
Abstract
Objectives
The Danish Veterinary Cancer Registry (DVCR) was founded at the University of Copenhagen (then the Royal Veterinary and Agricultural University) in 2005 and has collected data from feline neoplastic cases ever since. To date, only canine data have been published. The objective of the current publication was to describe the distribution of neoplasms in Danish cats based on data from the DVCR.
Methods
Feline DVCR data (2005–2023) were extracted in December 2023. Study parameters were age, sex, breed, tumour type, tumour biological behaviour, anatomical location and method for obtaining the diagnosis. Standard morbidity ratios (SMRs) were calculated using breed data from the Danish Cat Registry as the denominator.
Results
A total of 767 neoplasms were registered. More neoplasms were malignant (561, 73.1%) than benign (175, 22.8%). More neoplasms were registered in female cats (423, 55.8%) than in male cats (335, 44.2%). The mean (±SD) cat age was 10.4 ± 3.8 years. Malignant epithelial tumours were the most common type (259, 33.8%), followed by malignant lymphoma (141, 18.4%), benign epithelial (120, 15.6%) and soft tissue sarcomas (79, 10.3%). The most common anatomical location was skin including adnexal tissue (213, 27.8%), followed by haemolymphatic tissue (152, 19.8%) and mammary tissue (151, 19.7%). Domestic/European shorthair cats had SMRs less than 1.0, while all purebred cats with more than 15 registrations had SMRs greater than 2.0. The relative risk for having a mammary tumour was 2.08 for intact vs spayed female cats.
Conclusions and relevance
It was shown that Danish cats mainly get malignant tumours, and that skin and epithelial tumours were the most common. Overall, the results from the DVCR fit well with data from other recent European publications and will be helpful for informing owners and veterinarians about the occurrence of feline cancer in Denmark and comparable countries.
Plain language summary
This article investigates the demographics, such as age, breed and sex, as well as the tumour types and body location of benign and malignant tumours in cats in Denmark. The data come from the Danish Veterinary Cancer Registry (DVCR), which was established in Denmark in 2005. The period for data extraction was May 2005 to December 2023. Data on breed popularity from the Danish Cat Registry was used to assess whether some cat breeds were at an increased risk of tumours compared with others. The DVCR consists of cases submitted voluntarily by Danish veterinarians via an online survey (www.vetcancer.ku.dk). A total of 767 benign or malignant tumours were registered in the period. Tumours were more often malignant (73.1%) than benign (22.8%). The average age of the cats was 10.4 years, and the cats were more often female (55.8%) than male (44.2%). Domestic shorthair cats had a lower risk of tumours compared with other breeds. The risk of having a mammary tumour was higher in female cats that were not spayed compared with those that were spayed. The tumours most commonly originated in the skin, followed by lymphatic tissue and the mammary glands. These three tumour locations are also the most commonly reported in other recent European publications.
Introduction
Veterinary cancer registries are powerful sources of information on neoplasms in companion animals. 1 Therefore, there is a large interest in both national and international cancer registries. Current data describing the occurrence of feline neoplasia originate largely from retrospective histopathology- or insurance-based databases, not from hospital or population-based sources. One potential bias associated with histopathology-based databases is that the data are selected for those tumours where histopathology is commonly used or where the owner elects for surgery because of a perceived good prognosis. Nevertheless, histopathology-based databases have the advantage of including ‘gold standard’-verified diagnoses as well as additional histological information such as subtype, grade and mitotic count. In addition, these databases are commonly extensive, allowing a strong basis for conclusions. Insurance databases have the inherent bias of selecting for insured cats, and often there is no specific diagnosis, no differentiation into benign/malignant behaviour and no information on how the diagnosis was verified, just categories such as ‘mammary tumour’, ‘skin tumour’ and so on.
The increasing interest in veterinary cancer surveillance and reporting is evidenced by the establishment of the Global Initiative for Veterinary Cancer Surveillance (GIVCS) (https://www.givcs.org), which was launched in 2018. The GIVCS is a global network of cancer registries with a stated goal of promoting international collaboration and fostering standardised methods for animal surveillance. The collaborative parties and registries are described in a letter published in Veterinary and Comparative Oncology in 2020. 2 Some of the included cancer registries are based on prospectively collected clinical information, while others are based on pathology databases, for example.
