
Abstract
Case series summary
The objective of this study was to report the clinical presentation, diagnostic evaluation and outcome of ectopic ureter treatment in four female cats. Medical records of cats diagnosed with ectopic ureter between 2016 and 2021 were reviewed. Cats were included if they had a confirmed diagnosis of an extramural (three cases) or intramural (one case) ectopic ureter and underwent either surgical correction using an intravesicular end-to-side neoureterocystostomy technique or cystoscopic laser ablation. Information obtained from the medical records included history, signalment, clinicopathological data, imaging findings, treatment performed, postoperative complications and long-term clinical follow-up. Four female cats with unilateral ectopic ureters were identified, all of which (4/4) presented with urinary incontinence, with half (2/4) also having recurrent urinary tract infections. Pre-treatment diagnostics revealed three cases of extramural and one case of intramural ectopic ureters.
Relevance and novel information
Surgical correction was performed using intravesicular end-to-side neoureterocystostomy for the three cats with an extramural ectopic ureter and cystoscopic laser ablation for the cat with an intramural ectopic ureter. Long-term follow-up showed no recurrence of urinary incontinence or of lower urinary tract signs after ectopic ureter treatment (median follow-up 1705 days). This study demonstrates that both intravesicular end-to-side neoureterocystostomy and cystoscopic laser ablation are effective and safe long-term treatment options for cats with unilateral ectopic ureters.
Introduction
Ectopic ureters, although less commonly diagnosed in cats than in dogs, can result in persistent lower urinary signs and renal function impairment if left untreated, with the majority of current knowledge derived from canine studies.1,2 Although this condition is rare in cats, previous reports in dogs reveal that the most common clinical signs associated with ectopic ureters are urinary incontinence and often recurrent urinary tract infections (UTIs).1,2 Although research on the clinical presentation, treatment and outcomes of ectopic ureters in cats is limited compared with dogs, existing studies suggest that affected cats often present with urinary incontinence. In a small number of these cases, surgical correction has been shown to improve clinical signs. In one case study, chronic urinary incontinence successfully resolved in an 8-month-old female cat diagnosed with bilateral intramural ectopic ureters after treatment with cystoscopic laser ablation. 3 In a recent retrospective study of 12 cats undergoing cystoscopic or surgical correction for either unilateral or bilateral ectopic ureters, all cats had improvement in urinary incontinence after treatment. 4 Both studies reported excellent short-term outcomes for this patient population. Further research into the long-term outcomes of corrective treatments is essential for advancing the field’s knowledge of treatment efficacy and for providing accurate prognostic information for veterinarians managing these cases.
