
Abstract
Objectives
This study aimed to evaluate factors associated with recurrence of clinical signs after balloon dilation in cats with nasopharyngeal stenosis (NPS).
Methods
A retrospective multicentre study was conducted using data collected from the medical records of cats treated for NPS using balloon dilation. A total of 47 cats, each with a follow-up period of ⩾180 days, were included in the analysis of progression-free interval (PFI) and hazard ratio (HR) using Kaplan–Meier and Cox proportional hazards analyses.
Results
Multiple balloon dilations were planned for 26/47 cats. In total, 14 cats received three procedures and 12 cats received two. The dilations were performed at a median interval of 35 days (interquartile range [IQR] 29–39, range 15–127), regardless of transient recurrence. A single dilation was planned for the remaining 21 cats. Recurrence after the final balloon dilation occurred in 18/47 (38%) cats; in these cases, the median time from the final dilation to recurrence was 42 days (IQR 18–142, range 6–2303). The median PFI was 2303 days (range 6–2704), with 6-month and 1-year recurrence-free rates of 70% and 65%, respectively. Multivariate analysis revealed that performing planned multiple dilations was the only variable associated with improved PFI (HR 0.06, 95% confidence interval [CI] 0.01–0.30; P < 0.001). Specifically, cats undergoing planned multiple dilations had higher 6-month (92% vs 43%) and 1-year (88% vs 38%) progression-free rates than those undergoing a single dilation. No significant correlation was observed between PFI and the number of balloon dilation treatments.
Conclusions and relevance
Balloon dilation repeated two or three times, regardless of any recurrence of signs, may assist in the long-term resolution of NPS in some cases.
Introduction
Nasopharyngeal stenosis (NPS) in cats is characterised by pathological narrowing of the nasopharynx. It often causes inspiratory difficulty, stertor, sneezing, gagging, open-mouth breathing, dysphagia and nasal discharge; moreover, it may involve regurgitation, vomiting and anorexia, as well as dyspnoea in more severe cases.1 –16 NPS can occur as a congenital abnormality9,14 or develop secondarily to nasopharyngeal inflammation induced by upper respiratory infection,1 –3,7 chronic rhinitis,8,14 aspiration rhinitis caused by vomitus flowing into the nasopharynx, 14 trauma 14 or previous surgery.8,14
Treatments for NPS include forceps dilation, balloon dilation (BD), transpalatal reconstruction with or without mucosal flap rotation, metallic stent placement and covered metallic stent placement.1 –8,10 –14 Among them, BD is considered the most minimally invasive treatment and can be simultaneously performed with diagnostic endoscopy; however, it often only results in transient relief of clinical signs because of prompt NPS relapse.2,4,5,13,14 A previous case series suggested that systemic corticosteroid administration immediately after BD might effectively prevent recurrence; 7 however, this has not been confirmed by subsequent studies.13,14 In addition, although some case reports have suggested that multiple procedures may be necessary to maintain long-term improvement of clinical signs,4,13,14 the optimal protocol for BD remains to be established.
This retrospective study aimed to evaluate factors associated with recurrence of NPS after BD.
Materials and methods
Case selection
Medical records from the Veterinary Medical Teaching Hospital at Nippon Veterinary and Life Science University, Veterinary Teaching Hospital at Kagoshima University and Hyogo Pet Medical Center Higashinada, between February 2016 and June 2024, were reviewed to identify cats diagnosed with NPS through nasopharyngeal endoscopy. All cases in this study were referred to these institutions from primary care veterinarians. CT or MRI was also performed in some cases and cats that underwent BD as an initial treatment for NPS were included. Cases were excluded if there was a lack of follow-up information, or if they were still alive or had died from causes unrelated to NPS without relapse but had a follow-up period of fewer than 180 days after the completion of initial treatment.
Balloon dilation procedure
Cats were anaesthetised and intubated, and a flexible endoscope was retroflexed around the soft palate and into the nasopharynx to confirm stenosis. A BD catheter was introduced through the external nostril to assess nasopharyngeal patency. In cases where the catheter could not pass because of imperforate NPS, patency of the stenotic area was achieved through tissue curettage using endoscopic forceps or by employing an argon plasma laser. Once patency was endoscopically confirmed, a BD catheter was inserted through the external nostril and advanced into the nasopharynx. The position of the balloon catheter was determined using lateral radiographs to ensure that the balloon centre was positioned at the most stenotic site identified through radiography, CT or MRI. Balloon diameters and dilation times were available for 33/47 cases. Diameters were in the range of 6–10 mm (median 7) and dilation times were in the range of 2–20 mins (median 10). The balloon was endoscopically visualised during the procedure. After dilation, the catheter was removed, followed by nasopharyngeal endoscopy to confirm the success of the dilation. After BD, some cats received corticosteroids as nasal drops for 3–4 weeks, administered as difluprednate 0.5 mg/ml q12h or fluorometholone 0.2 mg/ml q12h, and others received inhaled fluticasone 100 μg q12h or prednisolone (0.5–1 mg/kg q24h PO), based on the clinician’s judgement.
