with a history of lymphoma; CNS involvement was suspected but not confirmed. The pathohistological examination of this cat revealed meningitis of unknown origin.
All cats (if available) with abnormal CSF results had an epileptic seizure within 72 h before CSF collection. Postictal pleocytosis has been reported in human medicine with a prevalence rate of 6–34% in patients with epileptic seizures without evidence of infectious or inflammatory causes.29–31 One suggested mechanism for an increase in TNCC on CSF analysis, associated with recent seizure activity, is a transient disruption to the blood–brain barrier. 32 Studies on dogs have provided various results. One study reported an association between the CSF TNCC and seizures, with the TNCC tending to decrease with increasing length of time between the last epileptic seizure and CSF collection. 33 However, this association was not found in all studies.3,4 Although no correlation analysis between CSF changes and the time of last seizure was found in our study, it is a logical assumption that mild postictal pleocytosis also exists in cats.
A high percentage of our samples showed some degree of blood contamination. We cannot compare this with previous studies, because the percentage of contaminated samples was not mentioned in these other studies. CSF contamination is most commonly iatrogenic, and the literature is conflicting about the impact of blood on the CSF analysis.34–36 The correction formulas to help estimate these effects on CSF cellularity have also been published, with inconsistent agreement.3,36,37 We decided to exclude cats with severe blood contamination and CSF pleocytosis from the study, to avoid misinterpretation of the results.
The limitations of this study include the fact that the diagnosis of idiopathic epilepsy could not be confirmed and subclinical disease-causing epileptic seizures could not be excluded. Because of its retrospective character, data on prior treatment, and pre- and interictal clinical and neurological examination were mostly unavailable. Excluding such cases would considerably reduce the number of included cats. We also did not evaluate the laboratory results or results of other diagnostic imaging, and we did not include follow-up and outcome data in all cases. Histopathology was only available in 11 cats. In these cases, considerable time had passed between MRI and histopathology, which makes a firm conclusion difficult.
Conclusions
In a cohort of cats with a history of seizures and unremarkable MRI or hippocampal signal changes only, CSF changes are rare, and the sporadic borderline pleocytosis does not change the diagnosis or management of these patients. However, CSF analysis is generally an important diagnostic test for CNS disorders, so the diagnostic benefit and risks should always be considered in individual cases.
Footnotes
Author note
The abstract was presented at the ECVIM Congress 2022.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.