Similar to dogs, ectopic ureters in cats are classified as extramural or intramural based on their position relative to the bladder wall.1,5 Extramural ectopic ureters bypass both the bladder and the normal sphincter mechanism, draining directly into a distal part of the urogenital system (Figure 1a,b). In contrast, intramural ectopic ureters travel through the bladder wall before diverting to an abnormal opening (Figure 2a,b), typically the urethra and the vagina in females or the prostatic urethra in males.2,6,7 The diagnosis of ectopic ureters in cats commonly utilizes a combination of imaging modalities, including abdominal ultrasound, CT (Figure 3a,b) and cystoscopy with contrast to guide treatment planning 8 (Figure 3c,d).5,9 Cystoscopy is only feasible in female cats because of the small size of the male cat urethra.10,11 Treatment options for cats diagnosed with an extramural ectopic ureter include surgical correction using either an intravesicular or extravesicular reimplantation technique (end-to-side neoureterocystostomy) (Figure 1c). For intramural ectopic ureters, treatment options include surgical correction using either a side-to-side neoureterocystostomy or a reimplantation technique. Alternatively, in female cats, a minimally invasive approach such as cystoscopic laser ablation (Figure 2b,c) can be utilized.6,12,13
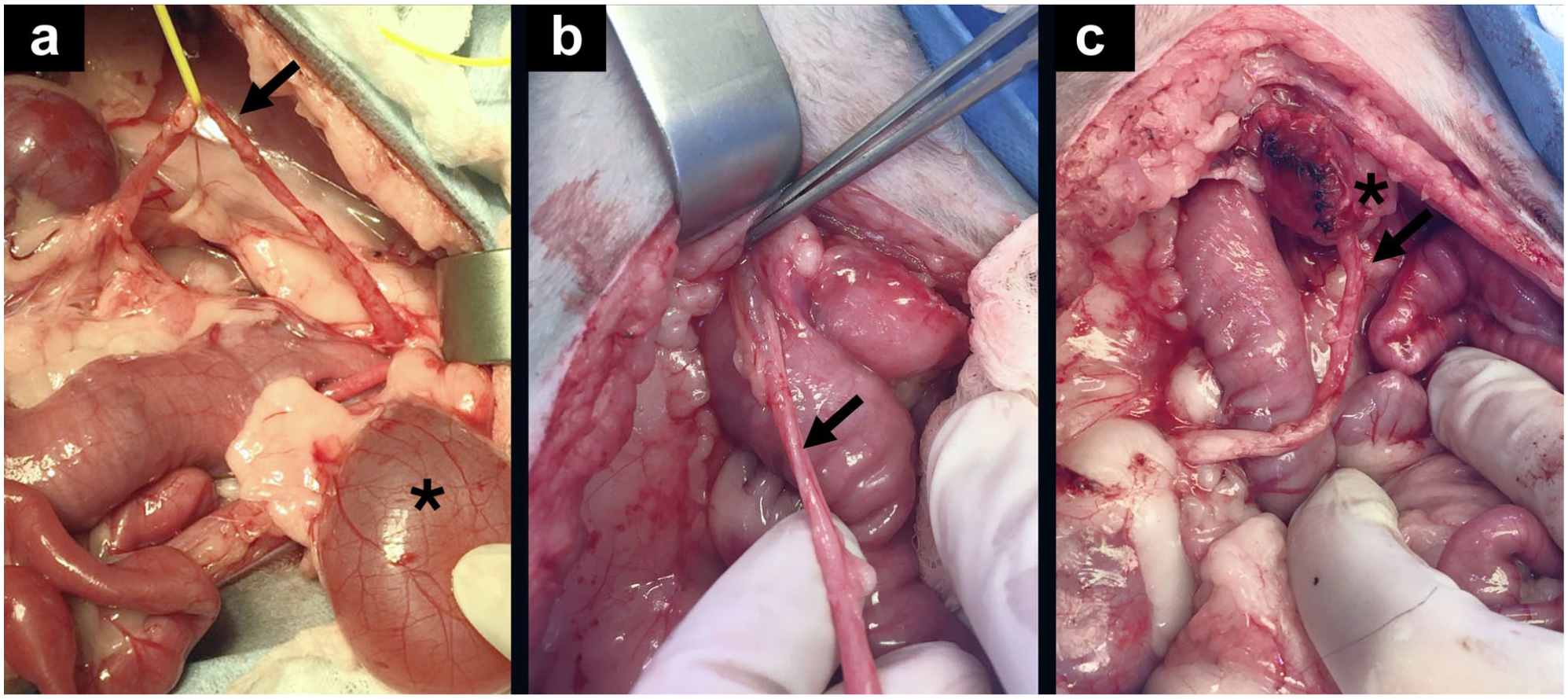
Representative images of extramural ectopic ureters (black arrows) (a,b) before surgical correction as well as (c) after end-to-side intravesicular neoureterocystostomy. Asterisks indicate the bladder (a,c)

Cystoscopy images of the cat with an intramural ectopic ureter: (a) before ablation; (b) showing the ureteral catheter and laser within the ureter; and (c) after ablation
This retrospective study reviewed the cases of four female cats diagnosed with unilateral ectopic ureters, focusing on their clinical presentation, diagnostic evaluation and treatment interventions. Notably, it provides the most extended follow-up reported to date for cats treated with either end-to-side intravesicular neoureterocystostomy or cystoscopic laser ablation for ectopic ureters. Furthermore, this case series includes a cat with a single functional kidney undergoing treatment for an ectopic ureter. By evaluating treatment outcomes, the study aims to enhance the current understanding of managing ectopic ureters in cats and to provide insights into the effectiveness of existing therapeutic approaches in achieving post-treatment urinary continence.