Our hypothesis was that performing multiple BDs, regardless of recurrence, would help achieve long-term remission of NPS. Therefore, 2–3 BDs were routinely performed at monthly intervals. However, the decision to proceed with these planned BDs ultimately depended on the preference and consent of the owner.
Medical record review and follow-up data
The following data were collected from the medical database: signalment; body weight; clinical signs at the time of presentation; duration of the clinical signs; pulse oximetry saturation; partial pressure of mixed venous carbon dioxide; radiography, CT and MRI findings; dates and procedures for BDs, including the number of dilations; whether multiple dilations were planned; administration of corticosteroids, antibiotics or both after the BD procedure; periprocedural complications associated with BD; and outcomes including the date of recurrence and last follow-up. The duration of the clinical signs was defined as the period from the owner-reported onset to the time of diagnosis.
Referring veterinarians or owners were contacted via telephone or email during data collection to obtain additional follow-up information. NPS recurrence was defined based on the presence of clinical signs such as stertor, sneezing and increased respiratory effort, with confirmation through nasopharyngeal endoscopy where possible.
Statistical analysis
The normality of continuous data distribution was assessed using the Shapiro–Wilk test, along with evaluations of skewness, kurtosis and q–q plots. Normally distributed variables are presented as mean ± SD and median (interquartile range [IQR]), respectively. The primary end point of the study was the progression-free interval (PFI), defined as the time from the last planned BD to the date of recurrence, which was considered to occur after the final planned dilation. The Kaplan–Meier method and Cox proportional hazards analysis were used to assess the association between PFI and each variable. Continuous variables were categorised based on their median or mean values. Univariate Cox proportional hazards analysis was first used to evaluate the association between PFI and each variable. Variables with a P value <0.10 in the univariate analysis were subsequently included in a multivariate Cox proportional hazards model. P <0.05 in the multivariate analysis was considered statistically significant.
All statistical analyses were carried out using R version 4.4.1 and EZR software, which is a graphical user interface for R and a modified version of R-Commander. 17
Results
Clinical characteristics
A total of 71 cats were considered for treatment with BD; of these, 47 met the inclusion criteria. Tables 1 and 2 summarise the clinical characteristics and diagnostic imaging findings, respectively. The breeds included 43 (91%) non-pedigree cats and four (9%) pedigree cats. Pedigree cats included Munchkin (n = 2), Abyssinian (n = 1) and American Shorthair (n = 1) cats. Head and thoracic radiography were performed in 40 and 42 cats, respectively. In 16 of these cats, fluoroscopy was also performed to detect dynamic alterations such as pharyngeal dilation and collapse. Of the 47 cats, 26 (55%) were diagnosed with episodes of suspected upper respiratory infections (URTI) by the referring veterinarian, which may cause NPS. Other suspected causes of NPS included vomiting or regurgitation (n = 4, 9%), cleft palate (n = 2, 4%), chronic sinorhinitis (n = 1, 2%) and prior anaesthesia (n = 1, 2%). The cause of NPS was not identified in 13 cats.
Signalment, clinical signs and respiratory parameters of cats with nasopharyngeal stenosis (n = 47)

Data are n (%), mean ± SD or median (IQR)
Percentages were calculated based on the number of available cases
IQR = interquartile range; PvCO2 = partial pressure of mixed venous carbon dioxide; SpO2 = pulse oximetry saturation
Radiographic, CT/MRI and endoscopic findings in cats with nasopharyngeal stenosis (NPS) (n = 47)

Data are n (%) or median (interquartile range [IQR])
Percentages were calculated based on the number of available cases
Follow-up and analysis of factors associated with recurrence
Of the 47 cats, 26 had planned multiple BDs (14 cats received three dilations and 12 received two dilations), with a median interval of 35 days (IQR 29–39, range 15–127). The remaining 21 cats were planned for a single dilation. Among the 26 cats that had planned multiple BDs, 3/26 (12%) experienced transient recurrence by the time of the second or third planned BD. Corticosteroids were administered to 36 cats after BD; these included fluorometholone (n = 15), prednisolone (n = 10), fluorometholone with prednisolone (n = 4), fluticasone (n = 3), fluticasone with fluorometholone (n = 2), prednisolone, fluorometholone with fluticasone (n = 1) and difluprednate (n = 1). Post-dilation complications were observed in 4/47 (9%) cats, including cleft palate (n = 2) and mediastinal and/or subcutaneous emphysema (n = 2). Two cats developed a cleft palate; however, in one case, the cat had a previous cleft palate that had been surgically repaired before BD that recurred after the procedure. The other developed a cleft palate after it underwent nine BDs.