The Danish Veterinary Cancer Registry (DVCR) was established in May 2005 at the Royal Veterinary and Agricultural University, now the Faculty of Health and Medical Sciences, University of Copenhagen. It was inspired by the Danish national human cancer incidence registry and was designed with assistance from individuals involved in the human registry. The registry contains submissions of neoplasms from cats and dogs from veterinary clinics across Denmark, including both general practice and referral clinics. The correctness of the registry data has been validated in a study from 2009. 3 Registrations to the DVCR are made voluntarily by veterinarians in private and university veterinary clinics via an electronic internet-based form on the DVCR website (www.vetcancer.ku.dk). The DVCR is incidence based, and each neoplasm is registered separately. All histological subtypes of neoplasms can be reported, and diagnoses can be based on cytology, histopathology or other diagnostic modalities – for example, diagnostic imaging, flow cytometry or thyroid hormone profiles – or they can be ‘unconfirmed’. The registry data are described in more detail in a publication by Brønden et al. 4
The registry has previously supplied data about the occurrence and distribution of canine neoplasia;4 –6 however, to date, no feline data have been presented for publication. Accordingly, the objective of the current publication was to describe the distribution of neoplasms in Danish cats based on data from the DVCR focusing on patient signalment, including sex, breed distribution, tumour type, biological behaviour and anatomical location.
Materials and methods
The data were extracted from the DVCR, using all entries from 15 May 2005 to 19 December 2023. The study population represents any cat with a neoplasm presenting to a veterinary clinic in this period, where the attending clinician decided to register the neoplasm in the DVCR. Any information collected and registered in the DVCR follows the EU General Data Protection Regulation article 6, litra e. All veterinary clinics registering data in the DVCR have a poster in their reception area stating that they support cancer research by supplying data from their patients to the DVCR. Study parameters extracted were age, sex, breed, diagnosis, biological behaviour (benign vs malignant), anatomical location and method for obtaining the diagnosis. It is possible to register a cat both as a ‘domestic shorthair’ (DSH) and as a ‘European Shorthair’ (ESH). These were grouped together for the breed analyses.
There are 212 possible diagnoses available to choose from when registering the neoplasm, such as ‘adenocarcinoma’, ‘meningioma’ and ‘histiocytoma’, and 174 possible anatomical locations, such as ‘respiratory organs – lungs’, ‘gastrointestinal system – liver’ and so on. For this publication, diagnoses were placed into larger categories, such as ‘carcinomas’, which included all types of malignant epithelial tumours independent of subtype, and ‘soft tissue sarcomas’. Similarly, the anatomical locations were grouped into categories, including ‘skin and adnexal tissue’, ‘mammary tissue’, ‘digestive organs’ and ‘haemolymphatic tissue’. For cases of malignant lymphoma where the neoplasia was not registered anatomically in the ‘haemolymphatic system’, but instead in, for example, the gastrointestinal tract, nasal cavity, skin or kidneys, these were manually moved to the ‘haemolymphatic’ category.
For age-related analyses, the ages were divided into the following groups: less than 3 years, 3–5 years, 6–8 years, 9–11 years, 12–14 years and more than 14 years.
Cats registered in the Danish Cat Registry (DCR) (katteregister.dk) as of May 2015 served as the background population for breed statistics. The DCR is a voluntary registry of Danish client-owned cats that are either ear-tattooed or microchipped. Although it is not mandatory to register cats in Denmark, more than 650,000 cats were registered in 2015.
Statistical analyses
Data were handled in Microsoft Excel and statistical analyses were performed in GraphPad Prism version 10.1.1 (GraphPad Software). The data were manually checked for doublets, which were subsequently removed. The Mann–Whitney U-test was used to test differences in mean age between females and males and between patients with benign and malignant tumours. A two-tailed binomial test was used to test differences in the proportion of males vs females, the proportion of benign vs malignant tumours overall, and the proportion of benign vs malignant tumours for age groups and for anatomical locations. To estimate the effect of neuter status on the risk of having a mammary tumour in female cats, a relative risk (RR) including 95% confidence intervals (CIs) was calculated.