Case series description
Medical records from the Matthew J Ryan Veterinary Hospital at the University of Pennsylvania School of Veterinary Medicine were reviewed for the period between 2016 and 2021 for cats diagnosed with ectopic ureter. The inclusion criteria for this case series required a diagnosis of an ectopic ureter, classified as either extramural or intramural, determined by clinical signs, diagnostic imaging and visual confirmation of ureteral ectopia via cystoscopic evaluation or during abdominal exploration. Ectopic ureters were classified as extramural (implantation in an abnormal location distal to the bladder neck without tunneling through the bladder wall) (Figure 1a,b) or intramural (traveling through the bladder wall before opening in an abnormal location) (Figure 3a,b). 14 The exclusion criteria included cats with suspected ectopic ureters on initial diagnostic imaging that were not corrected, as well as those with incomplete medical records.

(a,b) CT images with contrast of the cat with an intramural ectopic ureter before ablation. The asterisk indicates the distal ureter (b). Fluoroscopy images with contrast showing the intramural ectopic ureter identified with (c) the ureteral catheter and (d) after ablation, demonstrating no contrast extravasation
Data obtained from the medical records included case signalment, medical history, preoperative antibiotic use and previously available clinicopathologic data. All cats underwent a physical examination followed by preoperative diagnostics including a blood chemistry panel, complete blood count (CBC), urine culture and imaging (abdominal ultrasound ± cystoscopy ± CT scan). Three cats diagnosed with an extramural ectopic ureter underwent surgical correction using an intravesicular end-to-side neoureterocystostomy technique and one cat diagnosed with an intramural ectopic ureter underwent cystoscopic laser ablation. Perioperative information, including additional procedures performed (one cat underwent ovariohysterectomy and one cat underwent ovariectomy) under the same anesthetic event alongside the surgical correction of the ectopic ureter, was also noted.
Clinical presentation
Four female cats met the inclusion criteria for this study. The population consisted of two (50%) intact and two (50%) spayed females (age range 1–4 years; median 1, interquartile range [IQR] 1.5). Breeds represented included three (75%) domestic shorthairs and one (25%) Scottish Fold. The cats’ weights were in the range of 2.4–3.8 kg (median 3.05, IQR 1.4), and the time from ectopic ureter diagnosis to treatment was in the range of 1–38 days (median 5, IQR 20.5). All four (100%) cats exhibited clinical signs related to their ectopic ureter, most notably intermittent urinary incontinence in 4/4 (100%) cats. All four (100%) cats had reported continuous urine dribbling with the ability to void a urine stream. Of the four cats, three (75%) had urine scalding on their legs and tail base on physical examination at initial presentation. Three cats (75%) had received prior courses of antibiotics for their urinary signs before treatment for their ectopic ureter, with one cat receiving multiple treatments of amoxicillin/clavulanic acid (13.75 mg/kg PO q12h). One cat had a previously documented UTI with a positive culture for Staphylococcus pseudintermedius treated with marbofloxacin (3.0 mg/kg PO q24h) and another had recurrent UTIs caused by Escherichia coli, treated with multiple courses of amoxicillin/clavulanic acid (15 mg/kg PO q12h) and marbofloxacin (3.5 mg/kg PO q24h). One cat (25%) had reported pollakiuria and hematuria, which were responsive to a veterinary prescription urinary diet. At the time of surgery, no cats were receiving antibiotic therapy and all cats had confirmed negative cultures. One cat had a previous diagnosis of polycystic kidney disease with an ipsilateral ectopic ureter, for which the cat had previously undergone a nephrectomy.
Pre-treatment diagnostics
A CBC and blood chemistry panel were performed before treatment for all cats. On CBC, one (25%) cat showed a stress leukogram, but no other significant abnormalities were detected. Blood chemistry results were unremarkable in all cats. Urinalysis was performed in 2/4 (50%) cats and was unremarkable. All cats (100%) had urine cultures performed, which showed no growth. In addition, before treatment, all cats (100%) underwent abdominal imaging. One cat (25%) had an abdominal ultrasound only, one (25%) cat underwent cystoscopy only, one (25%) cat received both ultrasound and cystoscopy, and the final cat underwent an ultrasound, cystoscopy and CT scan before treatment. Abdominal imaging revealed that three (75%) cats had extramural ectopic ureters, while one (25%) cat had an intramural ectopic ureter. The cat with an intramural ectopic ureter demonstrated distal hydroureter on abdominal ultrasound, with an abnormally caudal insertion site at the vesicourethral junction, positioned adjacent to and parallel with the urethra. A contrast-enhanced CT examination was subsequently performed, revealing the ureteral insertion near the anticipated trigone; however, no contrast from the left ureter was seen entering the bladder. Instead, a tubular structure continuous with the ureter extended caudally into the urethra, consistent with an intramural ectopic ureter.