The median follow-up period was 482 days (IQR 260–1109, range 6–2704), with recurrence observed in 18/47 (38%) cats. Among the 18 cats with recurrence, the median time from the last BD to recurrence was 42 days (IQR 18–142, range 6–2303). Further, 10 and eight cases of recurrences were identified based on nasopharyngeal endoscopy and clinical signs, respectively. Of the 29 cats without recurrence, 25 were still alive without relapse at the time of data analysis, three were lost to follow-up and one died due to progression of chronic kidney disease. The median PFI for all 47 cats was 2303 days (range 6–2704), with the 6-month and 1-year progression-free rates being 70% and 65%, respectively.
Univariate Cox proportional hazards regression analysis identified two variables for consideration in the multivariate model (ie, P <0.10): middle location of NPS (HR 0.38, 95% CI 0.13–1.11; P = 0.08) and planned multiple BDs (HR 0.10, 95% CI 0.03–0.34; P <0.001) (Table 3). A subsequent multivariate analysis revealed that performing planned multiple BD was the only factor associated with improvement in PFI (HR 0.06, 95% CI 0.01–0.30; P <0.001) (Table 4). Specifically, cats undergoing planned multiple dilations did not reach the median PFI and had higher 6-month (92% vs 43%) and 1-year (88% vs 38%) progression-free rates than those undergoing a single dilation, which had a median PFI of 112 days (Figure 1). In addition, Cox proportional hazards analysis comparing cats that received two and three planned dilations revealed no significant between-group differences (HR 2.56, 95% CI 0.23–28.42; P = 0.45).
Progression-free rates and results of univariate Cox proportional hazards analysis to identify factors associated with recurrence in 47 cats with nasopharyngeal stenosis (NPS), with a follow-up period ⩾180 days after the final balloon dilation