To assess the breed distribution compared to a reference population, standard morbidity ratios (SMRs) were calculated. Cats registered in the DCR were used as the reference population for the general cat population across Denmark. The SMR was calculated only for breeds with 15 or more registrations in the DVCR. The SMR for the breed was calculated as the observed number of cases divided by the expected number of cases. The 95% CIs were calculated as described in Brønden et al. 4
Results
A total of 767 neoplasms from 748 cats were registered during the study period. Of the cats, 729 had one neoplasm registered and 19 had two neoplasms. Significantly more malignant neoplasms (561, 73.1%) were registered compared with benign neoplasms (175, 22.8%) (P <0.001). For 31 (4.0%) neoplasms, the biological behaviour of the neoplasm was reported to be ‘unknown’. The neoplasms were diagnosed by histology in 302 (39.4%) cases, cytology in 329 (42.9%) cases, by ‘other methods’ in 72 (9.4%) cases and not verified in 64 (8.3%) cases. More neoplasms were registered in females (423, 55.1%) than in males (335, 43.7%) (P = 0.0016). Nine (1.2%) cases were registered as unknown sex. When excluding mammary tumours, significantly more neoplasms were registered in males (332, 54.5%) than in females (277, 45.5%) (P = 0.029). The sex, the tumour biological behaviour and the mean age for the neoplasms sorted by sex are shown in Table 1. The overall mean (±SD) age was 10.4 ± 3.8 years, with a mean cat age of 10.6 ± 3.7 years for malignant neoplasms and 9.8 ± 4.2 years for benign neoplasms. There was no significant difference between the mean cat ages for benign vs malignant neoplasms (P = 0.052). The distribution of neoplasms, including biological behaviour, for the various age groups is shown in Figure 1. For the age groups 6–8 years, 9–11 years, 12–14 years and over 14 years, significantly more neoplasms were malignant than benign (P <0.0001 for all groups).
Tumour biological behaviour and mean age for the various sex groups

Data are n (%) or mean ± SD

Age distribution and tumour biological behaviour. * Indicates age groups with significantly more malignant than benign neoplasms (P <0.0001). NR = not reported
The anatomical locations with at least 20 registrations are shown in Table 2. Skin including adnexal tissue (213, 27.8%) was the most commonly affected anatomical location, followed by haemolymphatic tissue (152, 19.8%) and mammary tissue (151, 19.7%). A total of 102 malignant lymphoma cases were recategorised from other anatomical locations to the haemolymphatic category. If these were kept in their original categories, the most common anatomical locations were skin including adnexal tissue (223, 29.1%), mammary tissue (151, 19.7%) and digestive organs (147, 19.2%), with haemolymphatic tissue representing only 50 (6.5%) cases.