Of the three cats diagnosed with extramural ectopic ureters, one underwent abdominal ultrasound exclusively, which showed a variably dilated ureter near the caudal aspect of the bladder, though its termination could not be visualized. Based on these findings, an extramural ectopic ureter was suspected. Another cat initially had a suspected extramural ureter based on abdominal ultrasound. Cystoscopy performed 1.5 years later revealed ureteral insertion at the mid-urethra. A contrast cystourethrogram confirmed the extramural nature of the ureter before surgical correction. The remaining cat, which had a single kidney at the time of ectopic ureter correction, underwent cystoscopy for diagnosis. A ureteral opening was identified within the proximal urethra, consistent with an ectopic ureter. On abdominal ultrasound, two (50%) cats showed evidence of renal pelvic dilation, and three (75%) cats had ureteral dilation on the affected side. One cat (25%) had mild bilateral loss of corticomedullary detail, consistent with a chronic nephropathy. All four cats were unilaterally affected, with three (75%) being affected on the left ureter and one (25%) on the right ureter.
Surgical procedure
Of the four cats treated, three (75%) underwent end-to-side intravesicular neoureterocystostomy (Figure 1c) for correction of a unilateral extramural ectopic ureter, while one (25%) underwent a cystoscopic laser ablation technique for a unilateral intramural ectopic ureter (Figure 2b,c). Antibiotics were administered in all four (100%) cases, with three (75%) cats receiving cefazolin (22 mg/kg IV 60 mins before the procedure and administered every 90 mins intraoperatively) and one (25%) receiving ampicillin (30 mg/kg IV 60 mins before the procedure and administered every 90 mins intraoperatively).
Cats that underwent surgery were premedicated with a combination of butorphanol (0.1–0.4 mg/kg IM) and alfaxalone (1–3 mg/kg IM) followed by induction with alfaxalone or propofol (1 mg/kg IV) titrated to desired sedation. Cats were maintained on either isoflurane or sevoflurane inhalant for the procedure. After surgery, cats were administered methadone (0.1–0.2 mg/kg IV) as needed for pain management. Cats were placed in dorsal recumbency and a ventral midline laparotomy performed. The surgical technique was performed as previously described. 15 Briefly, the affected ureter was dissected, using both blunt and sharp dissection, from retroperitoneal attachments as distally as possible into the pelvic canal. The ureter was ligated with two sutures of 4-0 polydioxanone (PDS) proximal to its attachment on the urethra and transected. A ventral midline cystotomy was performed. A mosquito hemostat was used to puncture a hole in the bladder apex and the end of the ureter grasped and brought directly into the bladder. The bladder was everted and the distal end of the ureter removed. The ureter end was spatulated with microvascular scissors for a distance of approximately 0.75 cm if not dilated. The ureteral mucosa was sutured to bladder mucosa using 8-0 nylon. Ureteral patency and urine flow were confirmed, the bladder inverted and routine closure performed using 4-0 PDS in a simple interrupted pattern.