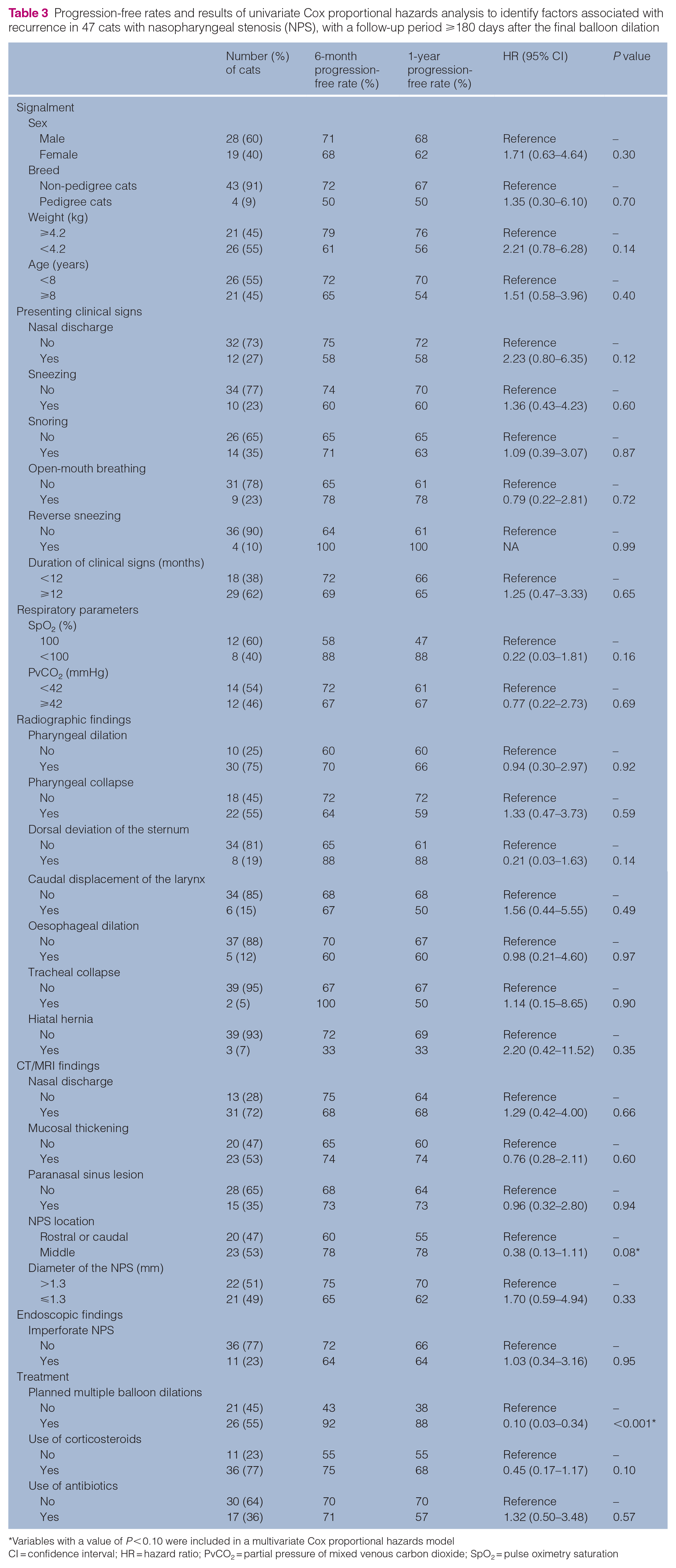
Variables with a value of P < 0.10 were included in a multivariate Cox proportional hazards model
CI = confidence interval; HR = hazard ratio; PvCO2 = partial pressure of mixed venous carbon dioxide; SpO2 = pulse oximetry saturation
Multivariate cox proportional hazard analysis results determining factors associated with recurrence in 47 cats with nasopharyngeal stenosis after the final balloon dilation

CI = confidence interval; HR = hazard ratio
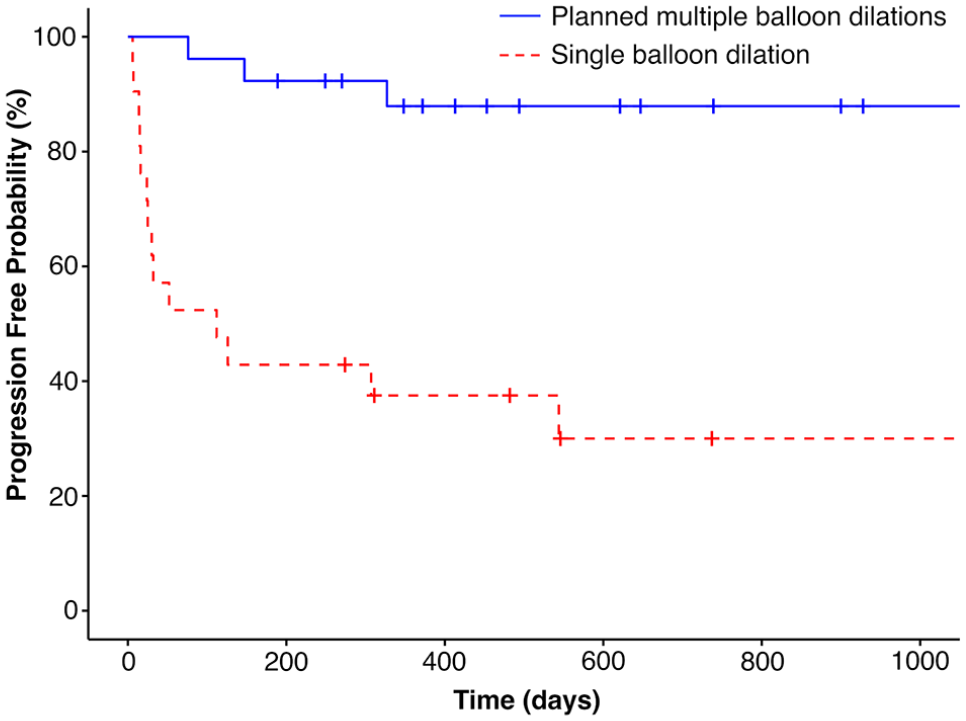
Kaplan–Meier curve of the progression-free interval (PFI) after the final balloon dilation (BD) in cats with nasopharyngeal stenosis that received (n = 26; blue solid line) or did not receive (n = 21; red dashed line) planned multiple BDs. Cats that underwent planned multiple BDs did not reach the median PFI and had higher 6-month (92% vs 43%) and 1-year (88% vs 38%) progression-free rates compared with those that received a single dilation (median PFI: 112 days). Tick marks indicate censored cats
Among 15 cats that received a single BD and experienced recurrence, eight received rescue therapy, including additional BD (n = 7) and placement of temporary silicone tubing (n = 1). Among the seven cats that received additional BD, four underwent only one dilation each; however, these four cats were lost to follow-up. The remaining three cats required multiple dilations owing to repeated recurrences, undergoing procedures four, eight and nine times, respectively; however, none of them achieved remission. One cat that underwent temporary silicone tube placement achieved remission.