Overview of affected body system for malignant and benign neoplasms with at least 20 total registrations
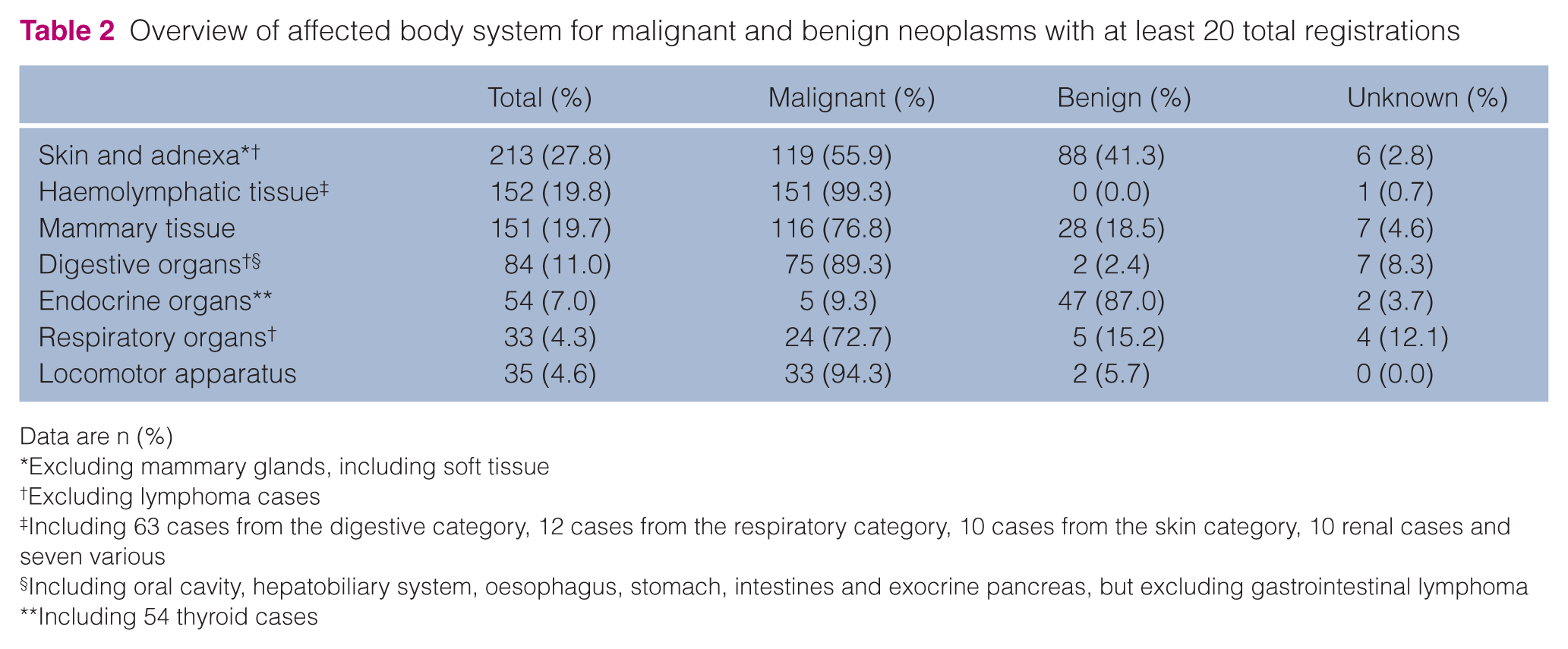
Data are n (%)
Excluding mammary glands, including soft tissue
Excluding lymphoma cases
Including 63 cases from the digestive category, 12 cases from the respiratory category, 10 cases from the skin category, 10 renal cases and seven various
Including oral cavity, hepatobiliary system, oesophagus, stomach, intestines and exocrine pancreas, but excluding gastrointestinal lymphoma
Including 54 thyroid cases
The RR of having a mammary tumour was 2.08 (95% CI 1.63–2.65) for intact vs spayed female cats. For intact females, 22.4% (n = 11) and 69.4% (n = 34) of mammary tumours were registered as benign and malignant, respectively. For spayed females, the equivalent percentages were 16.3% (n = 16) and 80.6% (n = 79), respectively. For all body systems listed in Table 2, there were significantly more malignant than benign neoplasms (P value 0.005 to <0.0001) except for endocrine organs, which had significantly more benign neoplasms (P <0.0001).
The distribution of neoplasms in the diagnostic categories with at least 20 registrations, as well as the diagnostic methods, are shown in Table 3. Epithelial neoplasms were the most common type for both malignant (259, 33.8%) and benign (120, 15.6%) registrations. A relatively large proportion of the benign epithelial registrations were thyroid adenomas (n = 47, 39.2%). The second and third most commonly registered malignant neoplasms were lymphoma (141, 18.4%) and soft tissue sarcomas (79, 10.3%).