Cystoscopic laser ablation
One cat was diagnosed with a unilateral intramural ectopic ureter and underwent a cystoscopic laser ablation technique. The same anesthetic protocol used for the surgical procedure was also applied to the cat undergoing laser ablation. The patient was placed under general anesthesia in dorsal recumbency, and cystoscopy with a 1.9 mm rigid endoscope within a 9 Fr sheath with a 3 Fr working channel to evaluate the lower urinary tract. A 3 Fr ureteral catheter was then placed over an 0.018-inch angled hydrophilic guidewire in the ectopic ureter. To confirm the intramural course of the ureter, a retrograde ureteropyelogram and urethrocystogram were performed using a 50:50 dilution of iohexol contrast administered via ureteral catheter. The intramural segment was clearly delineated during imaging, and the catheter was left in place to serve as a guide for subsequent laser ablation (Figure 2b,c). Laser ablation was performed using a 200 nm diode laser (DiodeVet), with serial contrast injections confirming the position and progression of the intramural tract. Ablation continued until the ureteral catheter was visualized exiting the bladder wall proximal to the trigone (Figure 3c). The new ureteral orifice was identified adjacent to the trigone, and a final contrast study confirmed correct positioning with no evidence of abdominal contrast extravasation (Figure 3d). There were no reported perioperative complications, and all four (100%) cats recovered uneventfully from anesthesia.
Post-treatment and long-term clinical follow-up
After surgery, 3/4 (75%) cats had no immediate postoperative complications. The cat with a solitary kidney after undergoing a previous nephrectomy developed azotemia (creatinine 6.7 mg/dl, blood urea nitrogen [BUN] 95 mg/dl) 24 h after intravesicular neoureterocystostomy. This cat was continued on cefazolin (22 mg/kg IV q8h) for 3 days in addition to fluid therapy (5 ml/kg/h IV balanced isotonic crystalloid) and two doses of an anti-inflammatory, dexamethasone sodium phosphate (0.11 mg/kg IV q24h). The cat was also administered a single dose of mannitol (0.25 g/kg IV) because of decreased urine production. At 72 h postoperatively, the cat’s creatinine and BUN returned to normal (creatinine 1.2 mg/dl and BUN 22 mg/dl) and antibiotics, as well as steroids, were discontinued at this time. The cat undergoing cystoscopic laser ablation for an intramural ectopic ureter received a single dose of dexamethasone sodium phosphate (0.11 mg/kg IV) and was discharged on a 5-day course of amoxicillin/clavulanic acid (16 mg/kg PO q12h), a standard practice after cystoscopic laser procedures to prevent secondary infection from contamination of the ablated tissue by perivulvar and vestibular flora.
The remaining three cats were not discharged on antibiotic therapy after surgery. None of the cats had positive urine cultures from samples collected during the procedures. No cats were azotemic at the time of discharge. By day 14 after the ectopic ureter correction, all cats had resolution of urinary incontinence and of lower urinary tract signs. Long-term follow-up for the cats was in the range of 1291–3181 days (median 1705 days, IQR 1350 days). At the time of follow-up, all cats were alive and none (0/4) had recurrence of incontinence or development of additional urinary signs. On follow-up urine cultures taken 14 days to 2 months after treatment, 3/4 (75%) cats showed no bacterial growth. One cat treated with end-to-side intravesicular neoureterocystostomy had a recurrence of E coli UTIs 1.5 years postoperatively and was consequently treated with marbofloxacin (3 mg/kg PO q24h) for multiple 14-day courses at subsequent follow-up appointments with the primary veterinarian. Most recently, this cat had a negative urine culture with no evidence of organism growth for 7 months at the time of writing this report. No cats required a second surgical procedure after ectopic ureter treatment. Abdominal ultrasound was performed 4–6 weeks after the procedure in 3/4 (75%) cats. Of the two cats with renal pelvic dilation before the procedure, both showed improvement, though not complete resolution of dilation. Similarly, the three cats with ureteral dilation before intervention had some improvement also identified. Throughout the follow-up period, all cats remained non-azotemic.
Long-term follow-up for the cats was in the range of 1291–3181 days (median 1705, IQR 1350). At the time of follow-up, all cats were alive, and none had recurrence of incontinence or development of additional urinary signs.
Statistical analysis
All collected data were presented as median and IQR. Summary statistics, including percentages, medians and IQRs, were calculated using GraphPad Prism.
Discussion
This study represents the longest-term reported case series of four female cats treated for unilateral ectopic ureters, including a unique case involving a cat with a single kidney, and provides valuable insights into their clinical presentation, diagnostic approach and outcomes after corrective treatment. Despite the small sample size, the resolution of clinical signs and the lack of long-term postoperative complications or recurrence of urinary incontinence point to positive outcomes for cats with ectopic ureters after treatment. These results suggest a favorable long-term prognosis after correction and the authors recommend that, when available, treatment for ectopic ureter correction should be pursued.