Two of the three cats that underwent planned multiple BD and experienced recurrence received additional BD as rescue therapy. One of these cats underwent one additional dilation but was subsequently lost to follow-up. Despite undergoing two additional dilations, the other cat experienced relapse and subsequently underwent silicone tubing placement. The cat developed acute gastroenteritis and respiratory failure and was euthanased 6 days after tube placement.
Discussion
Our findings indicated that planned multiple BDs are associated with an improvement in the PFI, which is consistent with previous small-scale reports, suggesting that multiple procedures may be needed to maintain long-term improvement of clinical signs of NPS.4,13,14 No significant correlation was observed between PFI and the number (two or three) of BD treatments, indicating the need for further studies to determine the optimal number of treatments. Most cats underwent additional BDs as a rescue treatment after recurrence. All four cats that underwent ⩾4 BDs experienced repeated recurrences and did not achieve long-term remission. Therefore, in cases where recurrence occurs even after three BDs, alternative interventions such as silicone tube or stent placement may be warranted.
Planned multiple BDs increased costs, required multiple anaesthetic events and came with a small risk of complications. Of the seven cats that relapsed after a single BD, four underwent one additional BD but were lost to follow-up and three received multiple additional BDs but did not achieve lasting remission. Therefore, it remains unclear whether the outcomes of additional BDs after relapse for cats that have undergone only a single procedure are comparable with those of cats with planned multiple BDs. Cases of single procedures may require additional procedures and therefore incur higher costs than planned multiple BDs. A previous study reported that a single procedure combining balloon or forceps dilation with temporary silicone tube placement achieved high rates of success; 11 however, a review reported poor tolerance (eg, severe gagging and local inflammation) and limited long-term remission. 12 Taken together, whereas planned multiple BDs may be useful if the anaesthesia risk and costs are acceptable, treatment should be individualised based on the severity of stenosis, owner preferences and the conditions of each case. Single-procedure alternatives should also be considered.
The NPS lesions were commonly localised in the middle third of the nasopharynx (53%). In the univariate analysis, lesions in the middle third of the nasopharynx were significantly associated with post-dilation PFI improvement compared with lesions in the rostral or caudal regions. However, these correlations were not retained in the multivariate analysis. In addition, a previous study reported that BD is most successful for lesions located in the caudal third of the nasopharynx. 14 In our study, a higher proportion of cats underwent planned BD in the middle third of the nasopharynx (16/23, 69%) than in the rostral or caudal third (9/20, 45%), which may have influenced the outcomes. Further studies are warranted to clarify the association between the lesion location and PFI after BD.
This study has several limitations. First, the retrospective design and presence of missing variables in some cases may have influenced the statistical analysis. In addition, the protocol for BD, including balloon diameter and dilation time, varied in accordance with the severity of stenosis in each case and the treatment institution. Although signs of suspected URTI were reported in over half of the cases based on the diagnosis of the referring veterinarian and owner-reported information, clinical signs of chronic URTI may overlap with those caused by NPS itself. Therefore, it is challenging to definitively determine whether URTI was a primary cause of NPS in these cases. As a result of this uncertainty, underlying diseases such as URTI were not included in the analysis.
Conclusions
BD repeated two or three times, regardless of recurrence of clinical signs, may assist in the long-term resolution of NPS in some cases.
Footnotes
Conflict of interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work was supported by the Initiative for Realizing Diversity in the Research Environment from MEXT, Japan, 2023–2025.
Ethical approval
The work described in this manuscript involved the use of non-experimental (owned or unowned) animals. Established internationally recognised high standards (‘best practice’) of veterinary clinical care for the individual patient were always followed and/or this work involved the use of cadavers. Ethical approval from a committee was therefore not specifically required for publication in JFMS. Although not required, where ethical approval was still obtained, it is stated in the manuscript.
Informed consent
Informed consent (verbal or written) was obtained from the owner or legal custodian of all animal(s) described in this work (experimental or non-experimental animals, including cadavers, tissues and samples) for all procedure(s) undertaken (prospective or retrospective studies). No animals or people are identifiable within this publication, and therefore additional informed consent for publication was not required.