Overview of registered diagnoses for neoplasms with at least 20 total registrations, including the diagnostic method used

Data are n (%). Included information is the total number of neoplasms per category as well as the number of neoplasms per diagnostic category where the diagnosis was made using histopathology, cytology, other methods or was not verified
Percentage of study total
Percentage of specific tumour type
MCT = mast cell tumour; OSA = osteosarcoma; STS = soft tissue sarcoma
The major skin tumour types (malignant and benign) were soft tissue sarcomas (47, 22.1%), benign epithelial tumours (46, 21.6%), mast cell tumours (41 in total [29 registered as malignant, 12 as benign], 19.2%) and carcinomas (36, 16.9%).
The haemolymphatic neoplasms were located in the digestive tract (63, 41.1%), haemolymphatic/lymph nodes (37, 24.3%), intrathoracic region including mediastinum (18, 11.8%), kidneys (10, 6.6%), skin (10, 6.6%), nasal region (7, 4.6%) and various/unknown (7, 4.6%).
The most common breeds were DSH/ESH (535, 69.8%), Maine Coon (53, 6.9%), Norwegian Forest Cat (41, 5.3%), Persian (29, 3.8%), Siamese (18, 2.3%), British Shorthair (15, 2.0%), Abyssinian (7, 0.9%), Burmese (7, 0.9%), Birman (7, 0.9%) and Somali cats (6, 0.8%). SMRs were calculated for breeds with more than 15 registrations in the DVCR. Data from these calculations are shown in Table 4. Notably, only the DSH/ESH had an SMR below 1.0, whereas all other breeds had SMRs >2.0 for both benign and malignant neoplasms.
Standard morbidity ratios for breeds with at least 15 total registrations and 10 malignant registrations

CI = confidence interval; DSH = domestic shorthair; ESH = European Shorthair; SMR = standard morbidity ratio
Discussion
When evaluating the literature describing the occurrence of feline cancer, it is relevant to divide it into those publications with data collected before the widespread introduction of testing and vaccination against feline leukaemia virus (FeLV) and those with data collected after this. The strong association between FeLV infection and the development of lymphoproliferative diseases7,8 means that early data may not be representative of the current situation. In 5/6 publications dating before 1990 with more than 50 included cases, the haemolymphatic system is stated as the most commonly affected system.9 –13 Only a South African publication from 1983 14 states the skin as being more commonly affected, which might be explained by the intense ultraviolet (UV) radiation cats are exposed to in this region. 15 This discrepancy between the early publications, all arising from North America, and the South African publication also illustrates how cancer occurrence will be affected by the geographical occurrence of risk factors, such as UV light and infectious diseases, as well as local neutering practices. Consequently, it is important to get global as well as regional information about cancer epidemiology.
In the current study with data collected from Danish cats between 2005 and 2023, skin was the most commonly affected location (27.8%), followed by an equal distribution of haemolymphatic (19.8%) and mammary (19.7%) tissue. The high proportion of cutaneous and subcutaneous tumours fits with updated European data from Portugal, 16 Croatia, 17 Italy18,19 and the UK. 20 The same publications also all place mammary gland in the top three tumour locations, which is interesting, as this is a tumour that almost exclusively occurs in female cats and has been shown to have a markedly decreased occurrence after early spaying. 21 The increased risk of mammary tumours in intact females is supported by our data, which showed a RR of 2.08 for this group. This finding aligns with a recent Italian publication reporting a higher rate of mammary tumours in intact female cats. 18
All data included in the current publication come from the post-FeLV-vaccination era, with data collection starting in 2005. Nevertheless, haemolymphatic tissue was the second most commonly occurring anatomical location together with mammary gland tissue, and lymphoma was the second most commonly occurring tumour type, surpassed only by malignant epithelial tumours. Interestingly, the 2021 UK publication by Rodríguez et al, 20 which included only recent cases, identified lymphoma as the most common diagnosis. Several other recent feline cancer publications also list lymphoma or round cell tumours among the three most common tumour types.16,17,19,22 FeLV has mainly been associated with the mediastinal and multicentric non-Hodgkin’s-like lymphoma types8,23 and is typically not implicated in lymphoma of other body sites. The digestive tract was the most commonly recorded anatomical site for lymphoma in the present study, aligning with recent reports that alimentary lymphoma is increasing in both relative frequency and overall prevalence.24,25 The FeLV status of cats in this study is unknown.