All four cats exhibited common clinical signs of ectopic ureters previously reported in both canine and feline patients, including urinary incontinence and, to a lesser extent, recurrent UTIs. In this report, end-to-side intravesicular neoureterocystostomy was the most frequently performed procedure, successfully correcting the extramural ectopic ureters in all three cats for which it was performed. The use of cystoscopic laser ablation for the single intramural case highlights the effectiveness of this minimally invasive technique for future use in female feline patients diagnosed with intramural ectopic ureters. The long-term follow-up in this study (range 1291–3181 days) is the longest reported to date for cats treated for ectopic ureters, highlighting the sustained efficacy of both correctional procedures. In addition, the successful treatment of an ectopic ureter in a cat with a solitary kidney highlights the effectiveness of treatment even in a cat with existing urogenital comorbidities. All four cats remained free of urinary incontinence after surgery, with only one developing UTIs after correction, which have since resolved. The cat that presented with pollakiuria and hematuria no longer exhibits these clinical signs after ectopic ureter correction. In addition, none of the cats required additional procedures for their ectopic ureter and none were azotemic at the time of writing this report, further supporting the long-term efficacy of both treatment approaches.
The favorable outcomes observed in the four cats from this case series underscore the necessity of comprehensive evaluation and accurate diagnosis of ectopic ureters, given the potential for successful treatment. Given the rarity and potential underdiagnosis of this condition, conducting a comprehensive clinical evaluation of cats with urinary incontinence, rather than defaulting to empirical treatment for more common issues such as feline idiopathic cystitis (FIC) or infection, could improve long-term outcomes. 16 In addition, an accurate diagnosis could reduce the risk of complications from untreated ectopic ureters, such as renal impairment caused by hydronephrosis resulting from partial ureteral obstruction secondary to ureteral ectopia.17,18 Interestingly, although this study, in conjunction with the previously reported outcomes in cats treated for ectopic ureters, involved a smaller number of cases compared with the literature on dogs treated for the same condition, initial findings suggest that the resolution of urinary incontinence in cats after either end-to-side intravesicular neoureterocystostomy or cystoscopic laser ablation may be superior to the results typically achieved in dogs. Although recent studies in dogs have reported success rates for resolving incontinence within 1 month of treatment in the range of 68–80%, a recently published case series on cats suggested a 92% success rate, and the present study reports a 100% success rate in resolving urinary incontinence in cats after treatment.4,19,20 Studies on ectopic ureter treatment in dogs suggest that many patients require additional procedures or ongoing medical management to address persistent urinary signs – such as medications (phenylpropanolamine and estriol), collagen injections or placement of a urethral hydraulic occluder for dogs with urethral sphincter mechanism incompetence (USMI).19,20 Although USMI and hydraulic occluder placement has been described in cats, there is no known incidence of USMI diagnosed in cats after ectopic ureter correction. 21 Although additional literature is needed to comprehensively evaluate the efficacy of ectopic ureter treatment in cats, initial reports suggest that cats may have a better prognosis for regaining urinary continence after correction, with fewer functional abnormalities (such as USMI) requiring additional treatment, compared with dogs.
This study has some limitations, notably the small sample size (n = 4) and retrospective nature of the study. Overall, this study provides evidence that both end-to-side intravesicular neoureterocystostomy and cystoscopic laser ablation are effective, safe and durable treatment options for ectopic ureters in cats. The favorable long-term outcomes, including the resolution of incontinence and stable renal function, are promising for the management of this condition. Future research should explore the underlying mechanisms behind treatment success and identify factors that may further improve outcomes for affected cats.
Conclusions
Surgical correction and cystoscopic laser ablation are effective treatment options for cats with extramural and intramural ectopic ureters and should be pursued after diagnosis. A better understanding of the positive long-term outcomes in these cases is essential for veterinarians to provide accurate guidance during treatment planning.
Footnotes
Acknowledgements
The authors would like to acknowledge the Ryan Veterinary Hospital faculty, staff and students involved in the diagnostics and treatments of these four cases.
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognized high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animals described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedures undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.