The demographics of the DVCR registrations were comparable to that previously described in similar publications. The mean age was 10.4 ± 3.8 years, which is equivalent to the mean age found by Pinello et al 26 (10.5 ± 3.4 years), and female cats were more common than male cats, which has also been shown by several other groups.18,19 In the present study, the difference between female and male cats was driven by mammary gland tumours, since male cats predominated if mammary tumours were excluded. Overall, 73.1% of tumours were registered as malignant. This is slightly lower than the proportion stated in similar publications with recent data, where the malignant proportion is commonly approximately 80% or higher.16 –19,27 This might be explained by the fact that cytology and other diagnostic methods are allowed when registering cases to the DVCR, which means that benign conditions are more likely to be included than in histopathology-based registries. For example, 47 cases of benign thyroid adenomas were included in the data set. Lastly, although DSH/ESH cats were the most commonly registered breed in the DVCR data set, the SMR calculations showed that they were actually underrepresented when accounting for overall breed popularity in Denmark. All purebred cats had an SMR above 2.0, with the highest value observed for Siamese cats. The relatively low SMR among DSH/ESH cats may reflect lower owner willingness to pursue veterinary evaluation or diagnostic procedures in non-purebred animals. Alternatively, purebred cats may truly have a greater disposition to neoplasia. The finding of the highest SMR in Siamese cats aligns with previous reports indicating an increased risk of neoplasia in this breed, supporting the results of the current study.24,28 –30
There are some limitations to the current data set. First, there are relatively few cases when compared with some of the pathology-based data sets, such as the SAVSNET publication 20 and the Swiss Feline Cancer Registry. 31 In comparison, the DVCR currently holds almost 9000 registrations from dogs from the same time period. This could suggest that cats in Denmark develop neoplasia less frequently, that veterinarians are less likely to register feline neoplastic cases or that cat owners are less inclined to pursue diagnostic investigation for suspected neoplasia. 32 It was recently discovered that only 24% of Danish cats vs 72% of dogs are insured, 33 which may also influence owner willingness to seek veterinary care. As another potential limitation, the DVCR diagnoses can be based on other diagnostic methods than histopathology and can even be ‘unconfirmed’. Only 39.4% of cases were diagnosed by histopathology. Although this can be viewed as a limitation, it may also be considered an advantage, as the data set is likely more complete when, for example, brain tumours diagnosed solely by MRI or lipomas diagnosed only by cytology can still be recorded. DVCR cases are not centrally registered but are submitted by various general practitioners across Denmark, which may introduce errors into the data set. Yet, the DVCR’s data quality was assessed in a 2009 validation study, 3 where information such as breed, tumour location and diagnosis were found to be accurate when compared with the original patient records. Only date-related data, such as birth dates and diagnosis dates, were not always accurate. Another concern with decentralised registration is the possibility that veterinarians may be more motivated to enter unusual or malignant cases than benign ones. Yet, the fact that the proportion of malignant cases in the current data set was actually lower than previously reported for cats, and that benign tumours are more common than malignant tumours in the canine DVCR data set, 4 suggests that Danish veterinarians register both benign and malignant tumours alike.
Conclusions
The present study using feline data from the DVCR found that females were more commonly affected by neoplasms than males, and that malignant neoplasms predominated. DSH/ESH cats had a lower reported tumour occurrence compared with purebred cats. The most frequently affected anatomical location was the skin, followed by haemolymphatic and mammary tissue. Carcinomas were the most common tumour type, followed by malignant lymphomas, benign epithelial tumours and soft tissue sarcomas.
Footnotes
Acknowledgements
The authors are grateful to the Danish Cat Registry for providing data on the breed distribution of cats in Denmark. The authors also wish to extend their gratitude to the Danish veterinarians who have registered the neoplastic cases on which this publication is based.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding has been obtained from the Danish Kennel Club for the creation and continuous running of the Danish Veterinary Cancer Registry.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
This work did not involve the use of animals (including cadavers) and therefore informed consent was not required. No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.